
Antibiotic Therapy in the Treatment of COVID-19 Pneumonia: Who and When?

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Recruitment
2.2. Data Collection
2.3. Study Endpoints
2.4. Statistical Analysis
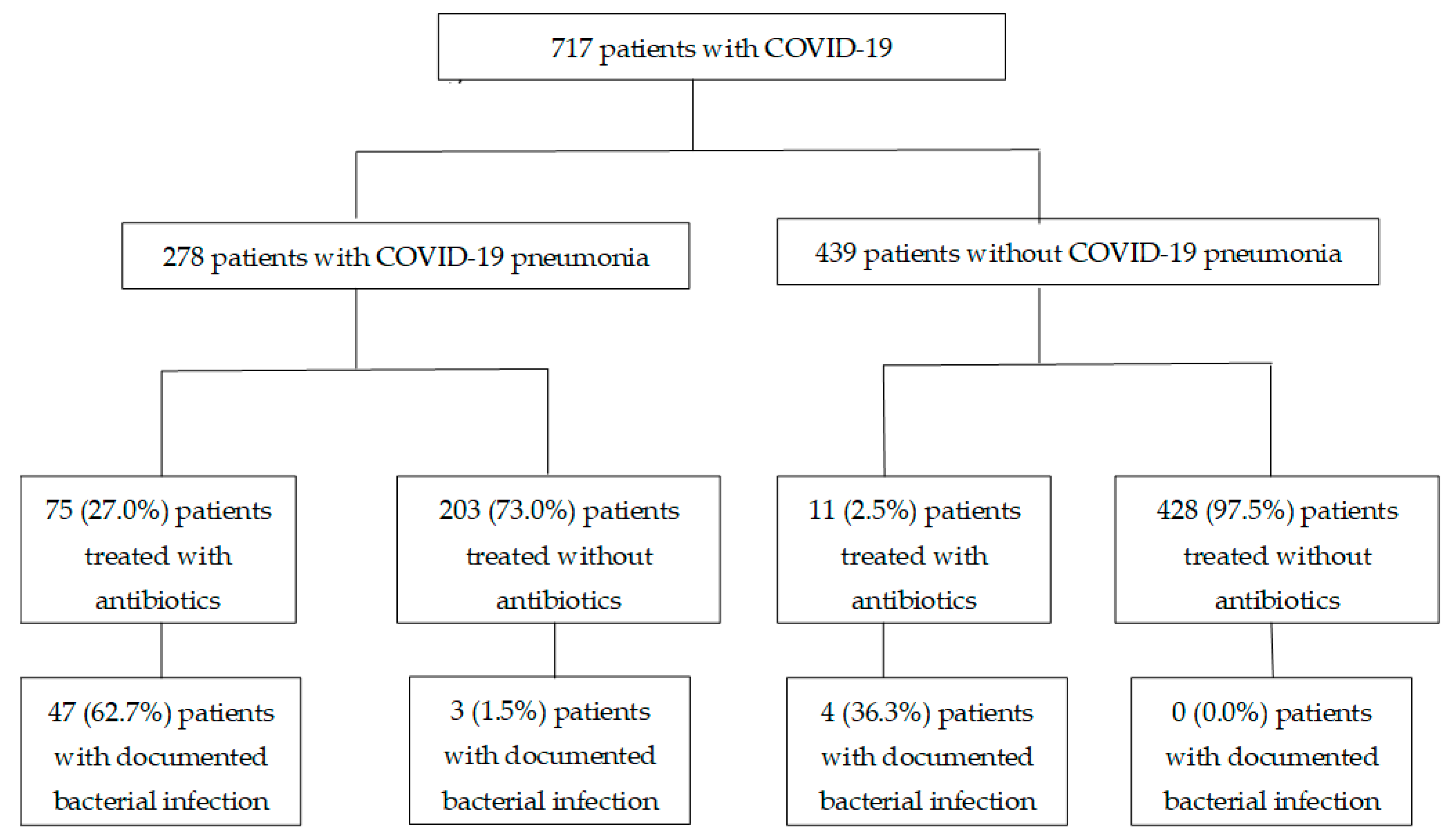
3. Results
3.1. Clinical Features
3.2. Evaluation of Predictors for Bacterial Co-Infection
3.3. Antibiotic Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| RT-PCR | Reverse-transcriptase polymerase chain reaction |
| WHO | World Health Organization |
| ISARIC | International Severe Acute Respiratory and Emerging Infection Consortium |
| AUC | Area under the curve |
| ICU | Intensive care unit |
References
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. COVID-19 Researchers Group. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Clinical Management of COVID-19: Living Guidance. 25 January 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 10 February 2021).
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 10 February 2021).
- Sieswerda, E.; de Boer, M.G.J.; Bonten, M.M.J.; Boersma, W.G.; Jonkers, R.E.; Aleva, R.M.; Kullberg, B.J.; Schouten, J.A.; van de Garde, E.M.; Verheij, T.J.; et al. Recommendations for antibacterial therapy in adults with COVID-19—An evidence-based guideline. Clin. Microbiol. Infect. 2021, 27, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Søgaard, K.K.; Baettig, V.; Osthoff, M.; Marsch, S.; Leuzinger, K.; Schweitzer, M.; Meier, J.; Bassetti, S.; Bingisser, R.; Nickel, C.H.; et al. Community-acquired and hospital-acquired respiratory tract infection and bloodstream infection in patients hospitalized with COVID-19 pneumonia. J. Intensive Care 2021, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, A.S.; Klugman, K.P. COVID-19 pneumonia and the appropriate use of antibiotics. Lancet Glob. Health 2020, 8, e1453–e1454. [Google Scholar] [CrossRef]
- World Health Organization. The 2019 WHO AWaRe Classification of Antibiotics for Evaluation and Monitoring of Use; WHO/EMP/IAU/2019.11; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Sharifpour, M.; Rangaraju, S.; Liu, M.; Alabyad, D.; Nahab, F.B.; Creel-Bulos, C.M.; Jabaley, C.S.; Emory COVID-19 Quality & Clinical Research Collaborative. C-Reactive protein as a prognostic indicator in hospitalized patients with COVID-19. PLoS ONE 2020, 15, e0242400. [Google Scholar] [CrossRef] [PubMed]
- Van Berkel, M.; Kox, M.; Frenzel, T.; Pickkers, P.; Schouten, J.; RCI-COVID-19 Study Group. Biomarkers for antimicrobial stewardship: A reappraisal in COVID-19 times? Crit. Care 2020, 24, 600. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| All COVID-19 Patients (n = 717) | Cut-Off | Sensitivity (%) | Specificity (%) | AUC (95% CI) |
|---|---|---|---|---|
| White blood cell count (109/L) | ≥7.2 | 64.8 | 78.4 | 0.767 (0.700–0.838) |
| Procalcitonin (ng/mL) a | ≥0.11 | 47.2 | 82.6 | 0.673 (0.570–0.777) |
| C-reactive protein (mg/L) | ≥59.8 | 66.7 | 86.0 | 0.822 (0.756–0.887) |
| COVID-19 pneumonia (n = 278) | ||||
| White blood cell count (109/L) | ≥7.2 | 68.0 | 67.3 | 0.719 (0.639–0.798) |
| Procalcitonin (ng/mL) b | ≥0.11 | 48.6 | 73.5 | 0.607 (0.493–0.721) |
| C-reactive protein (mg/L) | ≥73.2 | 68.0 | 69.7 | 0.720 (0.633–0.808) |
| 30-Day Mortality | |||
|---|---|---|---|
| Characteristics | Univariate analysis Odd ratio (95% CI) | Multivariate analysis Odd ratio (95% CI) | p |
| Age, years, median, IQR | 1.175 (1.100–1.259) | 1.265 (1.070–1.495) | 0.006 |
| Male (%) | 1.245 (0.356–4.356) | - | |
| Charlson’s score | 1.536 (1.114–2.118) | 0.860 (0.392–1.887) | 0.707 |
| Peak white cell count, 109/L | 1.016 (0.996–1.036) | - | |
| Peak C-reactive protein, mg/L | 1.015 (1.008–1.021) | 1.021 (1.002–1.039) | 0.023 |
| ICU admission at diagnosis of COVID-19 pneumonia (%) | 5.298 (1.453–19.307) | 0.024 (0.000–9.285) | 0.219 |
| Fraction of inspired oxygen, %, median, IQR | 1.041 (1.019–1.064) | 0.939 (0.863–1.021) | 0.140 |
| Mechanical ventilation | 8.727 (2.0314–37.493) | 470.581 (0.682–324642.500) | 0.065 |
| CURB-65 a | 3.897 (2.141–7.094) | 1.351 (0.382–4.786) | 0.470 |
| Remdesivir | 4.631 (1.139–18.836) | 1.703 (0.135–21.467) | 0.680 |
| Documented suspected or confirmed bacterial infection | 14.286 (3.640–56.061) | 0.652 (0.053–7.967) | 0.738 |
| Antibiotic therapy | 31.076 (3.904–247.400) | 14.492 (0.533–393.875) | 0.113 |
| Hospital Mortality | |||
|---|---|---|---|
| Characteristics | Univariate analysis | Multivariate analysis | p |
| Age, years, median, IQR | 1.163 (1.094–1.236) | 1.291 (1.103–1.510) | 0.001 |
| Male (%) | 1.622 (0.487–5.400) | - | - |
| Charlson’s score | 1.515 (1.111–2.065) | 0.748 (0.358–1.566) | 0.442 |
| Peak white cell count, 109/L | 1.016 (0.996–1.036) | - | - |
| Peak C-reactive protein, mg/L | 1.015 (1.009–1.021) | 1.026 (1.011–1.043) | 0.001 |
| ICU admission at diagnosis of COVID-19 pneumonia (%) | 4.086 (1.176–14.194) | 0.015 (0.000–6.929) | 0.179 |
| Fraction of inspired oxygen, %, median, IQR | 1.036 (1.015–1.058) | 0.930 (0.858–1.007) | 0.075 |
| Mechanical ventilation | 6.927 (1.667–28.786) | 618.086 (0.847–451009.000) | 0.056 |
| CURB-65 a | 3.381 (1.980–5.772) | 1.100 (0.361–3.351) | 0.867 |
| Remdesivir | 3.675 (0.935–14.439) | - | - |
| Documented suspected or confirmed bacterial infection | 8.495 (2.650–27.234) | 0.826 (0.074–9.221) | 0.876 |
| Antibiotic therapy | 10.256 (2.739–38.402) | 3.690 (0.240–56.811) | 0.349 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, T.M.; Ong, S.W.X.; Loo, A.Y.X.; Tan, S.H.; Tay, H.L.; Yap, M.Y.; Lye, D.C.; Lee, T.H.; Young, B.E. Antibiotic Therapy in the Treatment of COVID-19 Pneumonia: Who and When? Antibiotics 2022, 11, 184. https://doi.org/10.3390/antibiotics11020184
Ng TM, Ong SWX, Loo AYX, Tan SH, Tay HL, Yap MY, Lye DC, Lee TH, Young BE. Antibiotic Therapy in the Treatment of COVID-19 Pneumonia: Who and When? Antibiotics. 2022; 11(2):184. https://doi.org/10.3390/antibiotics11020184
Chicago/Turabian StyleNg, Tat Ming, Sean W. X. Ong, Audrey Y. X. Loo, Sock Hoon Tan, Hui Lin Tay, Min Yi Yap, David C. Lye, Tau Hong Lee, and Barnaby E. Young. 2022. "Antibiotic Therapy in the Treatment of COVID-19 Pneumonia: Who and When?" Antibiotics 11, no. 2: 184. https://doi.org/10.3390/antibiotics11020184
APA StyleNg, T. M., Ong, S. W. X., Loo, A. Y. X., Tan, S. H., Tay, H. L., Yap, M. Y., Lye, D. C., Lee, T. H., & Young, B. E. (2022). Antibiotic Therapy in the Treatment of COVID-19 Pneumonia: Who and When? Antibiotics, 11(2), 184. https://doi.org/10.3390/antibiotics11020184