1. Introduction
Dental caries, known as tooth decay, is among the most prevalent diseases worldwide [
1]. It is caused by internal factors, such as saliva secretion and components, nutritional and hormonal status, microbial flora colonizing the teeth, and tooth surface morphology and external factors, such as oral hygiene, fluoride availability, and diet [
2]. Dental caries causes pain, and may result in serious infection, hospitalization, and fatality under extreme circumstances [
3]. Bacteria, such as
Streptococcus mutans, exist within plaque buildup and process fermentable carbohydrates to produce weak acids [
4]. These acids cause calcium, carbonate, and phosphate ions to leach out of the enamel and dentine phases of the tooth, weakening the mineral and resulting in decay [
4,
5]. This process can be reversed by buffering the oral environment and restoring it to its original pH; saliva being an effective natural buffer [
1]. Demineralization and remineralization occur in a continuous cycle; if the pH is not restored or if the ions needed for remineralization are not available, demineralization dominates, resulting in lesions, and subsequently, cavities [
6].
Dentifrices are used to impede the erosion of the tooth surface [
7]. A dentifrice is a preparation that is generally used with a toothbrush in order to clean or polish teeth [
8]. Modern dentifrices often claim various beneficial effects, including plaque removal, anti-caries, and anti-bacterial effects and remineralization [
8]; the latter promoted by fluoride compounds, as well as strontium and potassium compounds [
7,
9]. Stannous fluoride (SnF
2), an ingredient in many toothpastes, can form complexes resistant to acid attack in vitro [
10,
11] as well as in situ [
12], through the deposition of a tin-rich surface on the enamel [
7]. Zinc fluoride (ZnF
2), another common ingredient in toothpaste, can provide the antibacterial action of zinc in addition to the cariostatic effect of fluoride [
11,
13].
Bioactive glasses can be formulated to deliver therapeutic ions that may bond with bone, initiate remineralization, and provide antibacterial effects [
14,
15,
16]. 45S5 Bioglass
® was the first inorganic material designed to bond with bone which did not form scar tissue upon implantation in rat femurs [
14,
17,
18]. Bioactive glasses can be doped with ions such as strontium (Sr
2+) and fluoride (F
−), which release from the glass to promote remineralization upon degradation [
19,
20,
21]. Antibacterial agents, such as silver and zinc, can also be incorporated into the glass phase [
22,
23]; their release minimizing further decay.
Incorporation of bioactive glasses into dentifrices has been reported in the literature, proving the efficacy of these glasses in occluding dentinal tubules to treat or prevent demineralization [
24]. NovaMin™, a phosphosilicate-based bioactive glass, has been added to toothpaste, and has been shown to reduce hypersensitivity [
25,
26,
27]. By embedding the glass in a dentifrice such as toothpaste, the dissolution of such glasses results in therapeutic ion release in the environment. This research evaluates the ability of silver-containing glasses, when embedded into a toothpaste, to reduce dental caries. A series of novel silver-containing bioactive glasses were synthesized, which were tailored to be a proactive solution to dental caries. Calcium and phosphorous are incorporated in order to increase remineralization effects, as both are key components of hydroxyapatite (HA); which chemically resembles the mineral component of dentine and enamel [
28]. Silver is included in ionic form as it is antibacterial [
29,
30,
31,
32,
33], even if the mechanism of action is not fully understood [
34]. Several attempts to explain the antibacterial effect of silver have been developed [
29,
34]. Silver has been reported to inactivate metabolism and inhibit bacterial growth [
35], uncouple the respiratory chain from phosphorylation [
36], interfere with membrane permeability to protons and phosphate [
37], and react with thiol groups of membrane-bound enzymes and proteins to inactivate bacteria [
34]. It is observed that the most common site of action at low concentrations is the cytoplasmic membrane [
38]. At higher concentrations, silver has been observed to interact with cytoplasmic components within the cell [
34].
By firing a series of glasses, the effect of different loadings of silver incorporated, and subsequently released in ionic form from a dentifrice, on enamel remineralization and biofilm formation can be determined.
3. Discussion
Bioactive glasses can be formulated to deliver therapeutic ions that may bond with bone, initiate remineralization, and provide antibacterial effects [
14,
15,
16]. The delivery of ions depends, to a large extent, on the network connectivity of the bioactive material. In the formulated glasses, SiO
2 is a network former contributing two bridging oxygens, whereas P
2O
5, CaO, and Na
2O are network modifiers. Ag
2O, however, is a network intermediate. Ca
2+ provides two non-bridging oxygens, while Na
+ provides one non-bridging oxygen per Na
+ ion. Recent work by Hill et al. has shown that P
2O
5 functions as an orthophosphate (Q
0) modifier, contributing three non-bridging oxygen per PO
43− ion [
39,
40]. However, since Ag
+ ions can function as a network former under certain circumstances, network connectivity has been calculated for the case of Ag
+ as a network modifier and as a network former.
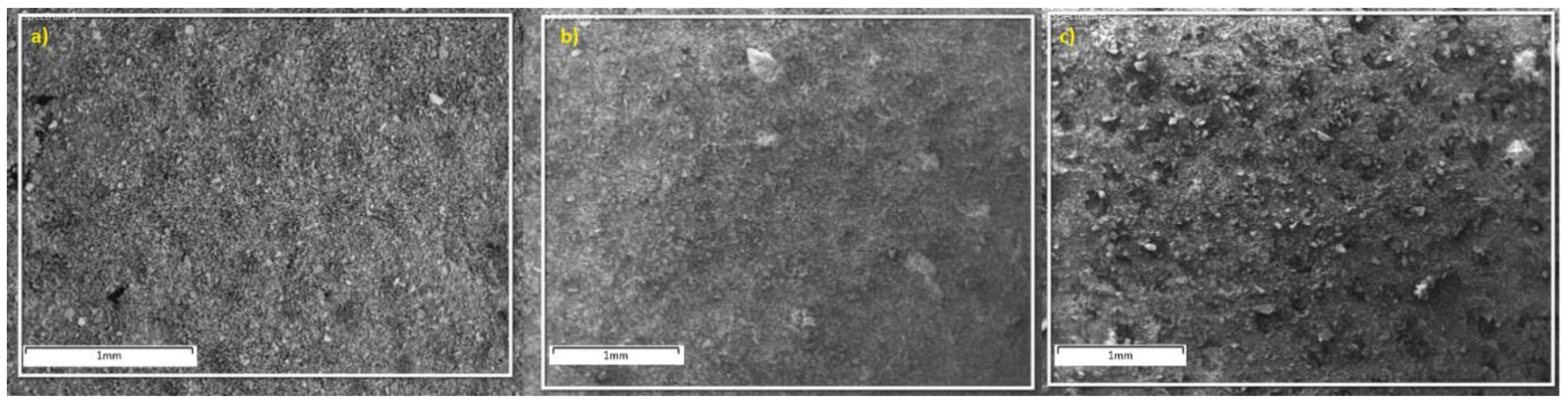
Particle sizes were also evaluated. Ideally, the particle sizes are required to be below 20 µm as smaller particle sizes promote faster dissolution due to their greater specific surface area [
41]. This allows for the particles to degrade faster, resulting in quicker release of therapeutic ions [
42]. The average particle diameter for all glasses was found to be approximately 4–5 µm. This is close to the 3 µm particle size that Mneimne et al. indicate is favorable so that the glass may enter the dentinal tubules, and ultimately, reduce dentine hypersensitivity [
43], and as these glasses were designed and proven to be degradable (
Section 2.3, Solubility studies), the 4–5 µm diameter would reduce and fit without Mneimne et al.’s criteria. Precipitation of apatite inside the tubules would occlude them and decrease sensitivity. Results show that particle sizes for all glasses are comparable, which means that any changes observed in the glasses’ behavior may be attributed to their different compositions and not to their particle size. SEM images confirmed that all compositions have similar particle sizes. However, morphology, on the small sample size examined, appeared different; Si-05 appears to be more granular and has sharper edges in its particles compared to the more homogeneous scans of Si-Control and Si-02.
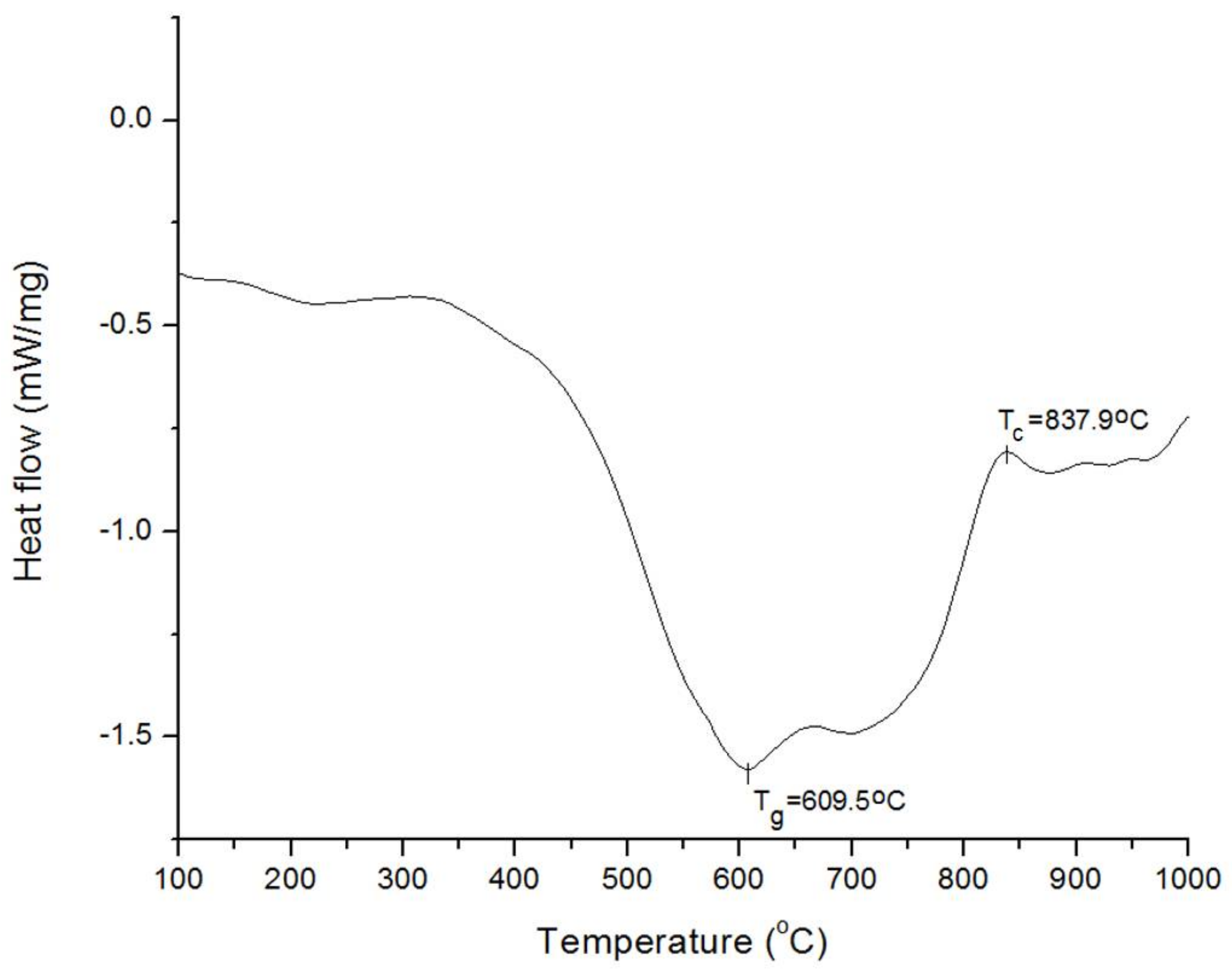
DSC results show that Tg was not significantly affected by the inclusion of Ag2O in the glass network, whereas an increase in Tc was first observed at 0.2 mol % Ag2O, with a decrease below the Tc of the control glass for 0.5 mol % Ag2O.
EDX traces confirm that all glass compositions were close to the reagent amounts fired in the crucible. This confirms that the glass thoroughly melted during the firing process, and an increase in silver content is also observed from Si-02 to Si-05.
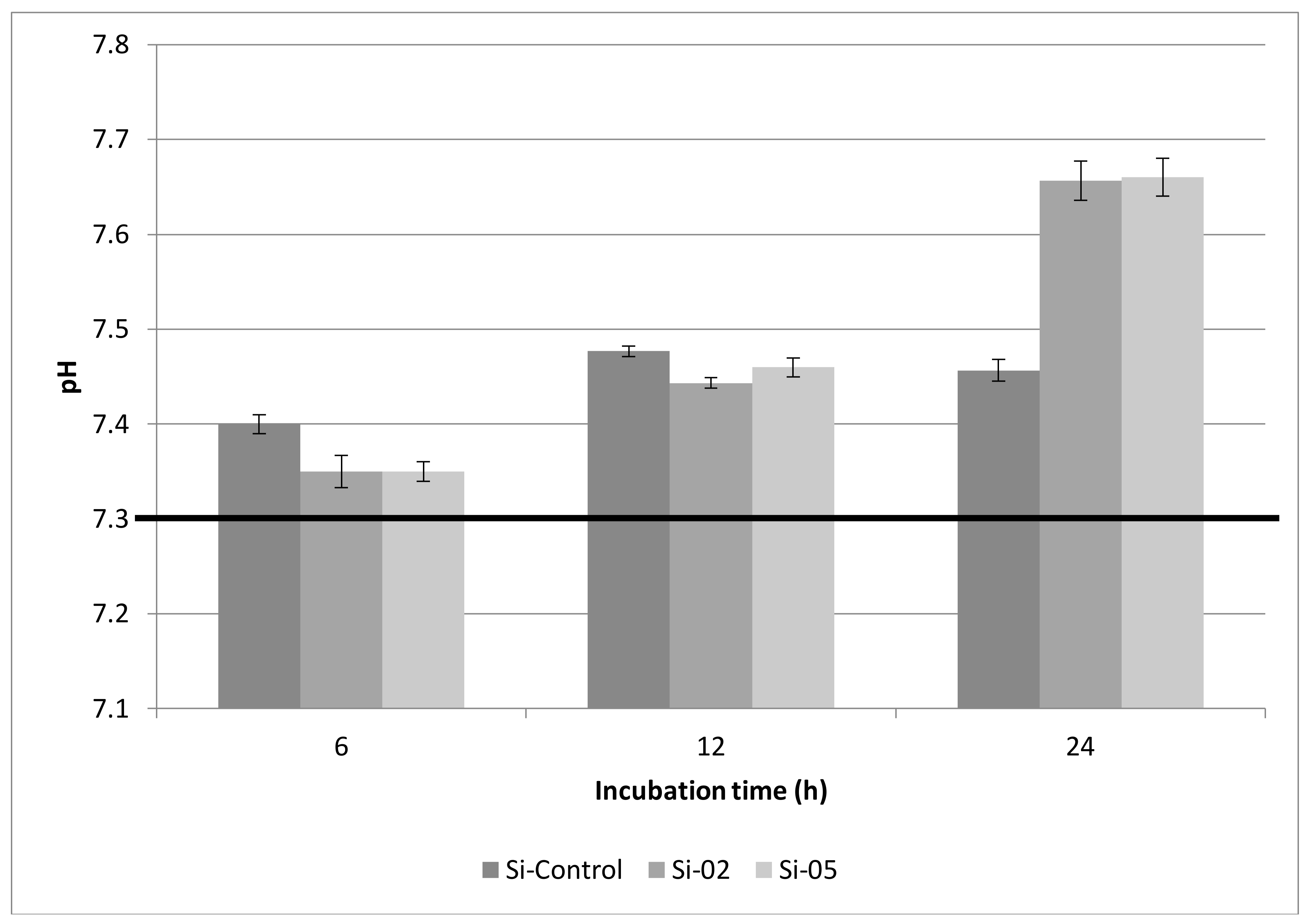
Based on the pH results, it can be postulated that bioactive glasses can increase the pH of an aqueous solution, such as Tris buffer, upon dissolution. This facilitates apatite formation but can also cause a pH rise too great for the oral environment; an oral pH greater than 7.5 can irritate the oral mucous membranes [
43,
44]. The Tris buffers containing the Si-02 and Si-05 compositions exhibited a pH of 7.35 at 6 h, while the solution containing Si-Control shows a higher pH rise at 7.4. These values were not determined to be significantly different at
p < 0.05. After 12 h, the pH responses of the solutions are 7.48, 7.44, and 7.46 for Si-Control, Si-02, and Si-05, respectively, indicating that the advantage gained by the early rise in pH of the Tris solution due to the control glass is lost over longer time frames. Indeed, by 24 h, solutions containing Si-02 and Si-05 both show a pH of 7.66 while the solution containing Si-Control shows a pH of 7.46. This compares favorably with other bioactive glasses in aqueous solution. Brauer et al. found the pH response of a simulated body fluid (SBF) solution containing fluoridated bioactive glass reached 7.6 after 24 h, but plateaued at 7.8 shortly afterward (from day 3 to the end of the experiment at 14 days) [
44]. Tris buffer solutions containing Si-02 and Si-05 both reached the same pH after 24 h, 7.66, while the solution containing Si-Control did not show a significant pH rise from 7.48 after 12 h. Time frames greater than 24 h were not examined, as they were not deemed relevant to the application of toothpaste in the oral environment; it is unlikely that the ions deposited from the degrading glass powders would remain in the mouth after a day’s consumption of liquids diluting the contents of the mouth.
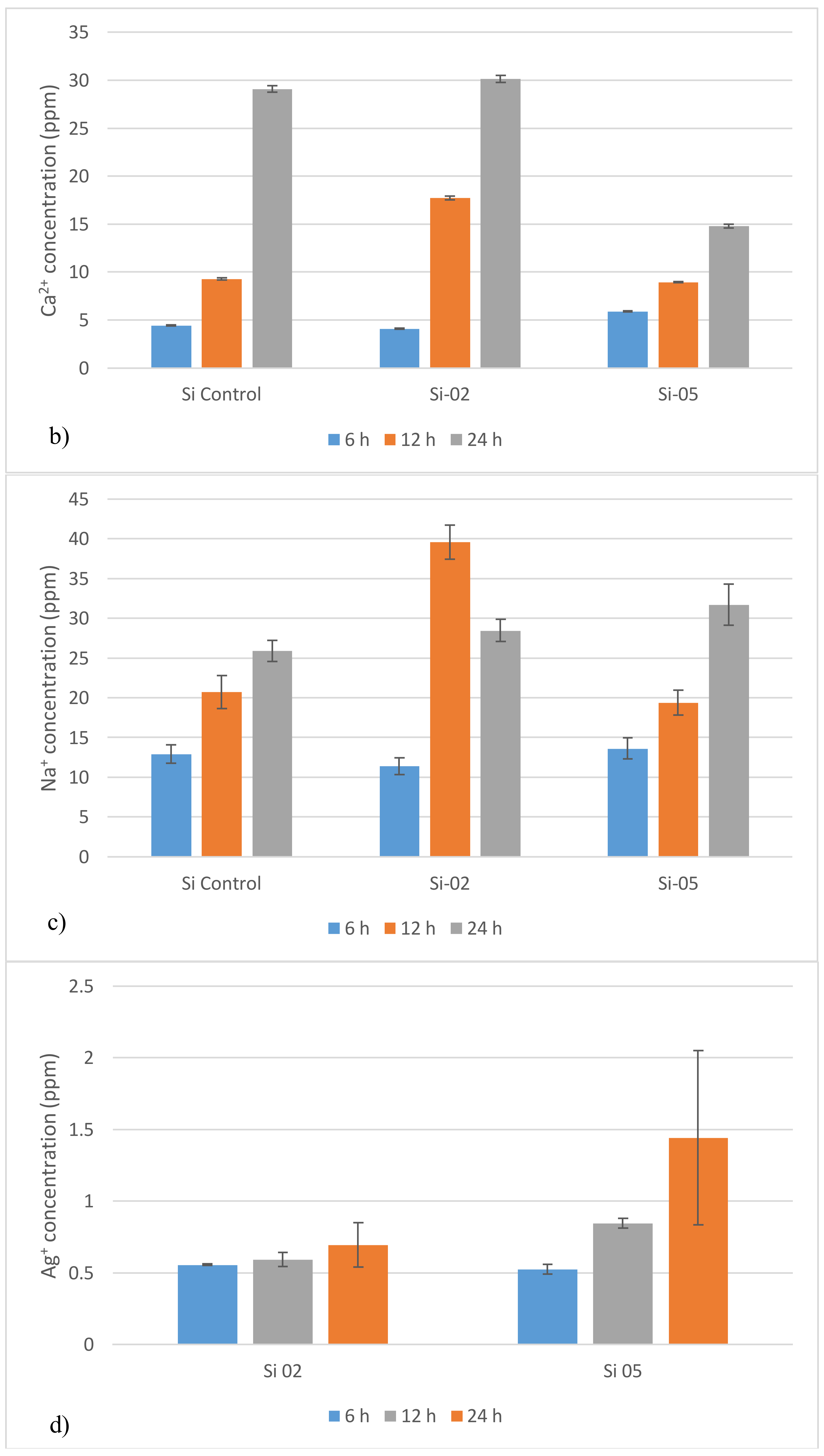
These glasses were designed with rapid ion release in mind, and it was observed that, after 12 h, the release rate accelerated. Si-02 releases Ag
+, on average, 2.5 times faster after 12 h, while Si-05 releases Ag
+ on average 1.5 times faster after 12 h. The incorporation of silver into the network structure changes the more linear response of the control composition into an accelerating one, although with a slower initial response time. This is due to the complex nature of the network structure when silver is incorporated. As silver oxide is added at the expense of silica, a network modifier is added at the expense of a network former, which should increase bioactivity and solubility of the glass as bridging oxygens are being lost and replaced with non-bridging oxygens facilitating a greater release of cations, specifically sodium and calcium ions, which are basic [
45,
46,
47], and will produce a pH rise. This would disrupt the dissolution mechanism and promote remineralization. However, the initial lag before the 12 h acceleration indicates that the cations are not exchanged as readily during the early stages of dissolution. The complex network may take longer to degrade, and favors dissolution of its formers more than its modifiers. This trend holds up when compared with the ion release profiles obtained in this study. The larger silver content yielded higher initial release volumes, but smaller release rates over time, leading to lower cumulative final release volumes. Interestingly, Si-Control displayed ion release volumes either between the two silver-containing compositions or closer to Si-02 ion profiles. Si-05 releases less silver ions initially, but greater quantities of all other ions when compared with Si-02 after 6 h, with the exception of sodium. However, over time, silver ion release rates increased rapidly for Si-05 while Si-02 released silver ions at a constant rate. Si-02 exhibited higher ion release volumes than Si-05 after 24 h for calcium. It was not possible to measure Silica release, but it may be useful in further explaining how the network degradation functioned as silica was the backbone of the network.
To measure the ion release kinetics of an alkali-silicate glass, the heterogeneous model was used [
48,
49], which assumes two stages in ionic release: first, the extraction of alkali and silica varies with the square root of time with the exchange of alkali with protons in solution dominating the glass dissolution, then, second, the ion extraction is linear with time. To confirm dissolution behavior under the heterogeneous model, the total silver ion concentration was graphed against the square root of the time, and a linear regression was employed. The correlation coefficient (R2) was above 0.95 for both Si-02 and Si-05 compositions, confirming the model. The network is expected to be complex, formed by a backbone of SiO
4 tetrahedra connected at the oxygen atoms to form a 3D network. However, the presence of alkali species breaks up the network continuity, hence increasing dissolution, as oxygen atoms no longer bridge to the next tetrahedra, but to an alkali ion instead. As silver ions were added at the expense of silica ions, this would further reduce the network connectivity as network formers were replaced with network modifiers. Ion release rates should be seen to be higher in Si-05 than Si-02, as well as being higher in Si-02 than Si-Control. While this was observed over short time periods, with the exception of silver ion release, longer dissolution time periods favored Si-02.
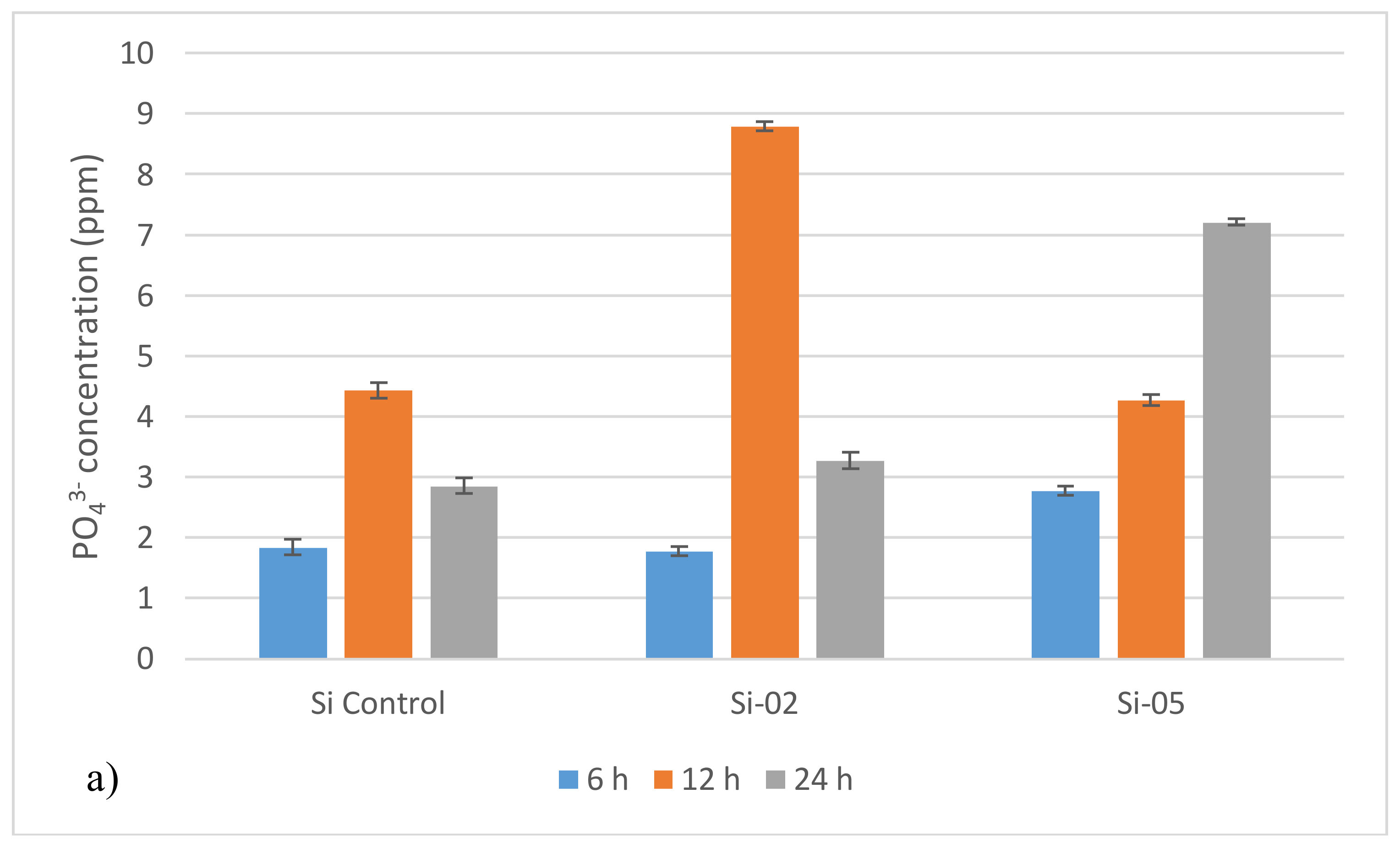
PO43− and Na+ release from Si-02 behaved differently to Ca2+ and Ag+ release as it reached a peak around 12 h and then diminished after 24 h. The decrease of PO43− and Na+ over longer time periods is assumed to be due to a measurement error. This conclusion is based on the fact that phosphorous content is low (3 mol %), and is not expected to release around 9 ppm after 12 h. This will be further investigated in future studies which would focus on pH and ion release of these materials when matured in deionized water, simulated body fluid, and Tris buffer.
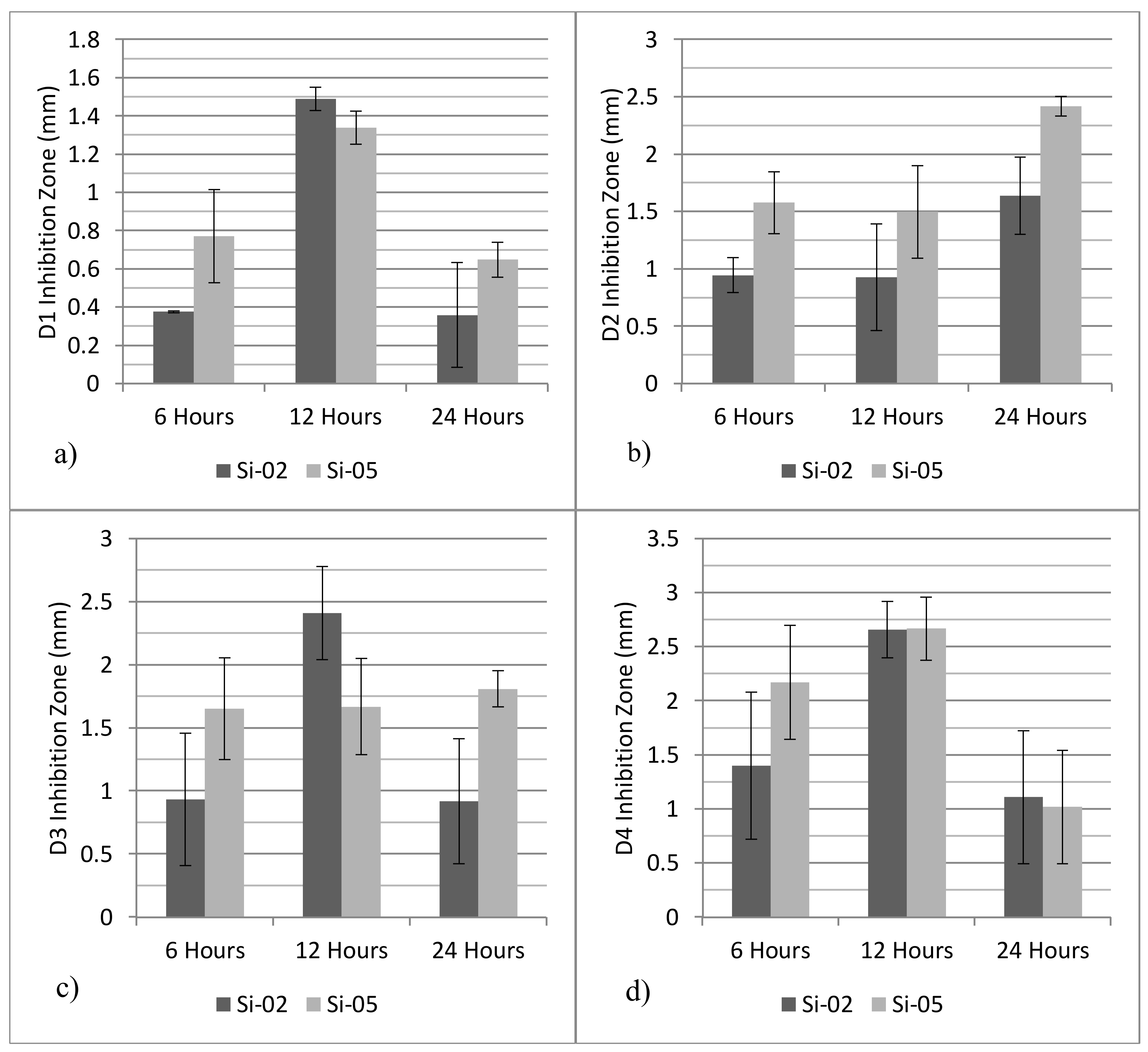
The inhibition zones against oral bacteria show that Si-05 exhibits a larger inhibition zone against D2 and D3 strains after 24 h, with statistically similar inhibition zones measured for D1 and D3 strains after 24 h. Additionally, the inhibition zone increased over time for bacteria D2 and D3, whereas D1 and D4 experienced a dip in the inhibition zone from 12 h to 24 h. Furthermore, since the control glasses did not produce any inhibition zone at any time period, the effects of pH rise can be eliminated as a potential bactericidal effect. Antibacterial studies were singularly affected by Ag
+ release as all agar discs were stored under similar conditions, and Si-Control exhibited no antibacterial response. It is therefore possible to eliminate pH as a bactericidal factor, since all compositions are known to cause similar pH rises. Referring to bacterial testing results, across all time frames and all bacterial strains, Si-05 outperformed Si-02 in its bactericidal efficacy, which further indicates that silver is the lone bactericidal agent. Silver is known to have wide ranging antibacterial properties; it is believed that DNA stops being able to replicate and proteins become inactive after contact with Ag
+ [
49]; additionally, positively charged silver ions induce an antibacterial effect through electrostatic attraction between negative charged cell membrane of the microorganism and the silver ions [
50].
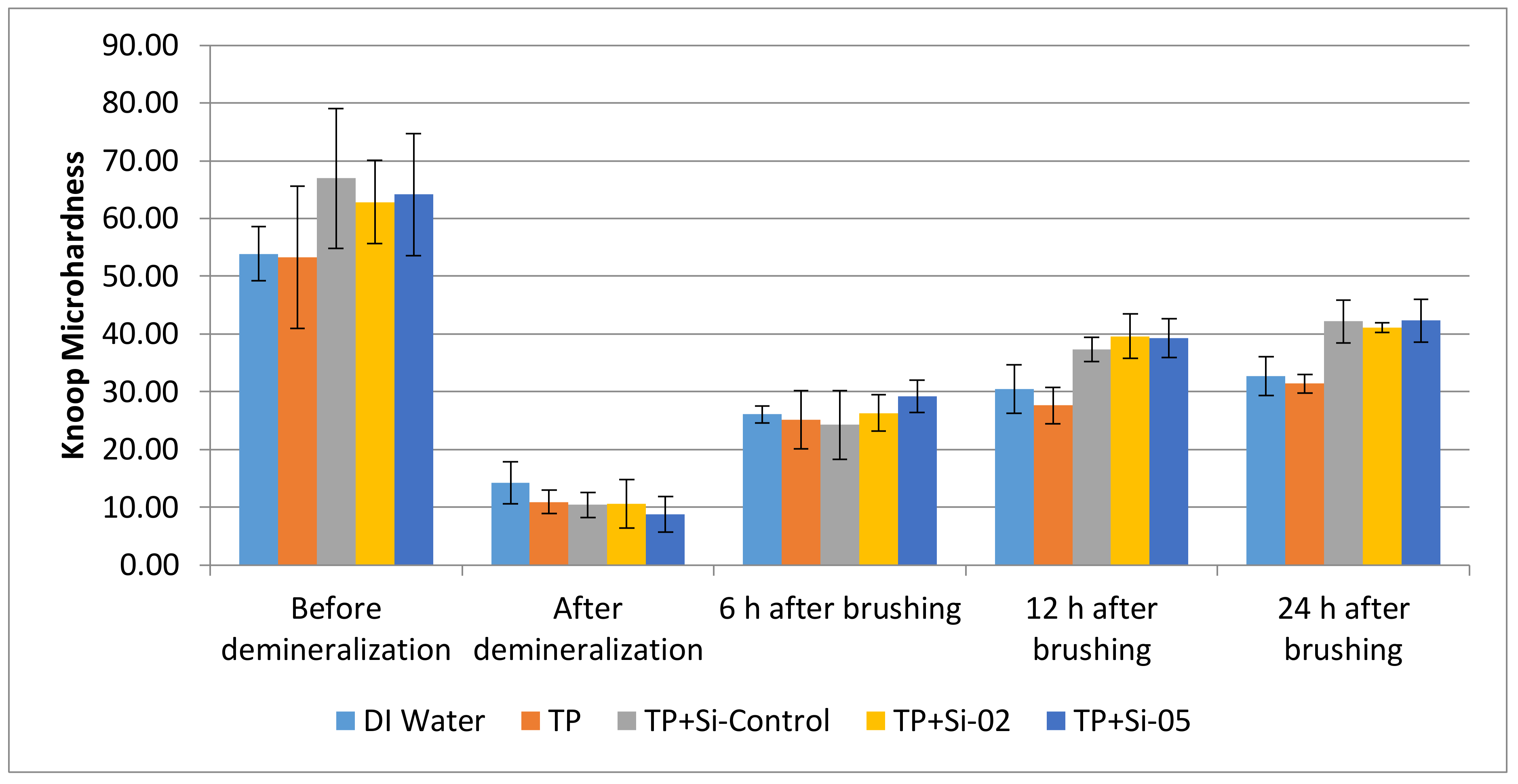
Demineralization and remineralization results show that the glass compositions were more effective than the controls, with the highest microhardness after 24 h belonging to toothpaste (TP) + Si-05 followed by TP + Si-Control, TP + Si-02, deionized (DI) water, and finally, TP. However, when taking into account the initial demineralization effects, TP+Si-Control, TP + Si-02 and TP + Si-05 had similar remineralization percentages. Additionally, the response was higher than just the dentifrice treatment alone, indicating that the glass had a positive effect to the mineralization treatments.
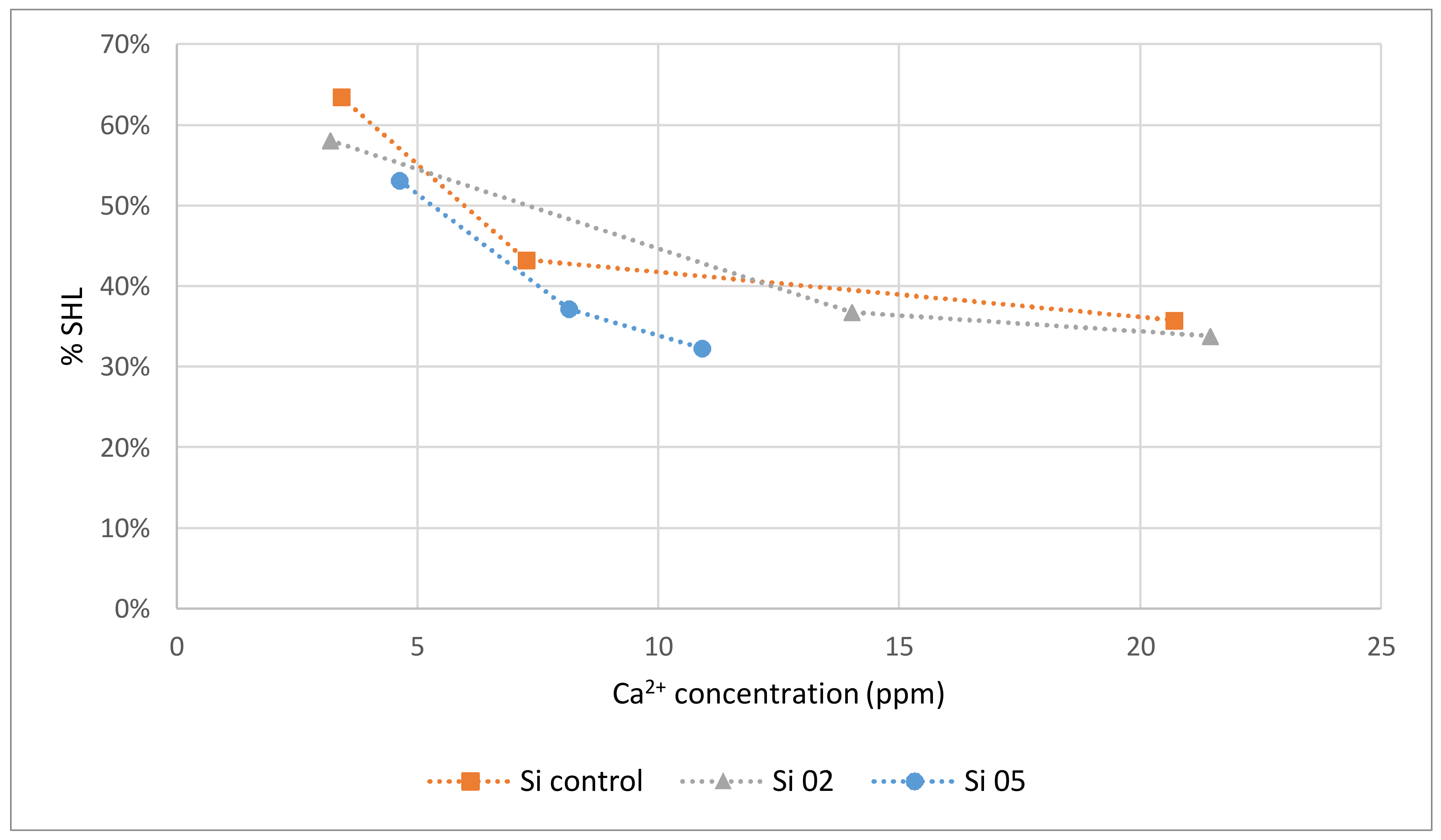
Referring to demineralization and remineralization results, all three glasses significantly remineralized enamel after 24 h compared to the demineralized samples. As Si-02 released the greatest amount of calcium and phosphorous after 12 h (17.7 ppm and 8.79 ppm, respectively), samples treated with Si-02 should have exhibited the greatest degree of remineralization at that time frame, which is consistent with the results; from 12 h to 24 h, remineralization of the teeth treated with the toothpaste embedded with Si-02 decreased from 37 to 34% surface hardness loss (%SHL). This study shows that higher Ca
2+ release resulted in a low %SHL (which is inversely proportional to the % remineralization). There was an upper limit to the amount of remineralization possible after demineralization observed in this experiment after 24 h, which is approximately 34%SHL. To compare, a toothpaste containing 1100 ppm fluoride exhibited a maximum of 38%SHL after four 7-day phases of demineralization/remineralization cycles [
51]. Percentage hardness losses for enamel treated with over the counter bleaching agents and then stored in artificial saliva range from 12–40%, according to Zantner et al. [
52], while a study by Chen et al. [
53] found an 18–32%SHL for enamel treated with fluoridated bleaching agents followed by buffer saline solution. The upper limit can be explained by calcium and phosphorous uptake into the enamel being limited by the concentration of the ions available as the remineralization process requires an excess of calcium and phosphate ions in order to take place [
54]: remineralization is hindered by insufficient Ca
2+ and PO
43− in the media. Therefore, there may simply not be enough calcium or phosphorous to repair the lesions and form HA. It is also possible that apatite crystals precipitated over the surface level of the pucks, preventing the penetration of glass deeper into the lesions and remineralization the bulk of the material. However, it is also possible that the reason the teeth did not fully remineralize is due to damage caused by stress propagation to the underlying dentin and cementum during the sample preparation process (grinding and mounting), as well as the resin holding the teeth [
55]. Since all compositions had the same amount of calcium and phosphorous, all pucks restored with the glass-loaded dentifrices are expected to reach a similar remineralizing point. While the dentifrice alone was effective at remineralizing the dentine (39 %SHL), the glass loading did increase the remineralization slightly, with a percent difference of 14% between the average glass remineralization and the toothpaste surface hardness loss. However, the difference was not statistically significant at the
p < 0.05 level.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}