1. Introduction
Epilepsy is a neurological disorder characterized by an enduring predisposition to spontaneous epileptic seizures, and affects over 70 million people worldwide [
1,
2]. The high disability and fatality rates in epilepsy constitute heavy global burdens, particularly in low- and middle-income countries [
3]. To date, antiepileptic drugs remain the first-line treatment, which a majority of epileptic patients needing to take them daily, despite being effective in only 60–70% of individuals [
4]. Among the available antiepileptic drugs, carbamazepine (CBZ) is the most commonly used drug in clinical practice [
5]. CBZ has a narrow therapeutic index and is a highly variable drug. Therapeutic drug monitoring (TDM) is considered a powerful tool for maximizing efficacy [
6,
7]. Particularly, TDM helps to investigate the effectiveness, pharmacokinetics, tolerability, dosage, and the possibility of withdrawing during CBZ treatment [
1]. In clinical care, the therapeutic reference range for CBZ is 4–12 µg/mL in plasma and 2–12 µg/mL in serum [
8].
Substantial efforts have been made to develop novel technologies to sensitively detect CBZ in multiple biological media, as reviewed recently [
9,
10,
11]. A majority of the CBZ bioassays are based on enzyme-linked immunosorbent assay (ELISA), high-performance liquid chromatography, and nanomaterial-based electrodes. The former two are benchmark methods routinely conducted in hospitals because of their reliable analytical performance, even when applied to tough samples such as dried blood spots [
12]. The latter can be developed into miniaturized devices for selectively detecting CBZ via a molecular imprinted polymer, an artificial antibody, as the sensing element [
13]. The most appropriate tool for monitoring CBZ is an in vivo microchip-based wireless device that obtains drug levels inside the body in real time [
14]. However, this requires substantial efforts to achieve. Till this develops, clinical practice urgently needs on-site TDM that goes beyond benchmark assays to provide quick, sensitive CBZ results in easy operation for individualized treatment [
15]. To achieve on-site TDM, a portable nano-plasmonic electrical field-enhanced resonating device and an immunochromatographic strip were built, but both failed to provide quantitative information on CBZ levels [
16,
17]. A suspension array fluorescence immunoassay that was developed to detect CBZ in wastewater has the potential to be applied for TDM of CBZ in clinical settings [
18]. Surface plasmon resonance biosensors have long proven their capacity in detecting various small molecules [
19,
20]. Another optical technique, biolayer interferometry, has gained increasing attention recently for drug analysis, in addition to its functions for kinetic study, drug discovery and vaccines research [
21,
22,
23].
Fiber-optic biolayer interferometry (FO-BLI) is an automated system and uses a robot arm to control multichannel for automated operation, as shown in
Scheme 1. Integration of multiple channels with microplates containing up to hundred samples enables multiplexed detection simultaneously and with high throughout. Fibers are made of glass with openings to connect to the robot arm and tips to interact with bioliquids. The three-dimensional fiber structure is shown in another work by our team, proving the capacity of FO-BLI for different applications [
24]. The ends of the fiber tips contain two reflection surfaces (I and II)—the former serves as internal reference and the latter serves as an active probe to capture targets. When vertical light is applied, the white light reflected from interfaces I and II forms an interference pattern. Fiber tips can be coated with specific sensing elements to capture targets in blood. Molecules bound cause a change in thickness in surface II and a further change in wavelength shifts in the interference pattern. During test, shifts are acquired automatically in real time and further processed to generate specific binding curves to interpolate the unknown.
This study investigates the potential of applying the FO-BLI technique for rapid, sensitive, and automated detection of small molecule CBZ in whole blood. One concern is that CBZ has a low mass and therefore fails to generate a large BLI signal above the sensor resolution threshold of approximately 0.01 nm. To address this concern, this study used two formats (indirect versus direct) of competitive binding to obtain sufficient signals for sensitive detection. The indirect FO-BLI biosensor includes sample preincubation with monoclonal antibodies towards CBZ (MA-CBZ), and immobilized biotinylated bovine serum albumin-CBZ conjugate (biotin-BSA-CBZ) competes for binding with MA-CBZ (
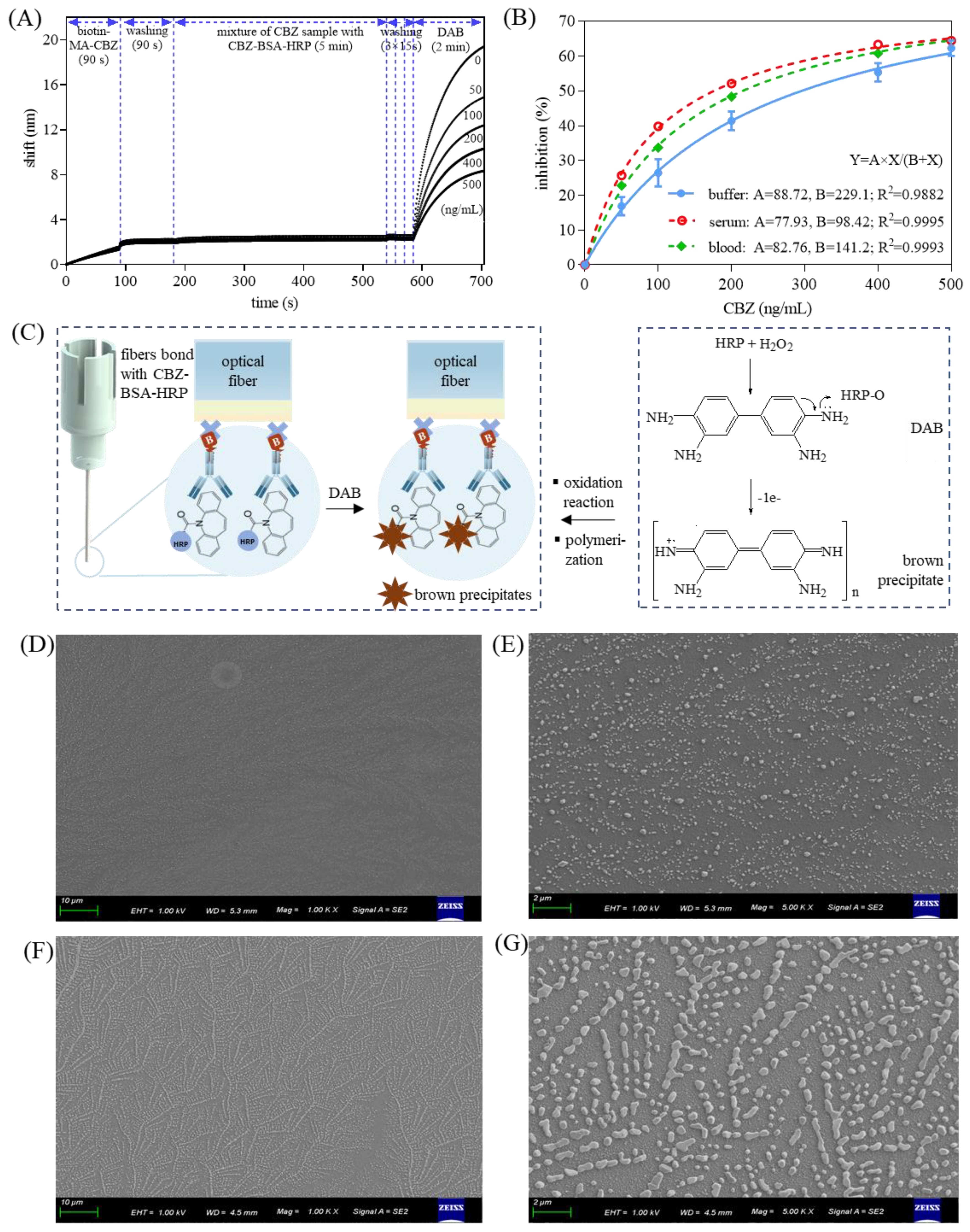
Figure 1A). The direct FO-BLI biosensor allows the CBZ in the samples and CBZ-BSA-horseradish peroxidase conjugate (CBZ-BSA-HRP) to directly compete for binding with immobilized biotin-MA-CBZ. Residual CBZ-BSA-HRP reacts with a metal precipitate 3,3′-diaminobenzidine (DAB) to amplify the signals in an effort to achieve higher sensitivity (
Figure 1B). After establishing both biosensors, strategies to control matric interreference (when sensors are used for single or several times) or biofouling (when sensors are used for continuous measurements) from blood on the sensor surface were also studied [
25,
26]. Comparison between the two biosensors included their performance in terms of sensitivity, selectivity, accuracy, time to result, and regeneration ability. The better performer was further evaluated ex vivo regarding its clinical utility using several paired sera and whole blood from CBZ-treated epileptic patients.
2. Materials and Methods
2.1. Materials
CBZ, valproate sodium, phenytoin sodium, primidone, Tween-20 and bovine serum albumin (BSA) were purchased from Sigma-Aldrich (Shanghai, China). CBZ antibody clone CA1 was obtained from Bio-Rad Laboratories (Shanghai, China). CBZ bovine serum albumin conjugate was purchased from Unibiotest Co., Ltd. (Wuhan, China). ZebaTM spin desalting columns (7 K MWCO, 0.5 mL), 3,3′- diaminobenzidine (DAB) enhanced liquid substrate system tetrahydrochloride, and SuperBlock™ (PBS) blocking buffer were obtained from Thermo Scientific (Shanghai, China). The biotinylating kit was obtained from Genemore (Suzhou, China). The horseradish peroxidase (HRP) Conjugation Kit-Lightning-Link® (ab102890) was from Abcam (Shanghai, China). Single donor human serum off the clot and human whole blood was obtained from Innovative Research (Novi, MI, USA). The 96-well polystyrene black microplates were obtained from Greiner Bio-One GmbH (Shanghai, China). The Octet® K2 2-channel system and streptavidin sensors were purchased from Sartorius Stedim Biotech GmbH (Gottingen, Germany). Phosphate-buffered saline (PBS, 10 mM, pH 7.4), PBS buffer containing 0.02% (v/v) Tween-20 and 0.1% BSA (referred to as sample diluent (SD) buffer), and SD buffer containing 274 mM NaCl (referred to as high-salt SD buffer) were used in this study.
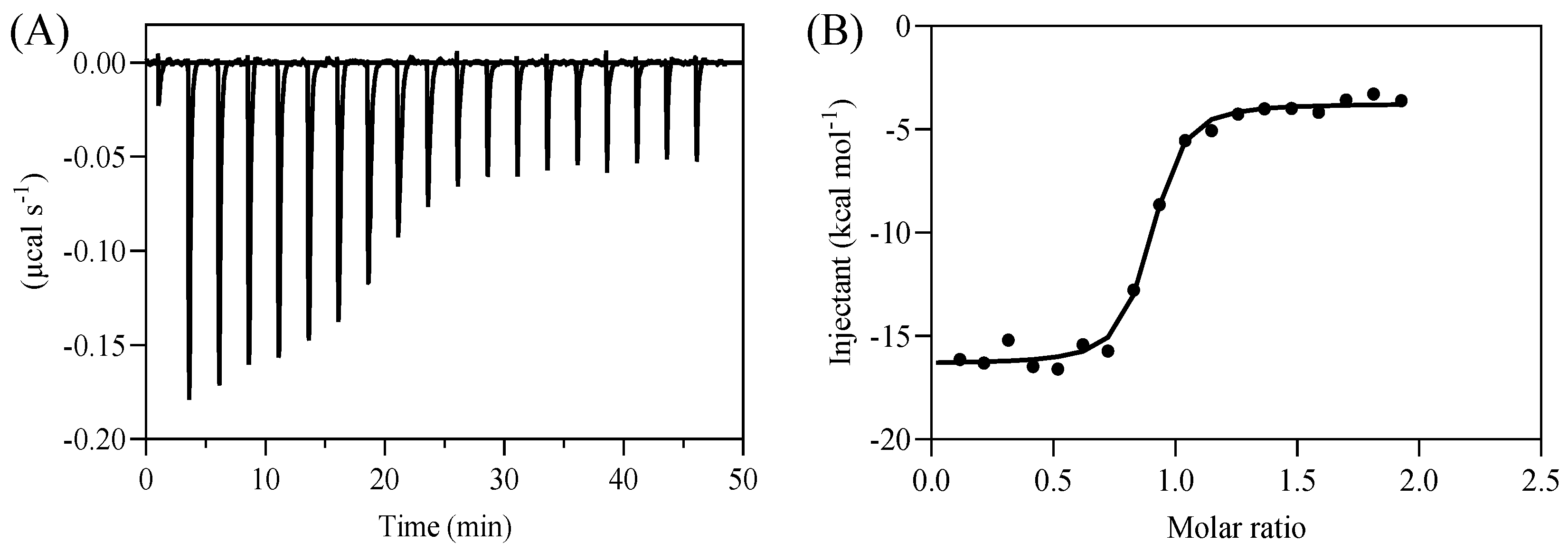
2.2. Isothermal Titration Calorimetry (ITC)
ITC was conducted using a MicroCal PEAQ-ITC microcalorimeter (Malvern Panalyical Limited, Malvern, Worcs, UK). The low-ionic-strength PBS buffer was used to disperse both CBZ and monoclonal antibody towards CBZ (MA-CBZ) to avoid background interference from the heat caused by the mixing of buffers. Prior to each measurement, all the solutions were degassed to avoid bubbles. Then, a 6.67 µM antibody was loaded in the ITC cell (0.3 mL) at 25 °C. CBZ (66.7 µM) at 25 °C was titrated (2 μL each time) into the cell through a syringe, except for the first injection (0.4 μL). All thermodynamic data (enthalpy (ΔH) and dissociation constant (Kd) were auto-analyzed with the MicroCal PEAQ-ITC Analysis Software using nonlinear least squares curve fitting. The profiles were reproduced by fitting the titration curves to a nonlinear regression (curve fit) model using GraphPad Prism.
2.3. Bioconjugation with Biotin and Horseradish Peroxidase
CBZ-BSA and MA-CBZ were biotinylated according to the protocol of a commercial biotinylating kit and purified by removing free biotin via short centrifugation at 1500× g for 2 min using desalting columns. CBZ-BSA was conjugated with HRP according to the manufacturer’s protocol to obtain a stock concentration of 1.0 mg/mL in PBS. All bioconjugates were stored at 4 °C.
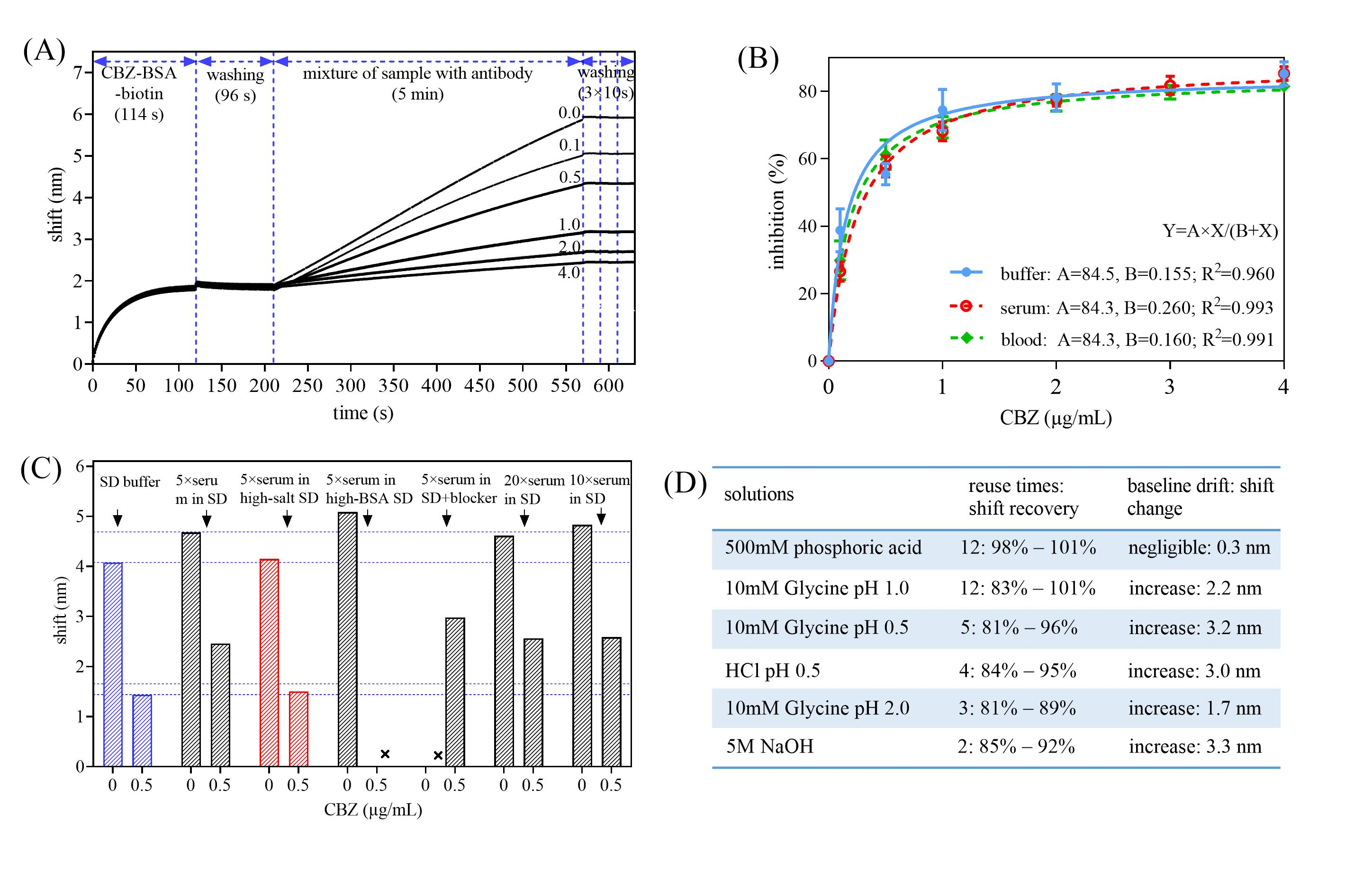
2.4. Strategies to Reduce FO-BLI Biosensor Biofouling Caused by Blood on Sensor Surface
Strategies applied to reduce biofouling on the sensor surface caused by blood included the followings: the dilution of serum and blood, use of high-salt SD buffer (SD buffer containing 270 mM NaCl), use of high-BSA SD buffer (SD buffer containing 1.0% BSA), and addition of Superblock buffer after surface functionalization. The objectives were to remove non-specifically adsorbed biomolecules from the sensor surface and to block excess binding sites. Antifouling performance of each strategy was assessed by comparing the wavelength shifts of two quality control samples with that obtained in pure SD buffer. The two controls have initial concentrations of 0 and 0.5 µg/mL for the indirect FO-BLI biosensor, and of 0 and 100 ng/mL for the direct FO-BLI biosensor.
2.5. Establishing an Indirect FO-BLI Biosensor for CBZ Detection in Buffer, Serum, and Whole Blood
Biotinylated BSA-CBZ coated onto streptavidin sensors was applied to detect CBZ via indirect competitive interaction. In the bioassay, free CBZ in a sample competed with immobilized biotin-CBZ-BSA for specific binding to the MA-CBZ, which was pre-added to the sample solution. Therefore, this bioassay was defined as an indirect FO-BLI biosensor. The higher the amount of CBZ present, the less MA-CBZ bound to the sensor, the fewer binding shifts were obtained. In particular, a loading shift of 1.5–2.0 nm was proposed when immobilizing the biotin-BSA-CBZ in order to have sufficient binding towards the target. CBZ was detected in three sample matrices: (i) in SD buffer with CBZ spiked from 0 to 4 µg/mL: 0—0.1—0.5—1.0—2.0—3.0—4.0 µg/mL, (ii) in 5× human serum and (iii) in 5× whole blood spiked with CBZ into a high-salt SD buffer within the detection range of 0 to 4.0 µg/mL. Spiked samples were mixed with a certain amount of MA-CBZ dissolved in the corresponding buffer in equal volumes for 20 min at 25 °C prior to analysis. The washing step was conducted between the steps to remove any unbound molecules. The generated signals were proportional to the amount of MA-CBZ residual in the sample mixture and inversely proportional to the amount of CBZ in the sample. The shifts of CBZ at 0 ng/mL were set as the reference, and the inhibition per point per sample was calculated as shown in Equation (1).
2.6. Establishing a Direct FO-BLI Biosensor for CBZ Detection in Buffer, Serum and Whole Blood
Biotinylated MA-CBZ was coated to allow direct competitive binding between free CBZ in a sample and pre-added CBZ-HRP conjugate, therefore being defined as a direct FO-BLI biosensor. Similarly, the lower the amount of CBZ present, the higher the amount of CBZ-HRP captured, and the higher the signals observed. Signals were amplified by submerging the sensors into the DAB solution, a metal precipitating substrate. The interaction of DAB with HRP generated precipitation on the fiber tip within seconds and induced changes in wave-length shifts. An appropriate concentration of CBZ-BSA-HRP was selected by comparing the shifts obtained from the series concentrations at 20—10—2—0.2—0.1 µg/mL. Optimal shifts for the highest target concentration were expected to reach approximately 15 nm. A 200× dilution was fixed for DAB by adding 5 µL DAB to 995 µL of substate buffer. In this bioassay, the loading shifts for biotin-MA-CBZ were aligned to be ap-proximately 1.5 nm for target capture. Similarly, CBZ was detected in three biological matrices: (i) in high-salt SD buffer with CBZ spiked from 0 to 400 ng/mL: 0—10—50—100—200—400 ng/mL, (ii) in 20× human serum, and (iii) in 20× whole blood spiked 0—400 ng/mL CBZ into high-salt SD buffer. Equal volume of CBZ-BSA-HRP was added to samples prior to analysis. Washing step was included in between. The inhibition per sample was determined followed Equation (1).
2.7. The Sensitivity, Specificity and Accuracy of the Two FO-BLI CBZ Biosensors
The limit of detection (LoD) was defined as the lowest CBZ concentration of the standard curve that could be detected but not reliably quantified with a coefficient of variation (CV) > 20%. The lower limit of quantification (LLoQ) was defined as the lowest CBZ concentration of the standard curve reliably measured with a CV ≤ 20%. The specificity was evaluated using three other anti-epileptic drugs, valproate sodium, phenytoin sodium, and primidone, at therapeutic concentrations of 100, 20, and 12 µg/mL, respectively. The accuracy was determined using a quality control sample of CBZ (6 µg/mL) to calculate its back recovery.
2.8. Regeneration of the Functionalized Optical Fibers
To evaluate whether the optical fibers could be regenerated and reused multiple times, a batch of regeneration buffers was used to evaluate the recovery of the wavelength shifts obtained at 0 µg/mL of CBZ. Regeneration solutions included 10 mM glycine (pH 2.0, 1.0, and 0.5, respectively), HCl (pH 0.5), 500 mM phosphoric acid, 5 M NaOH, and 0.01% sodium dodecyl sulfate. Regeneration was conducted via the ‘basic kinetic experiment’ model and three cycles of 10 s incubation in regeneration solution and 10 s in neutralization solution (high-salt SD buffer). Detection was conducted using the high-salt SD buffer to wash in between and at a shaking speed of 400 rpm at 30 °C. In the indirect FO-BLI, fibers were pre-loaded with biotin-BSA-CBZ to attain signals between 1.5 and 2.0 nm and further associated with the MA-CBZ at 10 µg/mL for 5 min to achieve signals at approximately 3.5 nm (referred to as Cycle 1). Afterwards, regeneration and neutralization were applied up to 12 times to measure the shifts of MA-CBZ at 10 µg/mL (referred to as Cycle 2, Cycle 3 to Cycle 12) and compared with that obtained in Cycle 1 for assessing the recovery. In the direct FO-BLI, fibers were pre-functionalized with biotin-MA-CBZ to attain a signal threshold of approximately 1.60 nm. Then, fibers were loaded with the CBZ-BSA-HRP conjugate at 1.0 µg/mL for 5 min and associated with DAB enhancer for 2 min, resulting in a sample shift at approximately 20 nm (referred to as Cycle 1). Afterwards, regeneration and neutralization were applied up to 12 times to measure the shifts of the same sample (consisting of 5 min loading of CBZ-BSA-HRP, 30 s washing, and 2 min DAB reaction) and compared with the shift obtained in Cycle 1.
2.9. Clinical Validation and Benchmarked against Ultra-Performance Liquid Chromatography
To evaluate the clinical utility of the FO-BLI biosensor, seven adult patients with epilepsy, who were prescribed regular CBZ drugs, were enrolled, as approved by the Institutional Review Boards of both Westlake University (20210608BSM001) and Second Affiliated Hospital of Zhejiang University School of Medicine (Research 2021-0778). Informed consent was obtained from all the participants. Sera and whole blood were collected between 4 and 5 h following the administration of conventional release tablets per individual and de-identified afterwards. Whole blood was collected by venipuncture in CBZ-treated epileptic patients using BD Vacutainer
® Lithium Heparin tubes. Sera were collected into the BD Vacutainer
® SSTTM II Advance Tubes simultaneously and centrifuged at 2000 rpm for 10 min at 25 °C to collect the supernatants. Each paired sample was measured four times in different runs by the selected FO-BLI biosensor. The inter-run variation was determined by dividing the standard deviation by the mean of the four separate measurements. As the biosensor was established to detect CBZ in whole blood, the relationship between whole blood and serum concentrations in adult epileptic patients was assessed by calculating the whole blood/serum ratio per paired. Measurements of the samples by the ultra-performance liquid chromatography (UPLC) followed the protocol as illustrated in the
Supplementary Figure S1.
2.10. Statistics
To reduce the amount of data for profiling the flowchart, the data per five readout points were assigned into and the means were calculated via the “aggregate” function in SPSS Statistics V.26 (IBM, Armonk, NY, USA). To quantify the correlation and agreement of CBZ measurements determined by the FO-BLI biosensor and the UPLC, GraphPad Prism 9.02 (GraphPad Software, San Diego, CA, USA) was used to calculate the Pearson r correlation coefficient and SPSS Statistics V.26 (IBM, Armonk, NY, USA) was used to calculate the intra-class correlation coefficient (ICC). The ICC calculation adopted the “two-way mixed single measure test (absolute agreement)”. Differences between the CBZ measurements obtained from the two methods were analyzed using the two-tailed t-test in GraphPad Prism. Inhibition curves of both FO-BLI biosensors were determined via “dose–response-inhibitor: log (inhibitor) vs. normalized response”. The level of statistical significance was set at p < 0.05.
4. Discussion and Conclusions
This study reports the development of two types of FO-BLI biosensors for on-site monitoring CBZ in serum and whole blood. The indirect FO-BLI biosensor, based on an indirectly competitive binding interaction, showed its capability to specifically detect CBZ within its clinically therapeutic range without interference from other anti-epileptic drugs. The indirect FO-BLI had an advantage in being regenerated up to 12 times with the use of 500 mM phosphoric acid, which reduced the test cost due to its capacity for multiple uses. However, the requirement to pre-mix each sample with the (commercial) target antibody on the one hand increased the cost and, on the other, resulted in a slow (25 min of assay time) and complex operation method. Given these limitations, the indirect FO-BLI was considered to be less effective when being implemented in modern clinical workflows. Conversely, the direct FO-BLI biosensor contributed to a much faster (approximately 7.5 min of time to result) and more straight-forward (by simple mixture) operation method. This was achieved by simply adding the sample into the CBZ-BSA-HRP conjugate of an equal volume for direct competitive binding towards the immobilized target antibody. Additionally, a much lower detection sensitivity of 10 ng/mL was obtained using a chromogen DAB to significantly simplify the signals without increasing significant background interreference. Unfortunately, the precipice-based signal enhancement failed to regenerate the sensors for the purpose of multiple uses. Despite this, the direct FO-BLI biosensor still maintains a reasonable cost per test as the biotinylated antibody and the HRP conjugated CBZ-BSA can be used for long term in addition to extra dilution before application. Additionally, a 20× final dilution of both the sera and blood into a high-salt SD buffer-minimized matrix interference to the biosensor performance. Further validation using six paired sera and whole blood samples from CBZ-treated epileptic patients demonstrated an excellent agreement between the direct FO-BLI and the benchmarked UPLC.
Altogether, the direct FO-BLI biosensor possesses multiple novel advantages, including the short turnaround time, full automation, and the delivery of CBZ values directly from whole blood, making it an effective and appropriate tool for on-site monitoring of CBZ in clinical practice. Additionally, the proposed technique can be applied for both single and high-throughout measurements. The limitation of the direct FO-BLI biosensor lies in the inability of the sensors to be regenerated for multiple uses in order to reduce costs. To address this, our next step is to investigate alternative effective signal enhancers for the direct FO-BLI. One bio-/nanomaterial that can both enhance signals (leading to a high sensitivity) and enable regeneration (reducing costs by reuse in multiple times) will greatly benefit the direct FO-BLI for clinical use.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}