
Potential Cost Savings Associated with Targeted Substitution of Current Guideline-Concordant Inpatient Agents with Omadacycline for the Treatment of Adult Hospitalized Patients with Community-Acquired Bacterial Pneumonia at High Risk for Clostridioides difficile Infections: Results of Healthcare-Decision Analytic Model from the United States Hospital Perspective


Abstract
:1. Introduction
2. Methods
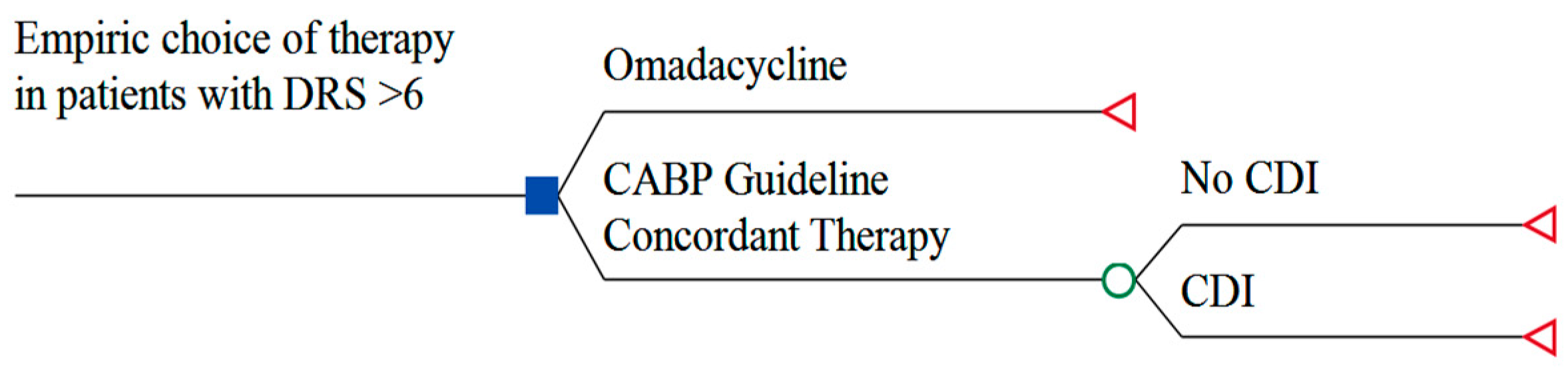
2.1. Model Structure and Study Population
2.2. Model Inputs and Assumptions
2.3. Model Output and Analyses
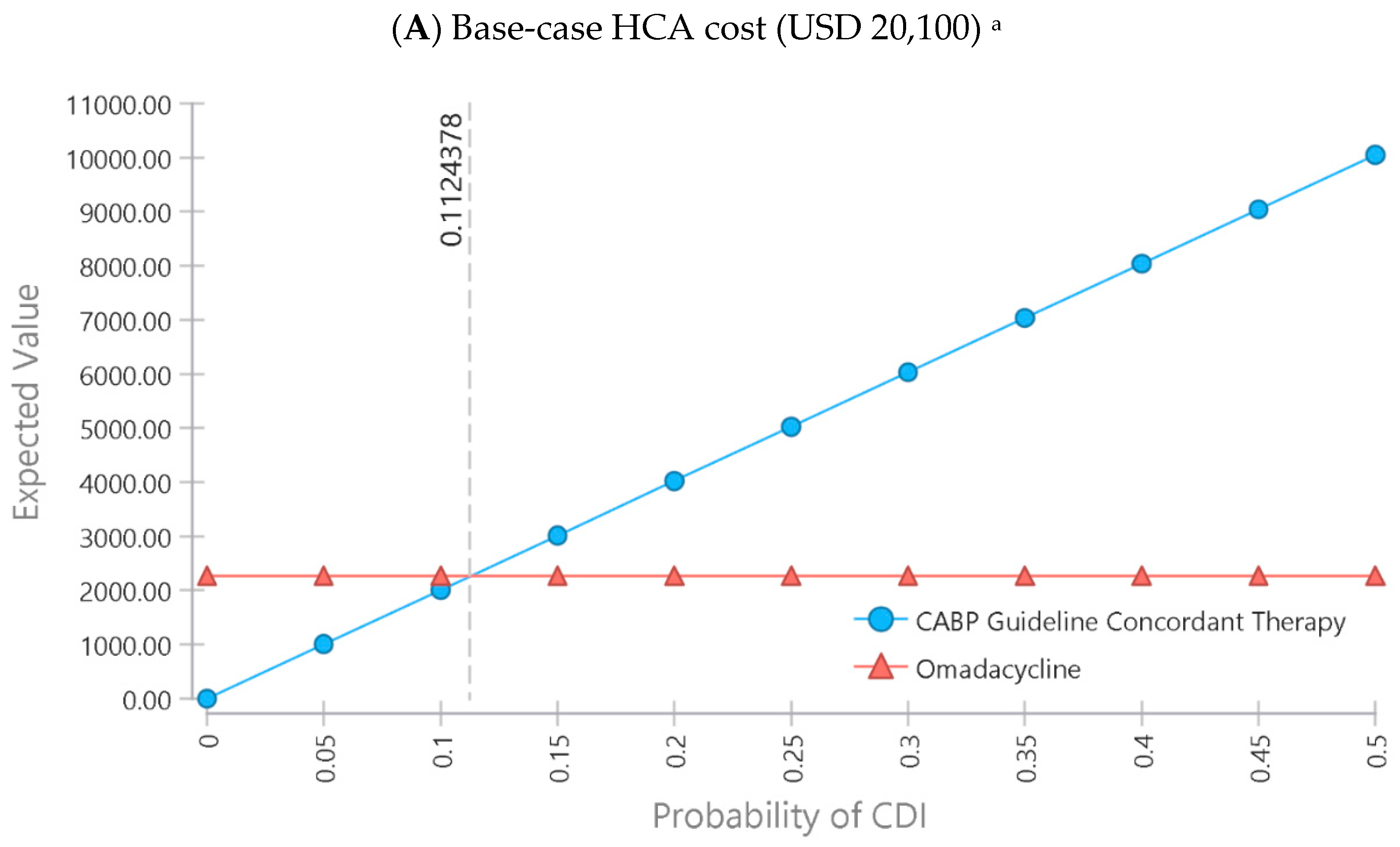
2.4. Parameter Sample Sensitivity Analyses
2.5. Sensitivity Analyses
3. Results
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Standard-of-Care Scenario for CABP Patients with DRS ≥ 6 | Cost Saving from Omadacycline Scenario Cost (USD Million) |
|---|---|
| Mean | 55 |
| Minimum | −68.1 |
| Maximum | 182.1 |
| 25th Percentile | 17.6 |
| Median | 55.4 |
| 75th Percentile | 93.7 |
References
- Schechner, V.; Fallach, N.; Braun, T.; Temkin, E.; Carmeli, Y. Antibiotic exposure and the risk of hospital-acquired diarrhoea and Clostridioides difficile infection: A cohort study. J. Antimicrob. Chemother. 2021, 76, 2182–2185. [Google Scholar] [CrossRef] [PubMed]
- Webb, B.J.; Subramanian, A.; Lopansri, B.; Goodman, B.; Jones, P.B.; Ferraro, J.; Stenehjem, E.; Brown, S.M. Antibiotic Exposure and Risk for Hospital-Associated Clostridioides difficile Infection. Antimicrob. Agents Chemother. 2020, 64, e02169-19. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.L.; Sparrow, H.G.; Ikwuagwu, J.O.; Musick, W.L.; Garey, K.W.; Perez, K.K. Multicentre derivation and validation of a simple predictive index for healthcare-associated Clostridium difficile infection. Clin. Microbiol. Infect. 2018, 24, 1190–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slimings, C.; Riley, T.V. Antibiotics and hospital-acquired Clostridium difficile infection: Update of systematic review and meta-analysis. J. Antimicrob. Chemother. 2014, 69, 881–891. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Khanafer, N.; Daneman, N.; Fisman, D.N. Meta-analysis of antibiotics and the risk of community-associated Clostridium difficile infection. Antimicrob. Agents Chemother. 2013, 57, 2326–2332. [Google Scholar] [CrossRef] [Green Version]
- Stevens, V.; Dumyati, G.; Fine, L.S.; Fisher, S.G.; van Wijngaarden, E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin. Infect. Dis. 2011, 53, 42–48. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Trigkidis, K.K.; Boukouvala, E.; Falagas, M.E. Clostridium difficile infection following systemic antibiotic administration in randomised controlled trials: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2016, 48, 1–10. [Google Scholar] [CrossRef]
- Balsells, E.; Shi, T.; Leese, C.; Lyell, I.; Burrows, J.; Wiuff, C.; Campbell, H.; Kyaw, M.H.; Nair, H. Global burden of Clostridium difficile infections: A systematic review and meta-analysis. J. Glob. Health 2019, 9, 010407. [Google Scholar] [CrossRef]
- Desai, K.; Gupta, S.B.; Dubberke, E.R.; Prabhu, V.S.; Browne, C.; Mast, T.C. Epidemiological and economic burden of Clostridium difficile in the United States: Estimates from a modeling approach. BMC Infect. Dis. 2016, 16, 303. [Google Scholar] [CrossRef] [Green Version]
- Zilberberg, M.D.; Nathanson, B.H.; Marcella, S.; Hawkshead, J.J., 3rd; Shorr, A.F. Hospital readmission with Clostridium difficile infection as a secondary diagnosis is associated with worsened outcomes and greater revenue loss relative to principal diagnosis: A retrospective cohort study. Medicine 2018, 97, e12212. [Google Scholar] [CrossRef]
- Nelson, W.W.; Scott, T.A.; Boules, M.; Teigland, C.; Parente, A.; Unni, S.; Feuerstadt, P. Health care resource utilization and costs of recurrent Clostridioides difficile infection in the elderly: A real-world claims analysis. J. Manag. Care Spec. Pharm. 2021, 27, 828–838. [Google Scholar] [CrossRef]
- National Action Plan to Prevent Health Care-Associated Infections: Road Map to Elimination. Available online: https://health.gov/our-work/health-care-quality/health-care-associated-infections/national-hai-action-plan (accessed on 1 August 2021).
- Centers for Medicare & Medicaid Services. Hospital-Acquired Condition Reduction Program (HACRP). Available online: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/HAC-Reduction-Program (accessed on 24 March 2020).
- C. diff Guidelines and Prevention Resources. Available online: https://www.cdc.gov/cdiff/clinicians/resources.html (accessed on 1 August 2021).
- Centers for Disease Control and Prevention. Core Elements of Hospital Antibiotic Stewardship Programs. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 1 August 2021).
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef]
- Torio, C.M.; Andrews, R.M. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011: Statistical Brief #160. 2013 Aug. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 February. Available online: https://www.ncbi.nlm.nih.gov/books/NBK169005/ (accessed on 1 August 2021).
- Chalmers, J.D.; Akram, A.R.; Singanayagam, A.; Wilcox, M.H.; Hill, A.T. Risk factors for Clostridium difficile infection in hospitalized patients with community-acquired pneumonia. J. Infect. 2016, 73, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care. Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, N.J.; Jozefczyk, C.C.; Moore, W.J.; Yarnold, P.R.; Harkabuz, K.; Maxwell, R.; Sutton, S.H.; Silkaitis, C.; Qi, C.; Wunderink, R.G.; et al. Characterizing Risk Factors for Clostridioides difficile Infection among Hospitalized Patients with Community-Acquired Pneumonia. Antimicrob. Agents Chemother. 2021, 65, e0041721. [Google Scholar] [CrossRef]
- Stets, R.; Popescu, M.; Gonong, J.R.; Mitha, I.; Nseir, W.; Madej, A.; Kirsch, C.; Das, A.F.; Garrity-Ryan, L.; Steenbergen, J.N.; et al. Omadacycline for Community-Acquired Bacterial Pneumonia. N. Engl. J. Med. 2019, 380, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Moura, I.B.; Buckley, A.M.; Ewin, D.; Shearman, S.; Clark, E.; Wilcox, M.H.; Chilton, C.H. Omadacycline Gut Microbiome Exposure Does Not Induce Clostridium difficile Proliferation or Toxin Production in a Model That Simulates the Proximal, Medial, and Distal Human Colon. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, O.; Leahy, R.G.; Traczewski, M.; Macone, A.; Steenbergen, J.; Tanaka, S.K. Activity and efficacy of omadacycline against Clostridium difficile. In Proceedings of the Conference Poster P1325 presented at ECCMID 2016, Amsterdam, The Netherlands, 9–12 April 2016; p. 1325. [Google Scholar]
- NUZYRA (omadacycline) for Injection, for Intravenous Use and NUZYRA (omadacycline) Tablets, for Oral Use Package Insert. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/209816_209817lbl.pdf (accessed on 1 August 2021).
- Rodriguez, M.; Wright, K.; Noble, R. Predicted risk and observed occurrence of Clostridioides difficile infection in patients with community-acquired bacterial pneumonia treated with omadacycline or moxifloxacin. In Proceedings of the Conference Poster P4548 pre-sented at ECCMID 2020, Paris, France, 18–21 April 2020; p. 4548. [Google Scholar]
- Kazakova, S.V.; Baggs, J.; McDonald, L.C.; Yi, S.H.; Hatfield, K.M.; Guh, A.; Reddy, S.C.; Jernigan, J.A. Association Between Antibiotic Use and Hospital-onset Clostridioides difficile Infection in US Acute Care Hospitals, 2006-2012: An Ecologic Analysis. Clin. Infect. Dis. 2020, 70, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Shea, K.M.; Hobbs, A.L.V.; Jaso, T.C.; Bissett, J.D.; Cruz, C.M.; Douglass, E.T.; Garey, K.W. Effect of a Health Care System Respiratory Fluoroquinolone Restriction Program To Alter Utilization and Impact Rates of Clostridium difficile Infection. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dingle, K.E.; Didelot, X.; Quan, T.P.; Eyre, D.W.; Stoesser, N.; Golubchik, T.; Harding, R.M.; Wilson, D.J.; Griffiths, D.; Vaughan, A.; et al. Effects of control interventions on Clostridium difficile infection in England: An observational study. Lancet Infect. Dis. 2017, 17, 411–421. [Google Scholar] [CrossRef] [Green Version]
- Estimating the Additional Hospital Inpatient Cost and Mortality Associated With Selected Hospital-Acquired Conditions. Agency for Healthcare Research and Quality, Rockville, MD. Available online: https://www.ahrq.gov/hai/pfp/haccost2017-results.html (accessed on 1 August 2021).
- Gabriel, L.; Beriot-Mathiot, A. Hospitalization stay and costs attributable to Clostridium difficile infection: A critical review. J. Hosp. Infect. 2014, 88, 12–21. [Google Scholar] [CrossRef]
- Zhang, S.; Palazuelos-Munoz, S.; Balsells, E.M.; Nair, H.; Chit, A.; Kyaw, M.H. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect. Dis. 2016, 16, 447. [Google Scholar] [CrossRef] [Green Version]
- RED BOOK (Micromedex®). Wholesale Acquisition Cost of Intravenous Omadaycycline. Available online: https://www.ibm.com/products/micromedex-red-book (accessed on 12 August 2021).
- Consumer Price Index Inflation Calculator. Available online: https://www.bls.gov/data/inflation_calculator.htm (accessed on 1 August 2021).
- LaPensee, K.; Mistry, R.; Lodise, T. Budget Impact Model of Omadacycline on Replacing a Proportion of Existing Treatment Options Among Patients Who Present to the Emergency Department with Acute Bacterial Skin and Skin Structure Infections. Am. Health Drug Benefits 2019, 12, S13–S24. [Google Scholar] [PubMed]
- Zhang, D.; Prabhu, V.S.; Marcella, S.W. Attributable Healthcare Resource Utilization and Costs for Patients With Primary and Recurrent Clostridium difficile Infection in the United States. Clin. Infect. Dis. 2018, 66, 1326–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, D.N.; Aitken, S.L.; Barragan, L.F.; Bozorgui, S.; Goddu, S.; Navarro, M.E.; Xie, Y.; DuPont, H.L.; Garey, K.W. Economic burden of primary compared with recurrent Clostridium difficile infection in hospitalized patients: A prospective cohort study. J. Hosp. Infect. 2016, 93, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Ghantoji, S.S.; Sail, K.; Lairson, D.R.; DuPont, H.L.; Garey, K.W. Economic healthcare costs of Clostridium difficile infection: A systematic review. J. Hosp. Infect. 2010, 74, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Feuerstadt, P.; Stong, L.; Dahdal, D.N.; Sacks, N.; Lang, K.; Nelson, W.W. Healthcare resource utilization and direct medical costs associated with index and recurrent Clostridioides difficile infection: A real-world data analysis. J. Med. Econ. 2020, 23, 603–609. [Google Scholar] [CrossRef] [Green Version]
- Tariq, R.; Cho, J.; Kapoor, S.; Orenstein, R.; Singh, S.; Pardi, D.S.; Khanna, S. Low Risk of Primary Clostridium difficile Infection With Tetracyclines: A Systematic Review and Metaanalysis. Clin. Infect. Dis. 2018, 66, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.; Sferra, T.J.; Hernandez, A.V.; Donskey, C.J. Community-associated Clostridium difficile infection and antibiotics: A meta-analysis. J. Antimicrob. Chemother. 2013, 68, 1951–1961. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Pardo, D.; Almirante, B.; Bartolome, R.M.; Pomar, V.; Mirelis, B.; Navarro, F.; Soriano, A.; Sorli, L.; Martinez-Montauti, J.; Molins, M.T.; et al. Epidemiology of Clostridium difficile infection and risk factors for unfavorable clinical outcomes: Results of a hospital-based study in Barcelona, Spain. J. Clin. Microbiol. 2013, 51, 1465–1473. [Google Scholar] [CrossRef] [Green Version]
- Louie, T.J.; Miller, M.A.; Mullane, K.M.; Weiss, K.; Lentnek, A.; Golan, Y.; Gorbach, S.; Sears, P.; Shue, Y.K.; Group, O.P.T.C.S. Fidaxomicin versus vancomycin for Clostridium difficile infection. N. Engl. J. Med. 2011, 364, 422–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowy, I.; Molrine, D.C.; Leav, B.A.; Blair, B.M.; Baxter, R.; Gerding, D.N.; Nichol, G.; Thomas, W.D., Jr.; Leney, M.; Sloan, S.; et al. Treatment with monoclonal antibodies against Clostridium difficile toxins. N. Engl. J. Med. 2010, 362, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S. Recurrent Clostridium difficile infection: A review of risk factors, treatments, and outcomes. J. Infect. 2009, 58, 403–410. [Google Scholar] [CrossRef] [PubMed]
- McFarland, L.V.; Elmer, G.W.; Surawicz, C.M. Breaking the cycle: Treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am. J. Gastroenterol. 2002, 97, 1769–1775. [Google Scholar] [CrossRef]
- Garey, K.W.; Sethi, S.; Yadav, Y.; DuPont, H.L. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J. Hosp. Infect. 2008, 70, 298–304. [Google Scholar] [CrossRef]
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinh, A.; Le Monnier, A.; Emery, C.; Alami, S.; Torreton, E.; Duburcq, A.; Barbier, F. Predictors and burden of hospital readmission with recurrent Clostridioides difficile infection: A French nation-wide inception cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1297–1305. [Google Scholar] [CrossRef]
- Abou Chakra, C.N.; Pepin, J.; Sirard, S.; Valiquette, L. Risk factors for recurrence, complications and mortality in Clostridium difficile infection: A systematic review. PLoS ONE 2014, 9, e98400. [Google Scholar] [CrossRef] [Green Version]
- Lurienne, L.; Bandinelli, P.A.; Galvain, T.; Coursel, C.A.; Oneto, C.; Feuerstadt, P. Perception of quality of life in people experiencing or having experienced a Clostridioides difficile infection: A US population survey. J. Patient Rep. Outcomes 2020, 4, 14. [Google Scholar] [CrossRef]
- Paterson, D.L. “Collateral Damage” from Cephalosporin or Quinolone Antibiotic Therapy. Clin. Infect. Dis. Issue 2004, 38 (Suppl. S4), S341–S345. [Google Scholar] [CrossRef]

| Factor | Parameter |
|---|---|
| Number of CABP admissions per year in United States of America [17] | 1,000,000 |
| Percentage (number of patients) of hospitalized CABP patients with DRS ≥ 6 [3,21,25] | 10% (n = 100,000) |
| Percentage (number of patients) of CABP patients with DRS ≥ 6 who developed CDI in the guideline-concordant standard of care scenario [21,25] | 14% (n = 14,000) |
| Cost per episode of healthcare associated CDI in base-case analysis [29] | USD 20,100 (95% CI: 10,900–29,300) |
| Lower bound of cost per episode of healthcare associated CDI in one-way sensitivity analysis [30] | USD 10,860 |
| Upper bound of cost per episode of healthcare associated CDI in one-way sensitivity analysis [31] | USD 39,700 |
| Omadacycline wholesale acquisition cost for 5-day cost of IV therapy [32] | USD 2260 |
| Factor | Cost (USD Million) |
|---|---|
| Guideline-concordant standard of care scenario for CABP patients with DRS ≥ 6 | 281.4 a |
| Cost of 5-day hospital treatment with omadacycline | 226.0 b |
| Cost saving from omadacycline scenario | 55.4 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lodise, T.; Rodriguez, M.; Chitra, S.; Wright, K.; Patel, N. Potential Cost Savings Associated with Targeted Substitution of Current Guideline-Concordant Inpatient Agents with Omadacycline for the Treatment of Adult Hospitalized Patients with Community-Acquired Bacterial Pneumonia at High Risk for Clostridioides difficile Infections: Results of Healthcare-Decision Analytic Model from the United States Hospital Perspective. Antibiotics 2021, 10, 1195. https://doi.org/10.3390/antibiotics10101195
Lodise T, Rodriguez M, Chitra S, Wright K, Patel N. Potential Cost Savings Associated with Targeted Substitution of Current Guideline-Concordant Inpatient Agents with Omadacycline for the Treatment of Adult Hospitalized Patients with Community-Acquired Bacterial Pneumonia at High Risk for Clostridioides difficile Infections: Results of Healthcare-Decision Analytic Model from the United States Hospital Perspective. Antibiotics. 2021; 10(10):1195. https://doi.org/10.3390/antibiotics10101195
Chicago/Turabian StyleLodise, Thomas, Mauricio Rodriguez, Surya Chitra, Kelly Wright, and Nimish Patel. 2021. "Potential Cost Savings Associated with Targeted Substitution of Current Guideline-Concordant Inpatient Agents with Omadacycline for the Treatment of Adult Hospitalized Patients with Community-Acquired Bacterial Pneumonia at High Risk for Clostridioides difficile Infections: Results of Healthcare-Decision Analytic Model from the United States Hospital Perspective" Antibiotics 10, no. 10: 1195. https://doi.org/10.3390/antibiotics10101195
APA StyleLodise, T., Rodriguez, M., Chitra, S., Wright, K., & Patel, N. (2021). Potential Cost Savings Associated with Targeted Substitution of Current Guideline-Concordant Inpatient Agents with Omadacycline for the Treatment of Adult Hospitalized Patients with Community-Acquired Bacterial Pneumonia at High Risk for Clostridioides difficile Infections: Results of Healthcare-Decision Analytic Model from the United States Hospital Perspective. Antibiotics, 10(10), 1195. https://doi.org/10.3390/antibiotics10101195