
Validation of Vancomycin Area under the Concentration—Time Curve Estimation by the Bayesian Approach Using One-Point Samples for Predicting Clinical Outcomes in Patients with Methicillin-Resistant Staphylococcus aureus Infections

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
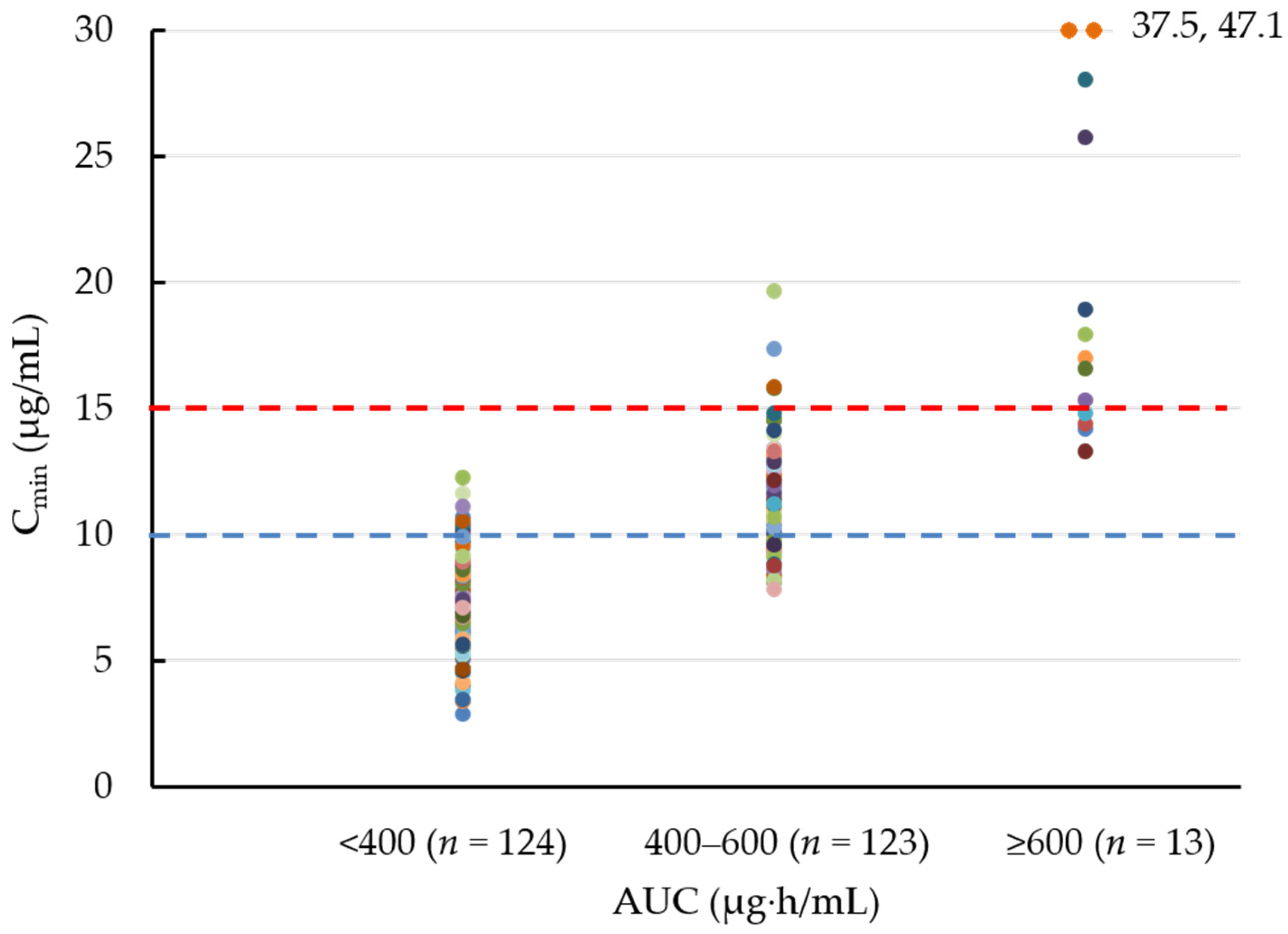
2.2. Bayesian Estimation of the AUC and the Cmin on Day 1, Day 2, and the Steady-State
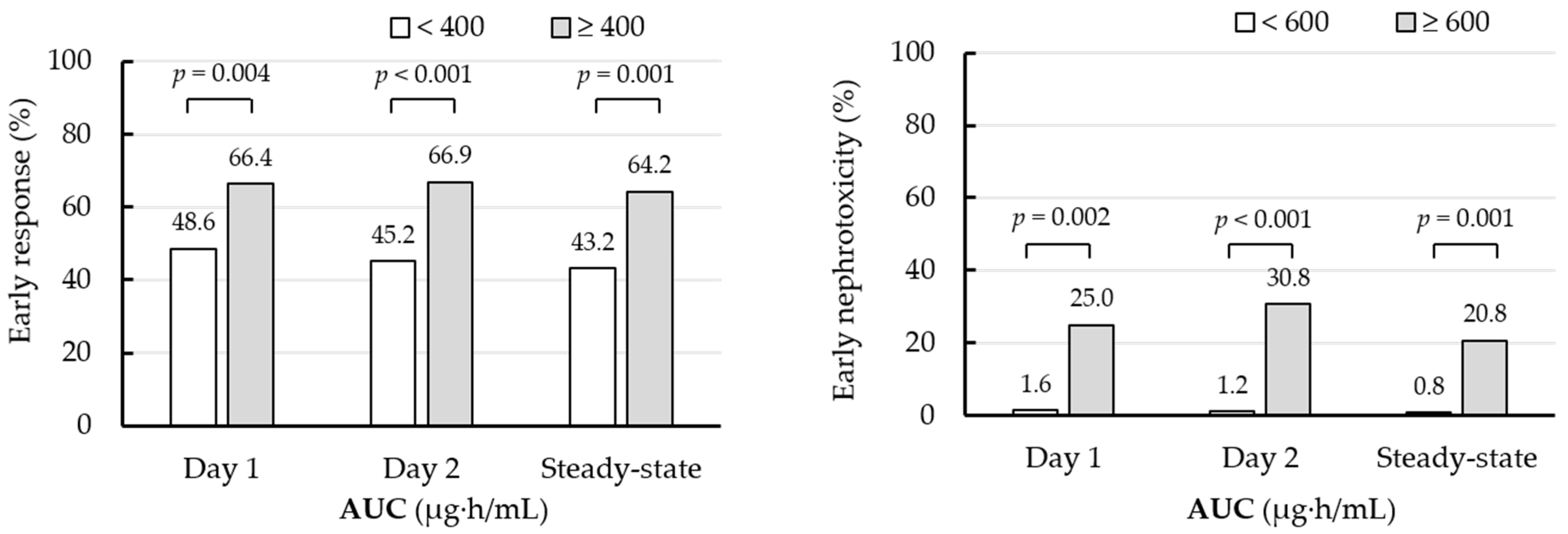
2.3. Early Treatment Response and Early Nephrotoxicity
2.4. Sub-Analyses of Clinical Outcomes According to Day 2 AUC Cutoff Values in Patients with Vancomycin q12h and q24h Administration, and Those with High/Moderate-Risk and Low-Risk MRSA Infections
3. Discussion
4. Materials and Methods
4.1. Patients and Protocol
4.2. AUC Evaluation
4.3. Adverse Effects and Clinical Efficacy
4.4. Subgroup Analyses
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectiousdiseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: Executive summary. Clin. Infect. Dis. 2011, 52, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Basic pharmacodynamics of antibacterials with clinical applications to the use of beta-lactams, glycopeptides, and linezolid. Infect. Dis. Clin. N. Am. 2003, 17, 479–501. [Google Scholar] [CrossRef]
- Rybak, M.J. The Pharmacokinetic and Pharmacodynamic Properties of Vancomycin. Clin. Infect. Dis. 2006, 42, S35–S39. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2020, 77, 835–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Men, P.; Li, H.B.; Zhai, S.D.; Zhao, R.S. Association between the AUC0-24/MIC Ratio of Vancomycin and Its Clinical Effectiveness: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e014622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neely, M.N.; Youn, G.; Jones, B.; Jelliffe, R.W.; Drusano, G.L.; Rodvold, K.A.; Lodise, T.P. Are Vancomycin Trough Concentrations Adequate for Optimal Dosing? Antimicrob. Agents Chemother. 2013, 58, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, C.J. Questioning the accuracy of trough concentrations as surrogates for area under the curve in determining van-comycin safety. Ther. Adv. Drug. Saf. 2014, 5, 118–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsuura, M.; Moriyama, H.; Kojima, N.; Mizukami, Y.; Tashiro, S.; Osa, S.; Enoki, Y.; Taguchi, K.; Oda, K.; Fujii, S.; et al. The monitoring of vancomycin: A systematic review and meta-analyses of area under the concentration-time curve-guided dosing and trough-guided dosing. BMC Infect. Dis. 2021, 21, 153. [Google Scholar] [CrossRef] [PubMed]
- Oda, K.; Hashiguchi, Y.; Kimura, T.; Tsuji, Y.; Shoji, K.; Takahashi, Y.; Matsumoto, K.; Kawamura, H.; Saito, H.; Takesue, Y. Performance of Area under the Concentration-Time Curve Estimations of Vancomycin with Limited Sampling by a Newly Developed Web Application. Pharm. Res. 2021, 38, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.; Lomaestro, B.; Rotschafer, J.C.; Moellering, R., Jr.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2009, 66, 82–98. [Google Scholar] [CrossRef] [PubMed]
- Casapao, A.M.; Lodise, T.P.; Davis, S.L.; Claeys, K.C.; Kullar, R.; Levine, D.P.; Rybak, M.J. Association between vancomycin day 1 exposure profile and outcomes among pa-tients with methicillin-resistant Staphylococcus aureus infective endocarditis. Antimicrob. Agents Chemother. 2015, 59, 2978–2985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodise, T.P., Jr.; Rosenkranz, S.L.; Finnemeyer, M.; Evans, S.; Sims, M.; Zervos, M.J.; Creech, C.B.; Patel, P.C.; Keefer, M.; Riska, P.; et al. The Emperor’s New Clothes: Prospective Observational Evaluation of the Association Between Initial Vancomycin Exposure and Failure Rates Among Adult Hospitalized Patients with Methicillin-resistant Staphylococcus aureus Bloodstream Infections (PROVIDE). Clin. Infect. Dis. 2020, 70, 1536–1545. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Takesue, Y.; Ohmagari, N.; Mochizuki, T.; Mikamo, H.; Seki, M.; Takakura, S.; Tokimatsu, I.; Takahashi, Y.; Kasahara, K.; et al. Practice guidelines for therapeutic drug monitoring of vancomycin: A consensus review of the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. J. Infect. Chemother. 2013, 19, 365–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wunderink, R.G.; Niederman, M.S.; Kollef, M.H.; Shorr, A.F.; Kunkel, M.J.; Baruch, A.; McGee, W.T.; Reisman, A.; Chastre, J. Linezolid in Methicillin-Resistant Staphylococcus aureus Nosocomial Pneumonia: A Randomized, Controlled Study. Clin. Infect. Dis. 2012, 54, 621–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wayne, P.A. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. Inf. Suppl. 2011, 31, 100–121. [Google Scholar]
- Yasuhara, M.; Iga, T.; Zenda, H.; Okumura, K.; Oguma, T.; Yano, Y.; Hori, R. Population pharmacokinetics of vancomycin in Japanese adult patients. Ther. Drug. Monit. 1998, 20, 139–148. [Google Scholar] [CrossRef]
- Ueda, T.; Takesue, Y.; Nakajima, K.; Ichiki, K.; Doita, A.; Wada, Y.; Tsuchida, T.; Takahashi, Y.; Ishihara, M.; Ikeuchi, H.; et al. Enhanced loading regimen of teicoplanin is necessary to achieve therapeutic pharmacokinetics levels for the improvement of clinical outcomes in patients with renal dysfunction. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Hanaki, H.; Kimura, T.; Nemoto, M.; Higashihara, M.; Yokota, H.; Oda, S.; Akiyama, N.; Miyao, N.; Yoshida, M.; et al. Clinical efficacy and safety of arbekacin sulfate in patients with MRSA sepsis or pneumonia: A multi-institutional study. J. Infect. Chemother. 2013, 19, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Takesue, Y.; Nakajima, K.; Ichiki, K.; Ishikawa, K.; Takai, Y.; Yamada, K.; Tsuchida, T.; Otani, N.; Takahashi, Y.; et al. Clinical efficacy and safety in patients treated with teicoplanin with a target trough concentration of 20 μg/mL using a regimen of 12 mg/kg for five doses within the initial 3 days. BMC Pharmacol. Toxicol. 2020, 21, 50. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pharmacokinetic Parameter | Pharmacokinetic Parameters of the Initial Vancomycin Regimen | |||
|---|---|---|---|---|
| Day 1 | Day 2 | Steady-State | ||
| AUC (µg·h/mL) | Median (IQR) | 382.7 (319.4–455.4) | 403.9 (332.4–454.0) | 422.4 (351.1–485.8) |
| <400 | 144 (55.4%) | 124 (47.7%) | 95 (36.5%) | |
| 400–600 | 104 (40.0%) | 123 (47.3%) | 141 (54.2%) | |
| ≥600 | 12 (4.6%) | 13 (5.0%) | 24 (9.2%) | |
| Cmin (μg/mL) | Median (IQR) | 8.0 (5.9–10.1) | 9.8 (7.5–11.3) | 10.3 (7.9–12.3) |
| <10 | 191 (73.5%) | 140 (53.8%) | 121 (46.5%) | |
| 10–15 | 63 (24.2%) | 107 (41.2%) | 110 (42.3%) | |
| 15–20 | 2 (0.8%) | 9 (3.5%) | 20 (7.7%) | |
| ≥20 | 4 (1.5%) | 4 (1.5%) | 9 (3.5%) | |
| Factors | No. of Patients with an Early Treatment Response (%) | p Value by Univariate Analysis | Adjusted Odds Ratio (95% Confidence Interval) | p Value by Multivariate Analyses | |
|---|---|---|---|---|---|
| Patients with Factor | Patients without Factor | ||||
| Day 2 AUC ≥ 400 µg·h/mL | 91/136 (66.9%) | 56/124 (45.2%) | <0.001 | 2.02 (1.15–3.53) | 0.014 |
| >65 years | 75/145 (51.7%) | 72/115 (62.6%) | 0.079 | ||
| Heart disease | 37/77 (48.1%) | 110/183 (60.1%) | 0.073 | ||
| Collagen disease | 12/35 (34.3%) | 135/225 (60.0%) | 0.004 | 0.28 (0.12–0.63) | 0.002 |
| Chronic respiratory disease | 12/30 (40.0%) | 135/230 (58.7%) | 0.052 | ||
| Serum albumin <2.5 g/dL | 38/79 (48.1%) | 109/181 (60.2%) | 0.070 | ||
| Ventilator use | 16/54 (29.6%) | 131/206 (63.6%) | <0.001 | ||
| Intensive care unit stay | 12/45 (26.7%) | 135/215 (62.8%) | <0.001 | 0.34 (0.15–0.78) | 0.011 |
| APCHE II score >10 | 34/92 (37.0%) | 113/168 (67.3%) | <0.001 | 0.44 (0.23–0.84) | 0.014 |
| Immunosuppressive therapy | 2/9 (22.2%) | 145/251 (57.8%) | 0.043 | ||
| VAP | 10/38 (26.3%) | 137/222 (61.7%) | <0.001 | ||
| Skin and soft tissue infection | 50/63 (79.4%) | 97/197 (49.2%) | <0.001 | ||
| Respiratory tract infectionsexcept for VAP | 30/68 (44.1%) | 117/192 (60.9%) | 0.016 | ||
| Factors | No of Patients with Early Nephrotoxicity (%) | p Value by Univariate Analysis | Adjusted Odds Ratio (95% Confidence Interval) | p Value by Multivariate Analyses | |
|---|---|---|---|---|---|
| Patients with Factor | Patients without Factor | ||||
| Day 2 AUC ≥ 600 µg·h/mL | 4/13 (30.8%) | 3/247 (1.2%) | <0.001 | 44.77 (6.65–301.65) | <0.001 |
| Concomitant piperalin/tazobactam | 5/54 (9.3%) | 2/206 (1.0%) | 0.005 | 12.93 (1.87–89.49) | 0.010 |
| Pharmacokinetics Parameter | Early Treatment Response, No. of Patients (%) | ||||
|---|---|---|---|---|---|
| q12h Administration | q24h Administration | ||||
| a. Early treatment response | |||||
| AUC on day 2 (µg·h/mL) | <400 | 44/92 (47.8%) | reference | 12/32 (37.5%) | reference |
| ≥400 | 77/110 (70.0%) | p = 0.001 | 14/26 (53.8%) | p = 0.213 | |
| b. Early nephrotoxicity | |||||
| AUC on day 2 (µg·h/mL) | <600 | 2/189 (1.1%) | reference | 1/58 (1.7%) | reference |
| ≥600 | 4/13 (30.8%) | p < 0.001 | 0/0 | – | |
| Pharmacokinetics Parameter | Early Treatment Response, No. of Patients (%) | ||||
|---|---|---|---|---|---|
| High/Moderate-Risk MRSA Infections | Low-Risk MRSA Infections | ||||
| a. Early treatment response | |||||
| AUC on day 2 (µg·h/mL) | <400 | 19/51 (37.3%) | reference | 37/73 (50.7%) | reference |
| ≥400 | 29/54 (53.7%) | p = 0.091 | 62/82 (75.6%) | p = 0.001 | |
| b. Early nephrotoxicity | |||||
| AUC on day 2 (µg·h/mL) | <600 | 1/100 (1.0%) | reference | 2/147 (1.4%) | reference |
| ≥600 | 2/5 (40.0%) | p = 0.005 | 2/8 (25.0%) | p = 0.013 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueda, T.; Takesue, Y.; Nakajima, K.; Ichiki, K.; Ishikawa, K.; Yamada, K.; Tsuchida, T.; Otani, N.; Takahashi, Y.; Ishihara, M.; et al. Validation of Vancomycin Area under the Concentration—Time Curve Estimation by the Bayesian Approach Using One-Point Samples for Predicting Clinical Outcomes in Patients with Methicillin-Resistant Staphylococcus aureus Infections. Antibiotics 2022, 11, 96. https://doi.org/10.3390/antibiotics11010096
Ueda T, Takesue Y, Nakajima K, Ichiki K, Ishikawa K, Yamada K, Tsuchida T, Otani N, Takahashi Y, Ishihara M, et al. Validation of Vancomycin Area under the Concentration—Time Curve Estimation by the Bayesian Approach Using One-Point Samples for Predicting Clinical Outcomes in Patients with Methicillin-Resistant Staphylococcus aureus Infections. Antibiotics. 2022; 11(1):96. https://doi.org/10.3390/antibiotics11010096
Chicago/Turabian StyleUeda, Takashi, Yoshio Takesue, Kazuhiko Nakajima, Kaoru Ichiki, Kaori Ishikawa, Kumiko Yamada, Toshie Tsuchida, Naruhito Otani, Yoshiko Takahashi, Mika Ishihara, and et al. 2022. "Validation of Vancomycin Area under the Concentration—Time Curve Estimation by the Bayesian Approach Using One-Point Samples for Predicting Clinical Outcomes in Patients with Methicillin-Resistant Staphylococcus aureus Infections" Antibiotics 11, no. 1: 96. https://doi.org/10.3390/antibiotics11010096
APA StyleUeda, T., Takesue, Y., Nakajima, K., Ichiki, K., Ishikawa, K., Yamada, K., Tsuchida, T., Otani, N., Takahashi, Y., Ishihara, M., Takubo, S., Ikeuchi, H., Uchino, M., Kimura, T., Matsumoto, K., Oda, K., & Kimura, T. (2022). Validation of Vancomycin Area under the Concentration—Time Curve Estimation by the Bayesian Approach Using One-Point Samples for Predicting Clinical Outcomes in Patients with Methicillin-Resistant Staphylococcus aureus Infections. Antibiotics, 11(1), 96. https://doi.org/10.3390/antibiotics11010096