
Point Prevalence Survey of Antibiotic Use across 13 Hospitals in Uganda


 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Antibiotic Prevalence
2.1.1. Prevalence by Indication
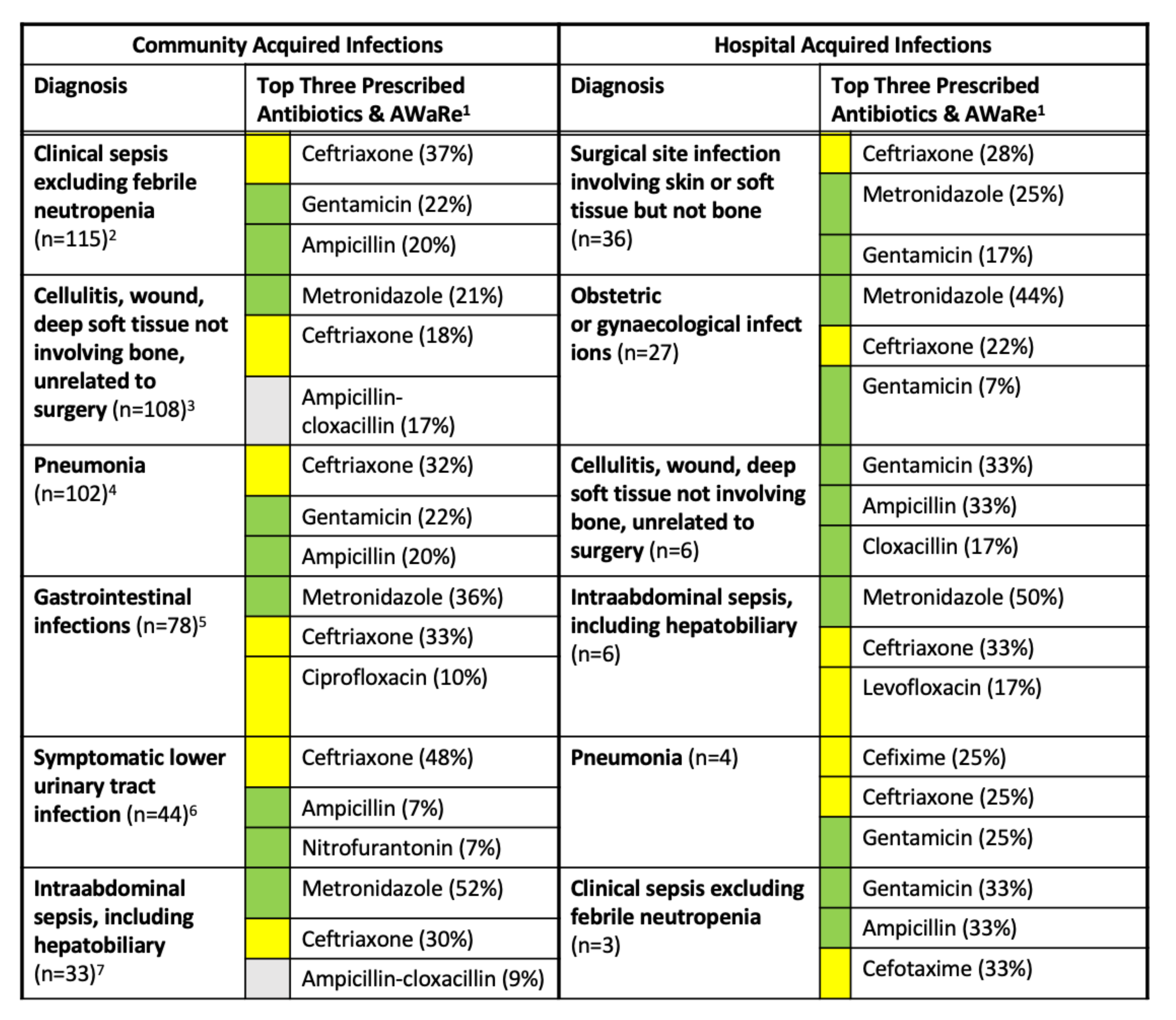
2.1.2. Prevalence by Diagnosis
2.1.3. Prevalence by Hospital
2.2. Antibiotic Stewardship Indicators
2.2.1. Guideline Compliance
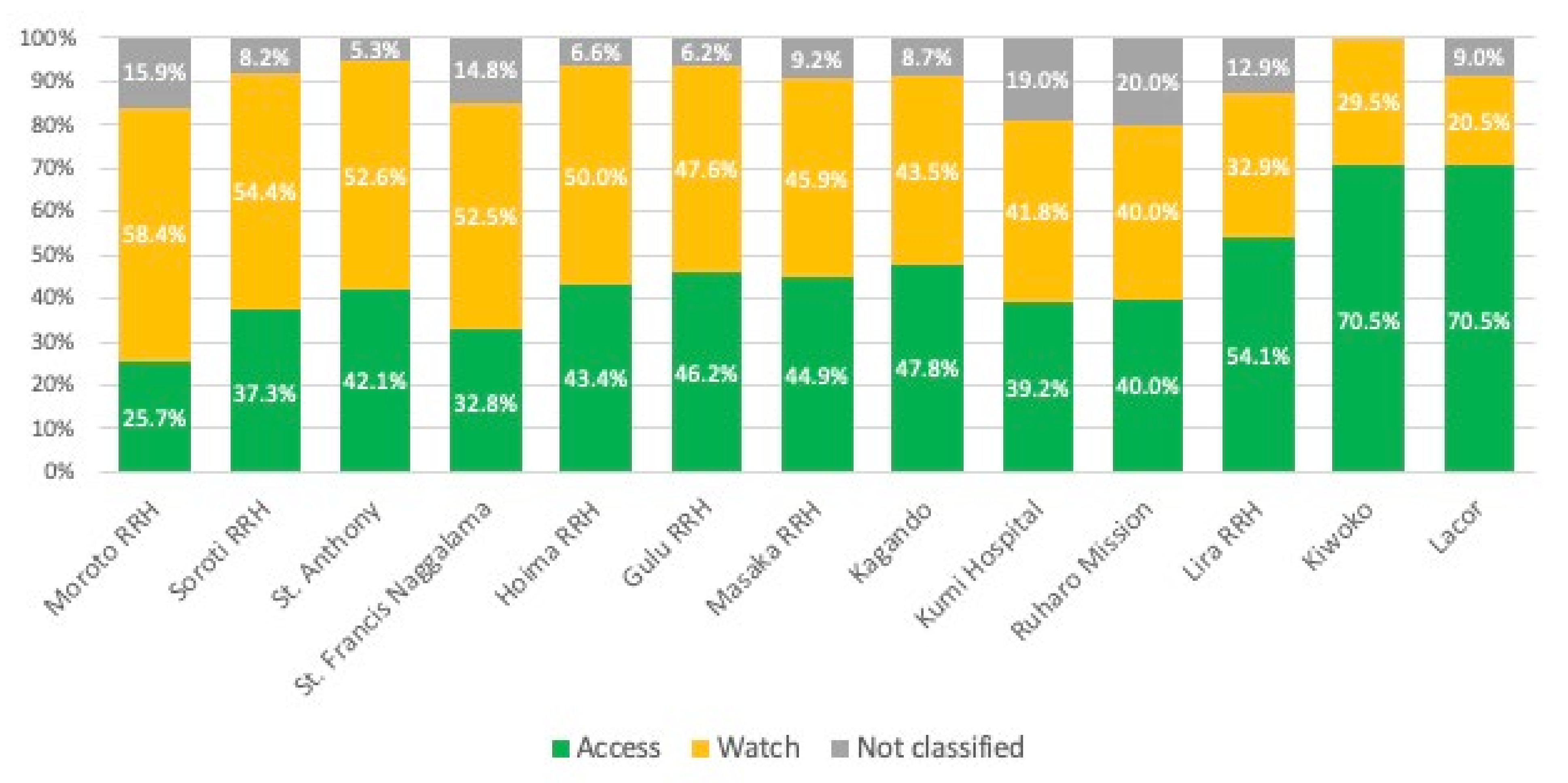
2.2.2. WHO AWaRe Classification
2.2.3. Missed Doses
2.2.4. Route of Administration
2.3. Antibiotics per Patient
Antibiotics by Sex
3. Discussion
3.1. Antibiotic Use and Prevalence by Patient Characteristics
3.2. Antibiotic Use Based on Uganda Clinical Guidelines and Hospital Setting
3.3. Proportion of Prescribed Antibiotic Doses Not Administered to Patients
3.4. Route of Administration
3.5. WHO AWaRE Antibiotic Classification
3.6. Limitations
4. Methods and Materials
4.1. Data Collection
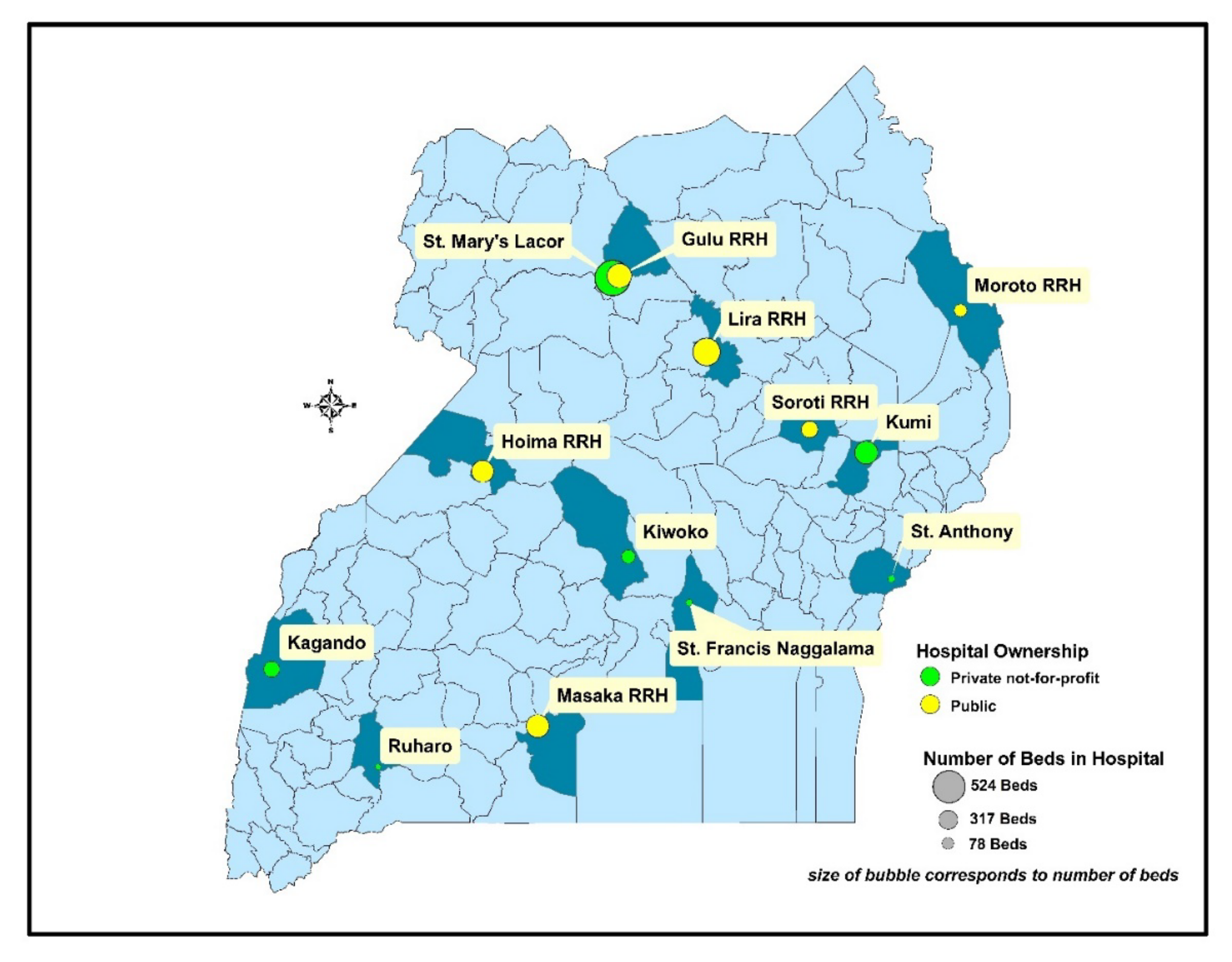
4.1.1. Setting
4.1.2. Data Collection
4.1.3. Study Ethics and Approval
4.2. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Knight, G.M.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.I.; Rao, P.C.; Dolecek, C.; Day, N.P.J.; Stergachis, A.; Lopez, A.D.; Murray, C.J.L. Measuring and mapping the global burden of antimicrobial resistance. BMC Med. 2018, 16, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernando-Amado, S.; Coque, T.M.; Baquero, F.; Martínez, J.L. Defining and combating antibiotic resistance from One Health and Global Health perspectives. Nat. Microbiol. 2019, 4, 1432–1442. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Review on Antimicrobial Resistance Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. London: Review on Antimicrobial Resistance. 2014. Available online: https://amr-review.org/Publications.html (accessed on 21 December 2021).
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442. [Google Scholar] [CrossRef]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef]
- Afshinnekoo, E.; Bhattacharya, C.; Burguete-García, A.; Castro-Nallar, E.; Deng, Y.; Desnues, C.; Dias-Neto, E.; Elhaik, E.; Iraola, G.; Jang, S.; et al. COVID-19 drug practices risk antimicrobial resistance evolution. Lancet Microbe 2021, 2, e135–e136. [Google Scholar] [CrossRef]
- Rodríguez-Baño, J.; Rossolini, G.M.; Schultsz, C.; Tacconelli, E.; Murthy, S.; Ohmagari, N.; Holmes, A.; Bachmann, T.; Goossens, H.; Canton, R.; et al. Key considerations on the potential impacts of the COVID-19 pandemic on antimicrobial resistance research and surveillance. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1122–1129. [Google Scholar] [CrossRef]
- Bloom, G.; Merrett, G.B.; Wilkinson, A.; Lin, V.; Paulin, S. Antimicrobial resistance and universal health coverage. BMJ Glob. Health 2017, 2, e000518. [Google Scholar] [CrossRef]
- Castro-Sánchez, E.; Moore, L.S.P.; Husson, F.; Holmes, A.H. What are the factors driving antimicrobial resistance? Perspectives from a public event in London, England. BMC Infect. Dis. 2016, 16, 465. [Google Scholar] [CrossRef] [Green Version]
- Vikesland, P.; Garner, E.; Gupta, S.; Kang, S.; Maile-Moskowitz, A.; Zhu, N. Differential Drivers of Antimicrobial Resistance across the World. Acc. Chem. Res. 2019, 52, 916–924. [Google Scholar] [CrossRef]
- Chatterjee, A.; Modarai, M.; Naylor, N.; Boyd, S.E.; Atun, R.; Barlow, J.; Holmes, A.H.; Johnson, A.; Robotham, J. Quantifying drivers of antibiotic resistance in humans: A systematic review. Lancet Infect. Dis. 2018, 18, e368–e378. [Google Scholar] [CrossRef] [Green Version]
- UNAS; CDDEP; GARP-Uganda; Mpairwe, Y.; Wamala, S. Antibiotic Resistance in Uganda: Situation Analysis and Recommendations; Uganda National Academy of Sciences: Kampala, Uganda; Center for Disease Dynamics, Economics & Policy: Washington, DC, USA, 2015; p. 107. [Google Scholar]
- Kajumbula, H.; Fujita, A.W.; Mbabazi, O.; Najjuka, C.; Izale, C.; Akampurira, A.; Aisu, S.; Lamorde, M.; Walwema, R.; Bahr, N.C.; et al. Antimicrobial Drug Resistance in Blood Culture Isolates at a Tertiary Hospital, Uganda. Emerg. Infect. Dis. 2018, 24, 174–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldin, O.P.; Mattison, D. Sex Differences in Pharmacokinetics and Pharmacodynamics. Clin. Pharmacokinet. 2009, 48, 143–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Action Plan on Antimicrobial Resistance; The World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Antimicrobial Resistance National Action Plan (2018–2023). The Republic of Uganda. 2018. Available online: https://www.heps.or.ug/index.php/publications/antimicrobial-resistance-national-action-plan-uganda-nap (accessed on 21 December 2021).
- WHO. World Health Organization Methodology for Point Prevalence Survey on Antibiotic Use in Hospitals; Version 1.1; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Ogunleye, O.O.; Oyawole, M.R.; Odunuga, P.T.; Kalejaye, F.; Yinka-Ogunleye, A.F.; Olalekan, A.; Ogundele, S.O.; Ebruke, B.E.; Richard, A.K.; Paramadhas, B.D.A.; et al. A multicentre point prevalence study of antibiotics utilization in hospitalised patients in an urban secondary and a tertiary healthcare facilities in Nigeria: Findings and implications. Expert Rev. Anti-Infect. Ther. 2022, 20, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, U. Antibiotic use among hospitalized patients in northern Nigeria: A multicenter point-prevalence survey. BMC Infect. Dis. 2020, 20, 86. [Google Scholar] [CrossRef] [Green Version]
- Bediako-Bowan, A.A.A.; Owusu, E.; Labi, A.-K.; Obeng-Nkrumah, N.; Sunkwa-Mills, G.; Bjerrum, S.; Opintan, J.A.; Bannerman, C.; Mølbak, K.; Kurtzhals, J.A.L.; et al. Antibiotic use in surgical units of selected hospitals in Ghana: A multi-center point prevalence survey. BMC Public Health 2019, 19, 797. [Google Scholar] [CrossRef]
- Godman, B.; Momanyi, L.; Opanga, S.; Nyamu, D.; Oluka, M.; Kurdi, A. Antibiotic prescribing patterns at a leading referral hospital in Kenya: A point prevalence survey. J. Res. Pharm. Pract. 2019, 8, 149–154. [Google Scholar] [CrossRef]
- Lanyero, H.; Ocan, M.; Obua, C.; Lundborg, C.S.; Nanzigu, S.; Katureebe, A.; Kalyango, J.N.; Eriksen, J. Antibiotic use among children under five years with diarrhea in rural communities of Gulu, northern Uganda: A cross-sectional study. BMC Public Health 2021, 21, 1254. [Google Scholar] [CrossRef]
- Sekikubo, M.; Hedman, K.; Mirembe, F.; Brauner, A. Antibiotic Overconsumption in Pregnant Women with Urinary Tract Symptoms in Uganda. Clin. Infect. Dis. 2017, 65, 544–550. [Google Scholar] [CrossRef] [Green Version]
- Saito, H.; Inoue, K.; Ditai, J.; Weeks, A.D. Pattern of Peri-Operative Antibiotic Use among Surgical Patients in a Regional Referral and Teaching Hospital in Uganda. Surg. Infect. 2020, 21, 540–546. [Google Scholar] [CrossRef] [Green Version]
- USAID Medicines, Technologies, and Pharmaceutical Services Program. MTaPS Support in Uganda. Available online: https://www.mtapsprogram.org/where-we-work/uganda/ (accessed on 21 December 2021).
- USAID MTaPS Program. A Technical Guide to Implementing Facility Level Antimicrobial Stewardship Programs in MTaPS Program Countries. Available online: https://www.mtapsprogram.org/wp-content/uploads/2021/03/USAID-MTaPS-Mini-guide-for-facility-AMS-program.pdf (accessed on 21 December 2021).
- Uganda Clinical Guidelines. National Guidelines for Management of Common Conditions; The Republic of Uganda, Ministry of Health: Kampala, Uganda, 2016.
- Okoth, C.; Opanga, S.; Okalebo, F.; Oluka, M.; Kurdi, A.; Godman, B. Point prevalence survey of antibiotic use and resistance at a referral hospital in Kenya: Findings and implications. Hosp. Pract. 2018, 46, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paramadhas, B.D.A.; Tiroyakgosi, C.; Mpinda-Joseph, P.; Morokotso, M.; Matome, M.; Sinkala, F.; Gaolebe, M.; Malone, B.; Molosiwa, E.; Shanmugam, M.G.; et al. Point prevalence study of antimicrobial use among hospitals across Botswana: Findings and implications. Expert Rev. Anti-Infect. Ther. 2019, 17, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Amponsah, O.K.O.; Buabeng, K.O.; Owusu-Ofori, A.; Ayisi-Boateng, N.K.; Hämeen-Anttila, K.; Enlund, H. Point prevalence survey of antibiotic consumption across three hospitals in Ghana. JAC-Antimicrob. Resist. 2021, 3, dlab008. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qader, D.H.; Ismael, N.S.; Albassam, A.; El-Shara’, A.; Aljamal, M.S.; Ismail, R.; Abdel-Qader, H.; Hamadi, S.; Al Mazrouei, N.; Ibrahim, O.M. Antibiotics use and appropriateness in two Jordanian children hospitals: A point prevalence study. J. Pharm. Health Serv. Res. 2021, 12, 166–172. [Google Scholar] [CrossRef]
- Pauwels, I.; Versporten, A.; Drapier, N.; Vlieghe, E.; Goossens, H.; Koraqi, A.; Hoxha, I.; Tafaj, S.; Cornistein, W.; Quiros, R.; et al. Hospital antibiotic prescribing patterns in adult patients according to the WHO Access, Watch and Reserve classification (AWaRe): Results from a worldwide point prevalence survey in 69 countries. J. Antimicrob. Chemother. 2021, 76, 1614–1624. [Google Scholar] [CrossRef] [PubMed]
- Maina, M.; Mwaniki, P.; Odira, E.; Kiko, N.; McKnight, J.; Schultsz, C.; English, M.; Tosas-Auguet, O. Antibiotic use in Kenyan public hospitals: Prevalence, appropriateness and link to guideline availability. Int. J. Infect. Dis. 2020, 99, 10–18. [Google Scholar] [CrossRef]
- Horumpende, P.G.; Mshana, S.E.; Mouw, E.F.; Mmbaga, B.T.; Chilongola, J.O.; De Mast, Q. Point prevalence survey of antimicrobial use in three hospitals in North-Eastern Tanzania. Antimicrob. Resist. Infect. Control 2020, 9, 149. [Google Scholar] [CrossRef]
- D’Arcy, N.; Ashiru-Oredope, D.; Olaoye, O.; Afriyie, D.; Akello, Z.; Ankrah, D.; Asima, D.M.; Banda, D.C.; Barrett, S.; Brandish, C.; et al. Antibiotic Prescribing Patterns in Ghana, Uganda, Zambia and Tanzania Hospitals: Results from the Global Point Prevalence Survey (G-PPS) on Antimicrobial Use and Stewardship Interventions Implemented. Antibiotics 2021, 10, 1122. [Google Scholar] [CrossRef]
- Porto, A.; Goossens, H.; Versporten, A.; Costa, S.; Brazilian Global-PPS Working Group. Global point prevalence survey of antimicrobial consumption in Brazilian hospitals. J. Hosp. Infect. 2020, 104, 165–171. [Google Scholar] [CrossRef]
- Elhajji, F.D.; Al-Taani, G.M.; Anani, L.; Al-Masri, S.; Abdalaziz, H.; Qabba’H, S.H.; Al Bawab, A.Q.; Scott, M.; Farren, D.; Gilmore, F.; et al. Comparative point prevalence survey of antimicrobial consumption between a hospital in Northern Ireland and a hospital in Jordan. BMC Health Serv. Res. 2018, 18, 849. [Google Scholar] [CrossRef] [Green Version]
- Vandael, E.; Latour, K.; Goossens, H.; Magerman, K.; Drapier, N.; Catry, B.; Versporten, A.; Belgian Point Prevalence Survey Study Group. Point prevalence survey of antimicrobial use and healthcare-associated infections in Belgian acute care hospitals: Results of the Global-PPS and ECDC-PPS 2017. Antimicrob. Resist. Infect. Control 2020, 9, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Taking Sex and Gender into Account in Emerging Infectious Disease Programmes. An Analytical Framework; World Health Organization Western Pacific Region: Manilla, Philippines, 2011; ISBN 978 92 9061 532 3. [Google Scholar]
- Mauvais-Jarvis, F.; Merz, N.B.; Barnes, P.J.; Brinton, R.D.; Carrero, J.-J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Accorsi, S.; Fabiani, M.; Nattabi, B.; Ferrarese, N.; Corrado, B.; Iriso, R.; Ayella, E.O.; Pido, B.; Yoti, Z.; Corti, D.; et al. Differences in hospital admissions for males and females in northern Uganda in the period 1992–2004: A consideration of gender and sex differences in health care use. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 929–938. [Google Scholar] [CrossRef] [PubMed]
- WHO. Tackling Antimicrobial Resistance (AMR) Together: Working Paper 5.0: Enhancing the Focus on Gender and Equity; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- WHO. Global Guidelines for the Prevention of Surgical Site Infection, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Cooper, L.; Sneddon, J.; Afriyie, D.K.; Sefah, I.A.; Kurdi, A.; Godman, B.; Seaton, R.A. Supporting global antimicrobial stewardship: Antibiotic prophylaxis for the prevention of surgical site infection in low- and middle-income countries (LMICs): A scoping review and meta-analysis. JAC-Antimicrob. Resist. 2020, 2, dlaa070. [Google Scholar] [CrossRef] [PubMed]
- Limato, R.; Nelwan, E.J.; Mudia, M.; de Brabander, J.; Guterres, H.; Enty, E.; Mauleti, I.Y.; Mayasari, M.; Firmansyah, I.; Hizrani, M.; et al. A multicentre point prevalence survey of patterns and quality of antibiotic prescribing in Indonesian hospitals. JAC-Antimicrob. Resist. 2021, 3, dlab047. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A.; Versporten, A.; Godman, B.; Hashmi, F.K.; Goossens, H.; Saleem, F. A multicenter point prevalence survey of antibiotic use in Punjab, Pakistan: Findings and implications. Expert Rev. Anti-Infect. Ther. 2019, 17, 285–293. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Releases the 2019 AWaRe Classification Antibiotics. 2019. Available online: https://www.who.int/news/item/01-10-2019-who-releases-the-2019-aware-classification-antibiotics (accessed on 21 December 2021).
- Nambasa, V.; Ndagije, H.; Serwanga, A.; Manirakiza, L.; Atuhaire, J.; Nakitto, D.; Kiguba, R.; Figueras, A. Prescription of Levofloxacin and Moxifloxacin in Select Hospitals in Uganda: A Pilot Study to Assess Guideline Concordance. Antibiotics 2020, 9, 439. [Google Scholar] [CrossRef]
- Maina, M.; McKnight, J.; Tosas-Auguet, O.; Schultsz, C.; English, M. Using treatment guidelines to improve antibiotic use: Insights from an antibiotic point prevalence survey in Kenya. BMJ Glob. Health 2021, 6, e003836. [Google Scholar] [CrossRef]
- Almazrou, S.; Alfaifi, S.; Alfaifi, S.; Hakami, L.; Al-Aqeel, S. Barriers to and Facilitators of Adherence to Clinical Practice Guidelines in the Middle East and North Africa Region: A Systematic Review. Healthcare 2020, 8, 564. [Google Scholar] [CrossRef]
- Seni, J.; Mapunjo, S.G.; Wittenauer, R.; Valimba, R.; Stergachis, A.; Werth, B.J.; Saitoti, S.; Mhadu, N.H.; Lusaya, E.; Konduri, N. Antimicrobial use across six referral hospitals in Tanzania: A point prevalence survey. BMJ Open 2020, 10, e042819. [Google Scholar] [CrossRef]
- Skosana, P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J. A point prevalence survey of antimicrobial utilisation patterns and quality indices amongst hospitals in South Africa; findings and implications. Expert Rev. Anti-Infect. Ther. 2021, 19, 1353–1366. [Google Scholar] [CrossRef] [PubMed]
- Policy Guidelines for Implementing Antimicrobial Stewardship; The United Republic of Tanzania, Ministry of Health, Community Development, Gender, Elderly and Children: Dodoma, Tanzania, 2020.
- Chetty, S.; Reddy, M.; Ramsamy, Y.; Naidoo, A.; Essack, S. Antimicrobial stewardship in South Africa: A scoping review of the published literature. JAC-Antimicrob. Resist. 2019, 1, dlz060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kagoya, E.K.; Van Royen, K.; Waako, P.; Van Royen, P.; Iramiot, J.S.; Obakiro, S.B.; Kostyanev, T.; Anthierens, S. Experiences and views of healthcare professionals on the prescription of antibiotics in Eastern Uganda: A qualitative study. J. Glob. Antimicrob. Resist. 2021, 25, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Knowledge Management Portal. Periodic Stock Status Report. Example of One Report Dated 29 April 2021. Available online: http://library.health.go.ug/publications/medicines/ministry-health-stock-status-report-1st-april-2021 (accessed on 21 December 2021).
- Muyinda, H.; Mugisha, J. Stock-outs, uncertainty and improvisation in access to healthcare in war-torn Northern Uganda. Soc. Sci. Med. 2015, 146, 316–323. [Google Scholar] [CrossRef] [PubMed]
- ReAct Group. Shortages and AMR—Why Should We Care? 4 Consequences of Antibiotic Shortages. 2020. Available online: https://www.reactgroup.org/news-and-views/news-and-opinions/year-2020/shortages-and-amr-why-should-we-care-4-consequences-of-antibiotic-shortages/ (accessed on 21 December 2021).
- Hwang, B.; Shroufi, A.; Gils, T.; Steele, S.J.; Grimsrud, A.; Boulle, A.; Yawa, A.; Stevenson, S.; Jankelowitz, L.; Versteeg-Mojanaga, M.; et al. Stock-outs of antiretroviral and tuberculosis medicines in South Africa: A national cross-sectional survey. PLoS ONE 2019, 14, e0212405. [Google Scholar] [CrossRef] [Green Version]
- Coleman, J.J.; Hodson, J.; Brooks, H.L.; Rosser, D. Missed medication doses in hospitalised patients: A descriptive account of quality improvement measures and time series analysis. Int. J. Qual. Health Care 2013, 25, 564–572. [Google Scholar] [CrossRef] [Green Version]
- Bonniface, M.; Nambatya, W.; Rajab, K. An Evaluation of Antibiotic Prescribing Practices in a Rural Refugee Settlement District in Uganda. Antibiotics 2021, 10, 172. [Google Scholar] [CrossRef]
- Engel, M.F.; Postma, D.F.; Hulscher, M.E.; van Berkhout, F.T.; Emmelot-Vonk, M.H.; Sankatsing, S.; Gaillard, C.A.; Bruns, A.H.; Hoepelman, A.I.; Oosterheert, J.J. Barriers to an early switch from intravenous to oral antibiotic therapy in hospitalised patients with CAP. Eur. Respir. J. 2013, 41, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Sayer, B.; Bortone, B.; Sharland, M.; Hsia, Y. Fixed-dose combination antibiotics: The search for evidence using the example of ampicillin–cloxacillin. Br. J. Clin. Pharmacol. 2021, 87, 2996–2999. [Google Scholar] [CrossRef]
- Bortone, B.; Jackson, C.; Hsia, Y.; Bielicki, J.; Magrini, N.; Sharland, M. High global consumption of potentially inappropriate fixed dose combination antibiotics: Analysis of data from 75 countries. PLoS ONE 2021, 16, e0241899. [Google Scholar] [CrossRef]
- Namugambe, J.; Delamou, A.; Moses, F.; Ali, E.; Hermans, V.; Takarinda, K.; Thekkur, P.; Nanyonga, S.; Koroma, Z.; Mwoga, J.; et al. National Antimicrobial Consumption: Analysis of Central Warehouses Supplies to in-Patient Care Health Facilities from 2017 to 2019 in Uganda. Trop. Med. Infect. Dis. 2021, 6, 83. [Google Scholar] [CrossRef] [PubMed]
- Kizito, M.; Lalitha, R.; Kajumbula, H.; Ssenyonga, R.; Muyanja, D.; Byakika-Kibwika, P. Antibiotic Prevalence Study and Factors Influencing Prescription of WHO Watch Category Antibiotic Ceftriaxone in a Tertiary Care Private Not for Profit Hospital in Uganda. Antibiotics 2021, 10, 1167. [Google Scholar] [CrossRef] [PubMed]
- Kutyabami, P.; Munanura, E.I.; Kalidi, R.; Balikuna, S.; Ndagire, M.; Kaggwa, B.; Nambatya, W.; Kamba, P.F.; Musiimenta, A.; Kesi, D.N.; et al. Evaluation of the Clinical Use of Ceftriaxone among in-Patients in Selected Health Facilities in Uganda. Antibiotics 2021, 10, 779. [Google Scholar] [CrossRef]
- Barbé, B.; Yansouni, C.; Affolabi, D.; Jacobs, J. Implementation of quality management for clinical bacteriology in low-resource settings. Clin. Microbiol. Infect. 2017, 23, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.; Hardy, L.; Semret, M.; Lunguya, O.; Phe, T.; Affolabi, D.; Yansouni, C.; Vandenberg, O. Diagnostic Bacteriology in District Hospitals in Sub-Saharan Africa: At the Forefront of the Containment of Antimicrobial Resistance. Front. Med. 2019, 6, 205. [Google Scholar] [CrossRef] [Green Version]
- Lamorde, M.; Mpimbaza, A.; Walwema, R.; Kamya, M.; Kapisi, J.; Kajumbula, H.; Sserwanga, A.; Namuganga, J.F.; Kusemererwa, A.; Tasimwa, H.; et al. A Cross-Cutting Approach to Surveillance and Laboratory Capacity as a Platform to Improve Health Security in Uganda. Health Secur. 2018, 16, S-76–S-86. [Google Scholar] [CrossRef] [Green Version]
- WHO. The 2019 WHO Aware Classification of Antibiotics for Evaluation and Monitoring of Use. 2019. Available online: https://aware.essentialmeds.org/groups (accessed on 21 December 2021).
- RStudio Team. RStudio: Integrated Development for R; RStudio Inc.: Boston, MA, USA, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Number (Proportion) (n = 1077) |
|---|---|
| Demographics | |
| Female | 609 (56.5%) |
| Male | 468 (43.5%) |
| Age a | 27 (10–38) |
| Hospital ownership | |
| Public | 706 (65.5%) |
| Private not-for-profit | 371 (34.4%) |
| Hospital | |
| Gulu RRH | 133 (12.3%) |
| Hoima RRH | 103 (9.6%) |
| Kagando | 61 (5.7%) |
| Kiwoko | 43 (4%) |
| Kumi | 47 (4.4%) |
| Lacor | 168 (15.6%) |
| Lira RRH | 119 (11%) |
| Masaka RRH | 127 (11.8%) |
| Moroto RRH | 99 (9.2%) |
| Ruharo Mission | 6 (0.6%) |
| Soroti RRH | 125 (11.6%) |
| St. Anthony | 12 (1.1%) |
| St. Francis Naggalama | 34 (3.2%) |
| Ward | |
| Maternal | 311 (28.8%) |
| Medical | 239 (22.2%) |
| Pediatric | 243 (22.5%) |
| Surgical | 284 (26.3%) |
| Underlying patient condition | |
| Central catheter | 3 (0.3%) |
| Peripheral catheter | 1049 (97.3%) |
| Urinary catheter | 60 (5.6%) |
| Intubation | 5 (0.5%) |
| Malaria | 118 (10.9%) |
| Tuberculosis | 20 (1.9%) |
| HIV | 46 (4.3%) |
| COPD | 12 (1.1%) |
| Malnutrition | 52 (4.8%) |
| Antibiotic | All Prescriptions (n = 1387) | Community Acquired Infection (n = 577) | Hospital Associated Infection (n = 87) | Medical Prophylaxis (n = 404) | Surgical Prophylaxis (n = 319) |
|---|---|---|---|---|---|
| Ceftriaxone | 513 | 183 (35.7%) | 21 (4.1%) | 177 (34.5%) | 132 (25.7%) |
| Metronidazole | 380 | 121 (31.8%) | 26 (6.8%) | 98 (25.8%) | 135 (35.5%) |
| Gentamicin | 119 | 70 (58.8%) | 12 (10.1%) | 22 (18.5%) | 15 (12.6%) |
| Ampicillin | 89 | 55 (61.8%) | 5 (5.6%) | 27 (30.3%) | 2 (2.2%) |
| Ampicillin-cloxacillin | 79 | 31 (39.2%) | 4 (5.1%) | 31 (39.2%) | 13 (16.5%) |
| Ciprofloxacin | 45 | 25 (55.6%) | 2 (4.4%) | 15 (33.3%) | 3 (6.7%) |
| Cloxacillin | 27 | 17 (63%) | 1 (3.7%) | 5 (18.5%) | 4 (14.8%) |
| Amoxicillin | 26 | 12 (46.2%) | 0 (0%) | 10 (38.5%) | 4 (15.4%) |
| Azithromycin | 19 | 15 (78.9%) | 0 (0%) | 3 (15.8%) | 1 (5.3%) |
| Penicillin | 16 | 10 (62.5%) | T0 (0%) | 5 (31.3%) | 1 (6.3%) |
| Levofloxacin | 15 | 10 (66.7%) | 4 (26.7%) | 1 (6.7%) | 0 (0%) |
| Other a | 59 | 28 (47.5%) | 12 (20.3%) | 10 (16.9%) | 9 (15.3%) |
| Antibiotic a | Total (n = 1387) | Public Hospitals (All Regional Referral Hospitals) | Private Not-for-Profit Hospitals | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gulu (n = 144) | Hoima (n = 151) | Lira (n = 170) | Masaka (n = 203) | Moroto (n = 111) | Soroti (n = 157) | Kagando (n = 90) | Kiwoko (n = 44) | Kumi (n = 77) | Lacor (n = 150) | Ruharo Mission (n = 10) | St. Anthony (n = 19) | St. Francis Naggalama (n = 61) | ||
| Ceftriaxone | 513 | 61 | 66 | 39 | 85 | 62 | 74 | 38 | 12 | 22 | 16 | 4 | 9 | 25 |
| Metronidazole | 380 | 43 | 53 | 52 | 62 | 14 | 47 | 28 | 10 | 16 | 33 | 3 | 6 | 13 |
| Gentamicin | 119 | 13 | 5 | 22 | 14 | 9 | 2 | 6 | 6 | 8 | 27 | 1 | 2 | 4 |
| Ampicillin | 89 | 5 | 2 | 11 | 14 | 6 | 5 | 5 | 5 | 6 | 28 | 0 | 0 | 2 |
| Ampicillin-cloxacillin | 79 | 8 | 7 | 19 | 9 | 11 | 8 | 6 | 0 | 3 | 1 | 0 | 1 | 6 |
| Ciprofloxacin | 45 | 6 | 5 | 8 | 4 | 3 | 4 | 1 | 0 | 2 | 11 | 0 | 0 | 1 |
| Cloxacillin | 27 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 20 | 0 | 0 | 1 |
| Amoxicillin | 26 | 6 | 4 | 4 | 1 | 0 | 0 | 4 | 6 | 0 | 1 | 0 | 0 | 0 |
| Azithromycin | 19 | 0 | 2 | 3 | 4 | 0 | 1 | 0 | 1 | 1 | 2 | 0 | 0 | 4 |
| Penicillin | 16 | 0 | 1 | 1 | 0 | 5 | 0 | 0 | 0 | 2 | 7 | 0 | 0 | 0 |
| Levofloxacin | 15 | 0 | 0 | 0 | 2 | 0 | 1 | 1 | 0 | 7 | 1 | 0 | 1 | 2 |
| Other b | 59 | 2 | 4 | 11 | 8 | 1 | 14 | 1 | 0 | 10 | 3 | 2 | 0 | 3 |
| Care Setting | Mean Antibiotics per Patient (Range) |
|---|---|
| Hospital ownership | |
| Public | 1.66 (1–4) |
| Private not-for-profit | 1.70 (1–4) |
| Hospital | |
| Gulu RRH | 1.631 (1–3) |
| Hoima RRH | 1.727 (1–3) |
| Kagando | 1.776 (1–3) |
| Kiwoko | 1.792 (1–4) |
| Kumi | 1.658 (1–3) |
| Lacor | 1.667 (1–3) |
| Lira RRH | 1.953 (1–3) |
| Masaka RRH | 1.685 (1–3) |
| Moroto RRH | 1.325 (1–4) |
| Ruharo Mission | 2.000 (1–3) |
| Soroti RRH | 1.646 (1–3) |
| St. Anthony | 1.727 (1–3) |
| St. Francis Naggalama | 1.625 (1–3) |
| Variable | Antibiotic Use (n [%]) | Univariate Model | Multivariate Model 2 | ||
|---|---|---|---|---|---|
| Odds Ratio | p-Value 1 | Odds Ratio | p-Value 1 | ||
| Age category | |||||
| <2 years | 102 (82.9%) | 1 (reference) | |||
| 2–50 years | 569 (71.7%) | 0.65 | 0.01 * | 0.63 | 0.08 |
| >50 years | 117 (75.8%) | 0.52 | 0.16 | 0.70 | 0.28 |
| Sex | |||||
| Female | 425 (69.8%) | 1 (reference) | |||
| Male | 369 (78.8%) | 1.15 | <0.001 * | 1.57 | 0.003 * |
| Hospital ownership | |||||
| Private not-for-profit | 245 (66.0%) | 1 (reference) | |||
| Public | 549 (77.8%) | 1.80 | <0.001 * | ||
| Hospital | |||||
| Gulu RRH | 84 (63.2%) | 1 (reference) | |||
| Hoima RRH | 88 (85.4%) | 3.42 | <0.001 * | ||
| Kagando | 49 (80.3%) | 2.38 | 0.02 * | ||
| Kiwoko | 24 (55.8%) | 0.74 | 0.39 | ||
| Kumi | 38 (80.9%) | 2.46 | 0.03 * | ||
| Lacor | 86 (51.2%) | 0.61 | 0.04 * | ||
| Lira RRH | 86 (70.3%) | 1.52 | 0.12 | ||
| Masaka RRH | 114 (89.8%) | 5.11 | <0.001 * | ||
| Moroto RRH | 81 (81.8%) | 2.62 | 0.002 * | ||
| Ruharo Mission | 5 (83.3%) | 2.92 | 0.33 | ||
| Soroti RRH | 96 (76.8%) | 1.93 | 0.02 * | ||
| St. Anthony | 11 (91.7%) | 6.41 | 0.08 | ||
| St. Francis Naggalama | 32 (94.1%) | 9.33 | 0.003 * | ||
| Ward | |||||
| Maternal | 219 (70.4%) | 1 (reference) | |||
| Medical | 170 (71.1%) | 1.04 | 0.86 | ||
| Pediatric | 188 (77.4%) | 1.44 | 0.06 | ||
| Surgical | 217 (76.4%) | 1.36 | 0.10 | ||
| Underlying conditions | |||||
| HIV (no) | 689 (71.7%) | 1 (reference) | |||
| HIV (yes) | 43 (93.5%) | 5.65 | 0.004 * | 5.90 | 0.003 * |
| TB (no) | 705 (71.9%) | 1 (reference) | |||
| TB (yes) | 18 (90%) | 3.51 | 0.09 | ||
| Malaria (no) | 667 (73.2%) | 1 (reference) | |||
| Malaria (yes) | 85 (72%) | 0.94 | 0.78 | 0.79 | 0.31 |
| COPD (no) | 752 (73.9%) | 1 (reference) | |||
| COPD (yes) | 9 (75.0%) | 1.06 | 0.93 | ||
| Malnutrition (no) | 738 (72.9%) | 1 (reference) | |||
| Malnutrition (yes) | 49 (94.2%) | 6.06 | 0.002 * | 5.78 | 0.004 * |
| Hosp in past 90 days (no) | 696 (72.8%) | 1 (reference) | |||
| Hosp in past 90 days (yes) | 65 (80.2%) | 1.51 | 0.15 | ||
| Setting | Guideline Compliance (n, %) |
|---|---|
| Hospital ownership | |
| Public | 289 (30.9%) |
| Private not-for-profit | 134 (29.7%) |
| Hospital | |
| Gulu RRH | 41 (28.5%) |
| Hoima RRH | 61 (40.4%) |
| Kagando | 17 (18.9%) |
| Kiwoko | 24 (54.5%) |
| Kumi | 12 (15.6%) |
| Lacor | 58 (38.7%) |
| Lira RRH | 61 (35.9%) |
| Masaka RRH | 67 (33%) |
| Moroto RRH | 34 (30.6%) |
| Ruharo Mission | 0 (0%) |
| Soroti RRH | 25 (15.9%) |
| St. Anthnoy | 5 (26.3%) |
| St. Francis Naggalama | 18 (29.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiggundu, R.; Wittenauer, R.; Waswa, J.; Nakambale, H.N.; Kitutu, F.E.; Murungi, M.; Okuna, N.; Morries, S.; Lawry, L.L.; Joshi, M.P.; et al. Point Prevalence Survey of Antibiotic Use across 13 Hospitals in Uganda. Antibiotics 2022, 11, 199. https://doi.org/10.3390/antibiotics11020199
Kiggundu R, Wittenauer R, Waswa J, Nakambale HN, Kitutu FE, Murungi M, Okuna N, Morries S, Lawry LL, Joshi MP, et al. Point Prevalence Survey of Antibiotic Use across 13 Hospitals in Uganda. Antibiotics. 2022; 11(2):199. https://doi.org/10.3390/antibiotics11020199
Chicago/Turabian StyleKiggundu, Reuben, Rachel Wittenauer, JP Waswa, Hilma N. Nakambale, Freddy Eric Kitutu, Marion Murungi, Neville Okuna, Seru Morries, Lynn Lieberman Lawry, Mohan P. Joshi, and et al. 2022. "Point Prevalence Survey of Antibiotic Use across 13 Hospitals in Uganda" Antibiotics 11, no. 2: 199. https://doi.org/10.3390/antibiotics11020199