1. Introduction
Urinary tract infections (UTIs) include infections that affect the urethra (urethritis), urinary bladder (cystitis), or kidneys (pyelonephritis) [
1]. UTIs are more prevalent in female subjects, even among individuals with a high risk of infections (e.g., catheterized patients) [
2]. Based on disease classification by Infectious Diseases Society of America (IDSA) and National Antimicrobial Guidelines (NAG) Malaysia, uncomplicated UTIs include acute, symptomatic bacterial cystitis and acute pyelonephritis in nonpregnant, premenopausal women without urological abnormalities or comorbidities [
3,
4]. On the other hand, UTI symptoms in men or the presence of a structural or functional abnormality in the urinary tract in women are considered complicated UTIs [
4]. Commonly identified etiologic microorganisms in UTIs include
Escherichia coli,
Staphylococcus spp.,
Klebsiella pneumoniae,
Enterobacter spp.,
Proteus mirabilis,
Enterococcus faecalis, group B
Streptococcus,
Pseudomonas aeruginosa, and
Candida spp. [
5,
6]. Uncomplicated UTIs in otherwise healthy women in the community are mainly caused by uropathogenic
E. coli (80%) [
2]. The second most common causative agent of UTIs is
K. pneumoniae, a highly relevant bacteria in complicated UTIs where patients are predisposed to infections due to underlying healthcare-associated risk factors [
6,
7].
Once diagnosed with UTIs, finite courses of antibiotics are often prescribed to resolve acute symptoms. The recommended first-line antibiotics for the treatment of acute uncomplicated UTIs include nitrofurantoin, trimethoprim-sulfamethoxazole, fosfomycin trometamol, and pivmecillinam (in regions where it is available), in a treatment course ranging from one to seven days [
3,
8]. In cases of treatment failure, second-line antibiotics that include fluoroquinolones and β-lactams may be prescribed for three to seven days [
8]. Besides, fluoroquinolones and β-lactam antibiotics are recommended for the treatment of acute pyelonephritis and complicated UTIs [
3,
4]. Given the recurrent nature of UTIs, antibiotic treatments may lead to development of resistance in bacterial pathogens, compromising the effectiveness of successive treatments [
2]. Moreover, the wide use of antimicrobial prophylaxis in patients predisposed to UTIs has also contributed to the rise in antimicrobial resistance (AMR) [
6,
7].
The increasing prevalence of AMR among the aetiologic agents of UTIs has been observed since the early 2000 s [
5]. Worldwide emergence and prevalence of extended-spectrum β-lactamase (ESBL)-producing
Enterobacteriaceae, including
E. coli and
K. pneumoniae, have become a serious threat to public health [
9]. The Institute of Medical Research (IMR), a Ministry of Health (MOH) agency in Malaysia, has been actively monitoring AMR rates in clinical isolates since 2003. To date, 41 hospitals and one public health laboratory have contributed to the national AMR database. AMR surveillance for urine isolates has documented relatively high rates of resistance to β-lactam antibiotics such as ampicillin, amoxicillin-clavulanate, piperacillin-tazobactam, cefepime, cefotaxime, ceftazidime, and cefuroxime (10–68% in
E. coli and 5–40% in
K. pneumoniae) and low rates for carbapenem resistance (less than 1% in
E. coli and less than 5% in
K. pneumoniae) over the past decade [
10]. ESBL-producing
E. coli and
K. pneumoniae have emerged and spread in Malaysia [
11].
Flomoxef is a broad-spectrum oxacephem antibiotic that was introduced to the medical field in the mid-1980s [
12]. The in vitro and clinical efficacy of flomoxef have been proven satisfactory in the treatment of infections caused by both Gram-positive and Gram-negative bacteria, with minimal side effects or unexpected laboratory results [
13,
14,
15]. The use of flomoxef in empiric and definitive therapy has been previously evaluated and was proven to be effective for ESBL-producing
E. coli bacteremia [
16]. Preclinical studies in China, Japan, Korea, and Taiwan have reported that flomoxef susceptibility among ESBL-producing
Enterobacteriaceae, especially in
E. coli, was comparable to cefmetazole, cefoxitin, imipenem, and meropenem [
17,
18,
19,
20,
21]. Clinical studies conducted in pediatric patients with UTIs caused by ESBL-producing
E. coli showed comparable susceptibility between flomoxef, cefmetazole, and imipenem [
22,
23].
The in vitro activity of flomoxef on ESBL-producing Enterobacteriaceae beyond Northeast Asian region has not been investigated. The current literature showed that flomoxef may be a potential alternative to carbapenems for the treatment of UTIs caused by ESBL-producers. Hence, we aimed to investigate the in vitro efficacy of flomoxef in comparison with other established β-lactam antibiotics against ESBL-producing E. coli and K. pneumoniae associated with UTIs in Malaysia.
3. Discussion
We observed high rates of resistance to penicillin antibiotics, third- and fourth-generation cephalosporins, and a high rate of nonsusceptibility to β-lactam combination agents among the ESBL-producing E. coli and K. pneumoniae strains isolated from urine samples. Both organisms showed similar AMR trends when tested with β-lactam antibiotics. The multi-resistance patterns detected in the E. coli and K. pneumoniae strains in this study were accompanied, in most cases, by ESBL-encoding genes. All ESBL-producing strains examined in this study were highly susceptible to carbapenems with low MIC values. Similarly, flomoxef exhibited an inhibitory effect on the ESBL producers at low concentrations, especially in E. coli.
The high rate of resistance to penicillins, cephalosporins (except cephamycins), trimethoprim-sulfamethoxazole, and ciprofloxacin observed in this study suggested that these antibiotics might be ineffective in the treatment of UTIs caused by ESBL-producing
E. coli and
K. pneumoniae in this region. These antibiotics are commonly prescribed in Malaysian primary care settings, constituting up to 93% of antibiotics prescribed for UTI treatment [
24]. β-lactam antibiotics, including penicillins, cephalosporins, and penicillin combinations with an enzyme inhibitor, are the most prescribed antibiotics in both public hospitals and private practice in Malaysia, accounting for approximately 66% of all antibiotics prescribed in primary care settings [
25]. The overuse of these antibiotics could have contributed to the development of resistance among
E. coli and
K. pneumoniae strains circulating in Malaysia. The NAG recommended an empirical drug for uncomplicated cystitis, nitrofurantoin, which remained highly effective against ESBL-producing
E. coli and, to a lesser extent,
K. pneumoniae in our study [
4]. Amoxicillin-clavulanate is recommended as an alternative drug for the treatment of uncomplicated cystitis and a drug of choice for pyelonephritis and complicated UTIs in Malaysia [
4]. However, high rates of resistance to amoxicillin-clavulanate were observed in ESBL-producing
E. coli and
K. pneumoniae in this study. Therefore, obtaining a urine sample for culture and susceptibility testing before starting treatment is essential to avoid treatment failure in infections caused by ESBL-producers.
Combining our findings with that of the national surveillance data, we observed that a greater resistance to penicillins, cephalosporins, and β-lactam combination agents is probably common among ESBL-producing
E. coli and
K. pneumoniae associated with UTIs, and carbapenems remained the most effective therapeutic agents in this region [
10]. Comparing to in vitro studies in China and Korea, which also examined a wide array of different β-lactam antibiotics, a similar AMR trend was observed among the ESBL producers [
19,
21]. ESBL-producing
E. coli and
K. pneumoniae reported in these studies were generally highly resistant to cephalosporins (MIC
50/90 ≥ 8/256 µg/mL) but also remained highly susceptible to carbapenems (MIC
50/90 ≤ 0.125/0.25 µg/mL) and flomoxef (0.06/0.25 µg/mL ≤ MIC
50/90 ≤ 1/16 µg/mL), as revealed in this study. Similarly, cephamycins remained largely effective against ESBL-producing strains [
19,
21]. However, ESBL producers in the reported studies showed greater susceptibility to β-lactam combinations, such as amoxicillin-clavulanate (MIC
50/90 = 8/16 µg/mL) and piperacillin-tazobactam (2/64 µg/mL ≤ MIC
50/90 ≤ 8/128 µg/mL), compared to the strains examined in this study. Although piperacillin-tazobactam and cefepime have shown comparable efficacy as carbapenems for infections caused by ESBL producers, this use is only recommended when the organisms are tested susceptible to these antibiotics [
26]. The highly resistant phenotype of the local ESBL producers seen in this study suggested against the use of piperacillin-tazobactam and cefepime as potential carbapenem-sparing strategies in Malaysia. Cephamycins may be an alternative to carbapenems for the treatment of UTIs caused by ESBL producers [
26]. Based on the data obtained in this study, cefmetazole would be a better option compared to cefoxitin, since a greater susceptibility to cefmetazole was seen with the ESBL-producing strains.
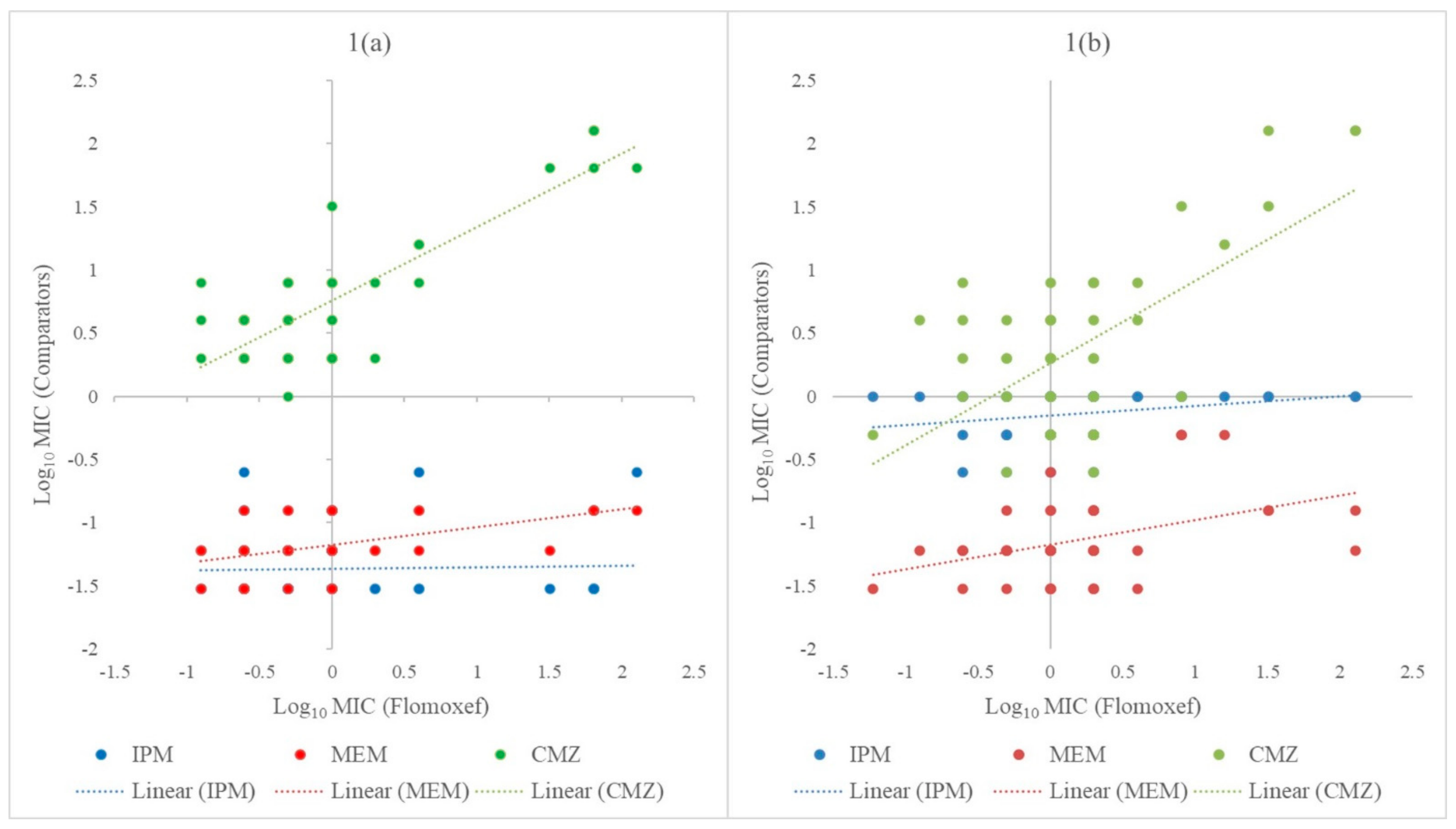
A comparison of the MIC
50/90 values obtained in this study showed that flomoxef exhibited a higher in vitro efficacy against ESBL-producing
E. coli and
K. pneumoniae than most of the β-lactam antibiotics tested, except for carbapenems. In the present study, a reduced susceptibility to flomoxef was found associated with an increased resistance to cefmetazole, while carbapenems remained consistently effective against all bacterial strains. Our results showed that carbapenems had the highest activity against the ESBL-producing strains, with the lowest MIC
50/90 values (≤0.03/0.06–1/1 µg/mL). On the other hand, the MIC
50/90 of flomoxef were lower than cefmetazole and cefoxitin in both
E. coli (two- to sixteen-fold reductions) and
K. pneumoniae (two- to four-fold reductions), indicating a slightly higher in vitro efficacy of flomoxef against the ESBL producers. Consistent observations were made in studies conducted in China, Japan, and Korea, where ESBL producers isolated in these regions were most susceptible to carbapenems, followed by flomoxef and cephamycins (cefmetazole or cefoxitin) [
17,
19,
21]. Clinical studies investigating the use of flomoxef for the treatment of UTIs caused by ESBL-producing
E. coli showed promising results and comparable efficacy with carbapenems [
22,
23]. However, a more variable outcome was produced when used in the treatment of bloodstream infections caused by ESBL producers [
26]. Taiwanese studies have documented increased mortality with the use of flomoxef in hemodialysis access-related bacteremia and lower efficacy compared to carbapenems for isolates with flomoxef MIC of 2–8 µg/mL [
27,
28]. Based on the MIC data obtained in this study, flomoxef may be considered as a potential alternative to carbapenems for less severe infections, such as UTIs caused by ESBL-producing
E. coli and
K. pneumoniae in this region.
Most of the UTI-associated
E. coli and
K. pneumoniae strains examined in this study carried at least one gene encoding for class A β-lactamases, which are known to confer a resistance to penicillins, extended-spectrum cephalosporins, and monobactams [
29]. The majority of the strains carried two to three ESBL genes, likely accounting for the high MIC values of β-lactam antibiotics observed in this study. Moreover, similar ESBL gene combinations could have explained the common β-lactam-resistant phenotypes shared between the
E. coli and
K. pneumoniae strains. Our findings are in agreement with local studies that identified
blaCTX-M as the most prevalent gene among the ESBL-producing
E. coli and
K. pneumoniae isolated from human and animal sources [
30,
31,
32,
33]. In these local reports, ESBL producers often carried multiple ESBL genes conferring a wide range of β-lactam resistance in the organisms, which is consistently observed in this study. The absence of
blaFOX within our strains pool is probably not unexpected, given that the rates of resistance to cephamycins (cefmetazole and cefoxitin) were relatively low among
E. coli and
K. pneumoniae. Consistent with the previous report, the cephamycins remained active against the majority of the investigated strains, as these organisms mostly produced TEM- and/or SHV-type β-lactamases that are ineffective against cephamycins [
34]. Approximately one-fifth of the ESBL-producing
E. coli did not harbor any of the four ESBL genes that were examined in this study. Since porin- and efflux-mediated mechanisms are not common in
E. coli and often only confer resistance to antibiotics at low concentrations, other ESBL genes (
blaOXA,
blaPER,
blaGES, etc.) could be responsible for the ESBL-producing phenotype of these strains [
35,
36]. Moreover, the production of AmpC β-lactamases, especially among
E. coli, is frequently associated with positive ESBL test outcomes [
37,
38].
One of the limitations of this study was the low number of ESBL-producing E. coli and K. pneumoniae collected within one year from a single study center in Malaysia. Although our strain pools may not represent the entire ESBL-producing Enterobacteriaceae population in this region, both temporally and geographically, the data generated in this study provided an insight into the extent of β-lactam resistance among ESBL producers associated with UTIs in Malaysia. Moreover, the susceptibility data obtained in this study support further consideration on the potential use of flomoxef as an alternative treatment for UTIs caused by ESBL producers. Another limitation of the study was that only four β-lactamase genes were targeted; therefore, the data obtained did not provide a comprehensive molecular epidemiology of ESBL production among the UTI-associated E. coli and K. pneumoniae strains in this region.


 ,
, 

{kind=link}