
Bio-Environment-Induced Degradation and Failure of Internal Fixation Implants


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Study and Discussion
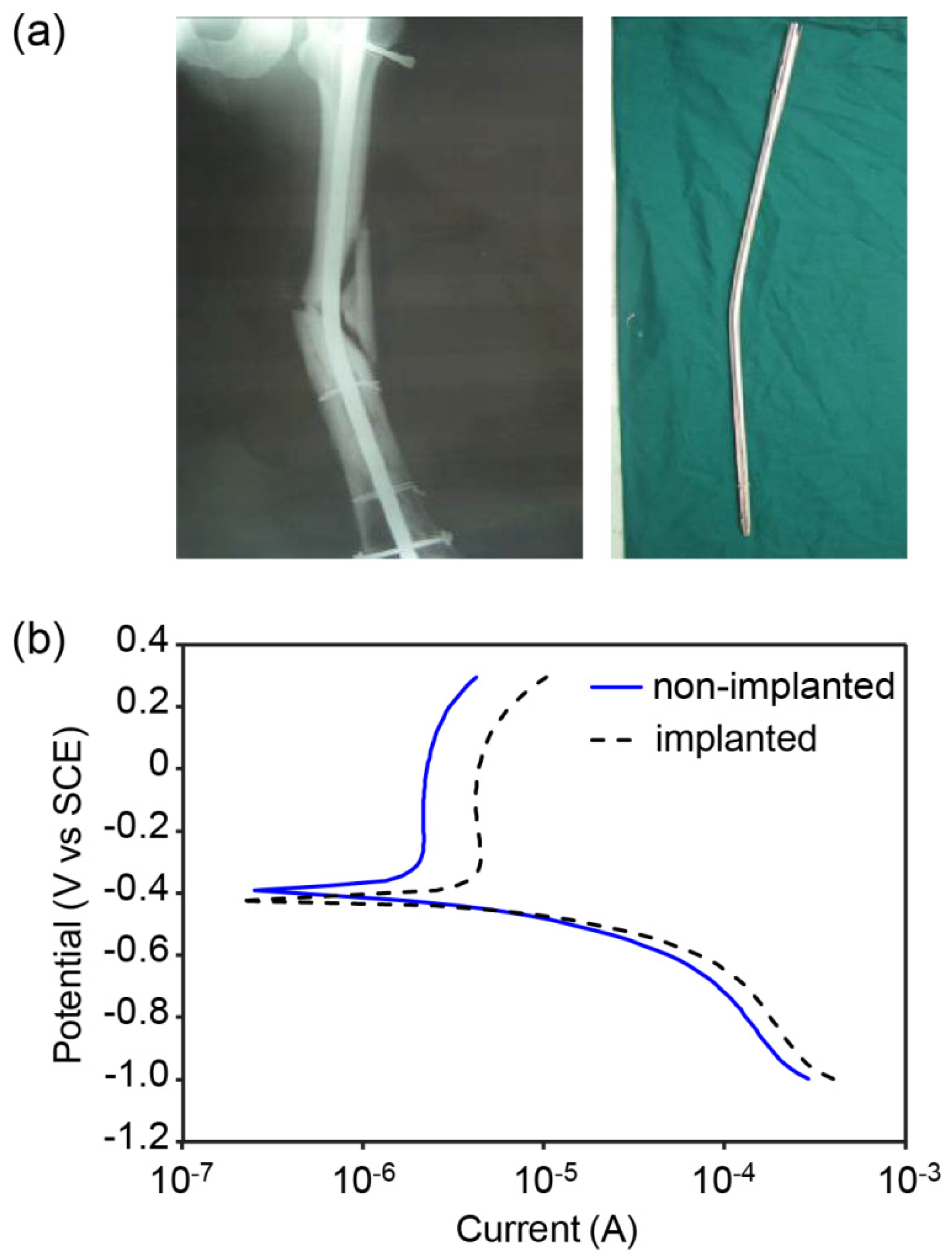
2.1. Case I, Bio-environmental Attack


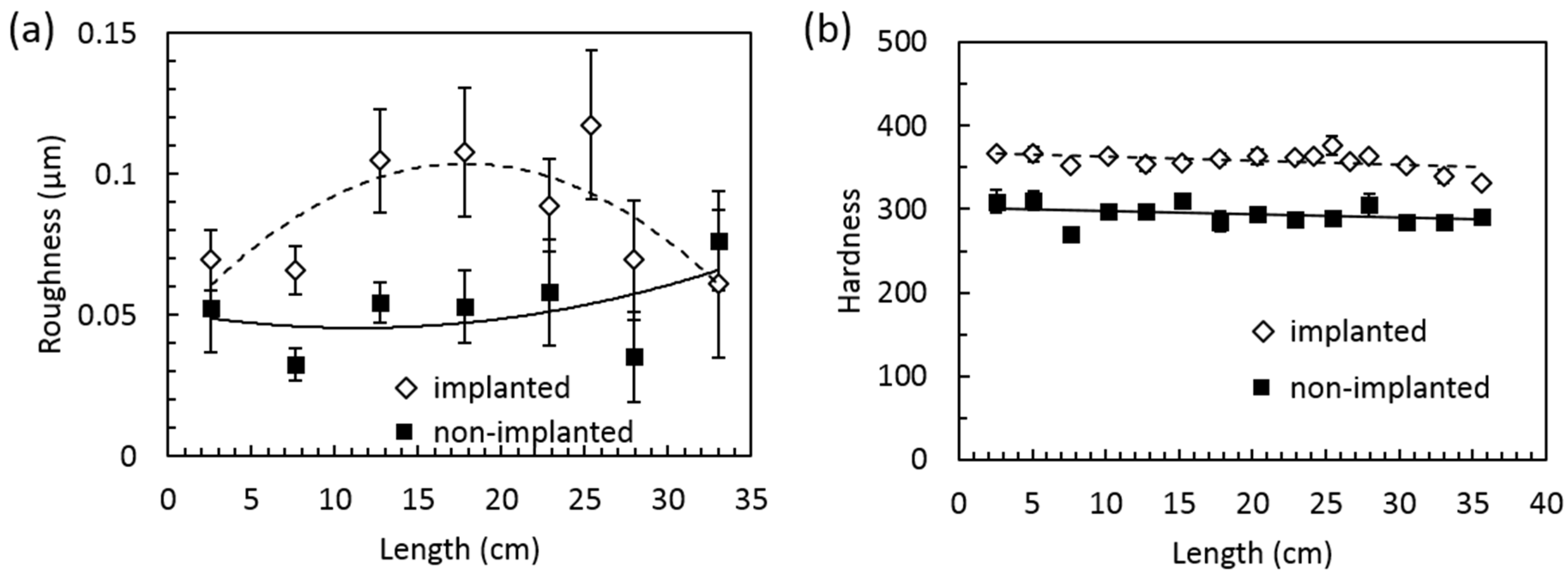
2.2. Case II, Surface Degradation


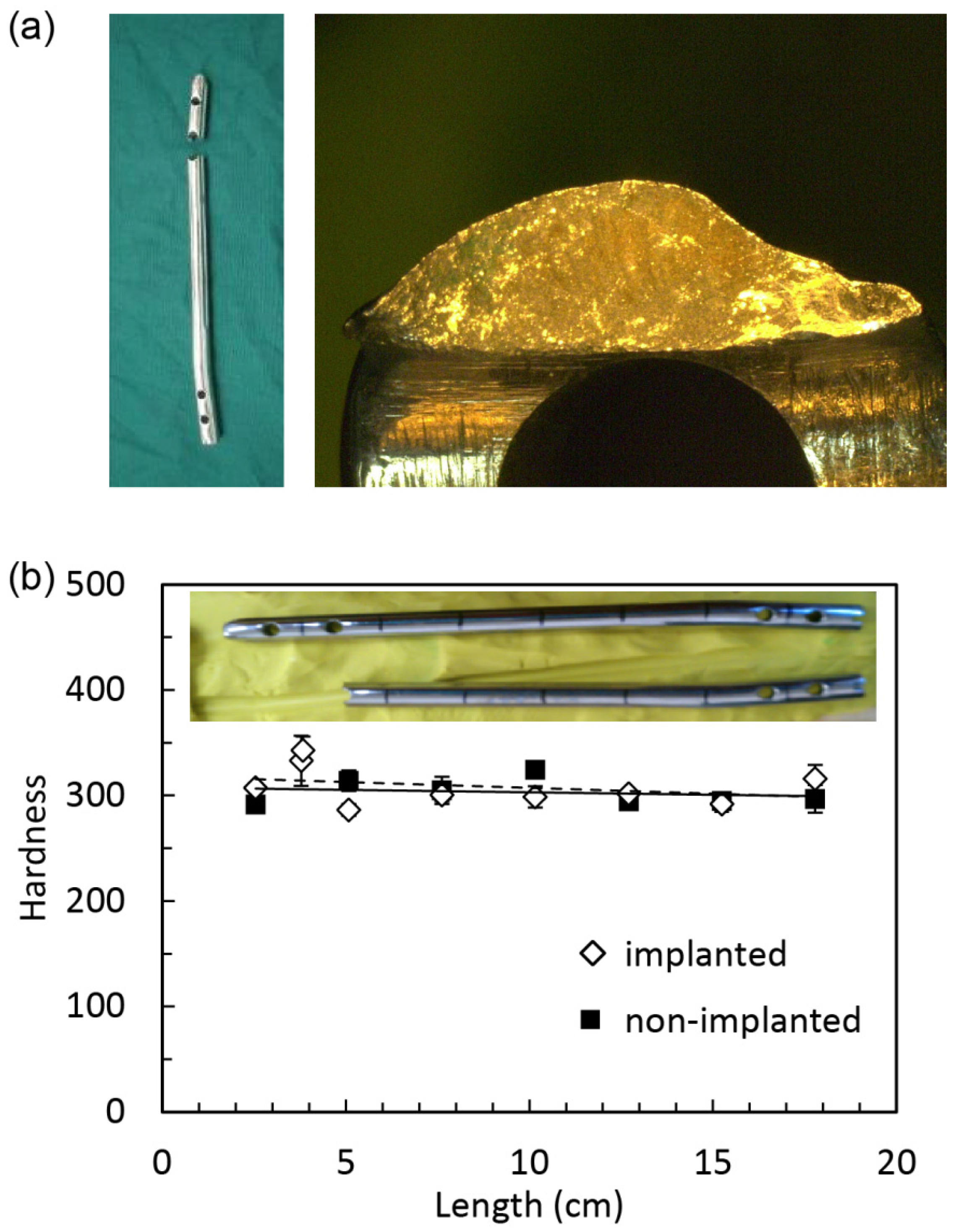
2.3. Case III, Fatigue

3. Experimental Procedure
3.1. Materials
3.2. Gamry Reference 600 Potentiostat Machine and Equipment
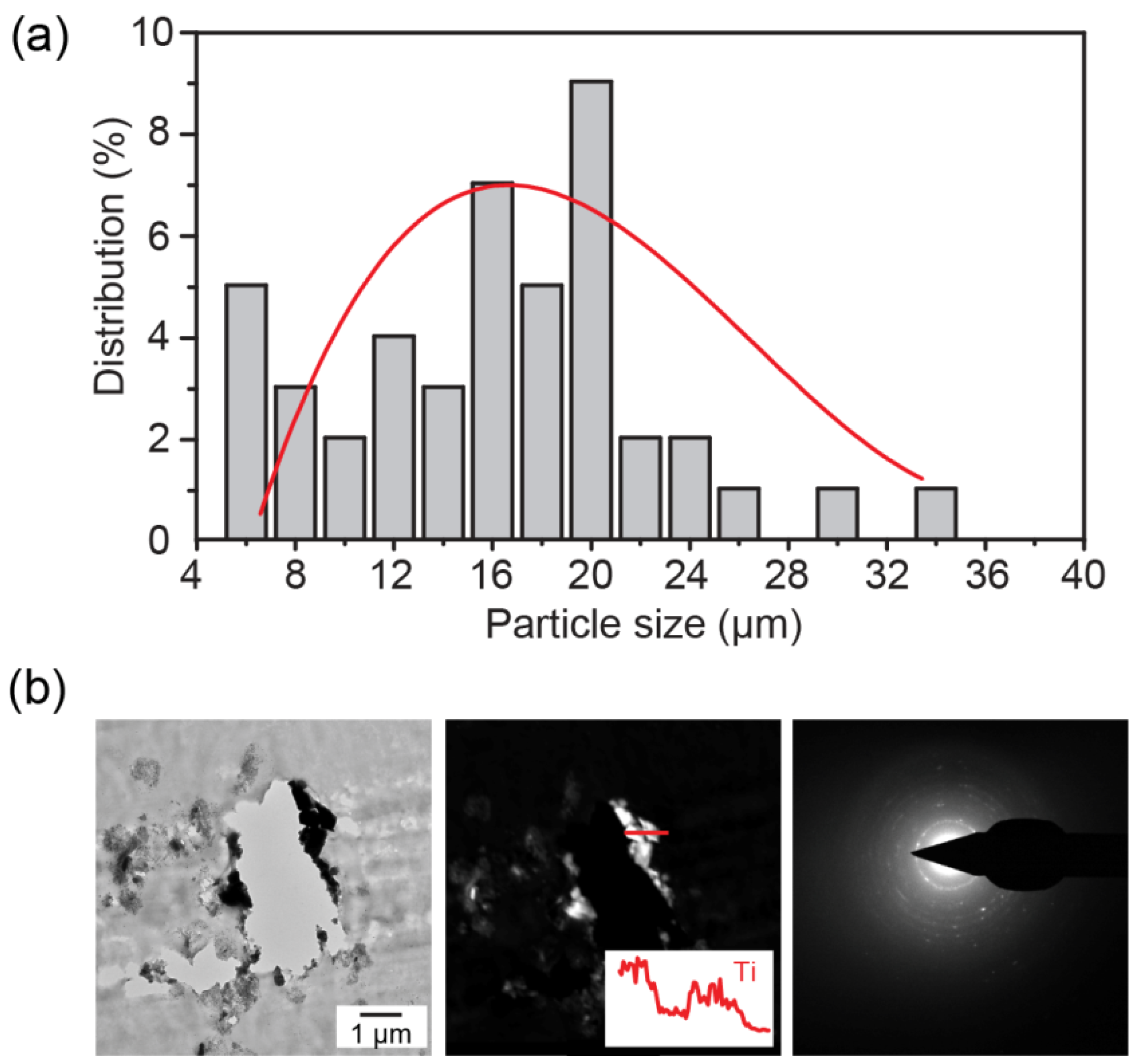
3.3. Particle Analysis
3.4. Surface Roughness and Micro-Hardness Analysis
4. Remarks
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lieberman, J.R.; Friedlaender, G.E. Bone Regeneration and Repair: Biology and Clinical Applications; Humana Press Inc.: Secaucus, NJ, USA, 2007; pp. 21–25. [Google Scholar]
- Ratner, B.D.; Hoffman, A.S.; Schoen, F.J.; Lemons, J.E. Biomaterials Science: An Introduction to Materials in Medicine; Academic Press: Waltham, MA, USA, 2013; pp. 855–859. [Google Scholar]
- Manivasagam, G.; Dhinasekaran, D.; Rajamanickam, A. Biomedical implants: Corrosion and its prevention—A review. Recent Patents Corros. Sci. 2010, 2, 40–54. [Google Scholar] [CrossRef]
- Williams, D. Tissue-biomaterial interactions. J. Mater. Sci. 1987, 22, 3421–3445. [Google Scholar] [CrossRef]
- Gotman, I. Characteristics of metals used in implants. J. Endourol. 1997, 11, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.F. Biocompatibility of Clinical Implant Materials; CRC Press: Boca Raton, FL, USA, 1981; pp. 9–98. [Google Scholar]
- Neale, S.D.; Haynes, D.R.; Howie, D.W.; Murray, D.W.; Athanasou, N.A. The effect of particle phagocytosis and metallic wear particles on osteoclast formation and bone resorption in vitro. J. Arthroplast. 2000, 15, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Cobelli, N.; Scharf, B.; Crisi, G.M.; Hardin, J.; Santambrogio, L. Mediators of the inflammatory response to joint replacement devices. Nature Rev. Rheumatol. 2011, 7, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Nine, M.J.; Choudhury, D.; Hee, A.C.; Mootanah, R.; Osman, N.A.A. Wear debris characterization and corresponding biological response: Artificial hip and knee joints. Materials 2014, 7, 980–1016. [Google Scholar] [CrossRef]
- Minoda, Y.; Kobayashi, A.; Iwaki, H.; Miyaguchi, M.; Kadoya, Y.; Ohashi, H.; Yamano, Y.; Takaoka, K. Polyethylene wear particles in synovial fluid after total knee arthroplasty. Clin. Orthop. Res. 2003, 410, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Doorn, P.F.; Campbell, P.A.; Worrall, J.; Benya, P.D.; McKellop, H.A.; Amstutz, H.C. Metal wear particle characterization from metal on metal total hip replacements: Transmission electron microscopy study of periprosthetic tissues and isolated particles. J. Biomed. Mater. Res. 1998, 42, 103–111. [Google Scholar] [CrossRef]
- Liang, H.; Shi, B.; Fairchild, A.; Cale, T. Applications of plasma coatings in artificial joints: An overview. Vacuum 2004, 73, 317–326. [Google Scholar] [CrossRef]
- Shi, B.; Ajayi, O.O.; Fenske, G.; Erdemir, A.; Liang, H. Tribological performance of some alternative bearing materials for artificial joints. Wear 2003, 255, 1015–1021. [Google Scholar] [CrossRef]
- Feng, F.; Zhou, Y.; Yun, H.; Rocha, A.; Polcar, T.; Cvrcek, L.; Liang, H. Potential application of a Ti–C:H coating in implants. J. Am. Ceram. Soc. 2011, 95, 2741–2745. [Google Scholar] [CrossRef]
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Y.; Perkins, L.A.; Wang, G.; Zhou, D.; Liang, H. Bio-Environment-Induced Degradation and Failure of Internal Fixation Implants. J. Funct. Biomater. 2015, 6, 1012-1020. https://doi.org/10.3390/jfb6041012
Zhou Y, Perkins LA, Wang G, Zhou D, Liang H. Bio-Environment-Induced Degradation and Failure of Internal Fixation Implants. Journal of Functional Biomaterials. 2015; 6(4):1012-1020. https://doi.org/10.3390/jfb6041012
Chicago/Turabian StyleZhou, Yan, Luke A. Perkins, Guodong Wang, Dongsheng Zhou, and Hong Liang. 2015. "Bio-Environment-Induced Degradation and Failure of Internal Fixation Implants" Journal of Functional Biomaterials 6, no. 4: 1012-1020. https://doi.org/10.3390/jfb6041012