
Utilizing Multi-Class Classification Methods for Automated Sleep Disorder Prediction



Abstract
1. Introduction
- Firstly, raw data analysis is applied to understand nominal features’ frequency of occurrence and the most representative category and identify their relatedness with the sleep disorder classes. Also, a statistical analysis of numerical features is presented in the whole dataset and per class group. One-way analysis of variance (ANOVA) [36] was applied to identify if there are differences in means among the three groups’ numerical features. Due to the rejection of means equality (null hypothesis), we proceeded to the Tukey–Kramer post hoc test to find which pairs were different.
- Secondly, emphasis is given to the feature-wise pre-processing step to ensure that feature data are correctly captured before feeding them to the block which is responsible for the prediction models’ training. For this purpose, an unsupervised filter is applied to turn attributes with discrete/categorical numeric values into nominal ones. Also, numerical data normalization is applied.
- Thirdly, pre-processing is followed by feature analysis to measure their importance to the sleep disorder class variable by selecting random forests (RFs) and, specifically, the Gini impurity index and information gain (InfoGain) methods.
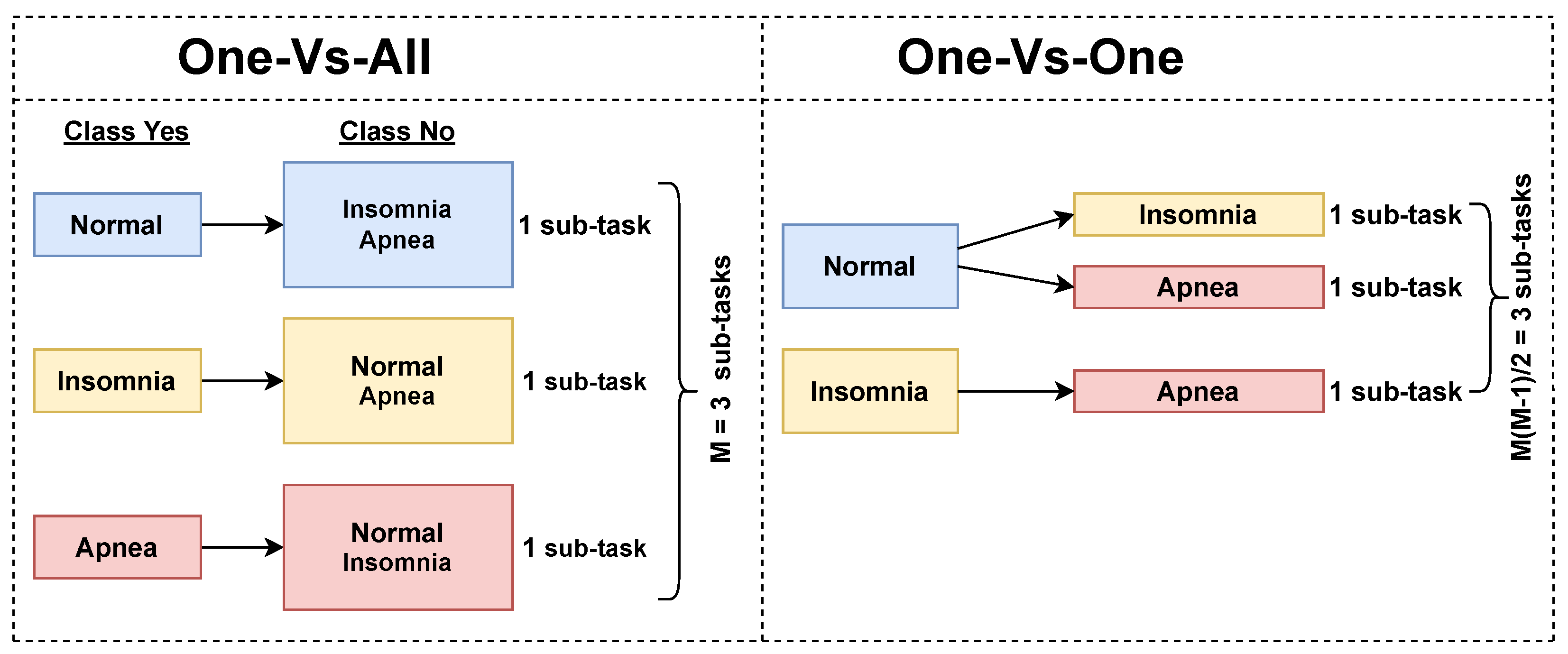
- Finally, a sleep disorder prediction approach is analytically presented where two well-known decomposition strategies, OVA and OVO, are adapted to the problem under consideration and are evaluated assuming LR and SVM as base models for building the 2-class classifiers involved in the internal mechanism of each strategy. To decide which of these strategies is more efficient, we considered two experimental cases, one with all available features and one after feature selection, where accuracy, kappa score (K), precision, recall, f-measure, and AUC metrics were measured and compared. All metrics unveiled that, irrespective of the strategy, 2-degree polynomial SVM prevailed over the other combinations; thus, it is the main proposition of this analysis.
2. Related Works
3. Materials and Methods
3.1. Dataset Description
- Age (years): The age of the person in years.
- Gender: The person’s gender (Male/Female).
- Occupation: The occupation or profession of the person.
- Sleep Duration (hours): The number of hours the person sleeps per day.
- Quality of Sleep—QoSleep (scale: 1–10): A subjective rating of the quality of the person’s sleep, ranging from 1 to 10.
- Physical Activity Level (minutes/day): The number of minutes the person engages in physical activity daily.
- Stress Level (scale: 1–10): A subjective rating of the stress level experienced by the person, ranging from 1 to 10.
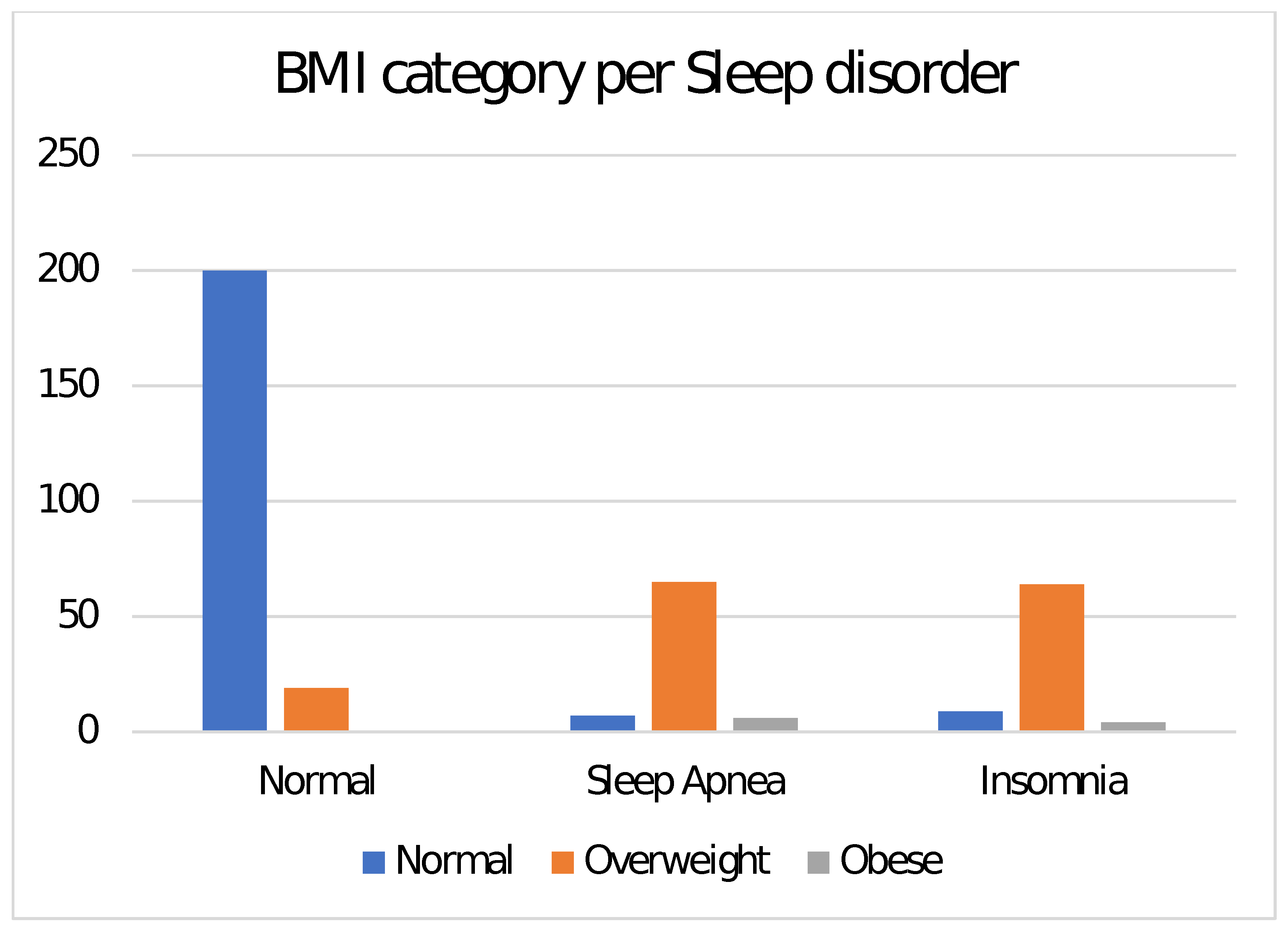
- Boby Mass Index (BMI) Category: The BMI category of the person (e.g., Underweight, Normal, Overweight).
- Blood Pressure (mmHg): The blood pressure measurements for the person, indicated as systolic blood pressure (SysBP) over diastolic blood pressure (DiasBP).
- Heart Rate (bpm): The resting heart rate of the person in beats per minute.
- Daily Steps: The number of steps the person takes daily.
- Asthma: A nominal feature that captures if a subject suffers from asthma or not.
- Sleep Disorder: This feature relates to the class variable and, thus, captures the presence or absence of a sleep disorder in the person spanning into Normal (219 instances), Sleep Apnea (78 instances) and Insomnia (77 instances) categories.
- Normal: The individual does not exhibit any specific sleep disorder.
- Insomnia: The individual experiences difficulty falling or staying asleep, leading to inadequate or poor-quality sleep.
- Sleep Apnea: The individual suffers from pauses in breathing during sleep, resulting in disrupted sleep patterns and potential health risks.
3.2. Dataset Analysis
- .
- or or .
3.3. Data Preprocessing
3.4. Features Importance
3.5. Multi-Class Classification Approach
- Linear: , where the first term is the inner product of feature vectors and and C is an optional constant.
- Radial Basis Function (RBF): , where and is an adjustable parameter for measuring the performance of the kernel.
- Polynomial: , where and d are adjustable parameters that stand for the slope, constant term and polynomial degree, respectively.
3.6. Confusion Matrix in Multi-Class Classification
3.7. Experiments Environment and Setup
4. Results
5. Conclusions and Future Works
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Solomon, C. Health Benefits of Sleep: Why Is Getting Enough Rest So Important. Altern. Med. 2022, 26–29. [Google Scholar]
- World Sleep Day. Available online: https://worldsleepday.org/ (accessed on 4 July 2024).
- Blumberg, M.S.; Lesku, J.A.; Libourel, P.A.; Schmidt, M.H.; Rattenborg, N.C. What is REM sleep? Curr. Biol. 2020, 30, R38–R49. [Google Scholar] [CrossRef] [PubMed]
- Dauvilliers, Y.; Schenck, C.H.; Postuma, R.B.; Iranzo, A.; Luppi, P.H.; Plazzi, G.; Montplaisir, J.; Boeve, B. REM sleep behaviour disorder. Nat. Rev. Dis. Prim. 2018, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Ramar, K.; Malhotra, R.K.; Carden, K.A.; Martin, J.L.; Abbasi-Feinberg, F.; Aurora, R.N.; Kapur, V.K.; Olson, E.J.; Rosen, C.L.; Rowley, J.A.; et al. Sleep is essential to health: An American Academy of Sleep Medicine position statement. J. Clin. Sleep Med. 2021, 17, 2115–2119. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Dutil, C.; Sampasa-Kanyinga, H. Sleeping hours: What is the ideal number and how does age impact this? Nat. Sci. Sleep 2018, 10, 421–430. [Google Scholar] [PubMed]
- Li, J.; Cao, D.; Huang, Y.; Chen, Z.; Wang, R.; Dong, Q.; Wei, Q.; Liu, L. Sleep duration and health outcomes: An umbrella review. Sleep Breath. 2021, 26, 1479–1501. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Dutil, C.; Featherstone, R.; Ross, R.; Giangregorio, L.; Saunders, T.J.; Janssen, I.; Poitras, V.J.; Kho, M.E.; Ross-White, A.; et al. Sleep duration and health in adults: An overview of systematic reviews. Appl. Physiol. Nutr. Metab. 2020, 45 (Suppl. 2), S218–S231. [Google Scholar]
- Mason, G.M.; Lokhandwala, S.; Riggins, T.; Spencer, R.M. Sleep and human cognitive development. Sleep Med. Rev. 2021, 57, 101472. [Google Scholar]
- Luyster, F.S. Sleep and health. In Encyclopedia of Behavioral Medicine; Springer International Publishing: Cham, Switzerland, 2020; pp. 2052–2055. [Google Scholar]
- Matricciani, L.; Paquet, C.; Galland, B.; Short, M.; Olds, T. Children’s sleep and health: A meta-review. Sleep Med. Rev. 2019, 46, 136–150. [Google Scholar] [CrossRef]
- Ophoff, D.; Slaats, M.A.; Boudewyns, A.; Glazemakers, I.; Van Hoorenbeeck, K.; Verhulst, S. Sleep disorders during childhood: A practical review. Eur. J. Pediatr. 2018, 177, 641–648. [Google Scholar] [CrossRef]
- Nelson, K.L.; Davis, J.E.; Corbett, C.F. Sleep quality: An evolutionary concept analysis. In Proceedings of the Nursing Forum; Wiley Online Library: Hoboken, NJ, USA, 2022; Volume 57, pp. 144–151. [Google Scholar]
- Hauri, P.J. Sleep Disorders; Routledge: London, UK, 2021; pp. 211–260. [Google Scholar]
- Nutt, D.; Wilson, S.; Paterson, L. Sleep disorders as core symptoms of depression. Dialogues Clin. Neurosci. 2022, 10, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef] [PubMed]
- The AASM International Classification of Sleep Disorders—Third Edition, Text Revision (ICSD-3-TR). Available online: https://aasm.org/clinical-resources/international-classification-sleep-disorders/ (accessed on 4 July 2024).
- Pavlova, M.K.; Latreille, V. Sleep disorders. Am. J. Med. 2019, 132, 292–299. [Google Scholar] [CrossRef]
- Kayabekir, M. Sleep physiology and polysomnogram, physiopathology and symptomatology in sleep medicine. In Updates in Sleep Neurology and Obstructive Sleep Apnea; BoD—Books on Demand: Norderstedt, Germany, 2019. [Google Scholar]
- Klingman, K.J.; Jungquist, C.R.; Perlis, M.L. Questionnaires that screen for multiple sleep disorders. Sleep Med. Rev. 2017, 32, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, M.; Beracci, A.; Martoni, M.; Meneo, D.; Tonetti, L.; Natale, V. Measuring subjective sleep quality: A review. Int. J. Environ. Res. Public Health 2021, 18, 1082. [Google Scholar] [CrossRef] [PubMed]
- Konstantoulas, I.; Kocsis, O.; Dritsas, E.; Fakotakis, N.; Moustakas, K. Sleep Quality Monitoring with Human Assisted Corrections. In Proceedings of the IJCCI, Online, 25–27 October 2021; pp. 435–444. [Google Scholar]
- Konstantoulas, I.; Dritsas, E.; Moustakas, K. Sleep quality evaluation in rich information data. In Proceedings of the 2022 13th International Conference on Information, Intelligence, Systems & Applications (IISA), Corfu, Greece, 18–20 July 2022; pp. 1–4. [Google Scholar]
- Trigka, M.; Dritsas, E. Long-term coronary artery disease risk prediction with machine learning models. Sensors 2023, 23, 1193. [Google Scholar] [CrossRef] [PubMed]
- Dritsas, E.; Alexiou, S.; Moustakas, K. COPD severity prediction in elderly with ML techniques. In Proceedings of the Proceedings of the 15th International Conference on PErvasive Technologies Related to Assistive Environments, Corfu, Greece, 15 February 2022; pp. 185–189. [Google Scholar]
- Singh, O.P.; Vallejo, M.; El-Badawy, I.M.; Aysha, A.; Madhanagopal, J.; Faudzi, A.A.M. Classification of SARS-CoV-2 and non-SARS-CoV-2 using machine learning algorithms. Comput. Biol. Med. 2021, 136, 104650. [Google Scholar] [CrossRef]
- Silva, G.F.; Fagundes, T.P.; Teixeira, B.C.; Chiavegatto Filho, A.D. Machine learning for hypertension prediction: A systematic review. Curr. Hypertens. Rep. 2022, 24, 523–533. [Google Scholar]
- Tavares, L.D.; Manoel, A.; Donato, T.H.R.; Cesena, F.; Minanni, C.A.; Kashiwagi, N.M.; da Silva, L.P.; Amaro, E., Jr.; Szlejf, C. Prediction of metabolic syndrome: A machine learning approach to help primary prevention. Diabetes Res. Clin. Pract. 2022, 191, 110047. [Google Scholar] [CrossRef]
- Amrane, M.; Oukid, S.; Gagaoua, I.; Ensari, T. Breast cancer classification using machine learning. In Proceedings of the 2018 electric electronics, computer science, biomedical engineerings’ meeting (EBBT), Istanbul, Turkey, 18–19 April 2018; pp. 1–4. [Google Scholar]
- Sirsat, M.S.; Fermé, E.; Camara, J. Machine learning for brain stroke: A review. J. Stroke Cerebrovasc. Dis. 2020, 29, 105162. [Google Scholar] [CrossRef]
- Garcia-d’Urso, N.; Climent-Pérez, P.; Sánchez-Sansegundo, M.; Zaragoza-Martí, A.; Fuster-Guilló, A.; Azorín-López, J. A non-invasive approach for total cholesterol level prediction using machine learning. IEEE Access 2022, 10, 58566–58577. [Google Scholar] [CrossRef]
- Schwartz, A.R.; Cohen-Zion, M.; Pham, L.V.; Gal, A.; Sowho, M.; Sgambati, F.P.; Klopfer, T.; Guzman, M.A.; Hawks, E.M.; Etzioni, T.; et al. Brief digital sleep questionnaire powered by machine learning prediction models identifies common sleep disorders. Sleep Med. 2020, 71, 66–76. [Google Scholar] [CrossRef]
- O’Mahony, A.M.; Garvey, J.F.; McNicholas, W.T. Technologic advances in the assessment and management of obstructive sleep apnoea beyond the apnoea-hypopnoea index: A narrative review. J. Thorac. Dis. 2020, 12, 5020. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.H.; Lech, M.; Wilkinson, R.H. Simultaneous Sleep Stage and Sleep Disorder Detection from Multimodal Sensors Using Deep Learning. Sensors 2023, 23, 3468. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.; Lesperance, M.L.; Zhang, X. Simultaneous prediction of multiple outcomes using revised stacking algorithms. Bioinformatics 2020, 36, 65–72. [Google Scholar]
- Kim, T.K. Understanding one-way ANOVA using conceptual figures. Korean J. Anesthesiol. 2017, 70, 22. [Google Scholar] [CrossRef]
- Kim, T.; Kim, J.W.; Lee, K. Detection of sleep disordered breathing severity using acoustic biomarker and machine learning techniques. Biomed. Eng. Online 2018, 17, 1–19. [Google Scholar] [CrossRef]
- Mencar, C.; Gallo, C.; Mantero, M.; Tarsia, P.; Carpagnano, G.E.; Foschino Barbaro, M.P.; Lacedonia, D. Application of machine learning to predict obstructive sleep apnea syndrome severity. Health Inform. J. 2020, 26, 298–317. [Google Scholar] [CrossRef]
- Rodrigues, J.F., Jr.; Pepin, J.L.; Goeuriot, L.; Amer-Yahia, S. An extensive investigation of machine learning techniques for sleep apnea screening. In Proceedings of the 29th ACM International Conference on Information & Knowledge Management, Virtual Event, 19–23 October 2020; pp. 2709–2716. [Google Scholar]
- Crivello, A.; Palumbo, F.; Barsocchi, P.; La Rosa, D.; Scarselli, F.; Bianchini, M. Understanding human sleep behaviour by machine learning. Cogn. Infocommun. Theory Appl. 2019, 227–252. [Google Scholar]
- Santaji, S.; Desai, V. Analysis of EEG signal to classify sleep stages using machine learning. Sleep Vigil. 2020, 4, 145–152. [Google Scholar] [CrossRef]
- Kristiansen, S.; Nikolaidis, K.; Plagemann, T.; Goebel, V.; Traaen, G.M.; Øverland, B.; Aakerøy, L.; Hunt, T.E.; Loennechen, J.P.; Steinshamn, S.L.; et al. Machine learning for sleep apnea detection with unattended sleep monitoring at home. ACM Trans. Comput. Healthc. 2021, 2, 1–25. [Google Scholar] [CrossRef]
- Sekkal, R.N.; Bereksi-Reguig, F.; Ruiz-Fernandez, D.; Dib, N.; Sekkal, S. Automatic sleep stage classification: From classical machine learning methods to deep learning. Biomed. Signal Process. Control 2022, 77, 103751. [Google Scholar] [CrossRef]
- Xu, S.; Faust, O.; Seoni, S.; Chakraborty, S.; Barua, P.D.; Loh, H.W.; Elphick, H.; Molinari, F.; Acharya, U.R. A review of automated sleep disorder detection. Comput. Biol. Med. 2022, 150, 106100. [Google Scholar] [CrossRef]
- Han, H.; Oh, J. Application of various machine learning techniques to predict obstructive sleep apnea syndrome severity. Sci. Rep. 2023, 13, 6379. [Google Scholar] [CrossRef]
- Cao, X.; Xing, L.; Majd, E.; He, H.; Gu, J.; Zhang, X. A systematic evaluation of supervised machine learning algorithms for cell phenotype classification using single-cell RNA sequencing data. Front. Genet. 2022, 13, 836798. [Google Scholar] [CrossRef]
- Casal-Guisande, M.; Torres-Durán, M.; Mosteiro-Añón, M.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.B.; Fernández-Villar, A.; Comesaña-Campos, A. Design and conceptual proposal of an intelligent clinical decision support system for the diagnosis of suspicious obstructive sleep apnea patients from health profile. Int. J. Environ. Res. Public Health 2023, 20, 3627. [Google Scholar] [CrossRef] [PubMed]
- Casal-Guisande, M.; Ceide-Sandoval, L.; Mosteiro-Añón, M.; Torres-Durán, M.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.B.; Fernández-Villar, A.; Comesaña-Campos, A. Design of an Intelligent Decision Support System Applied to the Diagnosis of Obstructive Sleep Apnea. Diagnostics 2023, 13, 1854. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.; George, T.; Brewster, G.S. Insomnia in older adults. Curr. Geriatr. Rep. 2019, 8, 271–290. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zhang, J.; Yan, H.; Li, Q. Multi-class imbalanced learning with one-versus-one decomposition: An empirical study. In Proceedings of the Cloud Computing and Security: 4th International Conference, ICCCS 2018, Haikou, China, 8–10 June 2018; Revised Selected Papers, Part III 4. Springer: Berlin/Heidelberg, Germany, 2018; pp. 617–628. [Google Scholar]
- Dimitriadis, S.I.; Liparas, D.; Tsolaki, M.N.; Alzheimer’s Disease Neuroimaging Initiative. Random forest feature selection, fusion and ensemble strategy: Combining multiple morphological MRI measures to discriminate among healhy elderly, MCI, cMCI and alzheimer’s disease patients: From the alzheimer’s disease neuroimaging initiative (ADNI) database. J. Neurosci. Methods 2018, 302, 14–23. [Google Scholar]
- Tangirala, S. Evaluating the impact of GINI index and information gain on classification using decision tree classifier algorithm. Int. J. Adv. Comput. Sci. Appl. 2020, 11, 612–619. [Google Scholar] [CrossRef]
- Haixiang, G.; Yijing, L.; Shang, J.; Mingyun, G.; Yuanyue, H.; Bing, G. Learning from class-imbalanced data: Review of methods and applications. Expert Syst. Appl. 2017, 73, 220–239. [Google Scholar] [CrossRef]
- Zhang, Z.L.; Luo, X.G.; Garcia, S.; Tang, J.F.; Herrera, F. Exploring the effectiveness of dynamic ensemble selection in the one-versus-one scheme. Knowl.-Based Syst. 2017, 125, 53–63. [Google Scholar] [CrossRef]
- Tharwat, A. Parameter investigation of support vector machine classifier with kernel functions. Knowl. Inf. Syst. 2019, 61, 1269–1302. [Google Scholar] [CrossRef]
- Bisong, E.; Bisong, E. Logistic regression. In Building Machine Learning and Deep Learning Models on Google Cloud Platform: A Comprehensive Guide for Beginners; Apress: Berkeley, CA, USA, 2019; pp. 243–250. [Google Scholar]
- Kautz, T.; Eskofier, B.M.; Pasluosta, C.F. Generic performance measure for multiclass-classifiers. Pattern Recognit. 2017, 68, 111–125. [Google Scholar] [CrossRef]
- Wardhani, N.W.S.; Rochayani, M.Y.; Iriany, A.; Sulistyono, A.D.; Lestantyo, P. Cross-validation metrics for evaluating classification performance on imbalanced data. In Proceedings of the 2019 International Conference on Computer, Control, Informatics and its Applications (IC3INA), Tangerang, Indonesia, 23–24 October 2019; pp. 14–18. [Google Scholar]
- Waikato Environment for Knowledge Analysis. Available online: https://www.weka.io/ (accessed on 4 July 2024).
- Chacón-Maldonado, A.M.; Asencio-Cortés, G.; Martínez-Álvarez, F.; Troncoso, A. FS-Studio: An extensive and efficient feature selection experimentation tool for Weka Explorer. SoftwareX 2023, 23, 101401. [Google Scholar]
- De Diego, I.M.; Redondo, A.R.; Fernández, R.R.; Navarro, J.; Moguerza, J.M. General Performance Score for classification problems. Appl. Intell. 2022, 52, 12049–12063. [Google Scholar]
- Trigka, M.; Dritsas, E.; Fidas, C. A Survey on Signal Processing Methods for EEG-based Brain Computer Interface Systems. In Proceedings of the 26th Pan-Hellenic Conference on Informatics, Athens, Greece, 25–27 November 2022; pp. 213–218. [Google Scholar]
- Kirac, D.; Akcay, T.; Ulucan, K. Genetics of Sleep and Sleep Disorders; Elsevier: Amsterdam, The Netherlands, 2020; pp. 49–54. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± Stdv | Min–Max | |
|---|---|---|
| Age | 42.18 ± 8.67 | 27–59 |
| SysBP | 128.58 ± 7.75 | 115–142 |
| DiasBP | 84.14 ± 5.66 | 75–95 |
| HeartRate | 71.71 ± 6.25 | 65–95 |
| Steps | 4224.59 ± 2905.87 | 500–10,000 |
| Sleep Duration | 7.13 ± 0.77 | 5.8–8.5 |
| Physical Activity | 39.73 ± 30.30 | 0–90 |
| Normal | Sleep Apnea | Insomnia | |||||
|---|---|---|---|---|---|---|---|
| Mean | Variance | Mean | Variance | Mean | Variance | p-Value | |
| Age | 39.04 | 61.27 | 43.52 | 23.12 | 49.71 | 80.83 | 8.85 |
| SysBP | 124.05 | 32.29 | 137.77 | 26.44 | 132.17 | 14.93 | 4.45 |
| DiasBP | 80.91 | 14.27 | 90.54 | 24.75 | 86.86 | 11.41 | 1.08 |
| HeartRate | 69.29 | 11.32 | 78.92 | 48.59 | 71.27 | 39.59 | 1.21 |
| Daily Steps | 5550.23 | 7,488,291.23 | 2378.21 | 4,832,375.96 | 2324.68 | 2,847,146.28 | 0 |
| Sleep Duration | 7.36 | 0.536 | 7.03 | 0.950 | 6.59 | 0.149 | 7.16 |
| Physical Activity | 50.59 | 927.86 | 26.15 | 534.36 | 22.59 | 477.37 | 4.75 |
| Pooled Variance | Pair 1 | Pair 2 | Pair 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AbsDiff | Significance | AbsDiff | Significance | AbsDiff | Significance | |||||
| Age | 57.52 | 10.67 | 1.706 | Yes | 4.48 | 2.858 | Yes | 7.16 | 2.877 | Yes |
| SysBP | 27.87 | 13.72 | 1.119 | Yes | 8.12 | 1.989 | Yes | 5.6 | 2.003 | Yes |
| DiasBP | 15.86 | 9.63 | 0.896 | Yes | 5.95 | 1.500 | Yes | 3.68 | 1.511 | Yes |
| HeartRate | 24.85 | 9.64 | 1.121 | Yes | 1.99 | 1.879 | Yes | 7.65 | 1.891 | Yes |
| Daily Steps | 5,986,316.86 | 3172.02 | 550.39 | Yes | 3225.55 | 922.26 | Yes | 53.53 | 928.21 | No |
| Sleep Duration | 0.5430 | 0.33 | 0.166 | Yes | 0.77 | 0.278 | Yes | 0.44 | 0.279 | Yes |
| Physical Activity | 753.907 | 24.44 | 6.17 | Yes | 28 | 10.35 | Yes | 3.56 | 10.42 | Yes |
| Attribute | Frequency per Category |
|---|---|
| Gender | Male (189), Female (185) |
| Occupation | Accountant (37), Doctor (29), Engineer (52), Lawyer (47), Manager (34), Nurse (35) Sales Representative (19), Teacher (40), Salesperson (32), Scientist (19), Software Engineer (30) |
| BMI Category | Normal (216), Overweight (148), Obese (10) |
| Asthma | Yes (32), No (342) |
| QoSleep | 4 (5), 5 (7), 6 (105), 7 (77), 8 (109), 9 (71) |
| Stress Level | 3 (71), 4 (70), 5 (67), 6 (46), 7 (50), 8 (70) |
| Base Models | Parameters |
|---|---|
| LR | ridge = useConjugateGradientDescent: False |
| Linear SVM | SVMType = C-SVC Classification kernelType = linear loss = 0.1 |
| Poly-SVM | SVMType = C-SVC Classification kernelType = Polynomial , = 1, loss = 0.1 |
| OVA LR | Precision | Recall | F-measure | AUC | OVO LR | Precision | Recall | F-measure | AUC | Class |
| 0.936 | 0.936 | 0.936 | 0.927 | 0.927 | 0.932 | 0.929 | 0.910 | Normal | ||
| 0.835 | 0.846 | 0.841 | 0.912 | 0.840 | 0.808 | 0.824 | 0.900 | Sleep Apnea | ||
| 0.829 | 0.818 | 0.824 | 0.905 | 0.785 | 0.805 | 0.795 | 0.893 | Insomnia | ||
| WAvg. | 0.893 | 0.893 | 0.893 | 0.919 | WAvg. | 0.880 | 0.880 | 0.880 | 0.905 | |
| OVA Linear SVM | Precision | Recall | F-measure | AUC | OVO Linear SVM | Precision | Recall | F-measure | AUC | Class |
| 0.921 | 0.959 | 0.940 | 0.939 | 0.945 | 0.945 | 0.945 | 0.931 | Normal | ||
| 0.865 | 0.821 | 0.842 | 0.910 | 0.848 | 0.859 | 0.854 | 0.935 | Sleep Apnea | ||
| 0.861 | 0.805 | 0.832 | 0.903 | 0.842 | 0.831 | 0.837 | 0.918 | Insomnia | ||
| WAvg. | 0.897 | 0.898 | 0.897 | 0.925 | WAvg. | 0.904 | 0.904 | 0.904 | 0.929 | |
| OVA Poly SVM | Precision | Recall | F-measure | AUC | OVO Poly SVM | Precision | Recall | F-measure | AUC | Class |
| 0.932 | 0.941 | 0.936 | 0.934 | 0.945 | 0.941 | 0.943 | 0.926 | Normal | ||
| 0.864 | 0.897 | 0.881 | 0.942 | 0.855 | 0.910 | 0.882 | 0.951 | Sleep Apnea | ||
| 0.889 | 0.831 | 0.859 | 0.914 | 0.890 | 0.844 | 0.867 | 0.916 | Insomnia | ||
| WAvg. | 0.909 | 0.909 | 0.909 | 0.931 | WAvg. | 0.915 | 0.914 | 0.914 | 0.930 |
| OVA LR | Precision | Recall | F-measure | AUC | OVO LR | Precision | Recall | F-measure | AUC | Class |
| 0.941 | 0.945 | 0.943 | 0.930 | 0.940 | 0.932 | 0.936 | 0.920 | Normal | ||
| 0.831 | 0.885 | 0.857 | 0.921 | 0.817 | 0.859 | 0.837 | 0.898 | Sleep Apnea | ||
| 0.873 | 0.805 | 0.838 | 0.928 | 0.840 | 0.818 | 0.829 | 0.902 | Insomnia | ||
| WAvg. | 0.904 | 0.904 | 0.903 | 0.928 | WAvg. | 0.894 | 0.893 | 0.893 | 0.912 | |
| OVA Linear SVM | Precision | Recall | F-measure | AUC | OVO Linear SVM | Precision | Recall | F-measure | AUC | Class |
| 0.921 | 0.959 | 0.940 | 0.943 | 0.945 | 0.950 | 0.948 | 0.934 | Normal | ||
| 0.867 | 0.833 | 0.850 | 0.912 | 0.846 | 0.846 | 0.846 | 0.932 | Sleep Apnea | ||
| 0.859 | 0.792 | 0.824 | 0.916 | 0.842 | 0.831 | 0.837 | 0.929 | Insomnia | ||
| WAvg. | 0.897 | 0.898 | 0.897 | 0.931 | WAvg. | 0.903 | 0.904 | 0.904 | 0.933 | |
| OVA Poly SVM | Precision | Recall | F-measure | AUC | OVO Poly SVM | Precision | Recall | F-measure | AUC | Class |
| 0.946 | 0.954 | 0.950 | 0.938 | 0.946 | 0.954 | 0.950 | 0.928 | Normal | ||
| 0.852 | 0.885 | 0.868 | 0.922 | 0.852 | 0.885 | 0.868 | 0.936 | Sleep Apnea | ||
| 0.889 | 0.831 | 0.859 | 0.902 | 0.889 | 0.831 | 0.859 | 0.914 | Insomnia | ||
| WAvg. | 0.914 | 0.914 | 0.914 | 0.928 | WAvg. | 0.914 | 0.914 | 0.914 | 0.927 |
| All Features | Poly SVM-OVO | Poly SVM-OVA | Lin SVM-OVO | Lin SVM-OVA | LR-OVA | LR-OVO |
| K (%) | 85.05 | 84.03 | 83.15 | 81.93 | 81.28 | 78.90 |
| Accuracy (%) | 91.44 | 90.91 | 90.37 | 89.84 | 89.37 | 87.97 |
| Selected Features | Poly SVM-OVO | Poly SVM-OVA | LR-OVA | Lin SVM-OVO | Lin SVM-OVA | LR-OVO |
| K (%) | 84.97 | 84.97 | 83.12 | 83.12 | 81.92 | 81.34 |
| Accuracy (%) | 91.44 | 91.44 | 90.37 | 90.37 | 89.84 | 89.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dritsas, E.; Trigka, M. Utilizing Multi-Class Classification Methods for Automated Sleep Disorder Prediction. Information 2024, 15, 426. https://doi.org/10.3390/info15080426
Dritsas E, Trigka M. Utilizing Multi-Class Classification Methods for Automated Sleep Disorder Prediction. Information. 2024; 15(8):426. https://doi.org/10.3390/info15080426
Chicago/Turabian StyleDritsas, Elias, and Maria Trigka. 2024. "Utilizing Multi-Class Classification Methods for Automated Sleep Disorder Prediction" Information 15, no. 8: 426. https://doi.org/10.3390/info15080426
APA StyleDritsas, E., & Trigka, M. (2024). Utilizing Multi-Class Classification Methods for Automated Sleep Disorder Prediction. Information, 15(8), 426. https://doi.org/10.3390/info15080426