
One-Piece Mini Dental Implant-Retained Mandibular Overdentures: 10-Year Clinical and Radiological Outcomes of a Non-Comparative Longitudinal Observational Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrolment
- Complete edentulism (minimum duration of 6 months);
- Interforaminal bone dimension of at least 4 mm clinical width (clinical examination with a periodontal probe) and a minimum height of approximately 13 mm (assessed by two-dimensional X-ray examination);
- Bone augmentation required for standard diameter implant placement;
- Good general health (ASA classification 1 or 2);
- Not dependent on care.
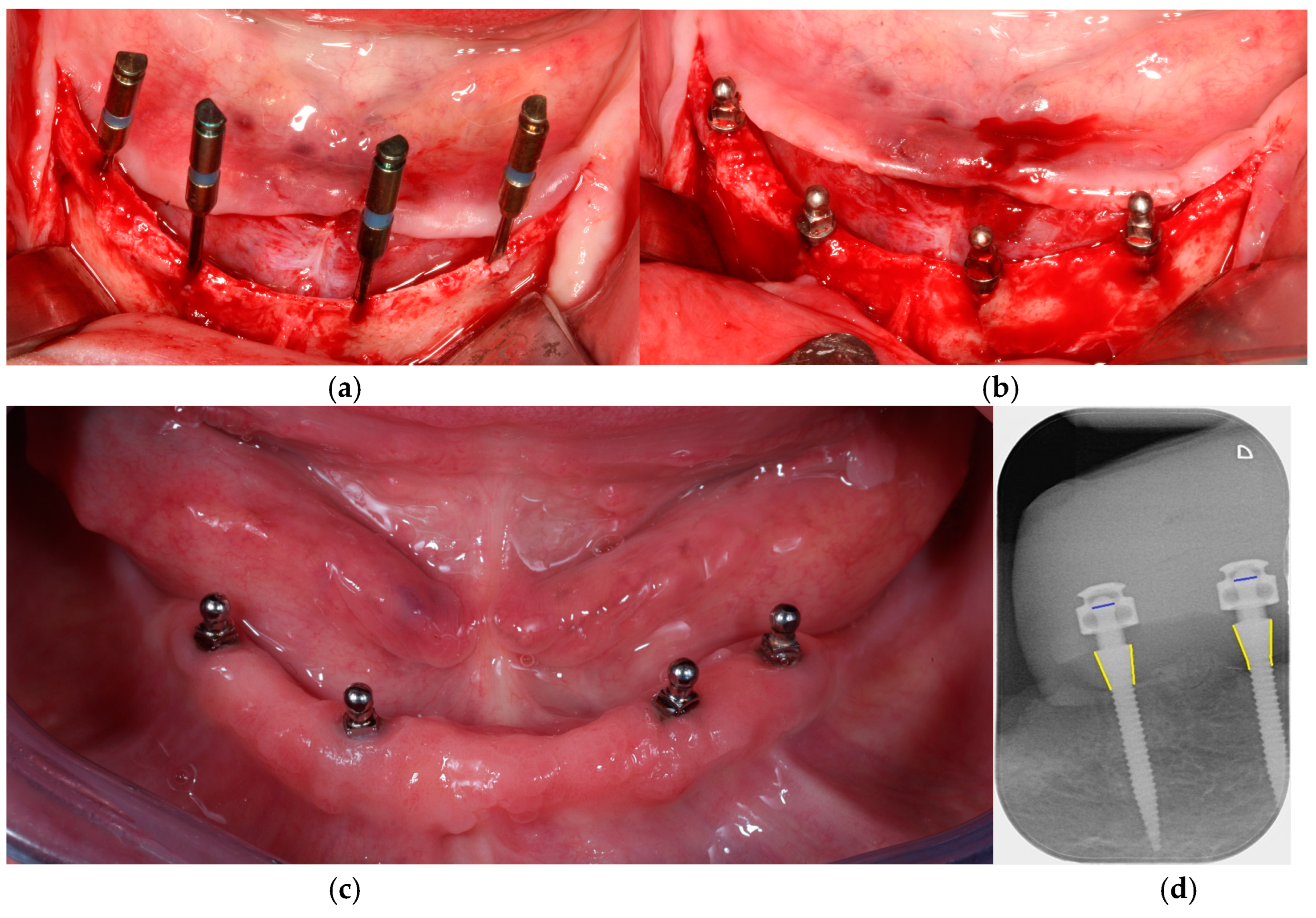
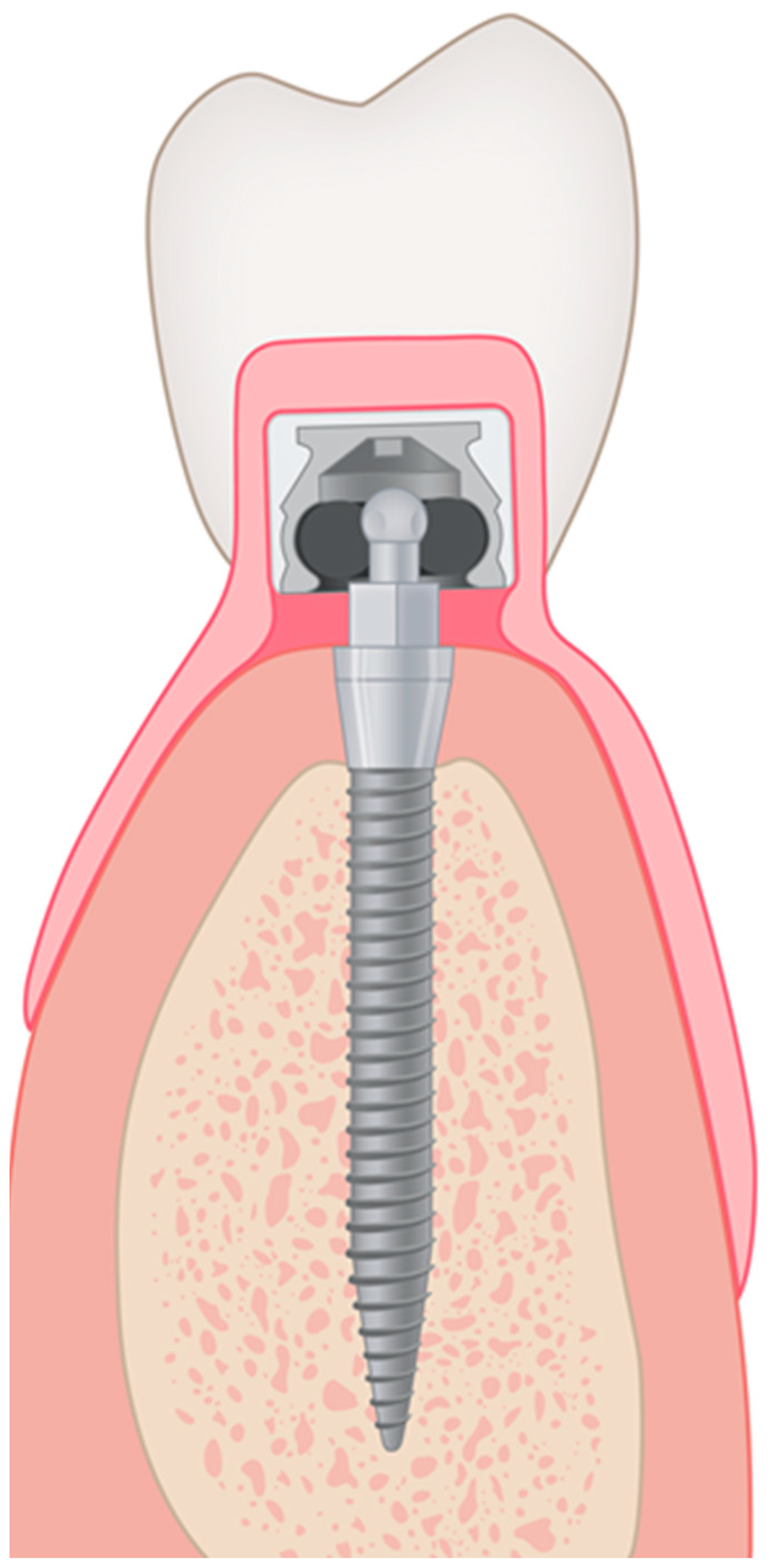
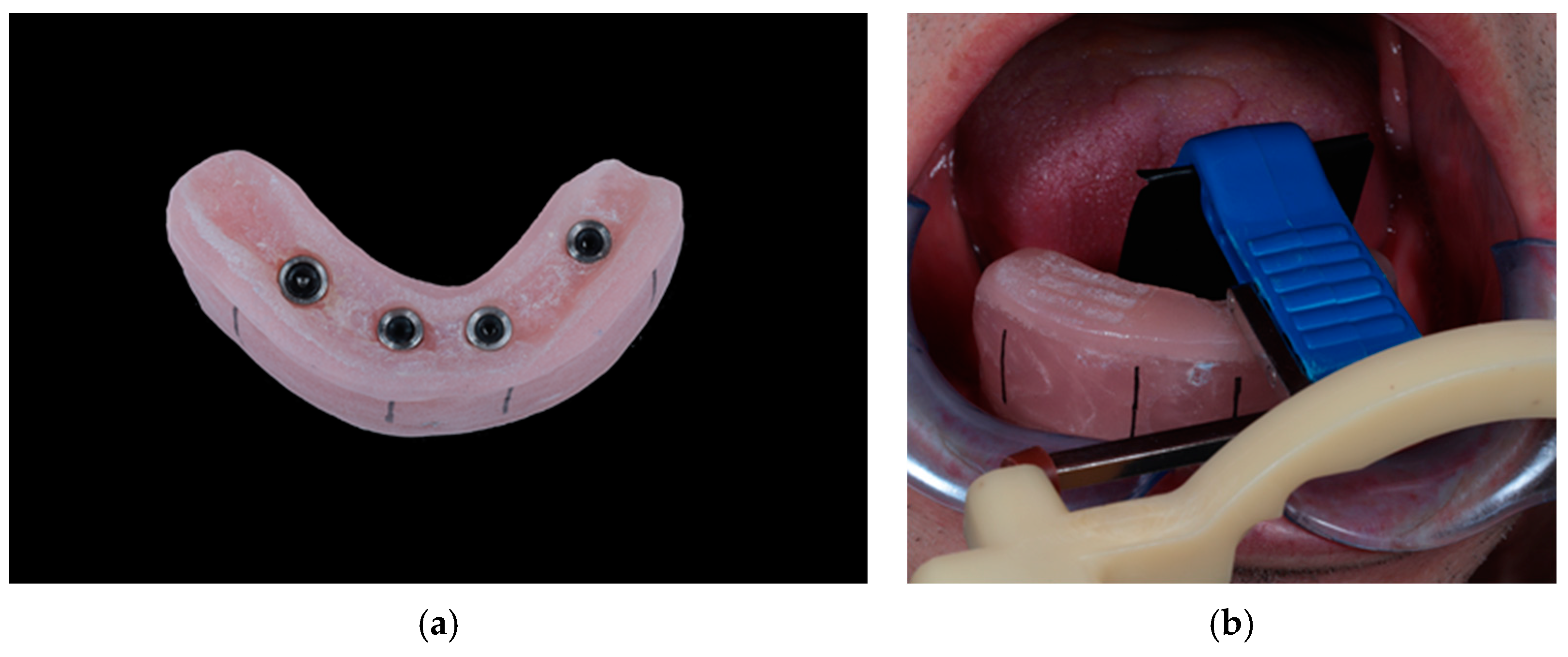
2.2. Study Procedures
2.3. Outcome Measures
2.3.1. Radiographic Analysis of Peri-Implant Bone Levels
2.3.2. Clinical Parameters
- mPI: modified Plaque Index [27];
- PPD: peri-implant probing pocket depth: measured to the nearest millimeter with a Hu-Friedy PGF–GFS periodontal probe (Hu-Friedy, Chicago, IL, USA);
- The occurrence of subsequent bleeding (yes/no);
- The presence of KM at the lingual and buccal aspects.
- Matrix loosening;
- Denture cracking and fractures;
- The need for relining;
- Any signs of wear at the male part.
2.3.3. Definition of Implant Survival, Success, and Denture Survival
2.4. Statistical Analyses
3. Results
3.1. Description of Participants
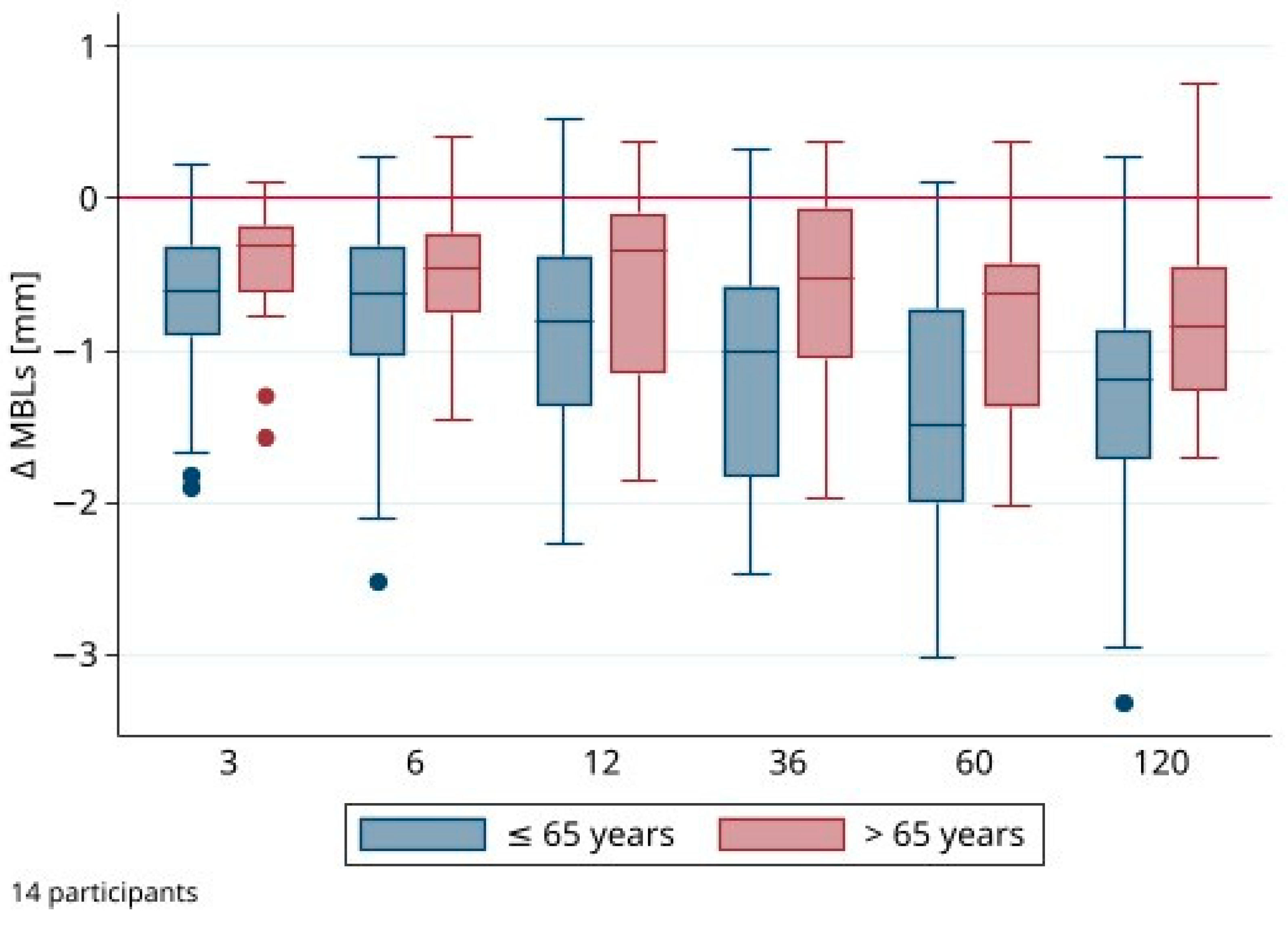
3.2. Marginal Bone Level Alterations (ΔMBLs)
3.3. Clinical Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schimmel, M.; Aarab, G.; Baad-Hansen, L.; Lobbezoo, F.; Svensson, P. A conceptual model of oro-facial health with an emphasis on function. J. Oral Rehabil. 2021, 48, 1283–1294. [Google Scholar] [CrossRef] [PubMed]
- Furuta, M.; Takeuchi, K.; Adachi, M.; Kinoshita, T.; Eshima, N.; Akifusa, S.; Kikutani, T.; Yamashita, Y. Tooth loss, swallowing dysfunction and mortality in Japanese older adults receiving home care services. Geriatr. Gerontol. Int. 2018, 18, 873–880. [Google Scholar] [CrossRef]
- Musacchio, E.; Perissinotto, E.; Binotto, P.; Sartori, L.; Silva-Netto, F.; Zambon, S.; Manzato, E.; Corti, M.C.; Baggio, G.; Crepaldi, G. Tooth loss in the elderly and its association with nutritional status, socio-economic and lifestyle factors. Acta Odontol. Scand. 2007, 65, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed]
- Thomason, J.M.; Kelly, S.A.M.; Bendkowski, A.; Ellis, J.S. Two implant retained overdentures—A review of the literature supporting the McGill and York consensus statements. J. Dent. 2012, 40, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Heydecke, G.; Locker, D.; Awad, M.A.; Lund, J.P.; Feine, J.S. Oral and general health-related quality of life with conventional and implant dentures. Community Dent. Oral Epidemiol. 2003, 31, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Hyland, R.; Ellis, J.; Thomason, M.; El-Feky, A.; Moynihan, P. A qualitative study on patient perspectives of how conventional and implant-supported dentures affect eating. J. Dent. 2009, 37, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Feine, J.S.; Carlsson, G.E.; Awad, M.A.; Chehade, A.; Duncan, W.J.; Gizani, S.; Head, T.; Heydecke, G.; Lund, J.P.; MacEntee, M.; et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology 2002, 19, 3–4. [Google Scholar] [PubMed]
- Thomason, J.M.; Feine, J.; Exley, C.; Moynihan, P.; Müller, F.; Naert, I.; Ellis, J.S.; Barclay, C.; Butterworth, C.; Scott, B.; et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients—The york consensus statement. Br. Dent. J. 2009, 207, 185–186. [Google Scholar] [CrossRef]
- Walter, C.; Al-Nawas, B.; Wolff, T.; Schiegnitz, E.; Grötz, K.A. Dental implants in patients treated with antiresorptive medication—A systematic literature review. Int. J. Implant Dent. 2016, 2, 9. [Google Scholar] [CrossRef]
- Visser, A.; Stellingsma, C.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A. A 15-Year Comparative Prospective Study of Surgical and Prosthetic Care and Aftercare of Overdenture Treatment in the Atrophied Mandible: Augmentation Versus Nonaugmentation. Clin. Implant Dent. Relat. Res. 2016, 18, 1218–1226. [Google Scholar] [CrossRef]
- Atieh, M.A.; Zadeh, H.; Stanford, C.M.; Cooper, L.F. Survival of short dental implants for treatment of posterior partial edentulism: A systematic review. Int. J. Oral Maxillofac. Implants 2012, 27, 1323–1331. [Google Scholar]
- Papaspyridakos, P.; De Souza, A.; Vazouras, K.; Gholami, H.; Pagni, S.; Weber, H.P. Survival rates of short dental implants (≤6 mm) compared with implants longer than 6 mm in posterior jaw areas: A meta-analysis. Clin. Oral Implants Res. 2018, 29, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI Consensus Report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implants Res. 2018, 29, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Elias, C.N.; Lima, J.H.C.; Valiev, R.; Meyers, M.A. Biomedical Applications of Titanium and Its Alloys. JOM 2008, 60, 46–49. [Google Scholar] [CrossRef]
- Koopaie, M.; Bordbar-Khiabani, A.; Kolahdooz, S.; Darbandsari, A.K.; Mozafari, M. Advanced surface treatment techniques counteract biofilm-associated infections on dental implants. Mater. Res. Express 2020, 7, 015417. [Google Scholar] [CrossRef]
- Abou-Ayash, S.; Schimmel, M.; Worni, A.; Enkling, N. O-Ring Attachments on One-Piece Mini Dental Implants: In-Vitro Analysis of Retention Force Reproducibility Using Different Pristine Matrix-O-Ring Combinations. Int. J. Prosthodont. 2023, 36, 59. [Google Scholar] [CrossRef] [PubMed]
- Morneburg, T.R.; Pröschel, P.A. Success rates of microimplants in edentulous patients with residual ridge resorption. Int. J. Oral Maxillofac. Implant. 2008, 23, 270–276. [Google Scholar]
- Mundt, T.; Schwahn, C.; Stark, T.; Biffar, R. Clinical response of edentulous people treated with mini dental implants in nine dental practices. Gerodontology 2015, 32, 179–187. [Google Scholar] [CrossRef]
- Temizel, S.; Heinemann, F.; Dirk, C.; Bourauel, C.; Hasan, I. Clinical and radiological investigations of mandibular overdentures supported by conventional or mini-dental implants: A 2-year prospective follow-up study. J. Prosthet. Dent. 2017, 117, 239–246.e2. [Google Scholar] [CrossRef]
- Enkling, N.; Moazzin, R.; Geers, G.; Kokoschka, S.; Abou-Ayash, S.; Schimmel, M. Clinical outcomes and bone-level alterations around one-piece mini dental implants retaining mandibular overdentures: 5-year follow-up of a prospective cohort study. Clin. Oral Implants Res. 2020, 31, 549–556. [Google Scholar] [CrossRef] [PubMed]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Enkling, N.; Saftig, M.; Worni, A.; Mericske-Stern, R.; Schimmel, M. Chewing efficiency, bite force and oral health-related quality of life with narrow diameter implants—A prospective clinical study: Results after one year. Clin. Oral Implants Res. 2017, 28, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Geering, A.H.; Kundert, M. Total- und Hybridprothetik; Thieme: Stuttgart, Germany, 1992; Volume 2. [Google Scholar]
- Misch, C.E. Bone Density: A Key Determinant for Clinical Success, 2nd ed.; Misch, C.E., Ed.; Contemporary Implant Dentistry, CV Mosby Company: St Louis, MO, USA, 1999. [Google Scholar]
- Mombelli, A.; Van Oosten, M.A.C.; Schiirch, E.; Lang, N.P. The microbiota associated with successfuiorfaiiing osseointegrated titanium impiants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) pisa consensus conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef]
- Park, J.-H.; Lee, J.-Y.; Shin, S.-W. Treatment Outcomes for Mandibular Mini-Implant–Retained Overdentures: A Systematic Review. Int. J. Prosthodont. 2017, 30, 269–276. [Google Scholar] [CrossRef]
- Marcello-Machado, R.M.; Faot, F.; Schuster, A.J.; Nascimento, G.G.; Del Bel Cury, A.A. Mini-implants and narrow diameter implants as mandibular overdenture retainers: A systematic review and meta-analysis of clinical and radiographic outcomes. J. Oral Rehabil. 2018, 45, 161–183. [Google Scholar] [CrossRef]
- Lemos, C.A.A.; Verri, F.R.; Batista, V.E.d.S.; Júnior, J.F.S.; Mello, C.C.; Pellizzer, E.P. Complete overdentures retained by mini implants: A systematic review. J. Dent. 2017, 57, 4–13. [Google Scholar] [CrossRef]
- De Souza, R.F.; Ribeiro, A.B.; Della Vecchia, M.P.; Costa, L.; Cunha, T.R.; Reis, A.C.; Albuquerque, R.F. Mini vs. standard implants for mandibular overdentures: A randomized trial. J. Dent. Res. 2015, 94, 1376–1384. [Google Scholar] [CrossRef]
- Curado, T.F.F.; Silva, J.R.; Nascimento, L.N.; Leles, J.L.R.; McKenna, G.; Schimmel, M.; Leles, C.R. Implant survival/success and peri-implant outcomes of titanium-zirconium mini implants for mandibular overdentures: Results from a 1-year randomized clinical trial. Clin. Oral Implants Res. 2023, 34, 769–782. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Weber, H.P.; Bragger, U.; Balsiger, C. Tissue integration of one-stage ITI implants: 3-year results of a longitudinal study with Hollow-Cylinder and Hollow-Screw implants. Int. J. Oral Maxillofac. Implants 1991, 6, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar] [PubMed]
- Ramanauskaite, A.; Schwarz, F.; Sader, R. Influence of width of keratinized tissue on the prevalence of peri-implant diseases: A systematic review and meta-analysis. Clin. Oral Implants Res. 2022, 33, 8–31. [Google Scholar] [CrossRef]
- Ravidà, A.; Arena, C.; Tattan, M.; Caponio, V.C.A.; Saleh, M.H.A.; Wang, H.L.; Troiano, G. The role of keratinized mucosa width as a risk factor for peri-implant disease: A systematic review, meta-analysis, and trial sequential analysis. Clin. Implant Dent. Relat. Res. 2022, 24, 287–300. [Google Scholar] [CrossRef]
- Marsh, P.D.; Percival, R.S.; Challacombe, S.J. The Influence of Denture-wearing and Age on the Oral Microflora. J. Dent. Res. 1992, 71, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Toolson, L.B.; Smith, D.E.; Phillips, C. A 2-year longitudinal study of overdenture patients. Part II: Assessment of the periodontal health of overdenture abutments. J. Prosthet. Dent. 1982, 47, 4–11. [Google Scholar] [CrossRef]
- Zenthöfer, A.; Baumgart, D.; Cabrera, T.; Rammelsberg, P.; Schröder, J.; Corcodel, N.; Hassel, A.J. Poor dental hygiene and periodontal health in nursing home residents with dementia: An observational study. Odontology 2017, 105, 208–213. [Google Scholar] [CrossRef]
- Schimmel, M.; Müller, F.; Suter, V.; Buser, D. Implants for elderly patients. Periodontology 2000 2017, 73, 228–240. [Google Scholar] [CrossRef]
- Schimmel, M.; Srinivasan, M.; McKenna, G.; Müller, F. Effect of advanced age and/or systemic medical conditions on dental implant survival: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 311–330. [Google Scholar] [CrossRef] [PubMed]
- Krennmair, S.; Weinländer, M.; Forstner, T.; Krennmair, G.; Stimmelmayr, M. Factors affecting peri-implant bone resorption in four Implant supported mandibular full-arch restorations: A 3-year prospective study. J. Clin. Periodontol. 2016, 43, 92–101. [Google Scholar] [CrossRef]
- Bryant, S.R. The effects of age, jaw site, and bone condition on oral implant outcomes. Int. J. Prosthodont. 1998, 11, 470–490. [Google Scholar] [PubMed]
- Maniewicz, S.; Buser, R.; Duvernay, E.; Vazquez, L.; Loup, A.; Perneger, T.; Schimmel, M.; Müller, F. Short Dental Implants Retaining Two-Implant Mandibular Overdentures in Very Old, Dependent Patients: Radiologic and Clinical Observation Up to 5 Years. Int. J. Oral Maxillofac. Implants 2017, 32, 415–422. [Google Scholar] [CrossRef]
- Müller, F.; Srinivasan, M.; Krause, K.H.; Schimmel, M. Periodontitis and peri-implantitis in elderly people experiencing institutional and hospital confinement. Periodontology 2000 2022, 90, 138–145. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Graves, C.L.; Gonzalez, O.A.; Dawson, D.; Morford, L.A.; Huja, P.E.; Hartsfield, J.K.; Huja, S.S.; Pandruvada, S.; Wallet, S.M. Aging, inflammation, immunity and periodontal disease. Periodontology 2000 2016, 72, 54–75. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-implantitis—Onset and pattern of progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Mifsud, D.P.; Cortes, A.R.G.; Zarb, M.J.; Attard, N.J. Maintenance and risk factors for fractures of overdentures using immediately loaded conventional diameter or mini implants with Locator abutments: A cohort study. Clin. Implant Dent. Relat. Res. 2020, 22, 706–712. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implant Position | 3 Months | 6 Months | 12 Months | 3 Years | 5 Years | 10 Years |
|---|---|---|---|---|---|---|
| 34 | −0.58 ± 0.62 | −0.68 ± 0.66 | −0.64 ± 0.62 | −1.00 ± 0.88 | −1.26 ± 0.89 | −1.42 ± 0.88 |
| 32 | −0.61 ± 0.42 | −0.79 ± 0.62 | −1.03 ± 0.67 | −1.19 ± 0.70 | −1.43 ± 0.73 | −1.06 ± 0.53 |
| 42 | −0.70 ± 0.52 | −0.69 ± 0.61 | −0.71 ± 0.79 | −0.96 ± 0.79 | −1.13 ± 0.73 | −1.04 ± 0.58 |
| 44 | −0.54 ± 0.39 | −0.49 ± 0.43 | −0.56 ± 0.62 | −0.68 ± 0.73 | −0.89 ± 0.75 | −0.95 ± 1.08 |
| Overall | −0.61 ± 0.49 | −0.66 ± 0.58 | −0.74 ± 0.68 | −0.96 ± 0.78 | −1.18 ± 0.78 | −1.12 ± 0.80 |
| Presence of Keratinized Mucosa | Implants (n = 56) | ΔMBL ≤ 2 (%) | ΔMBL 2–4 mm (%) |
|---|---|---|---|
| yes | 36 | 86.1 | 13.9 |
| no | 20 | 90.0 | 10.0 |
| Follow-Up (months) | PD (mm) | mPI (mv) | BOP (%) |
|---|---|---|---|
| 3 | 3.19 ± 0.87 | 0.39 ± 0.42 | 64.3 |
| 6 | 3.39 ± 0.88 | 0.21 ± 0.31 | 50.0 |
| 12 | 3.50 ± 0.54 | 0.44 ± 0.42 | 42.9 |
| 36 | 2.00 ± 0.46 | 0.36 ± 0.50 | 21.4 |
| 60 | 1.67 ± 0.38 | 0.55 ± 0.37 | 64.3 |
| 120 | 2.17 ± 0.51 | 0.75 ± 0.35 | 92.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schenk, N.; Bukvic, H.; Schimmel, M.; Abou-Ayash, S.; Enkling, N. One-Piece Mini Dental Implant-Retained Mandibular Overdentures: 10-Year Clinical and Radiological Outcomes of a Non-Comparative Longitudinal Observational Study. J. Funct. Biomater. 2024, 15, 99. https://doi.org/10.3390/jfb15040099
Schenk N, Bukvic H, Schimmel M, Abou-Ayash S, Enkling N. One-Piece Mini Dental Implant-Retained Mandibular Overdentures: 10-Year Clinical and Radiological Outcomes of a Non-Comparative Longitudinal Observational Study. Journal of Functional Biomaterials. 2024; 15(4):99. https://doi.org/10.3390/jfb15040099
Chicago/Turabian StyleSchenk, Nicole, Hristina Bukvic, Martin Schimmel, Samir Abou-Ayash, and Norbert Enkling. 2024. "One-Piece Mini Dental Implant-Retained Mandibular Overdentures: 10-Year Clinical and Radiological Outcomes of a Non-Comparative Longitudinal Observational Study" Journal of Functional Biomaterials 15, no. 4: 99. https://doi.org/10.3390/jfb15040099