
The Use of Premixed Calcium Silicate Bioceramic Sealer with Warm Carrier-Based Technique: A 2-Year Study for Patients Treated in a Master Program

 ,
,  ,
, 
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
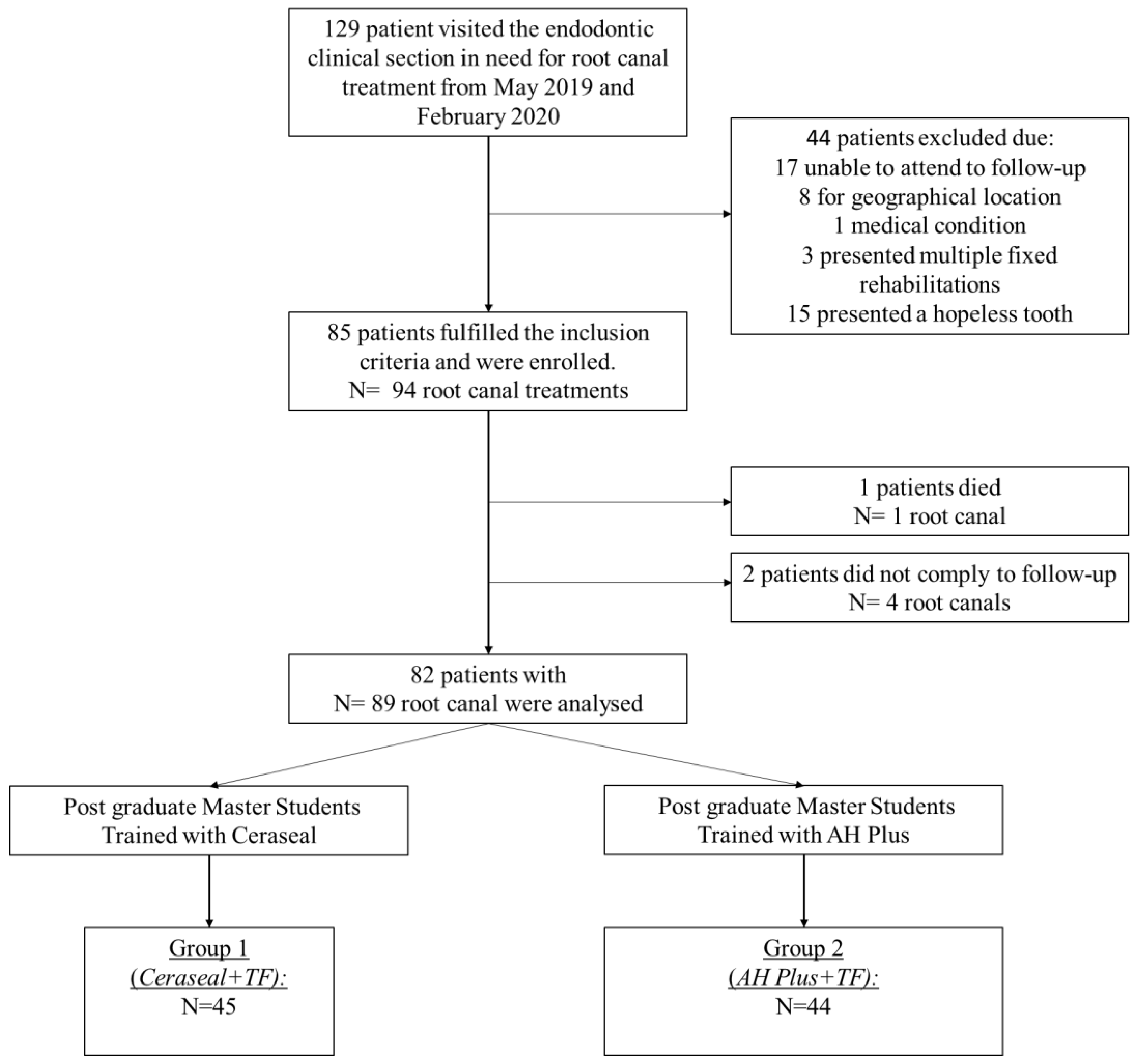
2.1. Study Design and Sample
2.2. Sample Size
2.3. Root Canal Treatment Procedures
2.4. Root Canal Filling Techniques and Filling Group Constitution
2.5. Tooth Restoration
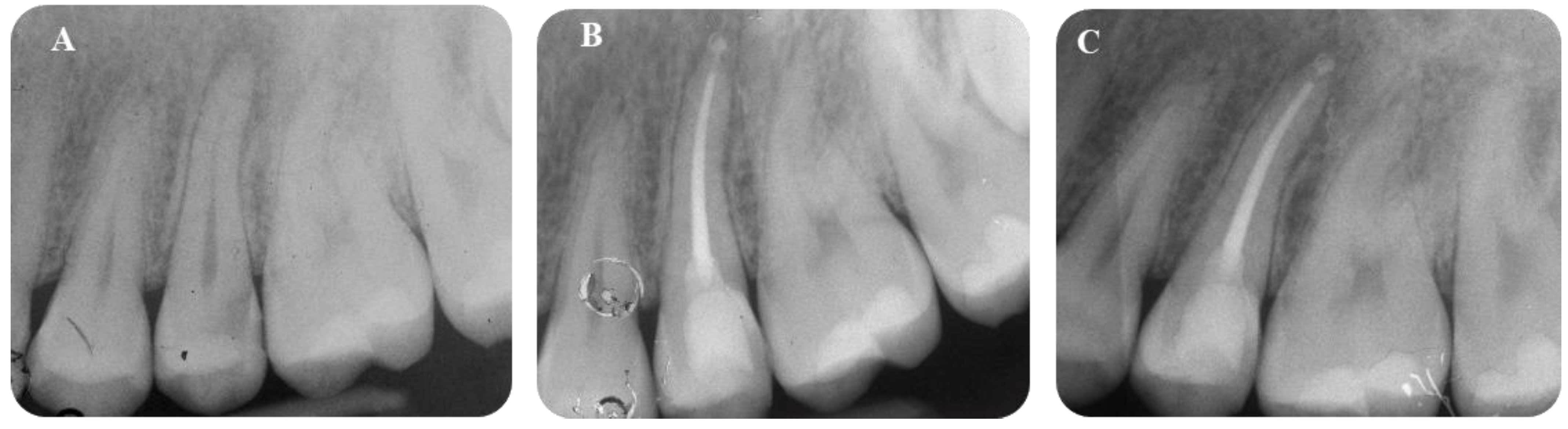
2.6. Radiological Evaluation
2.7. Definition of Success and Survival Criteria
2.8. Statistical Analysis
3. Results
3.1. Demographic Information
3.2. Outcome Measures
3.3. Sealer Extrusion and Sealer Resorption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Torabiinejad, M.; Chivian, N. Clinical applications of mineral trioxide aggregate. J. Endod. 1999, 25, 197–205. [Google Scholar] [CrossRef]
- Pitt-Ford, T.R.; Torabinejad, M.; McKendry, D.J.; Hong, C.U.; Kariyawasam, S.P. Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1995, 79, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Niu, L.N.; Jiao, K.; Wang, T.D.; Zhang, W.; Camilleri, J.; Bergeron, B.E.; Feng, H.L.; Mao, J.; Chen, J.H.; Pashley, D.H.; et al. A review of the bioactivity of hydraulic calcium silicate cements. J. Dent. Res. 2014, 42, 517–533. [Google Scholar] [CrossRef] [Green Version]
- Primus, C.M.; Tay, F.R.; Niu, L.N. Bioactive tri/dicalcium silicate cements for treatment of pulpal and periapical tissues. Acta Biomater. 2019, 96, 35–54. [Google Scholar] [CrossRef] [PubMed]
- Angerame, D.; De Biasi, M.; Pecci, R.; Bedini, R. Filling ability of three variants of the single-cone technique with bioceramic sealer: A micro-computed tomography study. J. Mater. Sci. Mater. Med. 2020, 31, 91–99. [Google Scholar] [CrossRef]
- Tanomaru-Filho, M.; Andrade, A.S.; Rodrigues, E.M.; Viola, K.S.; Faria, G.; Camilleri, J.; Guerreiro-Tanomaru, J.M. Biocompatibility and mineralized nodule formation of Neo MTA Plus and an experimental tricalcium silicate cement containing tantalum oxide. Int. Endod. J. 2017, 50, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Zamparini, F.; Siboni, F.; Prati, C.; Taddei, P.; Gandolfi, M.G. Properties of calcium silicate-monobasic calcium phosphate materials for endodontics containing tantalum pentoxide and zirconium oxide. Clin. Oral Investig. 2019, 23, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Giacomino, C.M.; Wealleans, J.A.; Kuhn, N.; Diogenes, A. Comparative Biocompatibility and Osteogenic Potential of Two Bioceramic Sealers. J. Endod. 2019, 45, 51–56. [Google Scholar] [CrossRef] [PubMed]
- López-García, S.; Myong-Hyun, B.; Lozano, A.; García-Bernal, D.; Forner, L.; Llena, C.; Guerrero-Gironés, J.; Murcia, L.; Rodríguez-Lozano, F.J. Cytocompatibility, bioactivity potential, and ion release of three premixed calcium silicate-based sealers. Clin. Oral Investig. 2020, 24, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Hadis, M.; Camilleri, J. Characterization of heat resistant hydraulic sealer for warm vertical obturation. Dent. Mater. 2020, 36, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Zamparini, F.; Prati, C.; Taddei, P.; Spinelli, A.; Di Foggia, M.; Gandolfi, M.G. Chemical-Physical Properties and Bioactivity of New Premixed Calcium Silicate-Bioceramic Root Canal Sealers. Int. J. Mol. Sci. 2020, 23, 13914. [Google Scholar] [CrossRef] [PubMed]
- Kharouf, N.; Arntz, Y.; Eid, A.; Zghal, J.; Sauro, S.; Haikel, Y.; Mancino, D. Physicochemical and Antibacterial Properties of Novel, Premixed Calcium Silicate-Based Sealer Compared to Powder-Liquid Bioceramic Sealer. J. Clin. Med. 2020, 9, 3096. [Google Scholar] [CrossRef]
- Goldberg, F.; Artaza, L.P.; De Silvio, A. Effectiveness of different obturation techniques in the filling of simulated lateral canals. J. Endod. 2001, 27, 362–364. [Google Scholar] [CrossRef] [PubMed]
- Mirfendereski, M.; Roth, K.; Bing, F.; Dubrowski, A.; Carnahan, H.; Azarpazhooh, A.; Basrani, B.; Torneck, C.D.; Friedman, S. Technique acquisition in the use of two thermoplasticized root filling methods by inexperienced dental students: A micro-CT analysis. J. Endod. 2009, 35, 1512–1517. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Zamparini, F.; Peters, O.A.; Iacono, F.; Gatto, M.R.; Generali, L.; Gandolfi, M.G.; Prati, C. The fate of root canals obturated with Thermafil: 10-year data for patients treated in a master program. Clin. Oral Investig. 2019, 23, 3367–3377. [Google Scholar] [CrossRef] [PubMed]
- Hale, R.; Gatti, R.; Glickman, G.N.; Opperman, L.A. Comparative analysis of carrier-based obturation and lateral compaction: A retrospective clinical outcomes study. Int. J. Dent. 2012, 2012, 954675. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.W.Y.; Tsang, C.S.C.; Zhang, S.; Li, S.K.Y.; Zhang, C.; Chu, C.H. Treatment outcomes of single-visit versus multiple-visit non-surgical endodontic therapy: A randomised clinical trial. BMC Oral Health 2015, 15, 162. [Google Scholar] [CrossRef] [Green Version]
- Demirci, G.K.; Caliskan, M.K. A prospective randomized comparative study of cold lateral condensation versus Core/Gutta-percha in teeth with periapical lesions. J. Endod. 2016, 42, 206–210. [Google Scholar] [CrossRef]
- Chu, C.H.; Lo, E.C.; Cheung, G.S. Outcome of root canal treatment using Thermafil and cold lateral condensation filling techniques. Int. Endod. J. 2005, 38, 179–185. [Google Scholar] [CrossRef]
- Chybowski, E.A.; Glickman, G.N.; Patel, Y.; Fleury, A.; Solomon, E.; He, J. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-cone Technique with Endosequence Bioceramic Sealer: A Retrospective Analysis. J. Endod. 2018, 44, 941–945. [Google Scholar] [CrossRef]
- Zavattini, A.; Knight, A.; Foschi, F.; Mannocci, F. Outcome of root canal treatments using a new calcium silicate root canal sealer: A non-randomized clinical trial. J. Clin. Med. 2020, 9, 782. [Google Scholar] [CrossRef] [Green Version]
- Bardini, G.; Casula, L.; Ambu, E.; Musu, D.; Mercadè, M.; Cotti, E. A 12-month follow-up of primary and secondary root canal treatment in teeth obturated with a hydraulic sealer. Clin. Oral Investig. 2021, 25, 2757–2764. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [Green Version]
- Dodson, T.B. A guide for preparing a patient-oriented research manuscript. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 307–315. [Google Scholar] [CrossRef]
- Prati, C.; Pirani, C.; Zamparini, F.; Gatto, M.R.; Gandolfi, M.G. A 20-year historical prospective cohort study of root canal treatments. A Multilevel analysis. Int. Endod. J. 2018, 51, 955–968. [Google Scholar] [CrossRef] [PubMed]
- Zamparini, F.; Pelliccioni, G.A.; Spinelli, A.; Gissi, D.B.; Gandolfi, M.G.; Prati, C. Root canal treatment of compromised teeth as alternative treatment for patients receiving bisphosphonates: 60-month results of a prospective clinical study. Int. Endod. J. 2021, 54, 156–171. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Cirulli, P.P.; Chersoni, S.; Micele, L.; Ruggeri, O.; Prati, C. Cyclic fatigue testing and metallographic analysis of nickel-titanium rotary instruments. J. Endod. 2011, 37, 1013–1016. [Google Scholar] [CrossRef]
- Chong, B.S.; Ford, T.R.P. The role of intracanal medication in root canal treatment. Int. Endod. J. 1992, 25, 97–106. [Google Scholar] [CrossRef]
- Pirani, C.; Paolucci, A.; Ruggeri, O.; Bossù, M.; Polimeni, A.; Gatto, M.R.; Gandolfi, M.G.; Prati, C. Wear and metallographic analysis of WaveOne and reciproc NiTi instruments before and after three uses in root canals. Scanning. 2014, 36, 517–525. [Google Scholar] [CrossRef]
- Ørstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Taddei, P.; Modena, E.; Siboni, F.; Prati, C. Biointeractivity-related versus chemi/physisorption-related apatite precursor-forming ability of current root end filling materials. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 1107–1123. [Google Scholar] [CrossRef]
- Rashid, F.; Shiba, H.; Mizuno, N.; Mouri, Y.; Fujita, T.; Shinohara, H.; Ogawa, T.; Kawaguchi, H.; Kurihara, H. The effect of extracellular calcium ion on gene expression of bone-related proteins inhuman pulp cells. J. Endod. 2003, 29, 104–107. [Google Scholar] [CrossRef]
- Sun, J.; Wei, L.; Liu, X.; Li, J.; Li, B.; Wang, G.; Meng, F. Influences of ionic dissolution products of dicalcium silicate coating on osteoblastic proliferation, differentiation and gene expression. Acta Biomater. 2009, 5, 1284–1293. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Iacono, F.; Agee, K.; Siboni, F.; Tay, F.; Pashley, D.H.; Prati, C. Setting time and expansion in different soaking media of experimental accelerated calcium-silicate cements and ProRoot MTA. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Iacono, F.; Gandolfi, M.G.; Huffman, B.; Sword, J.; Agee, K.; Siboni, F.; Tay, F.; Prati, C.; Pashley, D. Push-out strength of modified Portland cements and resins. Am. J. Dent. 2010, 23, 43–46. [Google Scholar]
- Gandolfi, M.G.; Taddei, P.; Siboni, F.; Modena, E.; Ginebra, M.P.; Prati, C. Fluoride-containing nanoporous calcium-silicate MTA cements for endodontics and oral surgery: Early fluorapatite formation in a phosphate-containing solution. Int. Endod. J. 2011, 44, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Pashley, D.H.; Rueggeberg, F.A.; Loushine, R.J.; Weller, R.N. Calcium phosphate phase transformation produced by the interaction of the portland cement component of white mineral trioxide aggregate with a phosphate-containing fluid. J. Endod. 2007, 33, 1347–1351. [Google Scholar] [CrossRef]
- Taddei, P.; Tinti, A.; Gandolfi, M.G.; Rossi, P.L.; Prati, C. Vibrational study on the bioactivity of Portland cement-based materials for endodontic use. J. Mol. Struct. 2009, 924, 548–554. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Taddei, P.; Tinti, A.; De Stefano Dorigo, E.; Prati, C. Alpha-TCP improves the apatite-formation ability of calcium-silicate hydraulic cement soaked in phosphate solutions. Mater. Sci. Eng. C 2011, 31, 1412–1422. [Google Scholar] [CrossRef]
- Han, L.; Kodama, S.; Okiji, T. Evaluation of calcium-releasing and apatite-forming abilities of fast-setting calcium silicate-based endodontic materials. Int. Endod. J. 2015, 48, 124–130. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, F.J.; López-García, S.; García-Bernal, D.; Tomás-Catalá, C.J.; Santos, J.M.; Llena, C.; Lozano, A.; Murcia, L.; Forner, L. Chemical composition and bioactivity potential of the new Endosequence BC Sealer formulation HiFlow. Int. Endod. J. 2020, 53, 1216–1228. [Google Scholar] [CrossRef]
- Hakki, S.S.; Bozkurt, B.S.; Ozcopur, B.; Gandolfi, M.G.; Prati, C.; Belli, S. The response of cementoblasts to calcium phosphate resin-based and calcium silicate-based commercial sealers. Int. Endod. J. 2013, 46, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Shah, S.N.; Feng, R.; Prati, C.; Akintoye, S.O. Biomimetic calcium-silicate cements support differentiation of human orofacial mesenchymal stem cells. J. Endod. 2011, 37, 1102–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandolfi, M.G.; Iezzi, G.; Piattelli, A.; Prati, C.; Scarano, A. Osteoinductive potential and bone-bonding ability of ProRoot MTA, MTA Plus and Biodentine in rabbit intramedullary model: Microchemical characterization and histological analysis. Dent. Mater. 2017, 33, 221–238. [Google Scholar] [CrossRef]
- Pirani, C.; Friedman, S.; Gatto, M.R.; Iacono, F.; Tinarelli, V.; Gandolfi, M.G.; Prati, C. Survival and periapical health after root canal treatment with carrier-based root fillings: Five-year retrospective assessment. Int. Endod. J. 2018, 51, 178–188. [Google Scholar] [CrossRef] [Green Version]
- Atmeh, A.R.; AlShwaimi, E. The Effect of Heating Time and Temperature on Epoxy Resin and Calcium Silicate-based Endodontic Sealers. J. Endod. 2017, 43, 2112–2118. [Google Scholar] [CrossRef]
- Yamauchi, S.; Watanabe, S.; Okiji, T. Effects of heating on the physical properties of premixed calcium silicate-based root canal sealers. J. Oral Sci. 2020, 63, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Antunes, T.B.M.; Janini, A.C.P.; Pelepenko, L.E.; Abuna, G.F.; Paiva, E.M.; Sinhoreti, M.A.C.; Raimundo, I.M., Jr.; Gomes, B.P.F.A.; de-Jesus-Soares, A.; Marciano, M.A. Heating stability, physical and chemical analysis of calcium silicate-based endodontic sealers. Int. Endod. J. 2021, 54, 1175–1188. [Google Scholar] [CrossRef]
- Donnermeyer, D.; Schäfer, E.; Bürklein, S. Real-time Intracanal Temperature Measurement during Different Obturation Techniques. J. Endod. 2018, 44, 1832–1836. [Google Scholar] [CrossRef] [PubMed]
- Generali, L.; Cavani, F.; Serena, V.; Pettenati, C.; Righi, E.; Bertoldi, C. Effect of Different Irrigation Systems on Sealer Penetration into Dentinal Tubules. J. Endod. 2017, 43, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Kwak, S.W.; Ha, J.H.; Lee, W.; Kim, H.C. Physicochemical Properties of Epoxy Resin-Based and Bioceramic-Based Root Canal Sealers. Bioinorg. Chem. Appl. 2017, 2017, 2582849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siboni, F.; Taddei, P.; Zamparini, F.; Prati, C.; Gandolfi, M.G. Properties of BioRoot RCS, a tricalcium silicate endodontic sealer modified with povidone and polycarboxylate. Int. Endod. J. 2017, 50, 120–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricucci, D.; Rôças, I.N.; Alves, F.R.; Loghin, S.; Siqueira, J.F., Jr. Apically Extruded Sealers: Fate and Influence on Treatment Outcome. J. Endod. 2016, 42, 243–249. [Google Scholar] [CrossRef]
- Goldberg, F.; Cantarini, C.; Alfie, D.; Macchi, R.L.; Arias, A. Relationship between unintentional canal overfilling and the long-term outcome of primary root canal treatments and nonsurgical retreatments: A retrospective radiographic assessment. Int. Endod. J. 2020, 53, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, B.; Coelho, M.S.; Bueno, C.E.D.S.; Fontana, C.E.; Martin, A.S.; Rocha, D.G.P. Assessment of Extrusion and Postoperative Pain of a Bioceramic and Resin-Based Root Canal Sealer. Eur. J. Dent. 2019, 3, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Schaeffer, M.A.; White, R.R.; Walton, R.E. Determining the optimal obturation length: A meta-analysis of literature. J. Endod. 2005, 31, 271–274. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Kulild, J.C. The impact of sealer extrusion on endodontic outcome: A systematic review with meta-analysis. Aust. Endod. J. 2020, 46, 123–129. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Ciapetti, G.; Perut, F.; Taddei, P.; Modena, E.; Rossi, P.L.; Prati, C. Biomimetic calcium-silicate cements aged in simulated body solutions. Osteoblast response and analyses of apatite coating. J. Appl. Biomater. Biomech. 2009, 7, 160–170. [Google Scholar]
- Elsayed, M.A.; Hassanien, E.E.; Elgendy, A.A.E. Ageing of TotalFill BC Sealer and MTA Fillapex in Simulated Body Fluid. Eur. Endod. J. 2021, 6, 183–188. [Google Scholar]
- Prati, C.; Gandolfi, M.G. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef]
- Reyes-Carmona, J.F.; Santos, A.R.; Figueiredo, C.P.; Felippe, M.S.; Felippe, W.T.; Cordeiro, M.M. In vivo host interactions with mineral trioxide aggregate and calcium hydroxide: Inflammatory molecular signaling assessment. J. Endod. 2011, 37, 1225–1235. [Google Scholar] [CrossRef]
- Jung, S.; Sielker, S.; Hanisch, M.R.; Libricht, V.; Schäfer, E.; Dammaschke, T. Cytotoxic effects of four different root canal sealers on human osteoblasts. PLoS ONE 2018, 13, e0194467. [Google Scholar] [CrossRef] [Green Version]
- Siboni, F.; Taddei, P.; Prati, C.; Gandolfi, M.G. Properties of NeoMTA Plus and MTA Plus cements for endodontics. Int. Endod. J. 2017, 50, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razdan, A.; Benetti, A.R.; Bjørndal, L. Do in vitro solubility studies on endodontic sealers demonstrate a high level of evidence? A systematic review. Acta Odontol. Scand. 2019, 77, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Hayashi, M.; Suzuki, Y.; Suzuki, N.; Maeno, M.; Ogiso, B. Calcium ions released from mineral trioxide aggregate convert the differentiation pathway of C2C12 Cells into osteoblast lineage. J. Endod. 2013, 39, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Gardin, C.; Zamparini, F.; Ferroni, L.; Esposti, M.D.; Parchi, G.; Ercan, B.; Manzoli, L.; Fava, F.; Fabbri, P.; et al. Mineral-Doped Poly(L-lactide) Acid Scaffolds Enriched with Exosomes Improve Osteogenic Commitment of Human Adipose-Derived Mesenchymal Stem Cells. Nanomaterials 2020, 10, 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandolfi, M.G.; Zamparini, F.; Esposti, M.D.; Chiellini, F.; Fava, F.; Fabbri, P.; Taddei, P.; Prati, C. Highly porous polycaprolactone scaffolds doped with calcium silicate and dicalcium phosphate dihydrate designed for bone regeneration. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 102, 341–361. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Taddei, P.; Pondrelli, A.; Zamparini, F.; Prati, C.; Spagnuolo, G. Demineralization, Collagen Modification and Remineralization Degree of Human Dentine after EDTA and Citric Acid Treatments. Materials 2019, 12, 25. [Google Scholar] [CrossRef] [Green Version]
- Tay, F.R.; Pashley, D.H. Guided tissue remineralisation of partially demineralised human dentine. Biomaterials 2008, 29, 1127–1137. [Google Scholar] [CrossRef]
- Tay, F.R.; Pashley, D.H. Biomimetic remineralization of resin-bonded acid-etched dentin. J. Dent. Res. 2009, 88, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Taddei, P.; Siboni, F.; Modena, E.; De Stefano, E.D.; Prati, C. Biomimetic remineralization of human dentin using promising innovative calcium-silicate hybrid “smart” materials. Dent. Mater. 2011, 27, 1055–1069. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Parrilli, A.P.; Fini, M.; Prati, C.; Dummer, P.M. 3D micro-CT analysis of the interface voids associated with Thermafil root fillings used with AH Plus or a flowable MTA sealer. Int. Endod. J. 2013, 46, 253–263. [Google Scholar] [CrossRef]
- Love, R.M.; Jenkinson, H.F. Invasion of dentinal tubules by oral bacteria. Crit. Rev. Oral Biol. Med. 2002, 13, 171–183. [Google Scholar] [CrossRef] [Green Version]
- Ricucci, D.; Siqueira, J.F., Jr. Biofilms and apical periodontitis: Study of prevalence and association with clinical and histopathologic findings. J. Endod. 2010, 36, 277–288. [Google Scholar] [CrossRef]
- Foschi, F.; Izard, J.; Sasaki, H.; Sambri, V.; Prati, C.; Müller, R.; Stashenko, P. Treponema denticola in disseminating endodontic infections. J. Dent. Res. 2006, 85, 761–765. [Google Scholar] [CrossRef] [Green Version]
- Buonavoglia, A.; Zamparini, F.; Lanave, G.; Pellegrini, F.; Diakoudi, G.; Spinelli, A.; Lucente, M.S.; Camero, M.; Vasinioti, V.I.; Gandolfi, M.G.; et al. Endodontic Microbial Communities in Apical Periodontitis. J. Endod. 2023, 49, 178–189. [Google Scholar] [CrossRef] [PubMed]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ✓ Aged 18–75 years |
| ✓ Healthy status (ASA 1 or 2) |
| ✓ No use of antiresorptive or antiangiogenic drug |
| ✓ Needing one or more root canal treatments |
| ✓ ASA > 3 |
| ✓ Lack of occlusal contacts |
| ✓ Heavy smoking (>15 cigarettes/day) |
| ✓ Pregnancy or breast feeding |
| ✓ Teeth with fewer than 2 walls of structural integrity |
| ✓ Any pathology that could compromise bone healing or the immune response |
| ✓ Malignant disease directly involving the jaws |
| ✓ Exposure to radiation therapy focused on the head and neck region |
| Parameters | Ceraseal-TF | AH Plus-TF | Chi Square Test | |
|---|---|---|---|---|
| Age | <30 30–55 >55 | 15 (33.3) 12 (26.6) 18 (40.0) | 7 (15.9) 19 (43.8) 18 (40.9) | Chi = 11.655 p = 0.020 |
| Gender | Males Females | 18 (40.0) 27 (60.0) | 20 (45.4) 24 (54.6) | Chi = 0.810 p = 0.667 |
| Tooth type | Incisors Canines Premolars Molars | 10 (22.2) 2 (4.4) 11 (24.4) 22 (48.8) | 4 (9.1) 2 (4.6) 10 (22.7) 28 (63.6) | Chi = 8.400 p = 0.078 |
| Tooth location | Maxilla Mandible | 27 (60.0) 18 (40.0) | 29 (65.9) 14 (31.8) | Chi = 5.05 p = 0.080 |
| Diagnosis | Prosthetic reasons Pulpitis Pulp Necrosis Re-exacerbated lesion | 3 (6.6) 15 (33.3) 18 (40.0) 9 (20.0) | 2 (4.6) 17 (38.6) 13 (29.5) 12 (27.2) | Chi = 15.672 p = 0.109 |
| Initial PAI | PAI ≤2 PAI ≥3 | 19 (44.2) 26 (55.8) | 21 (47.7) 23 (42.3) | Chi = 0.5332 p = 0.052 |
| Endodontic treatment | Primary root treatment Secondary treatment | 36 (80.0) 9 (20.0) | 32 (72.2) 12 (27.8) | Chi = 1.05 p = 0.608 |
| Obturation quality | Underfilled Adequate filling Overfilled | 2 (4.4) 38 (84.4) 5 (11.1) | 4 (9.1) 38 (86.3) 2 (4.6) | Chi = 3.287 p = 0.566 |
| Sealer extrusion | No Yes | 39 (86.6) 6 (13.4) | 33 (75.0) 11 (25.0) | Chi = 6.451 p = 0.040 |
| Long axis diameter of extrusion | 0 0.1–1.0 mm 1.1–3.0 mm >3.0 mm | 39 (84.4) 2 (4.4) 1 (2.2) 3 (6.6) | 33 (75.0) 3 (6.8) 6 (13.6) 2 (4.5) | Chi = 5.53 p = 0.477 |
| Definitive restoration | Composite Crown | 36 (80.0) 9 (20.0) | 37 (84.1) 7 (15.9) | Chi = 1.678 p = 0.416 |
| Total | 45 | 44 |
| n | Healed | Healing | Extracted | |
|---|---|---|---|---|
| Ceraseal-TF | 45 | 41 (91.1) | 3 (6.8) | 1 (2.3) |
| AH Plus-TF | 44 | 39 (88.6) | 4 (9.2) | 1 (2.2) |
| Parameters | Ceraseal-TF | AH Plus-TF | |||||
|---|---|---|---|---|---|---|---|
| n | Healed | Healing | n | Healed | Healing | ||
| Age | <30 | 15 | 15 (100) | 0 (0) | 7 | 7 (100%) | 0 (0) |
| 30–55 | 12 | 11 (91.6) | 1 (8.4) | 19 | 16 (84.2%) | 3 (15.8) | |
| >55 | 17 | 15 (88.2) | 2 (11.8) | 17 | 16 (94.1%) | 1 (5.9) | |
| Gender | Males | 17 | 16 (94.1) | 1 (5.9) | 19 | 18 (94.7%) | 1 (5.3) |
| Females | 27 | 25 (92.5) | 2 (7.5) | 24 | 21 (87.5%) | 3 (12.5) | |
| Tooth type | Incisors | 10 | 7 (70) | 3 (30) | 4 | 4 (100) | 0 (0) |
| Canine | 2 | 2 (100) | 0 (0) | 2 | 2 (100) | 0 (0) | |
| Premolars | 10 | 10 (100) | 0 (0) | 10 | 9 (90) | 1 (10) | |
| Molars | 22 | 22 (100) | 0 (0) | 27 | 24 (88.8) | 3 (11.2) | |
| Tooth location | Maxilla | 26 | 23 (88.4) | 3 (11.6) | 29 | 27 (93.1) | 2 (6.9) |
| Mandible | 18 | 18 (100) | 0 (0) | 13 | 11 (84.6) | 2 (15.4) | |
| Initial PAI | PAI ≤2 | 18 | 18 (100) | 0 (0) | 20 | 20 (100) | 0 (0) |
| PAI ≥3 | 26 | 23 (88.4) | 3 (11.6) | 23 | 19 (82.6) | 4 (17.4) | |
| Diagnosis | Prosthetic reasons | 3 | 3 (100) | 0 (0) | 2 | 2(100) | 0 (0) |
| Pulpitis | 14 | 14 (100) | 0 (0) | 16 | 16 (100) | 0 (0) | |
| Pulp necrosis | 18 | 18 (100) | 0 (0) | 13 | 12 (92.3) | 1 (7.7) | |
| Re-exacerbated lesion | 9 | 6 (66.6) | 3 (33.4) | 12 | 9 (75) | 3 (25) | |
| Endodontic treatment | Primary root treatment | 35 | 35 (100) | 0 (0) | 31 | 30 (96.7) | 1 (3.3) |
| Secondary treatment | 9 | 6 (66.6) | 3 (33.4) | 12 | 9 (75) | 3 (25) | |
| Obturation quality | Underfilled | 2 | 1 (50) | 1 (50) | 4 | 4 (100) | 0 (0) |
| Adequate | 37 | 37 (100) | 0 (0) | 37 | 34 (91.8) | 3 (8.2) | |
| Overfilled | 5 | 5 (100) | 0 (0) | 2 | 1 (50) | 1 (50) | |
| Extrusion | No | 38 | 37 (97.3) | 1 (6.7) | 32 | 29 (90.6) | 3 (9.4) |
| Yes | 6 | 4 (66.6) | 2 (33.4) | 11 | 10 (90.9) | 1 (9.1) | |
| Long axis diameter of extrusion | 0 | 38 | 37 (97.3) | 1 (2.7) | 32 | 29 (90.6) | 3 (9.4) |
| 0.1–1.0 mm | 2 | 2 (100) | 0 (0) | 3 | 3 (100) | 0 (0) | |
| 1.1–3.0 mm | 1 | 1 (100) | 0 (0) | 6 | 5 (83.3) | 1 (16.7) | |
| >3.0 mm | 3 | 1 (33.3) | 2 (66.7) | 2 | 2 (100) | 0 (0) | |
| Definitive restoration | Composite | 35 | 33 (94.2) | 2 (5.8) | 36 | 32 (88.8) | 4 (11.2) |
| Crown | 9 | 8 (88.8) | 1 (11.2) | 7 | 7 (100) | 0 (0) | |
| Parameters | Robust | 95% Confidence Interval | |||
|---|---|---|---|---|---|
| Coefficient | Standard Error | p Value | Lower Boundary | Upper Boundary | |
| Intercept | 1.488 | 0.201 | 0.000 | 1.0953 | 1.882 |
| Age | −0.934 | 0.582 | 0.108 | −2.075 | 0.206 |
| Gender | −1.125 | 1.036 | 0.277 | −3.156 | 0.905 |
| Tooth location | 0.643 | 0.542 | 0.235 | −0.418 | 1.706 |
| Diagnosis | 0.044 | 0.715 | 0.951 | −1.358 | 1.447 |
| Initial PAI | −0.134 | 0.047 | 0.005 | −0.228 | −0.040 |
| Endodontic treatment | −2.347 | 0.956 | 0.014 | −4.216 | −0.461 |
| Filling technique | 0.398 | 0.484 | 0.410 | −0.551 | 1.348 |
| Obturation quality | −1.60 | 0.917 | 0.081 | −3.39 | 0.197 |
| Sealer extrusion | 0.410 | 0.995 | 0.680 | −1.540 | 2.360 |
| Diameter of extrusion | −0.099 | 0.064 | 0.124 | −0.2271 | 0.027 |
| Definitive restoration | −0.609 | 0.435 | 0.162 | −1.463 | 0.244 |
| n | Stable | Resorbed | Total | |
|---|---|---|---|---|
| Ceraseal-TF | 45 | 3 (6.8) | 3 (6.8) | 6 (13.3) |
| AH Plus-TF | 44 | 11 (25) | 0 (0) | 11 (25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamparini, F.; Spinelli, A.; Cardinali, F.; Ausiello, P.; Gandolfi, M.G.; Prati, C. The Use of Premixed Calcium Silicate Bioceramic Sealer with Warm Carrier-Based Technique: A 2-Year Study for Patients Treated in a Master Program. J. Funct. Biomater. 2023, 14, 164. https://doi.org/10.3390/jfb14030164
Zamparini F, Spinelli A, Cardinali F, Ausiello P, Gandolfi MG, Prati C. The Use of Premixed Calcium Silicate Bioceramic Sealer with Warm Carrier-Based Technique: A 2-Year Study for Patients Treated in a Master Program. Journal of Functional Biomaterials. 2023; 14(3):164. https://doi.org/10.3390/jfb14030164
Chicago/Turabian StyleZamparini, Fausto, Andrea Spinelli, Filippo Cardinali, Pietro Ausiello, Maria Giovanna Gandolfi, and Carlo Prati. 2023. "The Use of Premixed Calcium Silicate Bioceramic Sealer with Warm Carrier-Based Technique: A 2-Year Study for Patients Treated in a Master Program" Journal of Functional Biomaterials 14, no. 3: 164. https://doi.org/10.3390/jfb14030164
APA StyleZamparini, F., Spinelli, A., Cardinali, F., Ausiello, P., Gandolfi, M. G., & Prati, C. (2023). The Use of Premixed Calcium Silicate Bioceramic Sealer with Warm Carrier-Based Technique: A 2-Year Study for Patients Treated in a Master Program. Journal of Functional Biomaterials, 14(3), 164. https://doi.org/10.3390/jfb14030164