1. Introduction
Antimicrobial resistance (AMR), particularly antibiotic resistance, is one of the most challenging global health threats of our time [
1]. Even under the shadow of COVID-19, AMR posed a substantial threat to patients who developed secondary bacterial infections [
2]. AMR causes challenges to the treatment of infections and infectious diseases, including HIV/AIDS, typhoid, cholera, tuberculosis, gonorrhoea, hospital-associated infections, and malaria, which disproportionately affect low- and middle-income countries (LMICs) [
1]. AMR is also particularly prevalent and problematic in LMICs where health systems and medical resources, including access to water, sanitation, and hygiene (WASH), are limited, as well as where socioeconomic drivers, such as extreme poverty, increase the risk of communicable diseases exponentially [
3]. The Fleming Fund was created in response to this need, and has funded many programmes of work, including the Commonwealth Partnerships for Antimicrobial Stewardship Programme (CwPAMS). CwPAMS addresses AMR through antimicrobial stewardship interventions in eight African Fleming Fund priority countries, using a health partnership approach.
Tackling AMR requires a multidisciplinary approach. Whether a clinical or healthcare team member is a nurse, doctor, pharmacist, cleaner, or other type of health worker, their contribution towards keeping patients safe from infection and the spread of resistant organisms is crucial to saving lives.
Existing literature portrays that games can be a good way to engage communities in joint learning [
4,
5]. Evidence shows that games have been used to promote health and wellbeing in regard to both infectious and non-infectious diseases [
6]. As a health education tool, games have proven to be an enjoyable method that enhances learning through stimulating players’ interests and motivation [
6,
7]. While existing studies largely point to games as an impactful educational tool for children and students, some studies have demonstrated that games can be used as a capacity-building intervention for health professionals [
8]. Games can be used for improving health professionals’ knowledge and skills, changing their attitudes and performance, and improving how they care for their patients [
8]. Despite the strong indication that games can improve knowledge, several studies including those conducted among health professionals do not show sufficient evidence that games can improve performance or change behaviour [
7,
9,
10,
11]. To this end, there is a need for more research with a focus on outcomes that go beyond knowledge assessment, to include outcomes such as skills, behaviour, and patient outcomes [
10].
Few existing studies highlight that AMS games can be an innovative way of spreading awareness on AMR. A study conducted in Saudi Arabia among students concluded that gamification using an AMS board game can significantly improve AMR knowledge, with better retention than a conventional lecture [
12]. In another study conducted in the UK among children aged 7–15 years, it was reported that antibiotic games improved knowledge on the use of antibiotics for bacterial versus viral infections and ensured that the course of antibiotics was completed [
13]. The antimicrobial stewardship (AMS) game described in this manuscript was developed to encourage players (healthcare teams including students, doctors, laboratory staff, pharmacists, and nurses) to discuss AMS and learn what they can do personally, and collectively, to improve stewardship in their organisation and their community. The intention was to create a game for groups to play, and in order to make the game more widely accessible, a physical printed tabletop board game was developed with an online version for groups working remotely. Further, it is intended that the game would encourage the player to understand the scale of the AMR problem and that everyone who uses, dispenses or prescribes antimicrobials is part of the solution to reduce the impact of AMR. Effective training and capacity building are vital to the success of stewardship programmes, particularly when staff are new to the concept. The AMS game is intended to make stewardship training engaging and inclusive, generating fun and enthusiasm with a serious purpose and clear outcomes.
Focus Games Ltd. was the game development partner for this project. Focus Games Ltd. has been a leading developer of ‘serious’ educational games/game-based learning and simulations since 2004. They have developed over 100 different games for staff, patients, and the public that address a wide range of clinical, health, and wellbeing issues.
Independent evaluations of these games demonstrate that they can improve knowledge and encourage beneficial changes in thinking and behaviour [
14].
Subject matter expertise, technical competency, and decision-making are diluted when individuals cannot communicate effectively with the people around them. These interpersonal skills can be learned and developed in the same way that subject matter expertise is developed. However, because these interpersonal ‘soft’ skills are largely intangible, we need to find appropriate ways of teaching.
Although there is not a definitive theoretical framework for the development of serious games, key elements of good practice have previously been summarised [
15]. In development of the AMS game several elements of published good practice [
15], were considered for incorporation:
Competition and goals, with players competing against other players both for the physical and online games.
Clear rules that define how the game is played.
Choice through the use of multiple-choice questions.
Challenges—players are provided with problems to solve in this game. We use the case studies as a way to provide additional challenges.
Coaching, debriefing, and feedback: to reinforce learning.
Performance assessment, so players know how they did.
Mechanics: the elements of the game that control gameplay.
The development of the AMS game involved a wide range of stakeholders from across the globe, who represented the target audience for which the game was being developed. To test the usability of the developed AMS game, we used online platforms to invite interested individuals including healthcare teams to play the AMS game and asked them to share their experiences through an online feedback survey form.
2. Materials and Methods
The game was developed by the Commonwealth Partnerships for Antimicrobial Stewardship Programme (CwPAMS), led by the Commonwealth Pharmacists Association (CPA) and Tropical Health and Education Trust (THET) in partnership with Focus Games Ltd. The CPA was the overall technical lead for developing the antimicrobial stewardship concepts (questions and answers) used in the game. Focus Games Ltd. was responsible for programming the AMS concepts into a playable game. THET’s coordination expertise was leveraged in bringing together relevant partners to support the development of the game.
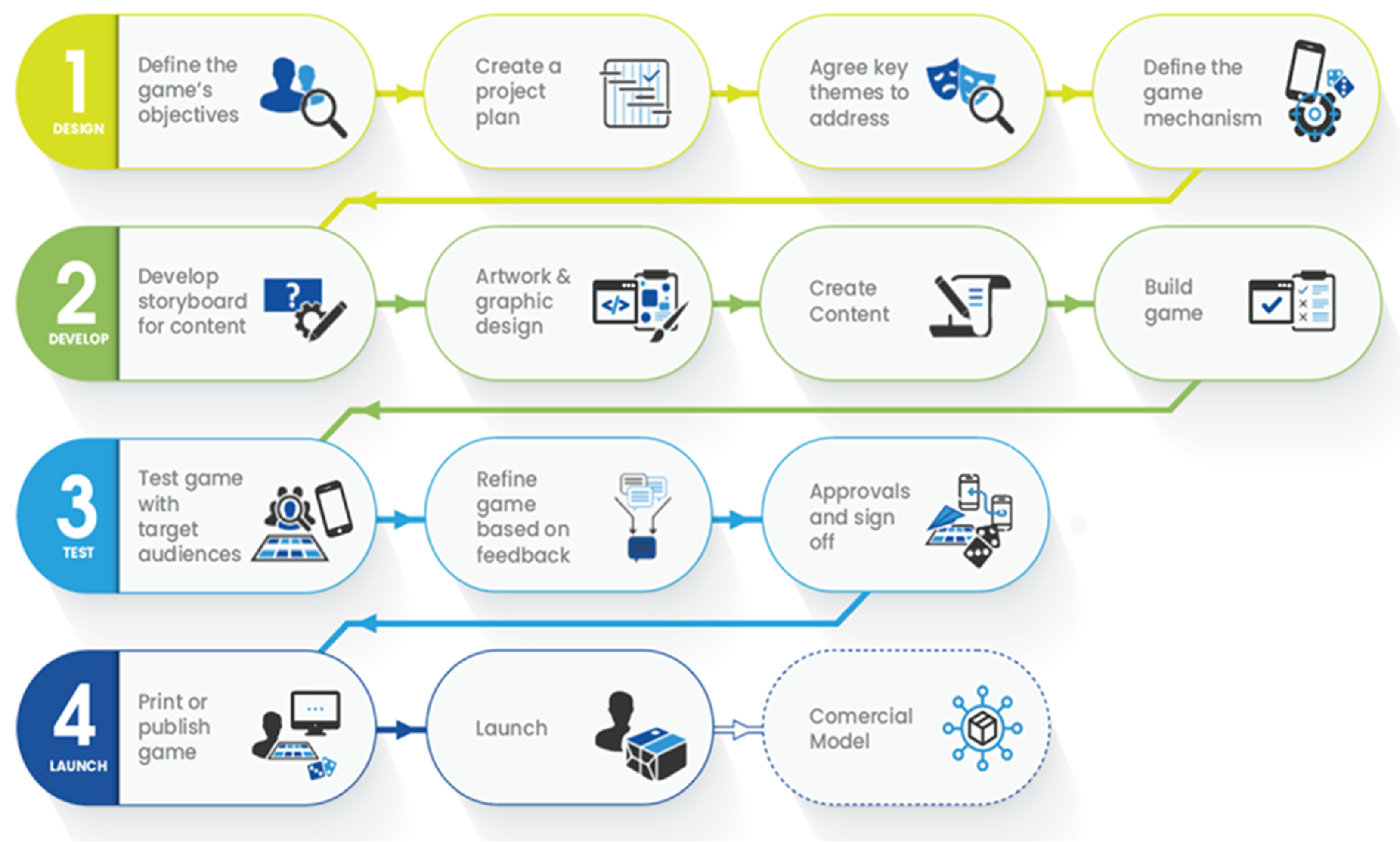
2.1. AMS Game Development
The AMS game used the Focus Games Ltd. development process/pathway (
Figure 1).
In order to optimise relationships and collaboration between stakeholders and programme team, Focus Games Ltd. used a range of project management tools to ensure that resources and priorities were managed efficiently and that they were overseen by a programme manager.
At the beginning of the project, a project plan and milestones were agreed upon as well as a specification document which included deliverables pertinent to the project. These deliverables formed the sign-off and approval for the completion of the project.
Focus Games used agile project management processes and tools (Jira). All code development was managed in Bitbucket (GIT repository), ensuring a strong development, test, and live approach. All staff are suitably qualified in their respective disciplines.
The development process for the AMS game included four key phases previously developed by Focus Games Ltd. (
Figure 1).
Phase 1—Define Objectives: Requirements for the game outcomes were derived from interviews with and feedback from individual stakeholders, ranging from national to frontline health professionals including pharmacists, doctors, and nurses from eight African countries and the UK. They acted as subject matter experts as well as representatives for the target audience of the game through the development and user testing phases, which included syntax and grammar that was considered acceptable across multiple countries. This identified the learning objectives for the narrative structure of the factual content and how the game design and mechanism will facilitate engagement and learning.
Phase 2—Develop Storyboards: Specific learning objectives and game dynamics were identified based on best practice derived from experience of previous games developed by Focus Games Ltd. This involved the creation of graphic design mock-ups of the game and a written storyboard outline of the factual content. These were discussed and agreed upon by the project team, which included subject matter experts as well as stakeholders across nine countries (Ghana, Kenya, Malawi, Nigeria, Sierra Leone, Tanzania, Uganda, United Kingdom, and Zambia) that were all part of the countries of focus for the CwPAMS programme.
Phase 3—Prototype and Testing: A rapid prototyping approach was used, incorporating data from the pilot scenario and interviews with subject matter experts (SMEs). The game mechanism and design were finalised. The written content was drafted and loaded into the game mechanism. The game was subsequently tested in workshops with SMEs whose feedback informed design iterations.
Phase 4—Refine, Rework, and Launch: production of the final design and implementation of the distribution and commercialisation strategy.
The model and process used are based on practical experience of developing 100 educational games that are being actively used by healthcare professionals around the world. Focus Games have previously evaluated third-party frameworks and models and have found many of them impractical for the purpose of developing game-based learning for the healthcare setting.
2.2. Target Audience for the AMS Game
The AMS game is intended to support education on antimicrobial stewardship among current and future healthcare team members, including doctors, nurses, pharmacy teams, laboratory staff, and students.
2.3. Stakeholder Engagement
The game was co-created between partners in the UK and eight African countries that were part of the CwPAMS programme to ensure that the game is relevant, effective, and was designed to be used in either a high-income or low- to middle-income setting. The four broad areas addressed in the game are introduction to antimicrobial resistance and stewardship, appropriate use of antimicrobial agents, infection prevention and control, and stewardship and surveillance.
Partners and their network of health professionals were asked to share insights on the game. Twenty-seven stakeholders ranging from national to frontline health professionals, including pharmacists, doctors, and nurses across nine countries (Ghana, Kenya, Malawi, Nigeria, Sierra Leone, Tanzania, Uganda, United Kingdom, and Zambia), were consulted on the type of the game—snakes and ladders, the question cards for the AMS game, and case studies to include in the AMS game. Stakeholders were asked to share broad comments about content and accuracy of the answers to the questions in the game within their context and also asked to suggest any additional questions. To guide the feedback process, a structured feedback form (available as
Supplementary File S1) was developed in Microsoft Word and shared with the stakeholders via email. The feedback form covered the following sections: demographics of the respondent (name, title, country, profession, job title, and email address), relevancy of the questions to the country, responsiveness of the questions to the key aspects of AMS, and also provided space for them to suggest other potential topics for inclusion in the game.
A guide was developed for the facilitators to provide direction on how to host the game (available in
Supplementary File S2). Sample questions and answers are available in
Supplementary File S3. A prize was planned for the participants of the game. The participants who completed the evaluation form of the game were entered into a draw to win access to the online AMS game for a period of one year
2.4. Recruitment of Participants and Playing the Game
The AMS game was first launched and played in August 2021, and then played again during the World Antimicrobial Awareness Week in November 2021 as part of a global tournament (
Supplementary File S4). On both occasions, the game was promoted globally through online channels including email, websites, and social media to encourage people across the globe to register as players or facilitators. The facilitators had a technical background in antimicrobial resistance and stewardship and the project team provided a short briefing session on how to steer the session between the playing teams.
The game was hosted on Zoom, where participants received a Zoom link upon registration and used it to join the game session. Players were allocated to different breakout rooms with facilitators. In each breakout room, players were divided into two teams. Teams took turns to answer and discuss a series of questions and case studies about AMR and AMS that were being shown after the facilitators rolled the dice. The game lasted for 45 min. The facilitators were responsible for organizing players into teams, and moderating the game by displaying questions, encouraging players to discuss the questions and agree on the response, and displaying the correct answer after the players’ responses. The facilitator guide is available as
Supplementary File S2.
2.5. Feedback from Players of the Game
We collected feedback from individuals who played the AMS game on 24 November 2021. The feedback was collected using an online questionnaire with quantitative and open/free response text-based options hosted on Survey Monkey. This was a short questionnaire with 13 questions that: collected the players’ demographic information, examined their experience in antimicrobial stewardship, assessed their knowledge gain and confidence in antimicrobial stewardship after playing the game, and assessed their perceptions on the game in terms of enjoyment and whether they would share lessons from the game and also recommend it to others.
2.6. Data Management
Data were collected anonymously, although survey respondents could voluntarily provide their name and email address should they wish to be contacted afterwards, e.g., for information about game prize winners and future relevant AMR events. All data were anonymised prior to data analysis. The data were held securely by the project team and in line with the General Data Protection Regulation 2016/679 [
18].
2.7. Data Analysis
Descriptive statistics on the frequency distributions and percentages were used to analyse the responses. Data were analysed using Stata 14.


 ,
, 


{kind=link}
{kind=link}