


Lymphatic Regeneration after Popliteal Lymph Node Excision and Implantation of Aligned Nanofibrillar Collagen Scaffolds: An Experimental Rabbit Model

 ,
,  , , , , ,
, , , , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Pre-Operative Procedures
2.2. Intra-Operative Procedures
2.3. Postoperative Procedures
2.4. Histopathological and Immunohistochemical Analyses
2.5. Statistical Analysis
3. Results
3.1. Treatment Group (G1)
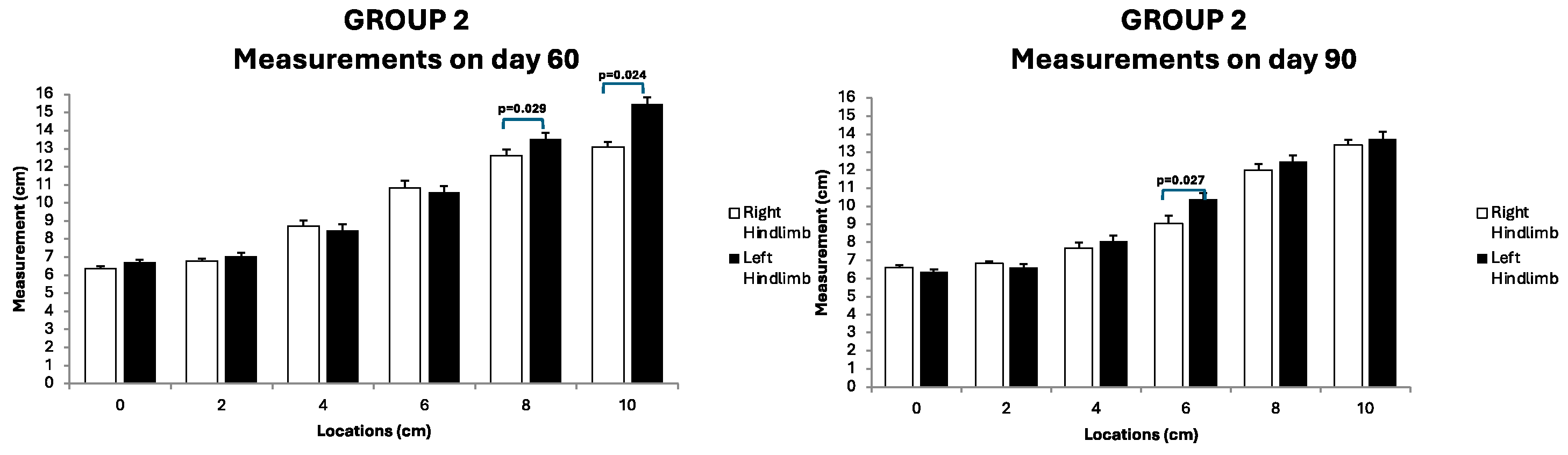
3.2. Preventive Group (G2)
3.3. Control Group (G3)
3.4. Follow-Up Assessments
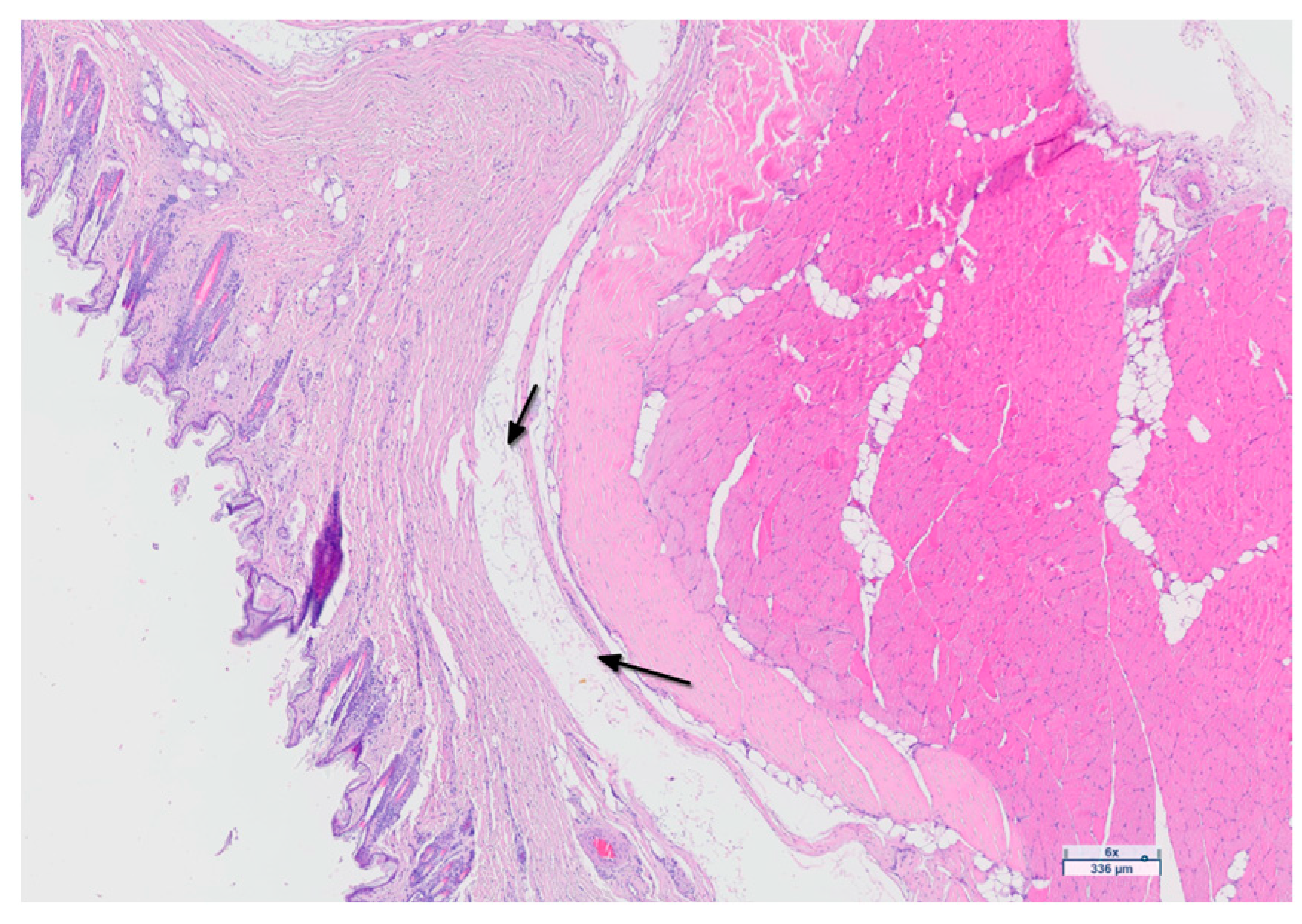
3.5. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warren, A.G.; Brorson, H.; Borud, L.J.; Slavin, S.A. Lymphedema: A comprehensive review. Ann. Plast. Surg. 2007, 59, 464–472. [Google Scholar] [CrossRef]
- Nguyen, D.; Zaitseva, T.S.; Zhou, A.; Rochlin, D.; Sue, G.; Deptula, P.; Tabada, P.; Wan, D.; Loening, A.; Paukshto, M.; et al. Lymphatic regeneration after implantation of aligned nanofibrillar collagen scaffolds: Preliminary preclinical and clinical results. J. Surg. Oncol. 2022, 125, 113–122. [Google Scholar] [CrossRef]
- Weber, E.; Aglianò, M.; Bertelli, E.; Gabriele, G.; Getnnaro, P.; Balrone, V. Lymphatic Collecting Vessels in Health and Disease: A Review of Histopathological Modifications in Lymphedema. Lymphat. Res. Biol. 2022, 20, 468–477. [Google Scholar] [CrossRef]
- Shaitelman, S.F.; Cromwell, K.D.; Rasmussen, J.C.; Stout, N.L.; Armer, J.M.; Lasinski, B.B.; Cormier, J.N. Recent progress in the treatment and prevention of cancer-related lymphedema. CA A Cancer J. Clin. 2015, 65, 55–81. [Google Scholar] [CrossRef]
- PDQ Supportive and Palliative Care Editorial Board. Lymphedema (PDQ®): Health Professional Version. In PDQ Cancer Information Summaries [Internet]; National Cancer Institute: Bethesda, MD, USA, 2002. [Google Scholar]
- Becker, C.; Vasile, J.V.; Levine, J.L.; Batista, B.N.; Studinger, R.M.; Chen, C.M.; Riquet, M. Microlymphatic surgery for the treatment of iatrogenic lymphedema. Clin. Plast. Surg. 2012, 39, 385–398. [Google Scholar] [CrossRef]
- Frueh, F.S.; Gousopoulos, E.; Rezaeian, F.; Menger, M.D.; Lindenblatt, N.; Giovanoli, P. Animal models in surgical lymphedema research—A systematic review. J. Surg. Res. 2016, 200, 208–220. [Google Scholar] [CrossRef]
- Szuba, A.; Cooke, J.P.; Yousuf, S.; Rockson, S.G. Decongestive lymphatic therapy for patients with cancer-related or primary lymphedema. Am. J. Med. 2000, 109, 296–300. [Google Scholar] [CrossRef]
- Thompson, B.; Gaitatzis, K.; de Jonge, X.J.; Blackwell, R.; Koetlmeyer, L.A. Manual lymphatic drainage treatment for lymphedema: A systematic review of the literature. J. Cancer Surviv. 2021, 15, 244–258. [Google Scholar] [CrossRef]
- Schaverien, M.V.; Badash, I.; Selber, J.C.; Cheng, M.-H.; Patel, K.M. Vascularized Lymph Node Transfer for Lymphedema. Semin. Plast. Surg. 2018, 32, 28–35. [Google Scholar] [CrossRef]
- Scaglioni, M.F.; Fontein, D.B.Y.; Arvanitakis, M.; Giovanoli, P. Systematic review of lymphovenous anastomosis (LVA) for the treatment of lymphedema. Microsurgery 2017, 37, 947–953. [Google Scholar] [CrossRef]
- Pereira, N.; Lee, Y.H.; Suh, Y.; Choi, D.H.; Suh, H.S.; Jeon, J.Y.; Hong, J.P.J. Cumulative Experience in Lymphovenous Anastomosis for Lymphedema Treatment: The Learning Curve Effect on the Overall Outcome. J. Reconstr. Microsurg. 2018, 34, 735–741. [Google Scholar] [CrossRef]
- Dionyssiou, D.; Demiri, E.; Tsimponis, A.; Sarafis, A.; Mpalaris, V.; Tatsidou, G.; Arsos, G. A randomized control study of treating secondary stage II breast cancer-related lymphoedema with free lymph node transfer. Breast Cancer Res. Treat. 2016, 156, 73–79. [Google Scholar] [CrossRef]
- Baumeister, R.G.H.; Frick, A. The microsurgical lymph vessel transplantation. Handchir. Mikrochir. Plast. Chir. 2003, 35, 202–209. [Google Scholar] [CrossRef]
- Campisi, C.; Eretta, C.; Pertile, D.; Da Rin, E.; Macciò, A.; Campisi, M.; Accogli, S.; Bellini, C.; Bonioli, E.; Boccardo, F. Microsurgery for treatment of peripheral lymphedema: Long-term outcome and future perspectives. Microsurgery 2007, 27, 333–338. [Google Scholar] [CrossRef]
- Duewell, S.; Hagspiel, K.D.; Zuber, J.; von Schulthess, G.K.; Bollinger, A.; A Fuchs, W. Swollen lower extremity: Role of MR imaging. Radiology 1992, 184, 227–231. [Google Scholar] [CrossRef]
- Tomczak, H.; Nyka, W.; Lass, P. Lymphoedema: Lymphoscintigraphy versus other diagnostic techniques--a clinician’s point of view. Nucl. Med. Rev. Cent. East. Eur. 2005, 8, 37–43. [Google Scholar]
- Marotel, M.; Cluzan, R.; Ghabboun, S.; Pascot, M.; Alliot, F.; Lasry, J.L. Transaxial computer tomography of lower extremity lymphedema. Lymphology 1998, 31, 180–185. [Google Scholar]
- Ogata, F.; Azuma, R.; Kikuchi, M.; Koshima, I.; Morimoto, Y. Novel lymphography using indocyanine green dye for near-infrared fluorescence labeling. Ann. Plast. Surg. 2007, 58, 652–655. [Google Scholar] [CrossRef]
- Huang, N.; Okogbaa, J.; Lee, J.; Jha, A.; Zaitseva, T.S.; Paukshto, M.V.; Sun, J.S.; Punjya, N.; Fuller, G.G.; Cooke, J.P. The modulation of endothelial cell morphology, function, and survival using anisotropic nanofibrillar collagen scaffolds. Biomaterials 2013, 34, 4038–4047. [Google Scholar] [CrossRef]
- Nakayama, K.H.; Hong, G.; Lee, J.C.; Patel, J.; Edwards, B.; Zaitseva, T.S.; Paukshto, M.V.; Dai, H.; Cooke, J.P.; Woo, Y.J.; et al. Aligned-Braided Nanofibrillar Scaffold with Endothelial Cells Enhances Arteriogenesis. ACS Nano 2015, 9, 6900–6908. [Google Scholar] [CrossRef]
- Hadamitzky, C.; Zaitseva, T.S.; Bazalova-Carter, M.; Paukshto, M.V.; Hou, L.; Strassberg, Z.; Ferguson, J.; Matsuura, Y.; Dash, R.; Yang, P.C.; et al. Aligned nanofibrillar collagen scaffolds–Guiding lymphangiogenesis for treatment of acquired lymphedema. Biomaterials 2016, 102, 259–267. [Google Scholar] [CrossRef]
- Dionyssiou, D.; Nguyen, D.; Topalis, A.; Deptula, P.; Paukshto, M.; Zaitseva, T.; Demiri, E.; Cheva, A.; Rockson, S. Treatment of Rat Lymphedema by Propeller Lymphatic Tissue Flap Combined with Nanofibrillar Collagen Scaffolds. J. Reconstr. Microsurg. 2024, 40, 145–155. [Google Scholar] [CrossRef]
- Nguyen, D.H.; Zhou, A.; Posternak, V.; Rochlin, D.H. Nanofibrillar Collagen Scaffold Enhances Edema Reduction and Formation of New Lymphatic Collectors after Lymphedema Surgery. Plast. Reconstr. Surg. 2021, 148, 1382–1393. [Google Scholar] [CrossRef]
- Cornelissen, A.J.; Qiu, S.S.; Penha, T.L.; Keuter, X.; de Grzymala, A.P.; Tuinder, S.; van der Hulst, R. Outcomes of vascularized versus non-vascularized lymph node transplant in animal models for lymphedema. Review of the literature. J. Surg. Oncol. 2017, 115, 32–36. [Google Scholar] [CrossRef]
- Hsu, J.F.; Yu, R.P.; Stanton, E.W.; Wang, J.; Wong, A.K. Current Advancements in Animal Models of Postsurgical Lymphedema: A Systematic Review. Adv. Wound Care 2022, 11, 399–418. [Google Scholar] [CrossRef]
- Peñuela, R.F.; Arazo, L.C.; Ayala, J.M. Outcomes in vascularized lymph node transplantation in rabbits: A reliable model for improving the surgical approach to lymphedema. Lymphat. Res. Biol. 2019, 17, 413–417. [Google Scholar] [CrossRef]
- Campos, J.L.; Pons, G.; Rodriguez, E.; Al-Sakkaf, A.M.; Vela, F.J.; Pires, L.; Jara, M.J.; Sánchez-Margallo, F.M.; Abellán, E.; Masiá, J. Popliteal vascular lymph node resection in the rabbit hindlimb for secondary lymphedema induction. J. Vis. Exp. 2022, 189, e64576. [Google Scholar] [CrossRef]
- Wolfe, J.H.; Rutt, D.; Kinmonth, J.B. Lymphatic obstruction and lymph node changes--a study of the rabbit popliteal node. Lymphology 1983, 16, 19–26. [Google Scholar]
- Jones-Bolin, S. Guidelines for the care and use of laboratory animals in biomedical research. Curr. Protoc. Pharmacol. 2012, 59, A-4B.1–A-4B.9. [Google Scholar] [CrossRef]
- Cemal, Y.; Pusic, A.; Mehrara, B.J. Preventative measures for lymphedema: Separating fact from fiction. J. Am. Coll. Surg. 2011, 213, 543–551. [Google Scholar] [CrossRef]
- Tammela, T.; Alitalo, K. Lymphangiogenesis: Molecular mechanisms and future promise. Cell 2010, 140, 460–476. [Google Scholar] [CrossRef]
- Rochlin, D.H.; Inchauste, S.; Zelones, J.; Nguyen, D.H. The role of adjunct nanofibrillar collagen scaffold implantation in the surgical management of secondary lymphedema: Review of the literature and summary of initial pilot studies. J. Surg. Oncol. 2020, 121, 121–128. [Google Scholar] [CrossRef]
- Nguyen, D.; Dionyssiou, D.; Zaitseva, T.S.; Zhou, A.T.; Sue, G.; Deptula, P.; Moroz, M.A.; Tabada, P.; Rockson, S.G.; Paukshto, M.V.; et al. Development of a rat model of lymphedema and the implantation of a collagen-based medical device for therapeutic intervention. Front. Cardiovasc. Med. 2023, 10, 1214116. [Google Scholar] [CrossRef]
- Yang, C.; Tinhofer, I.E.; Nguyen, D.; Cheng, M. Enhancing lymphangiogenesis and lymphatic drainage to vascularized lymph nodes with nanofibrillar collagen scaffolds. J. Surg. Oncol. 2022, 126, 1169–1175. [Google Scholar] [CrossRef]
- Daneshgaran, G.; Lo, A.Y.; Paik, C.B.; Cooper, M.N.; Sung, C.; Jiao, W.; Park, S.Y.; Ni, P.; Yu, R.P.; Vorobyova, I.; et al. A pre-clinical animal model of secondary head and neck lymphedema. Sci. Rep. 2019, 9, 18264. [Google Scholar] [CrossRef]
- Hadrian, R.; Palmes, D. Animal models of secondary lymphedema: New approaches in the search for therapeutic options. Lymphat. Res. Biol. 2017, 15, 2–16. [Google Scholar] [CrossRef]
- Lähteenvuo, M.; Honkonen, K.; Tervala, T.; Tammela, T.; Suominen, E.; Lähteenvuo, J.; Kholová, I.; Alitalo, K.; Ylä-Herttuala, S.; Saaristo, A. Growth factor therapy and autologous lymph node transfer in lymphedema. Circulation 2011, 123, 613–620. [Google Scholar] [CrossRef]
- Mapara, M.; Thomas, B.S.; Bhat, K.M. Rabbit as an animal model for experimental research. Dent. Res. J. 2012, 9, 111–118. [Google Scholar] [CrossRef]
- Breiteneder-Geleff, S.; Soleiman, A.; Kowalski, H.; Horvat, R.; Amann, G.; Kriehuber, E.; Diem, K.; Weninger, W.; Tschachler, E.; Alitalo, K.; et al. Angiosarcomas express mixed endothelial phenotypes of blood and lymphatic capillaries: Podoplanin as a specific marker for lymphatic endothelium. Am. J. Pathol. 1999, 154, 385–394. [Google Scholar] [CrossRef]
- Baluk, P.; McDonald, D.M. Markers for microscopic imaging of lymphangiogenesis and angiogenesis. Ann. N. Y. Acad. Sci. 2008, 1131, 1–12. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos, J.L.; Pons, G.; Al-Sakkaf, A.M.; Lusetti, I.L.; Pires, L.; Vela, F.J.; Ramos, E.; Crisóstomo, V.; Sánchez-Margallo, F.M.; Abellán, E.; et al. Lymphatic Regeneration after Popliteal Lymph Node Excision and Implantation of Aligned Nanofibrillar Collagen Scaffolds: An Experimental Rabbit Model. J. Funct. Biomater. 2024, 15, 235. https://doi.org/10.3390/jfb15080235
Campos JL, Pons G, Al-Sakkaf AM, Lusetti IL, Pires L, Vela FJ, Ramos E, Crisóstomo V, Sánchez-Margallo FM, Abellán E, et al. Lymphatic Regeneration after Popliteal Lymph Node Excision and Implantation of Aligned Nanofibrillar Collagen Scaffolds: An Experimental Rabbit Model. Journal of Functional Biomaterials. 2024; 15(8):235. https://doi.org/10.3390/jfb15080235
Chicago/Turabian StyleCampos, José Luis, Gemma Pons, Ali M. Al-Sakkaf, Irene Laura Lusetti, Laura Pires, Francisco Javier Vela, Elena Ramos, Verónica Crisóstomo, Francisco Miguel Sánchez-Margallo, Elena Abellán, and et al. 2024. "Lymphatic Regeneration after Popliteal Lymph Node Excision and Implantation of Aligned Nanofibrillar Collagen Scaffolds: An Experimental Rabbit Model" Journal of Functional Biomaterials 15, no. 8: 235. https://doi.org/10.3390/jfb15080235
APA StyleCampos, J. L., Pons, G., Al-Sakkaf, A. M., Lusetti, I. L., Pires, L., Vela, F. J., Ramos, E., Crisóstomo, V., Sánchez-Margallo, F. M., Abellán, E., & Masiá, J. (2024). Lymphatic Regeneration after Popliteal Lymph Node Excision and Implantation of Aligned Nanofibrillar Collagen Scaffolds: An Experimental Rabbit Model. Journal of Functional Biomaterials, 15(8), 235. https://doi.org/10.3390/jfb15080235