
Carbapenem Therapeutic Drug Monitoring in Critically Ill Adult Patients and Clinical Outcomes: A Systematic Review with Meta-Analysis

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
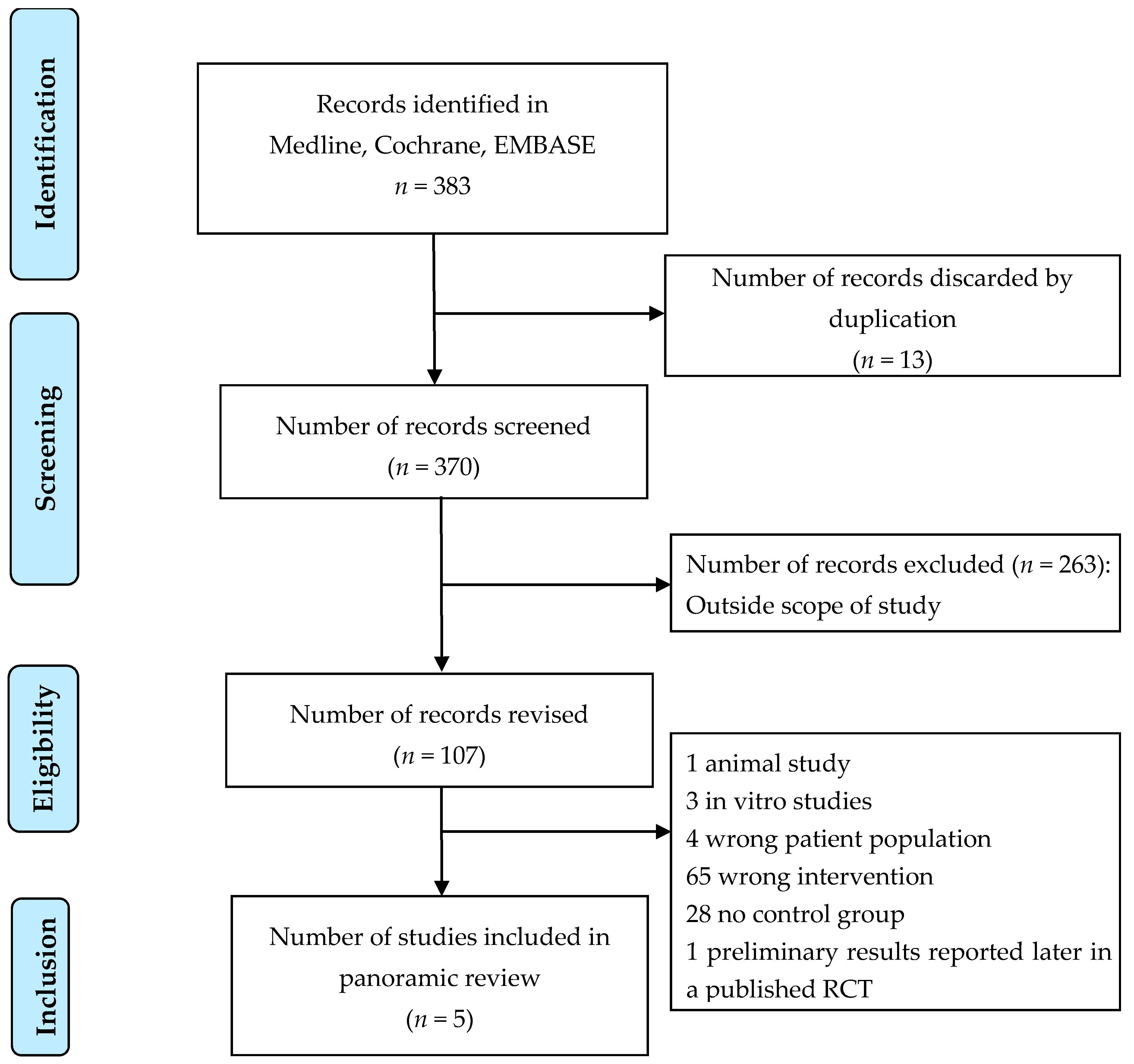
2.1. Search Results
2.2. Study Characteristics
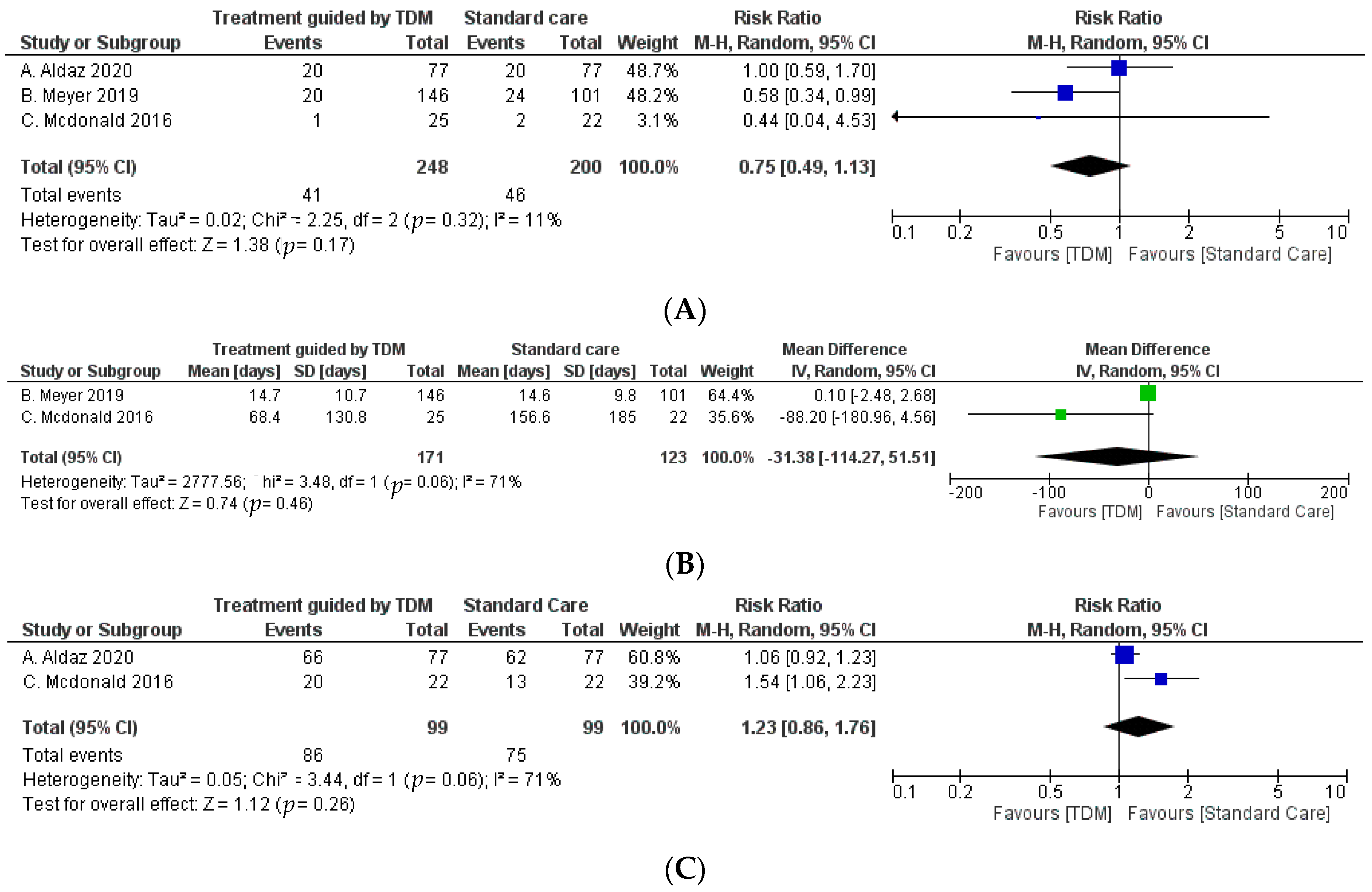
2.3. Clinical Outcome
2.4. Heterogeneity of Studies
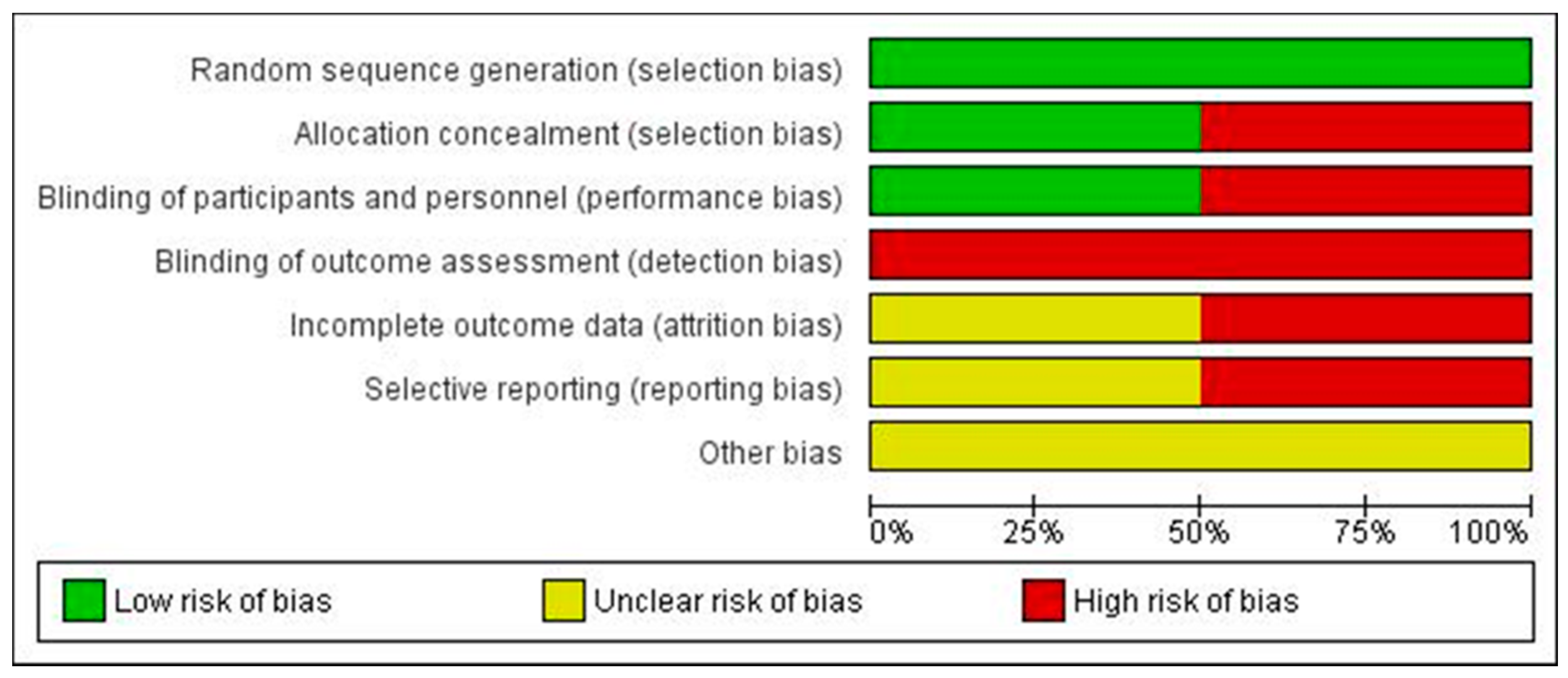
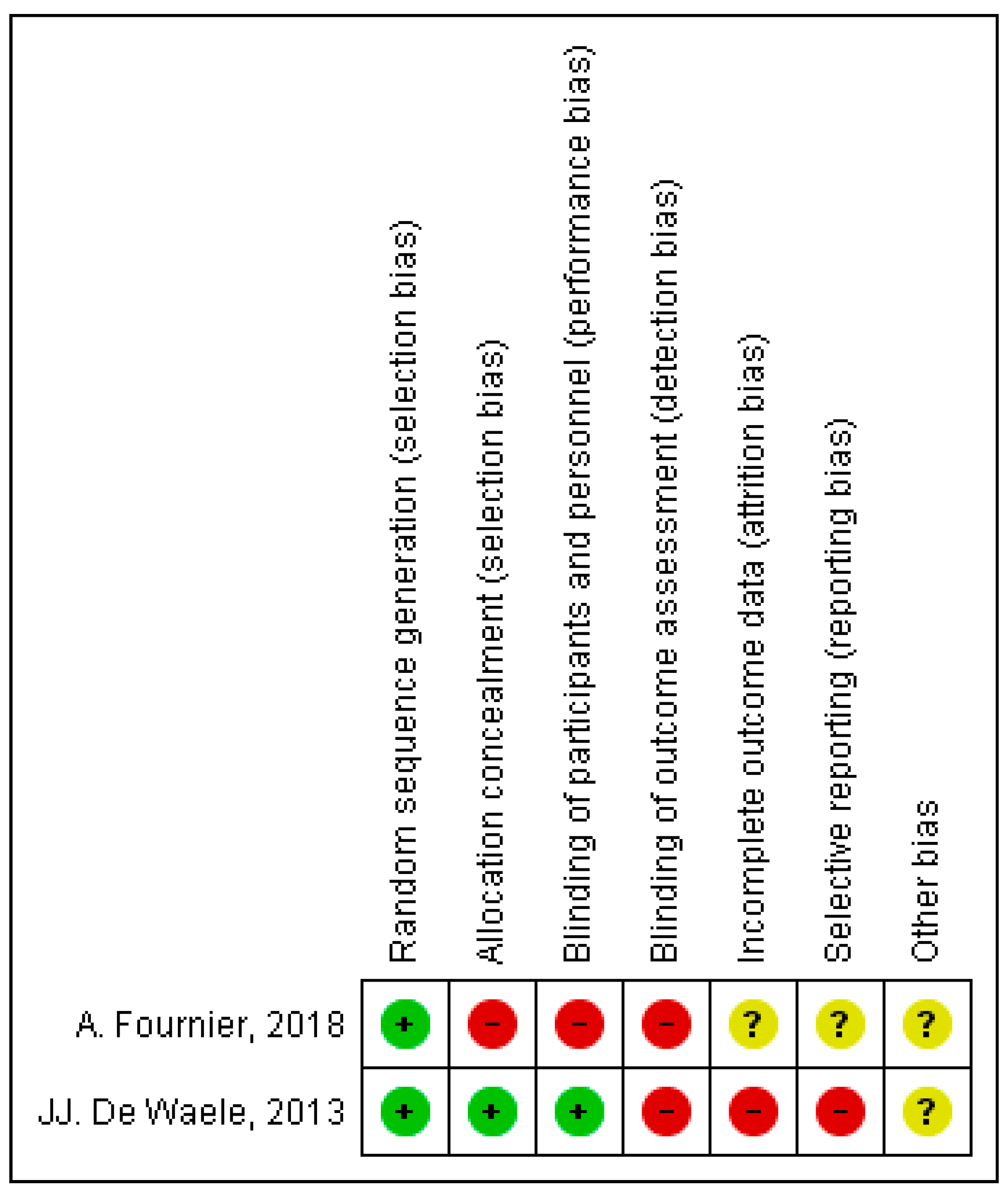
2.5. Publication Bias, Risk of Bias, and Quality of Evidence
3. Discussion
4. Materials and Methods
4.1. Data Sources and Searches
4.2. Search Eligibility Criteria
4.3. Data Extraction and Assessment of Methodological Quality
4.4. Data Synthesis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Clarke, W. Chapter 1—Overview of Therapeutic Drug Monitoring. In Clinical Challenges in Therapeutic Drug Monitoring; Clarke, W., Dasgupta, A., Eds.; Elsevier: San Diego, CA, USA, 2016; pp. 1–15. [Google Scholar] [CrossRef]
- Neugebauer, S.; Wichmann, C.; Bremer-Streck, S.; Hagel, S.; Kiehntopf, M. Simultaneous Quantification of Nine Antimicrobials by LC-MS/MS for Therapeutic Drug Monitoring in Critically Ill Patients. Ther. Drug Monit. 2019, 41, 29–37. [Google Scholar] [CrossRef]
- Kang, J.-S.; Lee, M.-H. Overview of Therapeutic Drug Monitoring. Korean J. Intern. Med. 2009, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Garzón, V.; Bustos, R.-H.; Pinacho, D.G. Personalized Medicine for Antibiotics: The Role of Nanobiosensors in Therapeutic Drug Monitoring. J. Pers. Med. 2020, 10, 147. [Google Scholar] [CrossRef]
- Oellerich, M.; Kanzow, P.; Walson, P.D. Therapeutic drug monitoring—Key to personalized pharmacotherapy. Clin. Biochem. 2017, 50, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Ates, H.C.; Roberts, J.A.; Lipman, J.; Cass, A.E.; Urban, G.A.; Dincer, C. On-Site Therapeutic Drug Monitoring. Trends Biotechnol. 2020, 38, 1262–1277. [Google Scholar] [CrossRef]
- Junaid, T.; Wu, X.; Thanukrishnan, H.; Venkataramanan, R. Chapter 30—Therapeutic Drug Monitoring. In Clinical Pharmacy Education, Practice and Research; Thomas, D., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 425–436. [Google Scholar] [CrossRef]
- Huttner, A.; Harbarth, S.; Hope, W.W.; Lipman, J.; Roberts, J.A. Therapeutic drug monitoring of the beta-lactam antibiotics: What is the evidence and which patients should we be using it for? J. Antimicrob. Chemother. 2015, 70, 3178–3183. [Google Scholar] [PubMed]
- Muller, A.E.; Huttner, B.; Huttner, A. Therapeutic Drug Monitoring of Beta-Lactams and Other Antibiotics in the Intensive Care Unit: Which Agents, Which Patients and Which Infections? Drugs 2018, 78, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Nicolau, D.P. Carbapenems: A potent class of antibiotics. Expert Opin. Pharmacother. 2007, 9, 23–37. [Google Scholar] [CrossRef]
- Baughman, R.P. The Use of Carbapenems in the Treatment of Serious Infections. J. Intensiv. Care Med. 2009, 24, 230–241. [Google Scholar] [CrossRef]
- Martínez, M.J.F.; García, M.I.G.; Sánchez, E.G.; Sánchez, J.E.G. Los carbapenems disponibles: Propiedades y diferencias. Enfermedades Infecciosas y Microbiología Clínica 2010, 28, 53–64. [Google Scholar] [CrossRef]
- Codjoe, F.S.; Donkor, E.S. Carbapenem Resistance: A Review. Med. Sci. 2017, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Meletis, G. Carbapenem resistance: Overview of the problem and future perspectives. Ther. Adv. Infect. Dis. 2015, 3, 15–21. [Google Scholar] [CrossRef]
- Breilh, D.; Texier-Maugein, J.; Allaouchiche, B.; Saux, M.-C.; Boselli, E. Carbapenems. J. Chemother. 2013, 25, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Neuner, E.A.; Gallagher, J.C. Pharmacodynamic and pharmacokinetic considerations in the treatment of critically Ill patients infected with carbapenem-resistant Enterobacteriaceae. Virulence 2016, 8, 440–452. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Wiebe, R.; Dilay, L.; Thomson, K.; Rubinstein, E.; Hoban, D.J.; Noreddin, A.M.; Karlowsky, J.A. Comparative Review of the Carbapenems. Drugs 2007, 67, 1027–1052. [Google Scholar] [CrossRef]
- Suchánková, H.; Rychlíčková, J.; Urbánek, K. Pharmacokinetics of carbapenems. Klin. Mikrobiol. Infekcni Lek. 2012, 18, 68–74. [Google Scholar]
- Mouton, J.W.; Touzw, D.J.; Horrevorts, A.M.; Vinks, A.A. Comparative pharmacokinetics of the carbapenems: Clinical implications. Clin. Pharmacokinet. 2000, 39, 185–201. [Google Scholar] [CrossRef]
- Guidelines for Intensive Care Unit Admission, Discharge, and Triage. Task Force of the American College of Critical Care Medicine, Society of Critical Care Medicine. Crit. Care Med. 1999, 27, 633–638. [Google Scholar]
- Roberts, J.A.; Aziz, M.H.A.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef]
- Hafiz, A.-A.M.; E Staatz, C.; Kirkpatrick, C.M.J.; Lipman, J.; A Roberts, J. Continuous infusion vs. bolus dosing: Implications for beta-lactam antibiotics. Minerva Anestesiol. 2011, 78, 94–104. [Google Scholar]
- Williams, P.; Cotta, M.O.; Roberts, M.S. Pharmacokinetics/Pharmacodynamics of β-Lactams and Therapeutic Drug Monitoring: From Theory to Practical Issues in the Intensive Care Unit. Semin. Respir. Crit. Care Med. 2019, 40, 476–487. [Google Scholar] [CrossRef]
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient—Concepts appraised by the example of antimicrobial agents. Adv. Drug Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef]
- Pea, F.; Viale, P.; Furlanut, M. Antimicrobial therapy in critically ill patients: A review of pathophysiological conditions responsible for altered disposition and pharmacokinetic variability. Clin. Pharmacokinet. 2005, 44, 1009–1034. [Google Scholar] [CrossRef] [PubMed]
- Fournier, A.; Eggimann, P.; Pantet, O.; Pagani, J.L.; Dupuis-Lozeron, E.; Pannatier, A.; Sadeghipour, F.; Voirol, P.; Que, Y.-A. Impact of Real-Time Therapeutic Drug Monitoring on the Prescription of Antibiotics in Burn Patients Requiring Admission to the Intensive Care Unit. Antimicrob. Agents Chemother. 2017, 62, e01818-17. [Google Scholar] [CrossRef]
- De Waele, J.J.; Carrette, S.; Carlier, M.; Stove, V.; Boelens, J.; Claeys, G.; Leroux-Roels, I.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; et al. Therapeutic drug monitoring-based dose optimisation of piperacillin and meropenem: A randomised controlled trial. Intensiv. Care Med. 2013, 40, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Aldaz, A.; Grijalba, A.I.I.; Ortega, A.; Aquerreta, I.; Monedero, P. Effectiveness Of Pharmacokinetic/Pharmacodynamic-Guided Meropenem Treatment in Critically Ill Patients. Ther. Drug Monit. 2020. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.; Tröger, U.; Lohmeier, S.; Bode-Böger, S.; Hansen, M.; Schmeißer, A.; Braun-Dullaeus, R.; Tanev, I. Benefit of meropenem therapeutic drug monitoring in critically ill patients with sepsis. Intensive Care Med. Exp. 2019, 7, 342–343. [Google Scholar]
- McDonald, C.; Cotta, M.O.; Little, P.J.; McWhinney, B.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Is high-dose β-lactam therapy associated with excessive drug toxicity in critically ill patients? Minerva Anestesiol. 2016, 82, 957–965. [Google Scholar]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensiv. Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef]
- Welty, T.E.; Copa, A.K. Impact of Vancomycin Therapeutic Drug Monitoring on Patient Care. Ann. Pharmacother. 1994, 28, 1335–1339. [Google Scholar] [CrossRef]
- Roberts, J.A.; Lipman, J. Antibacterial dosing in intensive care: Pharmacokinetics, degree of disease and pharmacodynamics of sepsis. Clin. Pharmacokinet. 2006, 45, 755–773. [Google Scholar] [CrossRef]
- Udy, A.; Roberts, J.A.; Lipman, J. Clinical implications of antibiotic pharmacokinetic principles in the critically ill. Intensiv. Care Med. 2013, 39, 2070–2082. [Google Scholar] [CrossRef]
- Felton, T.; Hope, W.; Roberts, J. How severe is antibiotic pharmacokinetic variability in critically ill patients and what can be done about it? Diagn. Microbiol. Infect. Dis. 2014, 79, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Tamargo, J.; Le Heuzey, J.-Y.; Mabo, P. Narrow therapeutic index drugs: A clinical pharmacological consideration to flecainide. Eur. J. Clin. Pharmacol. 2015, 71, 549–567. [Google Scholar] [CrossRef]
- Norrby, S.R. Carbapenems in serious infections: A risk-benefit assessment. Drug Saf. 2000, 22, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Abdulla, A.; Ewoldt, T.M.J.; Hunfeld, N.G.M.; Muller, A.E.; Rietdijk, W.J.R.; Polinder, S.; Van Gelder, T.; Endeman, H.; Koch, B.C.P. The effect of therapeutic drug monitoring of beta-lactam and fluoroquinolones on clinical outcome in critically ill patients: The DOLPHIN trial protocol of a multi-centre randomised controlled trial. BMC Infect. Dis. 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bricheux, A.; Lenggenhager, L.; Hughes, S.; Karmime, A.; Lescuyer, P.; Huttner, A. Therapeutic drug monitoring of imipenem and the incidence of toxicity and failure in hospitalized patients: A retrospective cohort study. Clin. Microbiol. Infect. 2019, 25, 383.e1–383.e4. [Google Scholar] [CrossRef]
- McKinnon, P.S.; Paladino, J.A.; Schentag, J.J. Evaluation of area under the inhibitory curve (AUIC) and time above the minimum inhibitory concentration (T>MIC) as predictors of outcome for cefepime and ceftazidime in serious bacterial infections. Int. J. Antimicrob. Agents 2008, 31, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining antibiotic levels in intensive care unit patients: Are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef]
- Pea, F.; Della Siega, P.; Cojutti, P.; Sartor, A.; Crapis, M.; Scarparo, C.; Bassetti, M. Might real-time pharmacokinetic/pharmacodynamic optimisation of high-dose continuous-infusion meropenem improve clinical cure in infections caused by KPC-producing Klebsiella pneumoniae? Int. J. Antimicrob. Agents 2017, 49, 255–258. [Google Scholar] [CrossRef]
- McNeill, R.P.; Barclay, M.L. Cost-effectiveness of therapeutic drug monitoring in inflammatory bowel disease. Curr. Opin. Pharmacol. 2020, 55, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Ried, L.D.; Horn, J.R.; McKenna, D.A. Therapeutic drug monitoring reduces toxic drug reactions: A meta-analysis. Ther. Drug. Monit. 1990, 12, 72–78. [Google Scholar] [CrossRef]
- Bootman, J.L.; Wertheimer, A.I.; Zaske, D.; Rowland, C. Individualizing Gentamicin Dosage Regimens in Burn Patients with Gram-Negative Septicemia: A Cost–Benefit Analysis. J. Pharm. Sci. 1979, 68, 267–272. [Google Scholar] [CrossRef] [PubMed]
- E Burton, M.; Ash, C.L.; Hill, D.P.; Handy, T.; Shepherd, M.D.; Vasko, M.R. A controlled trial of the cost benefit of computerized bayesian aminoglycoside administration. Clin. Pharmacol. Ther. 1991, 49, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Destache, C.J. Use of Therapeutic Drug Monitoring in Pharmacoeconomics. Ther. Drug Monit. 1993, 15, 608–660. [Google Scholar] [CrossRef] [PubMed]
- Bootman, J.L.; Harrison, D.L. Pharmacoeconomics and therapeutic drug monitoring. Pharm. World Sci. 1997, 19, 178–181. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Single or Multi-Centre/Design/N | Population/Intervention/Comparator/PK | Optimization Algorithm | Clinical Outcomes | Follow-Up Duration |
|---|---|---|---|---|---|
| A. Fournier, 2018 [26] | Prospective monocentric, randomized, controlled trial n = 38 | Population Burn patients treated with intravenous AB. Intervention TDM of AB and dose readjustment Comparator Patients without dose adjustment based on TDM. Pharmacokinetics: Bioanalysis methodology: HPLC-MS/MS; sample: serum; result: no mean concentrations were presented in patients with carbapenems | One step adjustment: ↓ Dose: in cases of excessive minimum levels >150% of the upper limit ↑ Dose: in cases of minimum levels between 50–100% of the objective Two-step adjustment: ↓/↑ Dose: in cases of trough levels >150 or 200% of the upper limit or 10–50% variation from minimum target Adaptation to patients according to clinical history and specific population. Interruption of antibiotic treatment in case of toxicity | Primary PKs: t to achieve anti-infective serum concentrations. Serum monitoring of AB outside the target range in a single treatment cycle Secondary PK: estimation of the favorable clinical outcome (resolution of infection episodes). Monitoring of AB concentrations within the target range. Total antibiotic consumption | 23 October 2013 and 31 October 2016 (3 years) |
| JJ. De Waele, 2013 [27] | Monocenter, prospective, partially blinded, and randomized controlled trial n = 41 | Population Patients receiving MEM or PTZ AB. Age: ≥18 years. Normal kidney function Intervention TMD was performed daily, allowing dosage adjustment in intervals outside the objective (100% fT>4MIC). AB administration: according to an extended infusion protocol Comparator Control group: TDM was developed daily. However, the physician did not know the results. Data used for comparison only Pharmacokinetics Bioanalytical Methodology: UHPLC-MS/MS, internal standard oxacillin; sample: serum; results: median AB concentration: <2 mg/mL (before randomization), interquartile range: <2–4 mg/L MEM AB | MIC: 2 mg/L for MEM; 16mg/mL PTZ Minimum target concentration: >8 mg/L for MEM ↑ dosing frequency: If concentration is <4 MIC (1 g every 6 h for MEM) ↑ 50% dosing frequency: If concentration <4 MIC No action: 4–10 MIC ↓ 50% dosing frequency: >10xMIC | Primary outcome: defined target: 100% fT>MIC First 72 h: 100% fT>4MIC Baseline value and 72 h after the start of treatment: Comparison of fT>MIC and fT>4MIC (intervention and control group) Secondary Outcome: absolute values of fT>MIC and fT>4MIC End of study: evaluation of clinical outcome and absence or persistence of bacteria at day 7 | April 2011 and February 2012, follow up 7 days |
| A. Aldaz, 2020 [28] | Retrospective, unicentric cohort study n = 154 | Population ICU patients with MEM AB treatment and dose administered according to TDM (n = 77) Intervention Propensity score-balanced patients receiving MEM dose-adjusted by TDM Comparator Patients with MEM AB treatment according to standard recommendations (without TDM). Dose adjustment: in patients with renal failure according to the recommendations established in the package insert Pharmacokinetics Bioanalytical methodology: HPLC; sample: serum; result: mean Cmax 27.21 µg/mL and mean Cmin: 6.69 µg/mL (TDM cohort) of MEM | n/a | Primary outcome: PCT measure with ≥80% reduction in relation to maximum levels obtained at the end of AB treatment with MEM Secondary outcome: clinical remission, microbiological remission, length of hospital stay, length of stay in ICU Side effects; hospital mortality, mortality 14 days after MEM treatment; sepsis score according to SOFA at admission and discharge | May 2011–December 2017 (67 months) |
| B. Meyer, 2019 [29] | Single-centre retrospective cohort study n = 247 | Population Critically ill adult patients with administration of standard doses of MEM antibiotic (n = 101); critically ill adult patients with administration of MEM antibiotic dose according to MDD (n = 146) Intervention Individualized treatment of MEM AB guided by TDM Comparator Patients with MEM AB treatment according to standard recommendations (without TDM) Pharmacokinetics Bioassay methodology: HPLC; sample: plasma; results: 3.2 measurement of the plasma level in the TDM cohort. MEM concentrations average and per patient were not mentioned | n/a | Primary outcome: correlation of TDM and MEM AB use in critically ill patients Secondary outcome: length of stay and survival | n/a |
| C. Mcdonald, 2016 [30] | Retrospective, monocentric cohort study n = 98 | Population ICU patients with administration of MEM antibiotic doses higher than those recommended (3–6 g/day) (n = 93 patients) (MEM n = 47 patients (LD = 22) (HD = 25) Intervention ↑ Doses at those recommended, when plasma free drug concentrations were below local PK/PD targets. Comparator Licensed doses usage of either MEM Pharmacokinetics Bioanalytical methodology: HPLC; sample: plasma; results: plasma MEM AB concentrations were 44 µg/mL (authorized dose group) and 81 µg/mL (high dose group) | n/a | Primary outcome measures: switch to narrower spectrum BA due to favorable outcome and resolution of infection. This was verified by microbiological data Results of the second day: healing failure, side effects by organic system, fT>100% MIC of isolated microorganisms, dose changes, duration of therapy, dosage, microbiological control, de-escalation, length of stay in the ICU, hospital destination (discharge from ICU, interhospital transfer and mortality), demographic variables | n/a |
| Study | Timing of Outcome | TDM Cohort n (%)/Mean (SD)/Median (IQR) | Comparator Group n (%)/Mean (SD)/Median (IQR) | OR/RR/MD (95% CI) | p-Value | Ref |
|---|---|---|---|---|---|---|
| Outcome 1: mortality | ||||||
| JJ. De Waele, 2013 * Single-centre, partially blinded RCT | At 7 days after treatment | In ICU: (4.8) Hospital and 28-day: (14.3) | In ICU: (20) Hospital and 28-day: (25) | n/a | In ICU: 0.18 Hospital and 28-day: 0.45 | [27] |
| A. Aldaz, 2020 Single-centre, retrospective cohort study | In-hospital At 14 days after treatment | In-hospital: 20/77 (26) 14-day: 2/77 (2.6) | In-hospital: 20/77 (26) 14-day: 3/77 (3.9) | In-hospital mortality: n/a Mortality at 14 days after treatment: RR = 0.667; 95% CI 0.11 to 1.88 | In-hospital: 1 14-day: 0.649 | [28] |
| B. Meyer, 2019 Single-centre retrospective cohort study | In-hospital | 20/146 (14) | 24/101 (24) | n/a | 0.042 | [29] |
| C. Mcdonald, 2016 Single-centre retrospective cohort study | In-hospital | 1/25 (4) | 2/22 (9.1) | n/a | n/a | [30] |
| Outcome 2: ICU length of stay (days) | ||||||
| A. Fournier, 2018 ** Single-centre not blinded RCT | n/a | 27 (13.0–45.0) | 20 (12.0–40.0) | n/a | n/a | [26] |
| A. Aldaz, 2020 Single-centre, retrospective cohort study | n/a | 8 (3–98) | 7 (3–99) | n/a | 0.473 | [28] |
| B. Meyer, 2019 Single-centre retrospective cohort study | n/a | 14.7 ± 10.7 | 14.6 ± 9.8 | n/a | n/a | [29] |
| C. Mcdonald, 2016 Single-centre retrospective cohort study | n/a | 68.4 ± 130.8 | 156.6 ± 185 | n/a | 0.17 | [30] |
| Outcome 3: clinical cure | ||||||
| A. Fournier, 2018 ** Single-centre not blinded RCT | n/a | Meropenem: 14/19 (34.2) Imipenem-cilastatin: 1 (2.4) Ertapenem: 1 (2.4) | Meropenem: 13/19 (31.7) Imipenem-cilastatin: 1 (2.4) Ertapenem: 1 (2.4) | n/a | n/a | [26] |
| A. Aldaz, 2020 Single-centre, retrospective cohort study | May 2011–December 2017 (67 months) | Reduction 80% in PCT: 55/77 (71.43) | Reduction 80% in PCT: 41/77 (53.25) | n/a | 0.02 | [28] |
| C. Mcdonald, 2016 Single-centre retrospective cohort study | n/a | Cessation or de-escalation of antibiotic 21/25 (84) | 15/22 (68.18) | n/a | n/a | [30] |
| Outcome 4: microbiological eradication | ||||||
| A. Aldaz, 2020 Single-centre, retrospective cohort study | May 2011–December 2017 (67 months) | 66/77 (85.7) | 62/77 (80.5) | n/a | 0.39 | [28] |
| C. Mcdonald, 2016 Single-centre retrospective cohort study | n/a | 20/22 (80) | 13/22 (59.1) | n/a | 0.48 | [30] |
| Outcome 5: target attainment | ||||||
| A. Fournier, 2018 ** Single-centre not blinded RCT | n/a | Cmin value: 28/36 (77,8) | Cmin value: 15/27 (55,6) | n/a | n/a | [26] |
| JJ. De Waele, 2013 * Single-centre, partially blinded RCT | 72 h | 100% fT>MIC: (94.7%) 100% fT>4MIC: (57.9%) | 100% fT>MIC: (68.4%) 100% fT>4MIC: (15.8%) | n/a | 100% fT>MIC: 0.045 100% fT>4MIC: 0.007 | [27] |
| C. Mcdonald, 2016 Single-centre retrospective cohort study | n/a | 100% fT>MIC: 15/28 (53.6) | 100% fT>MIC: 10/22 (45.5) | n/a | 0.57 | [30] |
| Outcome 6: antimicrobial resistance | ||||||
| JJ. De Waele, 2013 *,¥ Single-centre, partially blinded RCT | 7 days | 1 (n/a) | 5 (n/a) | n/a | 0.09 | [27] |
| A. Aldaz, 2020 ¥ Single-centre, retrospective cohort study | May 2011–December 2017 (67 months) | 11/77 (14.3) | 15/77 (19.5) | n/a | 0.39 | [28] |
| Outcome 7: adverse reactions | ||||||
| A. Aldaz, 2020 Single-centre, retrospective cohort study | May 2011–December 2017 (67 months) | Gastrointestinal: 11/77 (14.29) Hematologic: 40/77 (51.95) CNS: 4/77 (5.19) Dermatological: 3/77 (3.90) Hepatobiliary: 36/77 (46.75) | Gastrointestinal: 11/77 (14.29) Hematologic: 31/77 (40.26) CNS: 10/77 (12.99) Dermatological: 2/77 (2.60) Hepatobiliary: 36/77 (46.75) | n/a | Gastrointestinal: 1 Hematologic: 0.148 CNS: 0.093 Dermatoogical: 0.649 Hepatobiliary: 1 | [28] |
| C. Mcdonald, 2016 Single-centre retrospective cohort study | n/a | Hepatic Toxicity: Hepatocellular derangement: 5/28 (17.9) Cholestasis: 7/28 (28.0) Hematological Toxicity: Thromocytopenia: 3/28 (10.7) Neutropenia: 1/28 (3.6) Need for CRRT Incidence: 0/28 Resolved: 0/28 | Hepatic Toxicity: Hepatocellular derangement: 7/22 (31,8) Cholestasis: 3/22 (13.6) Hematological Toxicity: Thromocytopenia: 2/22 (9.1) Neutropenia:1/22 (4.5) Need for CRRT Incidence: 2/22 (9.1) Resolved: 1/22 (4.5) | n/a | Hepatic Toxicity: Hepatocellular derangement: 0.25 Cholestasis: 0.32 Hematological Toxicity: Thromocytopenia: 0.85 Neutropenia: 0.95 Need for CRRT Incidence: 0.10 Resolved: 0.25 | [30] |
| Outcome 8: hospital readmission | ||||||
| A. Aldaz, 2020 Single-centre, retrospective cohort study | May 2011–December 2017 (67 months) | 5/77 (6.49) | 7/77 (9.09) | n/a | 0.548 | [28] |
| Study | Representativeness of Exposed Cohort | Selection of Non-Exposed Cohort | Ascertainment of Exposure and Blinding | Outcome not Present at Outset | Study Controls for Important Confounder ± Additional Confounders, Including Differences in Care | Blind Assessment of Outcome | Follow-Up Long Enough | Follow-Up Adequacy | Total Number of Stars (Out of 9) |
|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome | |||||||
| A. Aldaz, 2020 | ★ | ★ | ★ | ★★ | ★ | ★ | 7 | ||
| B. Meyer, 2019 | ★ | ★ | ★ | ★ | 4 | ||||
| C. Mcdonald, 2016 | ★ | ★ | ★ | ★ | 4 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lechtig-Wasserman, S.; Liebisch-Rey, H.; Diaz-Pinilla, N.; Blanco, J.; Fuentes-Barreiro, Y.-V.; Bustos, R.-H. Carbapenem Therapeutic Drug Monitoring in Critically Ill Adult Patients and Clinical Outcomes: A Systematic Review with Meta-Analysis. Antibiotics 2021, 10, 177. https://doi.org/10.3390/antibiotics10020177
Lechtig-Wasserman S, Liebisch-Rey H, Diaz-Pinilla N, Blanco J, Fuentes-Barreiro Y-V, Bustos R-H. Carbapenem Therapeutic Drug Monitoring in Critically Ill Adult Patients and Clinical Outcomes: A Systematic Review with Meta-Analysis. Antibiotics. 2021; 10(2):177. https://doi.org/10.3390/antibiotics10020177
Chicago/Turabian StyleLechtig-Wasserman, Sharon, Hans Liebisch-Rey, Nicolas Diaz-Pinilla, Jhosep Blanco, Yuli-Viviana Fuentes-Barreiro, and Rosa-Helena Bustos. 2021. "Carbapenem Therapeutic Drug Monitoring in Critically Ill Adult Patients and Clinical Outcomes: A Systematic Review with Meta-Analysis" Antibiotics 10, no. 2: 177. https://doi.org/10.3390/antibiotics10020177
APA StyleLechtig-Wasserman, S., Liebisch-Rey, H., Diaz-Pinilla, N., Blanco, J., Fuentes-Barreiro, Y.-V., & Bustos, R.-H. (2021). Carbapenem Therapeutic Drug Monitoring in Critically Ill Adult Patients and Clinical Outcomes: A Systematic Review with Meta-Analysis. Antibiotics, 10(2), 177. https://doi.org/10.3390/antibiotics10020177