
Microbiological Characteristics and Surgical Management of Animal-Bite-Related Oral & Maxillofacial Injuries: A Single Center’s Experience


Abstract
:1. Introduction
2. Results
2.1. Demographic Data
2.2. Injury Patterns
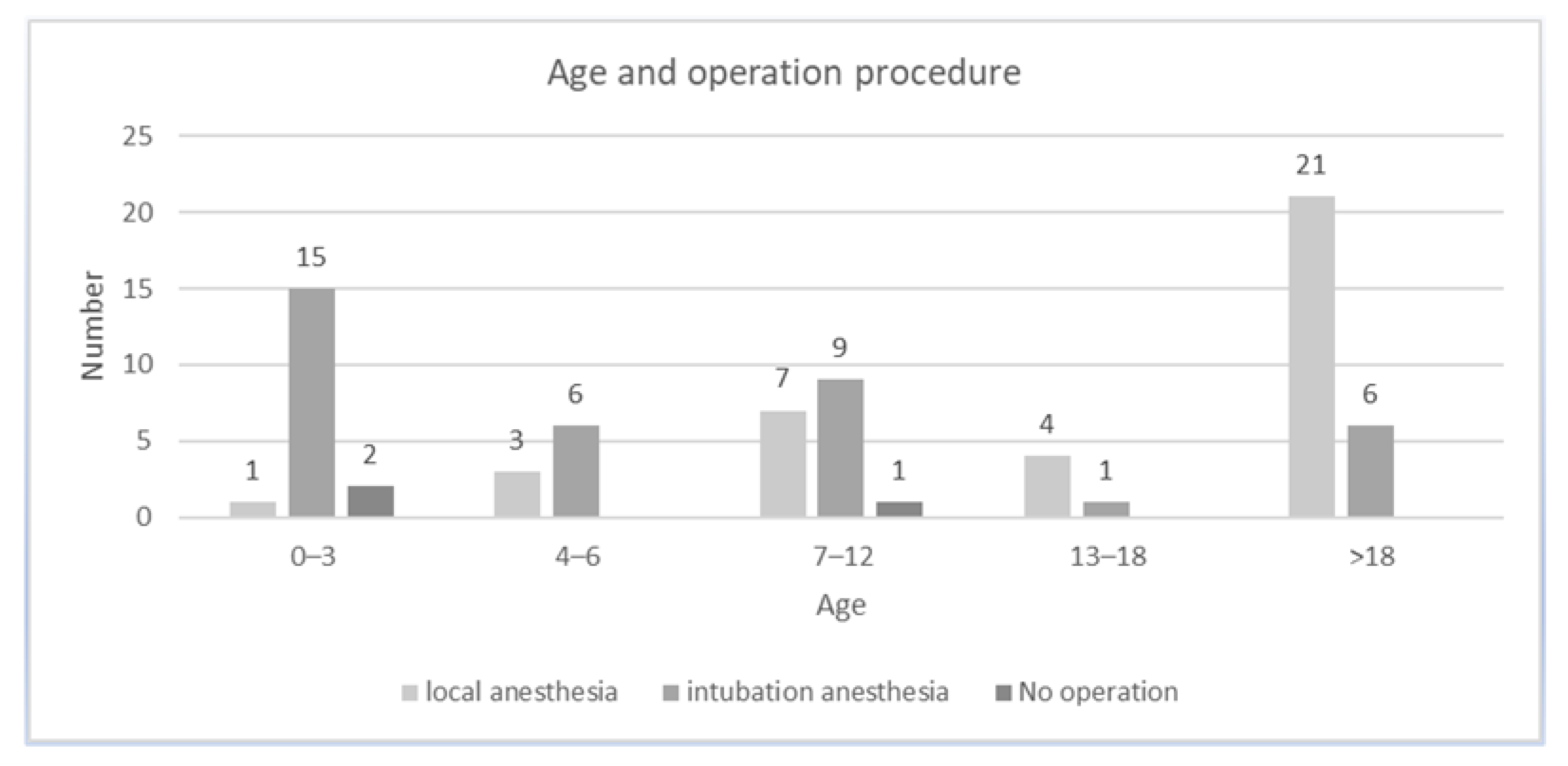
2.3. Treatment and Hospitalization
2.4. Pathogen Detection
3. Discussion
4. Materials and Methods
- Patient characteristics (age, gender);
- Own animal (±, if documented);
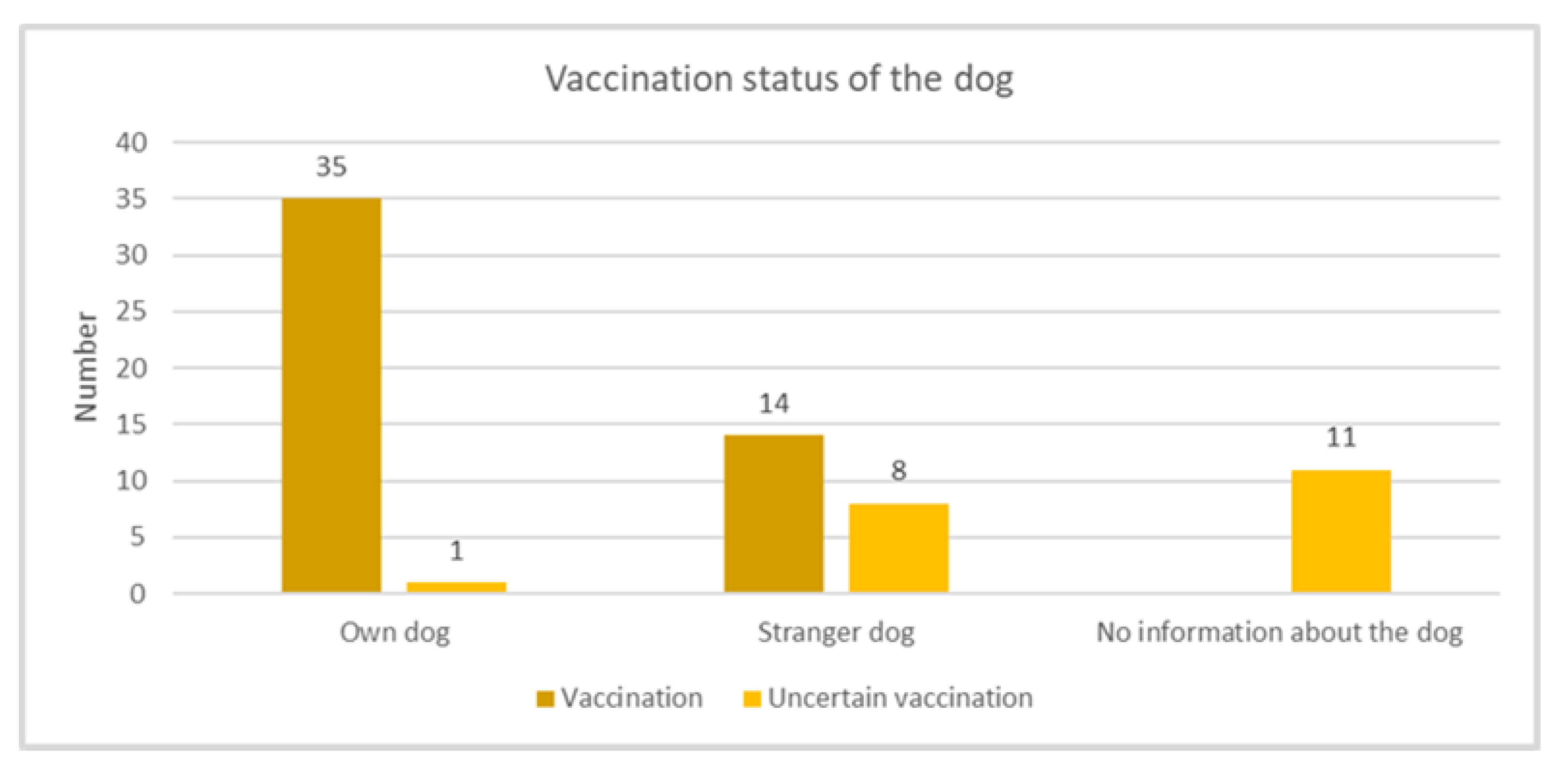
- Vaccine of the animal (±, if documented);
- Injury characteristics (area and extent of facial injury);
- Concomitant injuries (extremities, abdomen, thorax, etc.);
- Management;
- Pathogen;
- Duration of hospitalization;
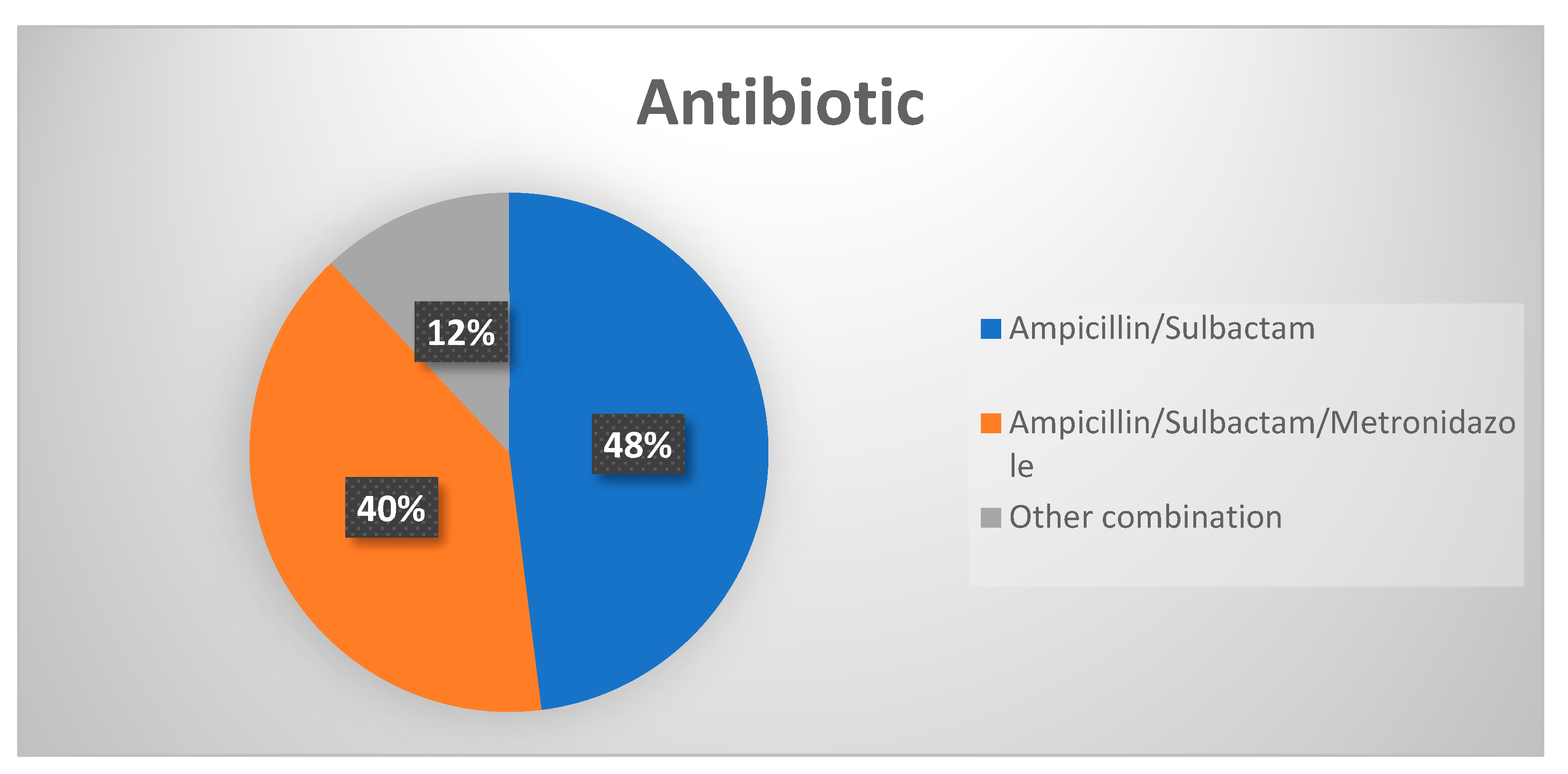
- Antibiotic therapy (intravenous and oral);
- Duration of antibiotic therapy.
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Merschin, D.; Ekkernkamp, A.; Seifert, J. The Vulnerable Heel of Achilles: Intratendinous Abscess Following a Cat Bite. Z. Orthop. Unfall. 2017, 155, 324–327. [Google Scholar] [CrossRef]
- Rothe, K.; Tsokos, M.; Handrick, W. Animal and Human Bite Wounds. Dtsch. Arztebl. Int. 2015, 112, 433–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfortmueller, C.A.; Efeoglou, A.; Furrer, H.; Exadaktylos, A.K. Dog bite injuries: Primary and secondary emergency department presentations—A retrospective cohort study. Scientific. World J. 2013, 2013, 393176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, S.; Quaresma, L.E.A.; Timoteo, C.A.; da Silva Fabris, A.L.; Faverani, L.P.; Francisconi, G.B.; Souza, F.A.; Júnior, I.R.G. The primary closure approach of dog bite injuries of the nose. J. Craniofac. Surg. 2014, 25, e216–e218. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, D.C.; Andre, T.B.; Robinson, A.D.; Squires, L.D.; Tollefson, T.T. Dog bites of the head and neck: An evaluation of a common pediatric trauma and associated treatment. Am. J. Otolaryngol. 2015, 36, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Stefanopoulos, P.K.; Tarantzopoulou, A.D. Management of facial bite wounds. Dent. Clin. North Am. 2009, 53, 691–705. [Google Scholar] [CrossRef]
- Chhabra, S.; Chhabra, N.; Gaba, S. Maxillofacial injuries due to animal bites. J. Maxillofac. Oral. Surg. 2015, 14, 142–153. [Google Scholar] [CrossRef] [Green Version]
- Bula-Rudas, F.J.; Olcott, J.L. Human and Animal Bites. Pediatr. Rev. 2018, 39, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, J.M.; Chi, J.J. Reconstruction of animal bite injuries to the head and neck. Curr. Opin. Otolaryngol. Head Neck Surg. 2019, 27, 407–412. [Google Scholar] [CrossRef]
- Hurt, J.B.; Maday, K.R. Management and treatment of animal bites. JAAPA 2018, 31, 27–31. [Google Scholar] [CrossRef]
- Pretty, I.A. Development and validation of a human bitemark severity and significance scale. J. Forensic. Sci. 2007, 52, 687–691. [Google Scholar] [CrossRef]
- Canzi, G.; De Ponti, E.; Fossati, C.; Novelli, G.; Cimbanassi, S.; Bozzetti, A.; Sozzi, D. Understanding the relevance of comprehensive facial injury (CFI) score: Statistical analysis of overall surgical time and length of stay outcomes. J. Craniomaxillofac. Surg. 2019, 47, 1456–1463. [Google Scholar] [CrossRef]
- Lyu, C.; Jewell, M.P.; Piron, J.; Ehnert, K.; Beeler, E.; Swanson, A.; Smith, L.V.; Kuo, T. Burden of Bites by Dogs and Other Animals in Los Angeles County, California, 2009–2011. Public Health Rep. 2016, 131, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Toure, G.; Angoulangouli, G.; Meningaud, J.P. Epidemiology and classification of dog bite injuries to the face: A prospective study of 108 patients. J. Plast. Reconstr. Aesthet. Surg. 2015, 68, 654–658. [Google Scholar] [CrossRef]
- Owczarczak-Garstecka, S.C.; Watkins, F.; Christley, R.; Westgarth, C. Online videos indicate human and dog behaviour preceding dog bites and the context in which bites occur. Sci. Rep. 2018, 8, 7147. [Google Scholar] [CrossRef] [PubMed]
- Piccart, F.; Dormaar, J.T.; Coropciuc, R.; Schoenaers, J.; Bila, M.; Politis, C. Dog Bite Injuries in the Head and Neck Region: A 20-Year Review. Craniomaxillofac. Trauma Reconstr. 2019, 12, 199–204. [Google Scholar] [CrossRef]
- Park, J.W.; Kim, D.K.; Jung, J.Y.; Lee, S.U.; Chang, I.; Kwak, Y.H.; Hwang, S. Dog-bite injuries in Korea and risk factors for significant dog-bite injuries: A 6-year cross-sectional study. PLoS ONE 2019, 14, e0210541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, N.M.; Fraser, D. Animal control measures and their relationship to the reported incidence of dog bites in urban Canadian municipalities. Can. Vet. J. 2013, 54, 145–149. [Google Scholar]
- Raval, P.; Khan, W.; Haddad, B.; Mahapatra, A.N. Bite injuries to the hand-review of the literature. Open Orthop. J. 2014, 8, 204–208. [Google Scholar] [CrossRef]
- Jaindl, M.; Oberleitner, G.; Endler, G.; Thallinger, C.; Kovar, F.M. Management of bite wounds in children and adults—An analysis of over 5000 cases at a level I trauma centre. Wien. Klin. Wochenschr. 2016, 128, 367–375. [Google Scholar] [CrossRef]
- Macedo, J.L.; Rosa, S.C.; Queiroz, M.N.; Gomes, T.G. Reconstruction of face and scalp after dog bites in children. Rev. Col. Bras. Cir. 2016, 43, 452–457. [Google Scholar] [CrossRef]
- Yadav, A.K.; Jaisani, M.R.; Pradhan, L.; Dongol, A.; Singh, A.; Acharya, P.; Sagtani, A. Animal Inflicted Maxillofacial Injuries: Treatment Modalities and Our Experience. J. Maxillofac. Oral. Surg. 2017, 16, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Kwak, Y.G.; Choi, S.H.; Kim, T.; Park, S.Y.; Seo, S.H.; Kim, M.B.; Choi, S.H. Clinical Guidelines for the Antibiotic Treatment for Community-Acquired Skin and Soft Tissue Infection. Infect. Chemother. 2017, 49, 301–325. [Google Scholar] [CrossRef]
- Ellis, R.; Ellis, C. Dog and cat bites. Am. Fam. Phys. 2014, 90, 239–243. [Google Scholar]
- Cavalcanti, A.L.; Porto, E.; Dos Santos, B.F.; Cavalcanti, C.L.; Cavalcanti, A.F.C. Facial dog bite injuries in children: A case report. Int. J. Surg. Case Rep. 2017, 41, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, I.; Saconato, H. Antibiotic prophylaxis for mammalian bites. Cochrane Database Syst. Rev. 2001. [Google Scholar] [CrossRef]
- Henton, J.; Jain, A. Cochrane corner: Antibiotic prophylaxis for mammalian bites (intervention review). J. Hand Surg. Eur. Vol. 2012, 37, 804–806. [Google Scholar] [CrossRef] [PubMed]
- Mensa, M.; Cubitt, J.J.; Javed, M.; Bragg, T. Dog bites and diabetic peripheral neuropathy: A dangerous combination. BMJ Case Rep. 2017, 2017. [Google Scholar] [CrossRef]
- Esposito, S.; Picciolli, I.; Semino, M.; Principi, N. Dog and cat bite-associated infections in children. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 971–976. [Google Scholar] [CrossRef]
- Erickson, B.P.; Feng, P.W.; Liao, S.D.; Modi, Y.S.; Ko, A.C.; Lee, W.W. Dog bite injuries of the eye and ocular adnexa. Orbit 2019, 38, 43–50. [Google Scholar] [CrossRef]
- Heitz, C.; Louzada, G.P.; Conci, R.A.; Rodrigues, R.L.; Fritscher, G.G. Primary Repair of a Complex Panfacial Fracture by Dog Bite. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1719. [Google Scholar] [CrossRef]
- Birdsey, M.; Edwards, G.; Abetz, J.; Jennings, N.; Mitra, B. Bite wounds and antibiotic prescription among patients presenting to an Australian emergency department. Int. Emerg. Nurs. 2016, 27, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, J.; Hoopes, J.; Epp, T. Scoping decades of dog evidence: A scoping review of dog bite-related sequelae. Can. J. Public Health 2019, 110, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Abrahamian, F.M.; Goldstein, E.J. Microbiology of animal bite wound infections. Clin. Microbiol. Rev. 2011, 24, 231–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, D.; Landon, A.; Powell, J.; Brown, G.R. Evaluating and treating mammalian bites. JAAPA 2017, 30, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Bhaumik, S.; Kirubakaran, R.; Chaudhuri, S. Primary closure versus delayed or no closure for traumatic wounds due to mammalian bite. Cochrane Database Syst. Rev. 2019, 12. [Google Scholar] [CrossRef]
- Kesting, M.R.; Holzle, F.; Pox, C.; Thurmuller, P.; Wolff, K.D. Animal bite injuries to the head: 132 cases. Br. J. Oral. Maxillofac. Surg. 2006, 44, 235–239. [Google Scholar] [CrossRef]
- Agrawal, A.; Kumar, P.; Singhal, R.; Singh, V.; Bhagol, A. Animal Bite Injuries in Children: Review of Literature and Case Series. Int. J. Clin. Pediatr. Dent. 2017, 10, 67–72. [Google Scholar] [CrossRef]
- McGuire, C.; Morzycki, A.; Simpson, A.; Williams, J.; Bezuhly, M. Dog Bites in Children: A Descriptive Analysis. Plast. Surg. 2018, 26, 256–262. [Google Scholar] [CrossRef]
- Shen, J.; Rouse, J.; Godbole, M.; Wells, H.L.; Boppana, S.; Schwebel, D.C. Systematic Review: Interventions to Educate Children About Dog Safety and Prevent Pediatric Dog-Bite Injuries: A Meta-Analytic Review. J. Pediatr. Psychol. 2017, 42, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Murray, G.E. Examining evidence on dog bite injuries and their management in children. Nurs. Child. Young People 2017, 29, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Deleyiannis, F.W.; Wilkinson, C.; O’Neill, B.R. Neurosurgical sequelae of domestic dog attacks in children. J. Neurosurg. Pediatr. 2017, 19, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Decade of Life | n | % |
|---|---|---|
| 0–3 | 18 | 24 |
| 4–6 | 9 | 12 |
| 7–12 | 17 | 22.67 |
| 13–18 | 5 | 6.67 |
| >18 | 26 | 34.67 |
| Specific Body Part | Number of Injuries |
|---|---|
| Head | 2 |
| Upper eyelid/forehead | 13 |
| Lower eyelid/cheek | 37 |
| Ear | 3 |
| Nose | 5 |
| Upper lip | 18 |
| Lower lip | 12 |
| Chin | 4 |
| Neck | 3 |
| Hand | 3 |
| Wound infection/abscess | 13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spille, J.; Schulz, J.; Spille, D.C.; Naujokat, H.; Wieker, H.; Wiltfang, J.; Gülses, A. Microbiological Characteristics and Surgical Management of Animal-Bite-Related Oral & Maxillofacial Injuries: A Single Center’s Experience. Antibiotics 2021, 10, 998. https://doi.org/10.3390/antibiotics10080998
Spille J, Schulz J, Spille DC, Naujokat H, Wieker H, Wiltfang J, Gülses A. Microbiological Characteristics and Surgical Management of Animal-Bite-Related Oral & Maxillofacial Injuries: A Single Center’s Experience. Antibiotics. 2021; 10(8):998. https://doi.org/10.3390/antibiotics10080998
Chicago/Turabian StyleSpille, Johannes, Juliane Schulz, Dorothee Cäcilia Spille, Hendrik Naujokat, Henning Wieker, Jörg Wiltfang, and Aydin Gülses. 2021. "Microbiological Characteristics and Surgical Management of Animal-Bite-Related Oral & Maxillofacial Injuries: A Single Center’s Experience" Antibiotics 10, no. 8: 998. https://doi.org/10.3390/antibiotics10080998
APA StyleSpille, J., Schulz, J., Spille, D. C., Naujokat, H., Wieker, H., Wiltfang, J., & Gülses, A. (2021). Microbiological Characteristics and Surgical Management of Animal-Bite-Related Oral & Maxillofacial Injuries: A Single Center’s Experience. Antibiotics, 10(8), 998. https://doi.org/10.3390/antibiotics10080998