
Biomaterial Material Applications in Postoperative Surgical Fields of Uvulopalatopharyngoplasty: A Comparative Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Participants and Baseline Data
2.3. Materials Used in the Surgical Field
2.3.1. Fibrin Tissue Glue
2.3.2. Polyglycolic Acid Sheet
2.3.3. PRP
2.4. Grouping of Patients
2.5. Data Parameters
2.6. Statistical Analysis
3. Results
3.1. Baseline Demographics
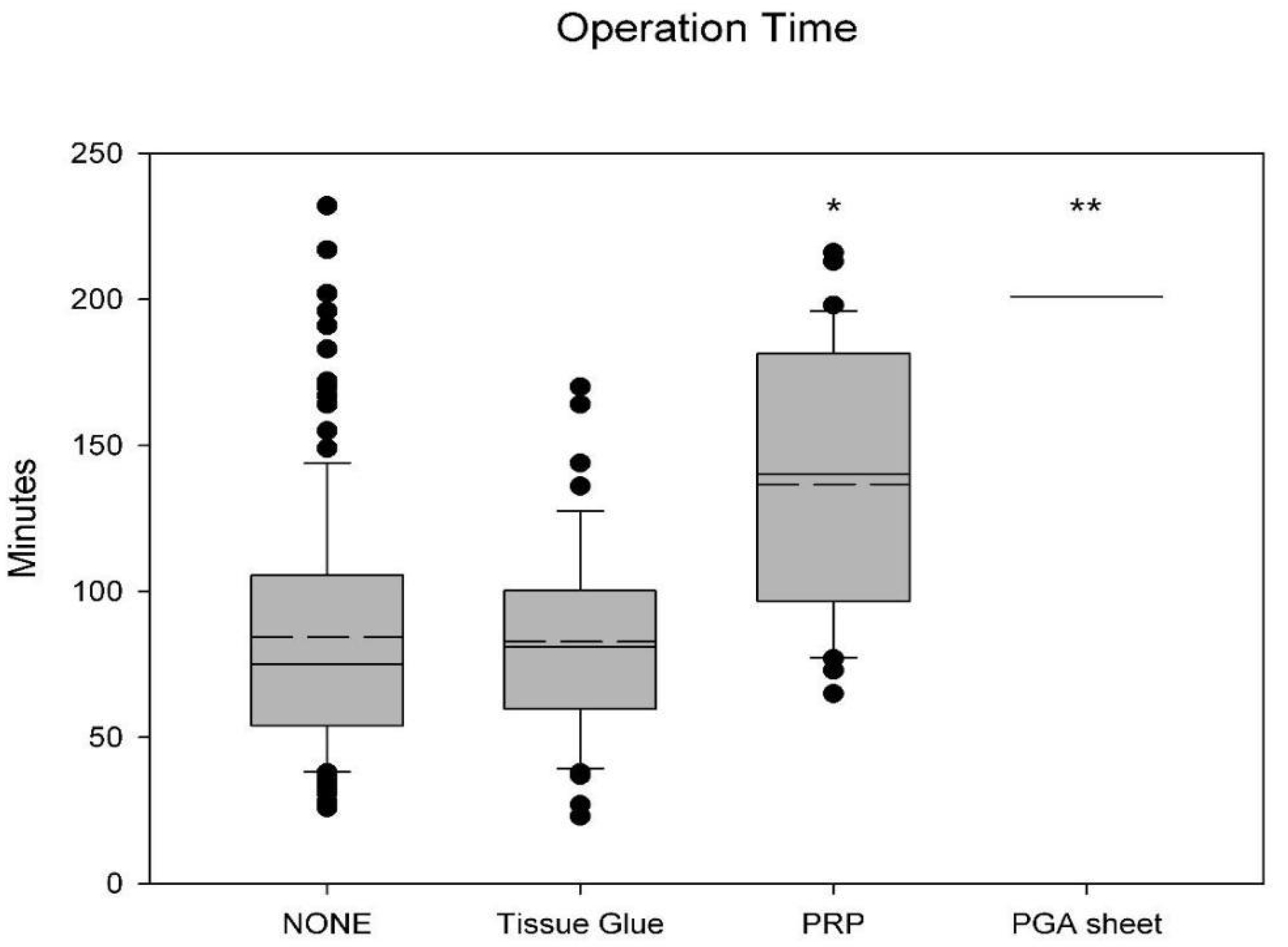
3.2. Operation Time
3.3. Bleeding Amount
3.4. Postoperative Pain
3.5. Postoperative Complications and Emergency Room Visits
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Khan, A.; Ramar, K.; Maddirala, S.; Friedman, O.; Pallanch, J.F.; Olson, E.J. Uvulopalatopharyngoplasty in the management of obstructive sleep apnea: The mayo clinic experience. Mayo Clin. Proc. 2009, 84, 795–800. [Google Scholar] [CrossRef] [Green Version]
- Sheen, D.; Abdulateef, S. Uvulopalatopharyngoplasty. Oral Maxillofac. Surg. Clin. 2021, 33, 295–303. [Google Scholar] [CrossRef]
- Shepard, J.W., Jr.; Olsen, K.D. Uvulopalatopharyngoplasty for treatment of obstructive sleep apnea. Mayo Clin. Proc. 1990, 65, 1260–1267. [Google Scholar] [CrossRef]
- Croft, C.B.; Golding-Wood, D.G. Uses and complications of uvulopalatopharyngoplasty. J. Laryngol. Otol. 1990, 104, 871–875. [Google Scholar] [CrossRef]
- Haavisto, L.; Suonpää, J. Complications of uvulopalatopharyngoplasty. Clin. Otolaryngol. Allied Sci. 1994, 19, 243–247. [Google Scholar] [CrossRef]
- Kandasamy, T.; Wright, E.D.; Fuller, J.; Rotenberg, B.W. The incidence of early post-operative complications following uvulopalatopharyngoplasty: Identification of predictive risk factors. J. Otolaryngol. Head Neck Surg. 2013, 42, 15. [Google Scholar] [CrossRef] [Green Version]
- Zohar, Y.; Finkelstein, Y.; Talmi, Y.P.; Bar-Ilan, Y. Uvulopalatopharyngoplasty: Evaluation of postoperative complications, sequelae, and results. Laryngoscope 1991, 101, 775–779. [Google Scholar] [CrossRef]
- Waldron, M.G.; Judge, C.; Farina, L.; O’Shaughnessy, A.; O’Halloran, M. Barrier materials for prevention of surgical adhesions: Systematic review. BJS Open 2022, 6, zrac075. [Google Scholar] [CrossRef]
- Razali, R.A.; Vijakumaran, U.; Fauzi, M.B.; Lokanathan, Y. Maximizing Postoperative Recovery: The Role of Functional Biomaterials as Nasal Packs—A Comprehensive Systematic Review without Meta-Analysis (SWiM). Pharmaceutics 2023, 15, 1534. [Google Scholar] [CrossRef]
- Lu, Y.-C.; Hsu, L.-I.; Lin, C.-F.; Hsu, C.-P.; Chang, T.-K.; Cheng, C.-C.; Huang, C.-H. Biomechanical characteristics of self-expanding sinus stents during crimping and deployment_A comparison between different biomaterials. J. Mech. Behav. Biomed. Mater. 2023, 138, 105669. [Google Scholar] [CrossRef]
- McMillan, A.; McMillan, N.; Gupta, N.; Kanotra, S.P.; Salem, A.K. 3D bioprinting in otolaryngology: A review. Adv. Healthc. Mater. 2023; early view. [Google Scholar] [CrossRef]
- Bunnell, A.M.; Fernandes, R.P. Operative airway management and tracheostomy. In Modern Management of Obstructive Sleep Apnea; Springer: Cham, Switzerland, 2019; pp. 107–116. [Google Scholar]
- Vaiman, M.; Shlamkovich, N.; Eviatar, E.; Segal, S. Effect of modern fibrin glue on bleeding after tonsillectomy and adenoidectomy. Ann. Otol. Rhinol. Laryngol. 2003, 112, 410–414. [Google Scholar] [CrossRef]
- Derkay, C.S.; Baydoun, H.A.; Stone, L. Intraoperative use of QuikClot during adenotonsillectomy: A prospective pediatric trial. Ann. Otol. Rhinol. Laryngol. 2015, 124, 384–391. [Google Scholar] [CrossRef]
- Vaiman, M.; Krakovski, D.; Gavriel, H. Fibrin sealant reduces pain after tonsillectomy: Prospective randomized study. Ann. Otol. Rhinol. Laryngol. 2006, 115, 483–489. [Google Scholar] [CrossRef]
- Brennan, M. Fibrin glue. Blood Rev. 1991, 5, 240–244. [Google Scholar] [CrossRef]
- Kim, S.H.; Ahn, J.H.; Yoon, H.J.; Kim, J.H.; Hwang, Y.M.; Choi, Y.S.; Yi, J.W. Effect of a Polyglycolic Acid Mesh Sheet (Neoveil™) in Thyroid Cancer Surgery: A Prospective Randomized Controlled Trial. Cancers 2022, 14, 3901. [Google Scholar] [CrossRef]
- Tsou, Y.-A.; Tien, V.H.-C.; Chen, S.-H.; Shih, L.-C.; Lin, T.-C.; Chiu, C.-J.; Chang, W.-D. Autologous Fat Plus Platelet-Rich Plasma versus Autologous Fat Alone on Sulcus Vocalis. J. Clin. Med. 2022, 11, 725. [Google Scholar] [CrossRef]
- Oneto, P.; Etulain, J. PRP in wound healing applications. Platelets 2021, 32, 189–199. [Google Scholar] [CrossRef]
- Liu, L.; Rodman, C.; Worobetz, N.E.; Johnson, J.; Elmaraghy, C.; Chiang, T. Topical biomaterials to prevent post-tonsillectomy hemorrhage. J. Otolaryngol. Head Neck Surg. 2019, 48, 45. [Google Scholar] [CrossRef] [Green Version]
- Sidman, J.D.; Lander, T.A.; Finkelstein, M. Platelet-rich plasma for pediatric tonsillectomy patients. Laryngoscope 2008, 118, 1765–1767. [Google Scholar] [CrossRef]
- Gokce Kutuk, S.; Ozdas, T. The impact of platelet-rich plasma therapy on short-term postoperative outcomes of pediatric tonsillectomy patients. Eur. Arch. Otorhinolaryngol. 2019, 276, 489–495. [Google Scholar] [CrossRef]
- Albazee, E.; Diab, S.; Awad, A.K.; Aboeldahab, H.; Abdella, W.S.; Abu-Zaid, A. The analgesic and anti-haemorrhagic efficacy of platelet-rich plasma in tonsillectomy: A systematic review and meta-analysis of randomised controlled trials. Clin. Otolaryngol. 2023, 48, 1–9. [Google Scholar] [CrossRef]
- Kouketsu, A.; Nogami, S.; Fujiwara, M.; Mori, S.; Yamauchi, K.; Hashimoto, W.; Miyashita, H.; Kurihara, J.; Kawai, T.; Higuchi, K. Clinical evaluations of autologous fibrin glue and polyglycolic acid sheets as oral surgical wound coverings after partial glossectomy. J. Cranio-Maxillofac. Surg. 2016, 44, 964–968. [Google Scholar] [CrossRef]
- Takeuchi, J.; Suzuki, H.; Murata, M.; Kakei, Y.; Ri, S.; Umeda, M.; Komori, T. Clinical evaluation of application of polyglycolic acid sheet and fibrin glue spray for partial glossectomy. J. Oral Maxillofac. Surg. 2013, 71, e126–e131. [Google Scholar] [CrossRef]
- Miyaguchi, S.-i.; Horii, A.; Kambara, R.; Takemoto, N.; Akazawa, H.; Takahashi, N.; Baba, H.; Inohara, H. Effects of covering surgical wounds with polyglycolic acid sheets for posttonsillectomy pain. Otolaryngol. Head Neck Surg. 2016, 155, 876–878. [Google Scholar] [CrossRef]
- Akhundov, K.; Pietramaggiori, G.; Darwiche, S.; Guerid, S.; Scaletta, C.; Hirt-Burri, N.; Applegate, L.; Raffoul, W. Development of a cost-effective method for platelet-rich plasma (PRP) preparation for topical wound healing. Ann. Burn. Fire Disasters 2012, 25, 207–213. [Google Scholar]
- Naito, M.; Sato, T.; Nakamura, T.; Yamanashi, T.; Miura, H.; Tsutsui, A.; Watanabe, M. Secure overlap stapling using a linear stapler with bioabsorbable polyglycolic acid felt. Asian J. Endosc. Surg. 2017, 10, 308–312. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.; Osoegawa, T.; Kubokawa, M.; Esaki, M.; Minoda, Y.; Ogino, H.; Ihara, E. Circumferential suture delivery method of polyglycolic acid sheets for gastric postendoscopic submucosal dissection ulcers. Endoscopy 2023, 55, E68–E69. [Google Scholar] [CrossRef]
- Giuffrè, G.; Caputo, G.; Misso, S.; Peluso, F. Platelet-rich plasma treatment and hemostasis in patients with hemorrhagic risk. Minerva Stomatol. 2006, 55, 599–609. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| None Use | Tissue Glue | PRP | PGA Sheet | |
|---|---|---|---|---|
| AGE | 38.02 ± 12.31 | 38.57 ± 11.54 | 38.64 ± 9.81 | 39 ± 4.24 |
| GENDER (M:F) | 83:49 | 34:12 | 23:10 | 2:0 |
| BMI | 26.68 ± 4.87 | 27.44 ± 5.82 | 27.09 ± 4.41 | 25.87 ± 2.64 |
| Hemoglobin | 14.50 ± 1.43 | 14.35 ± 1.53 | 14.51 ± 1.24 | 13.35 ± 1.77 |
| Platelet | 267.54 ± 61.36 | 269.24 ± 50.80 | 272.73 ± 60.94 | 268.00 ± 107.48 |
| PT | 12.76 ± 0.80 | 12.95 ± 0.76 | 12.75 ± 0.71 | 13.15 ± 0.64 |
| APTT | 34.17 ± 4.20 | 32.63 ± 3.72 | 30.94 ± 2.46 | 27.50 ± 2.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, T.-C.; Huang, T.-C.; Chen, P.-Y.; Shih, C.-C.; Chang, W.-W. Biomaterial Material Applications in Postoperative Surgical Fields of Uvulopalatopharyngoplasty: A Comparative Study. J. Funct. Biomater. 2023, 14, 337. https://doi.org/10.3390/jfb14070337
Yu T-C, Huang T-C, Chen P-Y, Shih C-C, Chang W-W. Biomaterial Material Applications in Postoperative Surgical Fields of Uvulopalatopharyngoplasty: A Comparative Study. Journal of Functional Biomaterials. 2023; 14(7):337. https://doi.org/10.3390/jfb14070337
Chicago/Turabian StyleYu, Tsung-Che, Ting-Chieh Huang, Po-Yueh Chen, Chun-Che Shih, and Wei-Wen Chang. 2023. "Biomaterial Material Applications in Postoperative Surgical Fields of Uvulopalatopharyngoplasty: A Comparative Study" Journal of Functional Biomaterials 14, no. 7: 337. https://doi.org/10.3390/jfb14070337