

Shoe-Integrated Sensor System for Diagnosis of the Concomitant Syndesmotic Injury in Chronic Lateral Ankle Instability: A Prospective Double-Blind Diagnostic Test

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of the Shoe-Integrated Sensor System
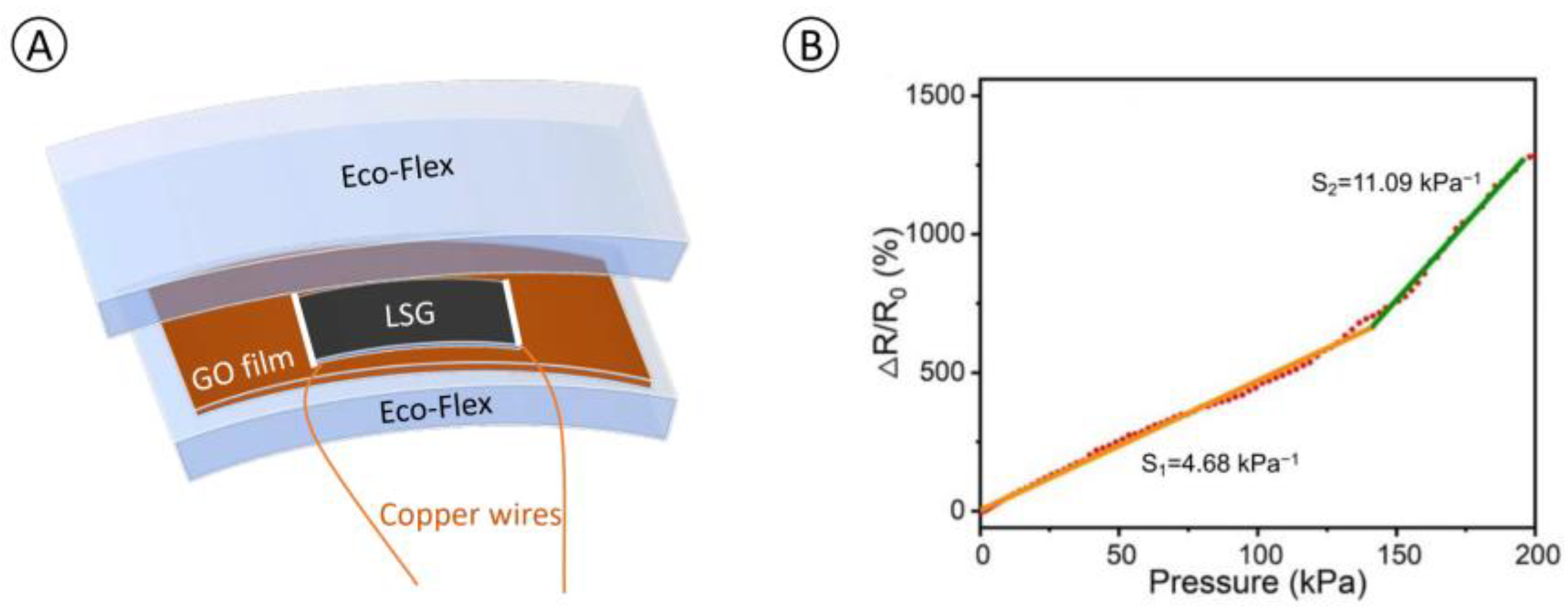
2.1.1. Development of a Graphene-Based Force Sensing Resistive (FSR) Sensor
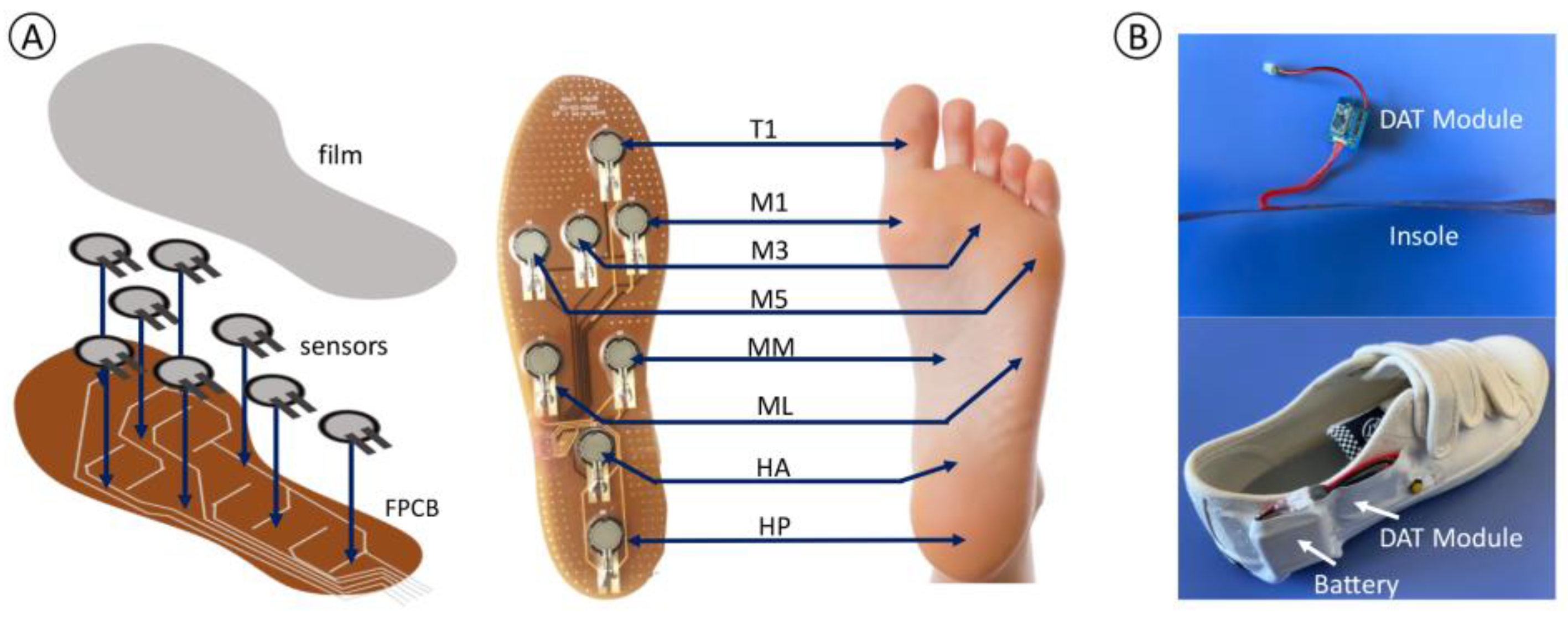
2.1.2. Method of Integration into the Shoe
2.1.3. System Hardware Information
2.1.4. System Workflow
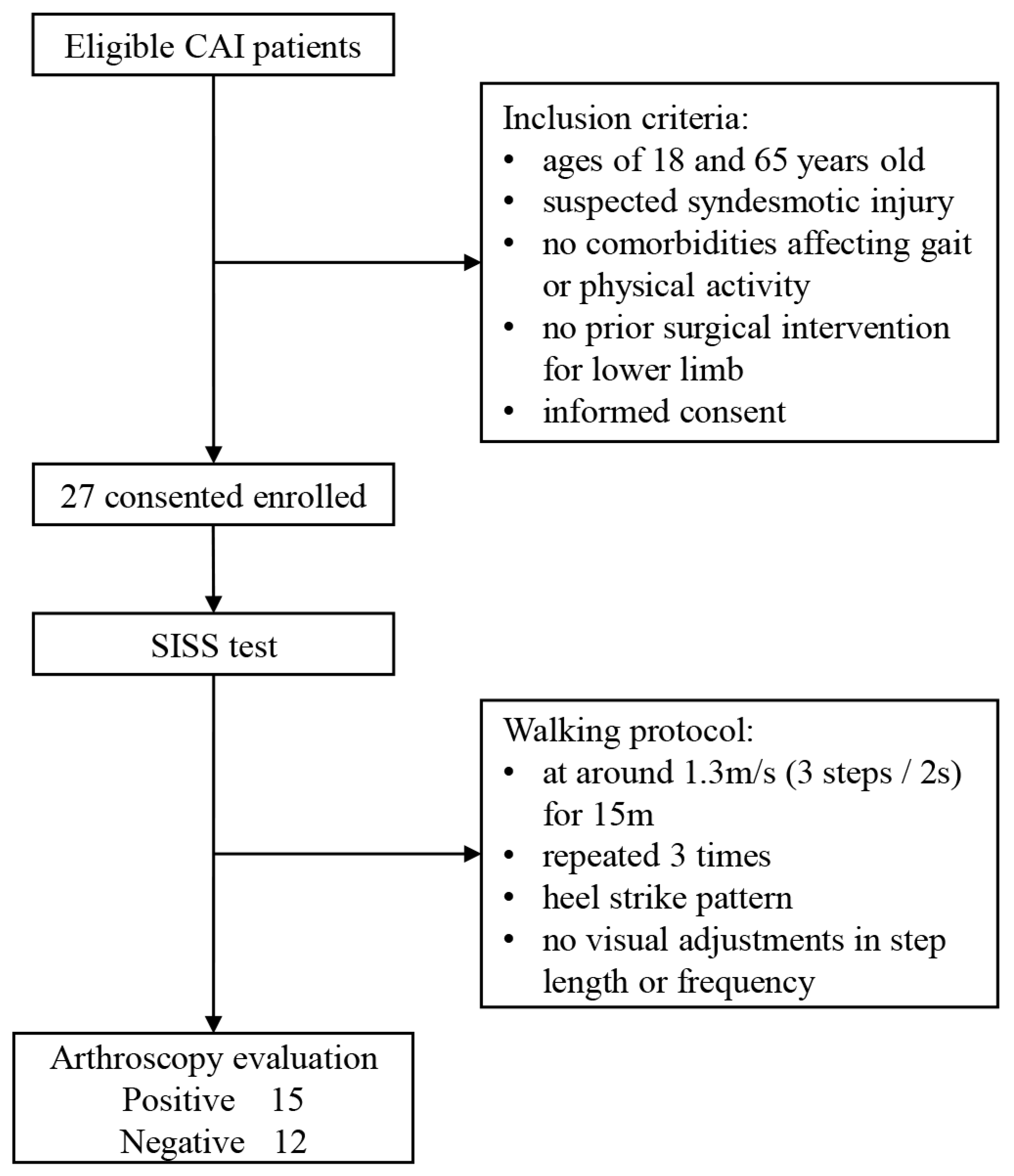
2.2. Study Design
2.2.1. Participants and Selection Criteria
2.2.2. Data Collection: Shoe-Integrated Sensor System
2.2.3. Arthroscopic Examination
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristic
3.2. Plantar Pressure Measurements
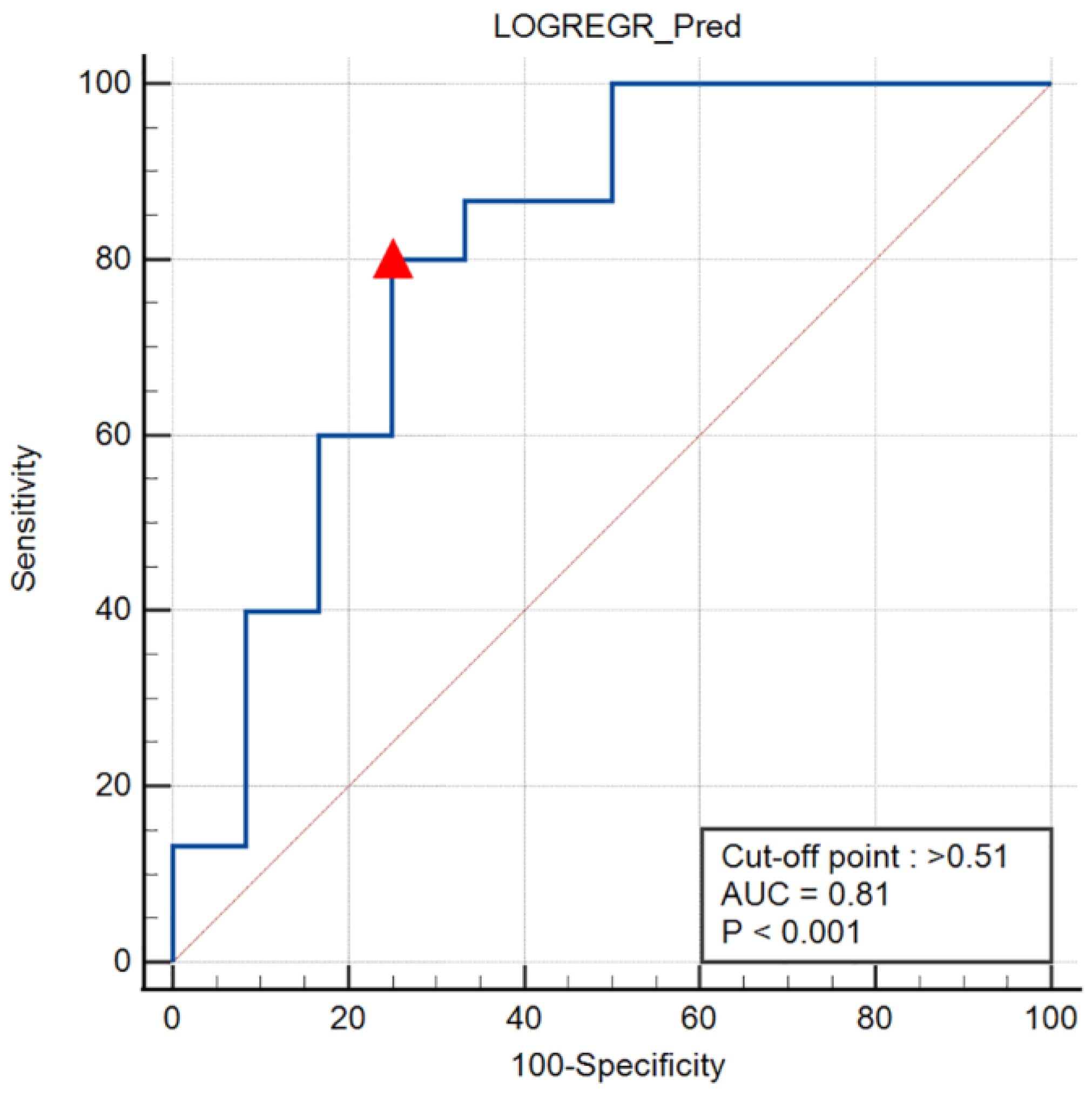
3.3. ROC Curve and Cut-Off Point
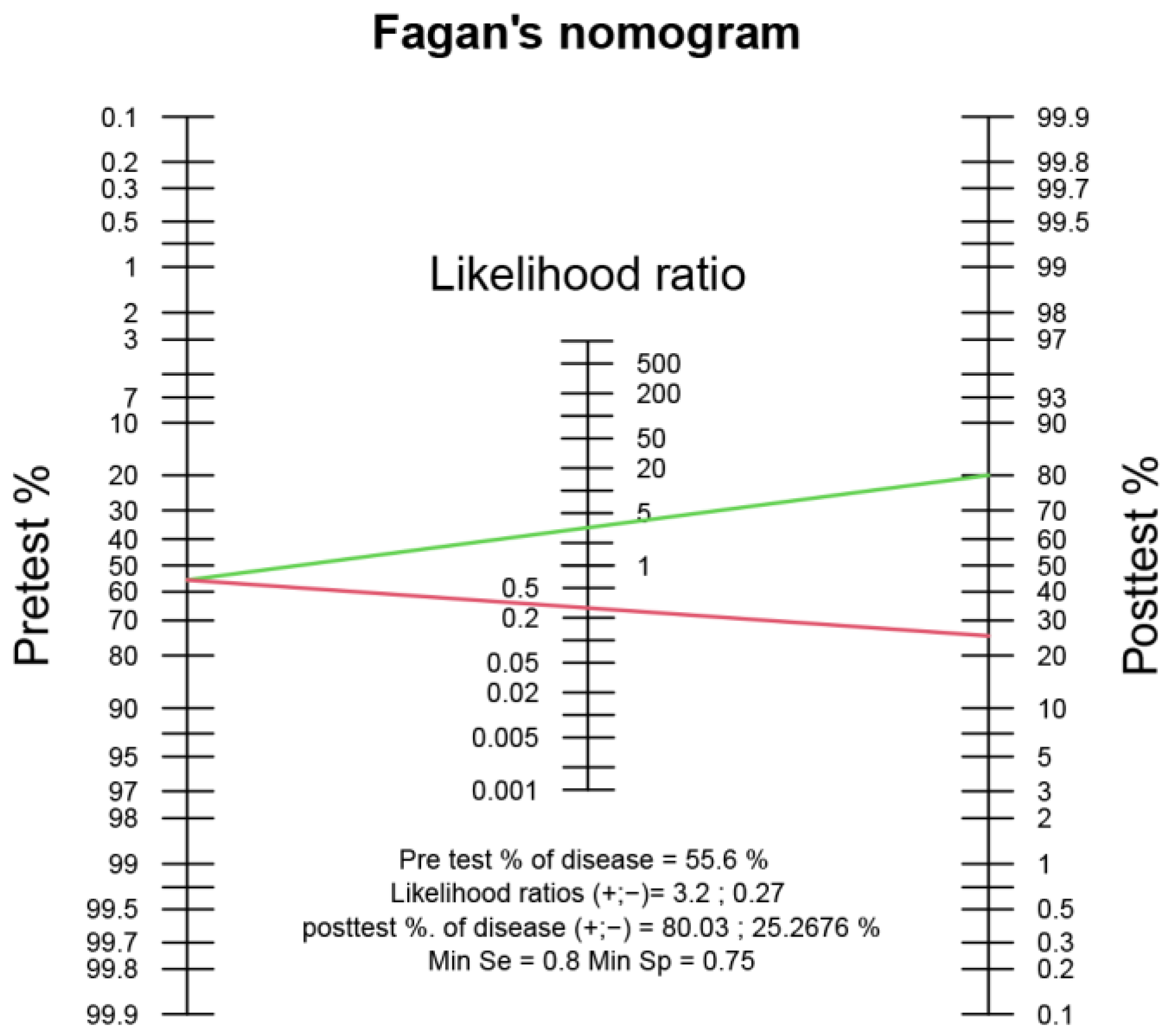
3.4. Sensitivity, Specificity, Positive and Negative Predictive Values, and Likelihood Ratios
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C. The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sport. Med. 2014, 44, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Herzog, M.M.; Kerr, Z.Y.; Marshall, S.W.; Wikstrom, E.A. Epidemiology of Ankle Sprains and Chronic Ankle Instability. J. Athl. Train. 2019, 54, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Schabrun, S.; Romero, R.; Bialocerkowski, A.; van Dieen, J.; Marshall, P. Factors Contributing to Chronic Ankle Instability: A Systematic Review and Meta-Analysis of Systematic Reviews. Sport. Med. 2018, 48, 189–205. [Google Scholar] [CrossRef]
- Clanton, T.O.; Ho, C.P.; Williams, B.T.; Surowiec, R.K.; Gatlin, C.C.; Haytmanek, C.T.; Laprade, R.F. Magnetic resonance imaging characterization of individual ankle syndesmosis structures in asymptomatic and surgically treated cohorts. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2089–2102. [Google Scholar] [CrossRef] [PubMed]
- Takao, M.; Ochi, M.; Oae, K.; Naito, K.; Uchio, Y. Diagnosis of a tear of the tibiofibular syndesmosis. The role of arthroscopy of the ankle. J. Bone Jt. Surg. Br. 2003, 85, 324–329. [Google Scholar] [CrossRef]
- Tourné, Y.; Molinier, F.; Andrieu, M.; Porta, J.; Barbier, G. Diagnosis and treatment of tibiofibular syndesmosis lesions. Orthop. Traumatol. Surg. Res. 2019, 105, S275–S286. [Google Scholar] [CrossRef]
- Sman, A.D.; Hiller, C.E.; Rae, K.; Linklater, J.; Black, D.; Nicholson, L.; Burns, J.; Refshauge, K. Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br. J. Sport. Med. 2015, 49, 323–329. [Google Scholar] [CrossRef]
- Kellett, J.J. The clinical features of ankle syndesmosis injuries: A general review. Clin. J. Sport. Med. 2011, 21, 524–529. [Google Scholar] [CrossRef]
- Han, S.H.; Lee, J.W.; Kim, S.; Suh, J.S.; Choi, Y.R. Chronic tibiofibular syndesmosis injury: The diagnostic efficiency of magnetic resonance imaging and comparative analysis of operative treatment. Foot Ankle Int. 2007, 28, 336–342. [Google Scholar] [CrossRef]
- Jiao, C.; Gui, J.; Kurokawa, H.; Tanaka, Y.; Yung, P.; Han, S.H.; Angthong, C.; Song, Y.; Hua, Y.; Li, H.; et al. APKASS Consensus Statement on Chronic Syndesmosis Injury, Part 1: Clinical Manifestation, Radiologic Examination, Diagnosis Criteria, Classification, and Nonoperative Treatment. Orthop. J. Sport. Med. 2021, 9, 23259671211021056. [Google Scholar] [CrossRef]
- Rosenbaum, D.; Becker, H.P. Plantar pressure distribution measurements. Technical background and clinical applications. Foot Ankle Surg. 1997, 3, 1–14. [Google Scholar] [CrossRef]
- Nyska, M.; Shabat, S.; Simkin, A.; Neeb, M.; Matan, Y.; Mann, G. Dynamic force distribution during level walking under the feet of patients with chronic ankle instability. Br. J. Sport. Med. 2003, 37, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Luthi, F.; Jolles, B.M.; Siegrist, O.; Najafi, B.; Aminian, K. A new ambulatory system for comparative evaluation of the three-dimensional knee kinematics, applied to anterior cruciate ligament injuries. Knee Surg. Sport. Traumatol. Arthrosc. 2006, 14, 592–604. [Google Scholar] [CrossRef]
- Patterson, M.R.; Delahunt, E.; Sweeney, K.T.; Caulfield, B. An ambulatory method of identifying anterior cruciate ligament reconstructed gait patterns. Sensors 2014, 14, 887–899. [Google Scholar] [CrossRef]
- van der Straaten, R.; De Baets, L.; Jonkers, I.; Timmermans, A. Mobile assessment of the lower limb kinematics in healthy persons and in persons with degenerative knee disorders: A systematic review. Gait Posture 2018, 59, 229–241. [Google Scholar] [CrossRef]
- Wu, Q.; Qiao, Y.; Guo, R.; Naveed, S.; Hirtz, T.; Li, X.; Fu, Y.; Wei, Y.; Deng, G.; Yang, Y.; et al. Triode-Mimicking Graphene Pressure Sensor with Positive Resistance Variation for Physiology and Motion Monitoring. ACS Nano 2020, 14, 10104–10114. [Google Scholar] [CrossRef] [PubMed]
- DuPont, R.L. The D.C. heroin epidemic: Progress report. N. Engl. J. Med. 1972, 287, 1154. [Google Scholar] [CrossRef]
- Portney, L.; Watkins, M. Chapter 27: Statistical measures of validity. In Foundations of Clinical Research: Applications to Practice, 3rd ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2009; pp. 619–658. [Google Scholar]
- Deeks, J.J.; Altman, D.G. Diagnostic tests 4: Likelihood ratios. BMJ 2004, 329, 168–169. [Google Scholar] [CrossRef]
- Deeks, J.J. Systematic reviews in health care: Systematic reviews of evaluations of diagnostic and screening tests. BMJ 2001, 323, 157–162. [Google Scholar] [CrossRef]
- Riddle, D.L.; Stratford, P.W. Interpreting validity indexes for diagnostic tests: An illustration using the Berg balance test. Phys. Ther. 1999, 79, 939–948. [Google Scholar] [CrossRef]
- Jaeschke, R.; Guyatt, G.H.; Sackett, D.L. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group. JAMA 1994, 271, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Fetters, L.; Tilson, J. Evidence Based Physical Therapy; FA Davis: Philadelphia, PA, USA, 2018. [Google Scholar]
- Luczak, T.; Burch, V.R.F.; Smith, B.K.; Carruth, D.W.; Lamberth, J.; Chander, H.; Knight, A.; Ball, J.; Prabhu, R. Closing the Wearable Gap-Part V: Development of a Pressure-Sensitive Sock Utilizing Soft Sensors. Sensors 2019, 20, 208. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, A.; Iba, K.; Murahashi, Y.; Shoji, H.; Hirota, K.; Kawai, M.; Ikeda, Y.; Imamura, R.; Kamiya, T.; Watanabe, K.; et al. Quantitative Evaluation of Ankle Instability Using a Capacitance-Type Strain Sensor. Foot Ankle Int. 2021, 42, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhang, D.; Sun, Z.; Zhou, S.; Li, W.; Li, C.; Li, W.; Tang, W.; Wang, Z.L. Active-Matrix Sensing Array Assisted with Machine-Learning Approach for Lumbar Degenerative Disease Diagnosis and Postoperative Assessment. Adv. Funct. Mater. 2022, 32, 2113008. [Google Scholar] [CrossRef]
- Goh, G.L.; Agarwala, S.; Yeong, W.Y. High resolution aerosol jet printing of conductive ink for stretchable electronics. In Proceedings of the 3rd International Conference on Progress in Additive Manufacturing (PRO-AM), Singapore, 14–17 May 2018; pp. 109–114. [Google Scholar]
- Lo, L.; Shi, H.; Wan, H.; Xu, Z.; Tan, X.; Wang, C. Inkjet-Printed Soft Resistive Pressure Sensor Patch for Wearable Electronics Applications. Adv. Mater. Technol. 2020, 5, 1900717. [Google Scholar] [CrossRef]
- Sun, J.; Sun, Y.; Jia, H.; Bi, H.; Chen, L.; Que, M.; Xiong, Y.; Han, L.; Sun, L. A novel pre-deposition assisted strategy for inkjet printing graphene-based flexible pressure sensor with enhanced performance. Carbon 2022, 196, 85–91. [Google Scholar] [CrossRef]
- Goh, G.L.; Agarwala, S.; Yong, W.Y. 3D printing of microfludic sensor for soft robots: A preliminary study in design and fabrication. In Proceedings of the 2nd International Conference on Progress in Additive Manufacturing (Pro-AM 2016), Singapore, 16–19 May 2016; pp. 177–181. [Google Scholar]
- Zhou, X.; Zhang, L.; Wang, Y.; Zhao, S.; Zhou, Y.; Guo, Y.; Wang, Y.; Liang, J.; Chen, H. Aerosol Jet Printing of Multi-Dimensional OECT Force Sensor with High Sensitivity and Large Measuring Range. Adv. Mater. Technol. 2023, 8, 2201272. [Google Scholar] [CrossRef]
- Blumenthal, T.; Fratello, V.; Nino, G.; Ritala, K. Conformal printing of sensors on 3D and flexible surfaces using aerosol jet deposition. In Nanosensors, Biosensors, and Info-Tech Sensors and Systems 2013; SPIE: Bellingham, WA, USA, 2013; Volume 8691, pp. 118–126. [Google Scholar]
- de César, P.C.; Avila, E.M.; de Abreu, M.R. Comparison of magnetic resonance imaging to physical examination for syndesmotic injury after lateral ankle sprain. Foot Ankle Int. 2011, 32, 1110–1114. [Google Scholar] [CrossRef]
- Großterlinden, L.G.; Hartel, M.; Yamamura, J.; Schoennagel, B.; Bürger, N.; Krause, M.; Spiro, A.; Hoffmann, M.; Lehmann, W.; Rueger, J.M.; et al. Isolated syndesmotic injuries in acute ankle sprains: Diagnostic significance of clinical examination and MRI. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 1180–1186. [Google Scholar] [CrossRef]
- Fallat, L.; Grimm, D.J.; Saracco, J.A. Sprained ankle syndrome: Prevalence and analysis of 639 acute injuries. J. Foot Ankle Surg. 1998, 37, 280–285. [Google Scholar] [CrossRef]
- Vosseller, J.T.; Karl, J.W.; Greisberg, J.K. Incidence of syndesmotic injury. Orthopedics 2014, 37, e226–e229. [Google Scholar] [CrossRef] [PubMed]
- Boytim, M.J.; Fischer, D.A.; Neumann, L. Syndesmotic ankle sprains. Am. J. Sport. Med. 1991, 19, 294–298. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 27 | |
|---|---|
| Age (yr) | 29.4 ± 10.2 |
| Gender | |
| Male | 14 (52%) |
| Female | 13 (48%) |
| Body mass index (kg/m2) | 24.9 ± 4.2 |
| Height (cm) | 170.1 ± 9.9 |
| Weight (kg) | 73.1 ± 15.9 |
| Beighton score | 2.2 (0–7) |
| Pain | |
| At rest (VAS 0–10) | 2.9 ± 2.0 |
| Under weight-bearing (VAS 0–10) | 4.6 ± 1.5 |
| Post-injury duration (mo) | 19 (3–72) |
| Peak Force | Ratio | |||||
|---|---|---|---|---|---|---|
| Affected | Unaffected | p | Syndesmotic Injury Group | Control Group | p | |
| T1 | 0.12 ± 0.06 | 0.13 ± 0.05 | 0.20 | 0.97 ± 0.35 | 0.97 ± 0.37 | 0.66 |
| M1 | 0.16 ± 0.05 | 0.20 ± 0.05 | 0.01 * | 0.81 ± 0.22 | 0.88 ± 0.43 | 0.24 |
| M3 | 0.23 ± 0.05 | 0.24 ± 0.04 | 0.01 * | 0.92 ± 0.14 | 0.97 ± 0.08 | 0.13 |
| M5 | 0.15 ± 0.03 | 0.16 ± 0.03 | 0.04 * | 0.93 ± 0.19 | 0.97 ± 0.12 | 0.32 |
| ML | 0.06 ± 0.03 | 0.07 ± 0.03 | 0.11 | 0.85 ± 0.27 | 1.10 ± 0.40 | 0.04 * |
| HA | 0.08 ± 0.04 | 0.08 ± 0.04 | 0.77 | 1.08 ± 0.32 | 1.05 ± 0.37 | 0.52 |
| HP | 0.20 ± 0.04 | 0.20 ± 0.05 | 0.10 | 1.01 ± 0.11 | 0.98 ± 0.15 | 0.45 |
| SISS Test Accuracy (95% CI) | |
|---|---|
| Diagnostic accuracy | 78% (95% CI 58–91%) |
| Sensitivity | 80% (95% CI 52–96%) |
| Specificity | 75% (95% CI 43–95%) |
| Positive predictive value | 80% (95% CI 59–92%) |
| Negative predictive value | 75% (95% CI 51–90%) |
| LR+ | 3.20 (95% CI 1.16–8.80) |
| LR− | 0.27 (95% CI 0.09–0.77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Guo, R.; Wang, Y.; Ma, J.; Miao, X.; Yang, J.; Zhang, Z.; Wu, X.; Ren, T.; Jiang, D. Shoe-Integrated Sensor System for Diagnosis of the Concomitant Syndesmotic Injury in Chronic Lateral Ankle Instability: A Prospective Double-Blind Diagnostic Test. Nanomaterials 2023, 13, 1539. https://doi.org/10.3390/nano13091539
Li Y, Guo R, Wang Y, Ma J, Miao X, Yang J, Zhang Z, Wu X, Ren T, Jiang D. Shoe-Integrated Sensor System for Diagnosis of the Concomitant Syndesmotic Injury in Chronic Lateral Ankle Instability: A Prospective Double-Blind Diagnostic Test. Nanomaterials. 2023; 13(9):1539. https://doi.org/10.3390/nano13091539
Chicago/Turabian StyleLi, Yanzhang, Rui Guo, Yuchen Wang, Jingzhong Ma, Xin Miao, Jie Yang, Zhu Zhang, Xiaoming Wu, Tianling Ren, and Dong Jiang. 2023. "Shoe-Integrated Sensor System for Diagnosis of the Concomitant Syndesmotic Injury in Chronic Lateral Ankle Instability: A Prospective Double-Blind Diagnostic Test" Nanomaterials 13, no. 9: 1539. https://doi.org/10.3390/nano13091539
APA StyleLi, Y., Guo, R., Wang, Y., Ma, J., Miao, X., Yang, J., Zhang, Z., Wu, X., Ren, T., & Jiang, D. (2023). Shoe-Integrated Sensor System for Diagnosis of the Concomitant Syndesmotic Injury in Chronic Lateral Ankle Instability: A Prospective Double-Blind Diagnostic Test. Nanomaterials, 13(9), 1539. https://doi.org/10.3390/nano13091539