
The Implementation of National Action Plan (NAP) on Antimicrobial Resistance (AMR) in Bangladesh: Challenges and Lessons Learned from a Cross-Sectional Qualitative Study


Abstract
:1. Introduction
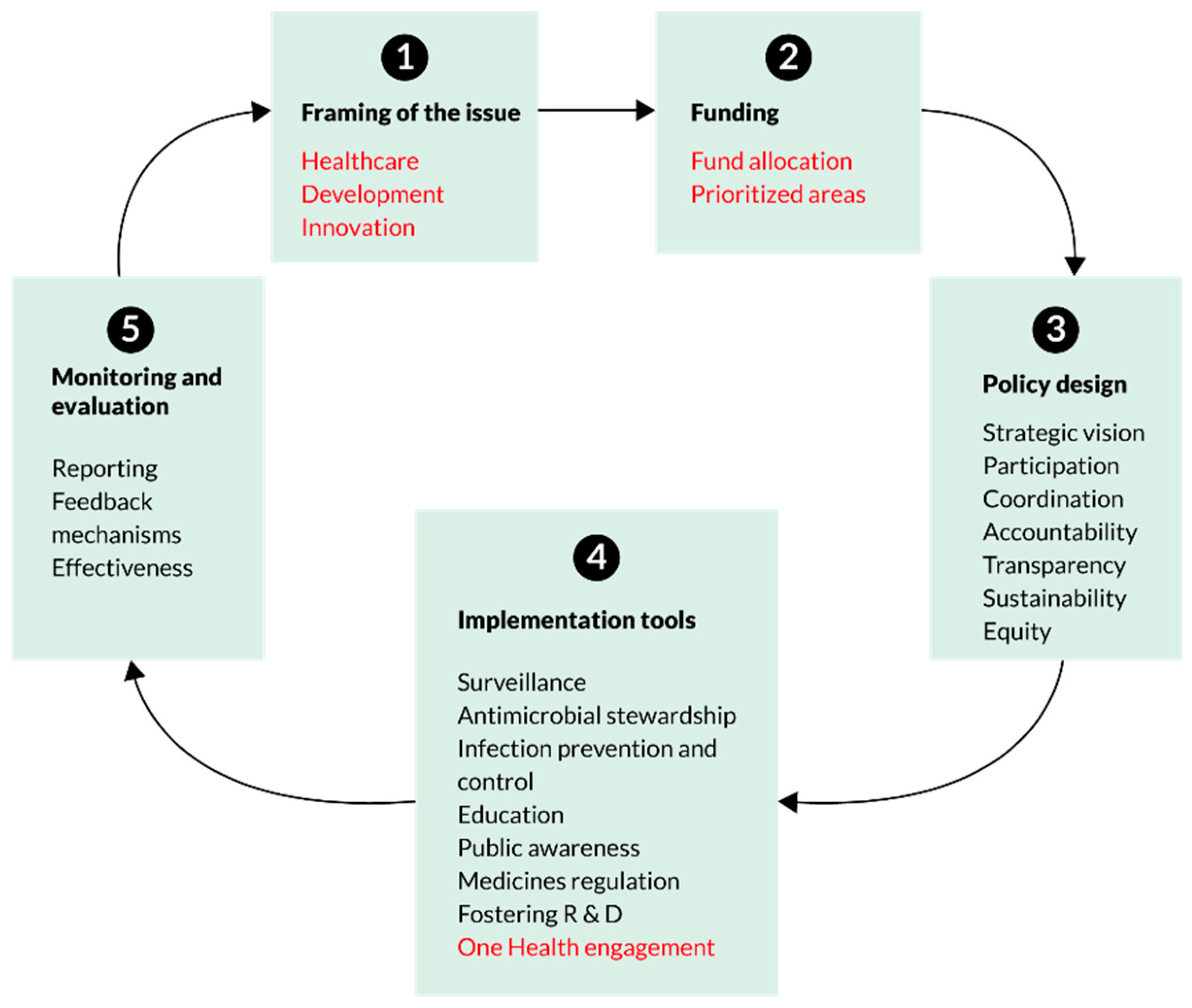
Conceptual Framework
2. Materials and Methods
2.1. Sampling Frame and Sample
2.2. Tool Development
2.3. Ethical Approval
2.4. Data Collection and Management
2.5. Data Analysis
3. Findings
3.1. Setting the Context
3.1.1. Respondent Profile
3.1.2. Framing of AMR
3.1.3. AMR and COVID-19
“COVID-19 is a visible pandemic whereas AMR is a silent one…due to increased use of these drugs, the people of Bangladesh will suffer a lot as no medicine (antibiotics) is going to work for them anymore.”(R16)
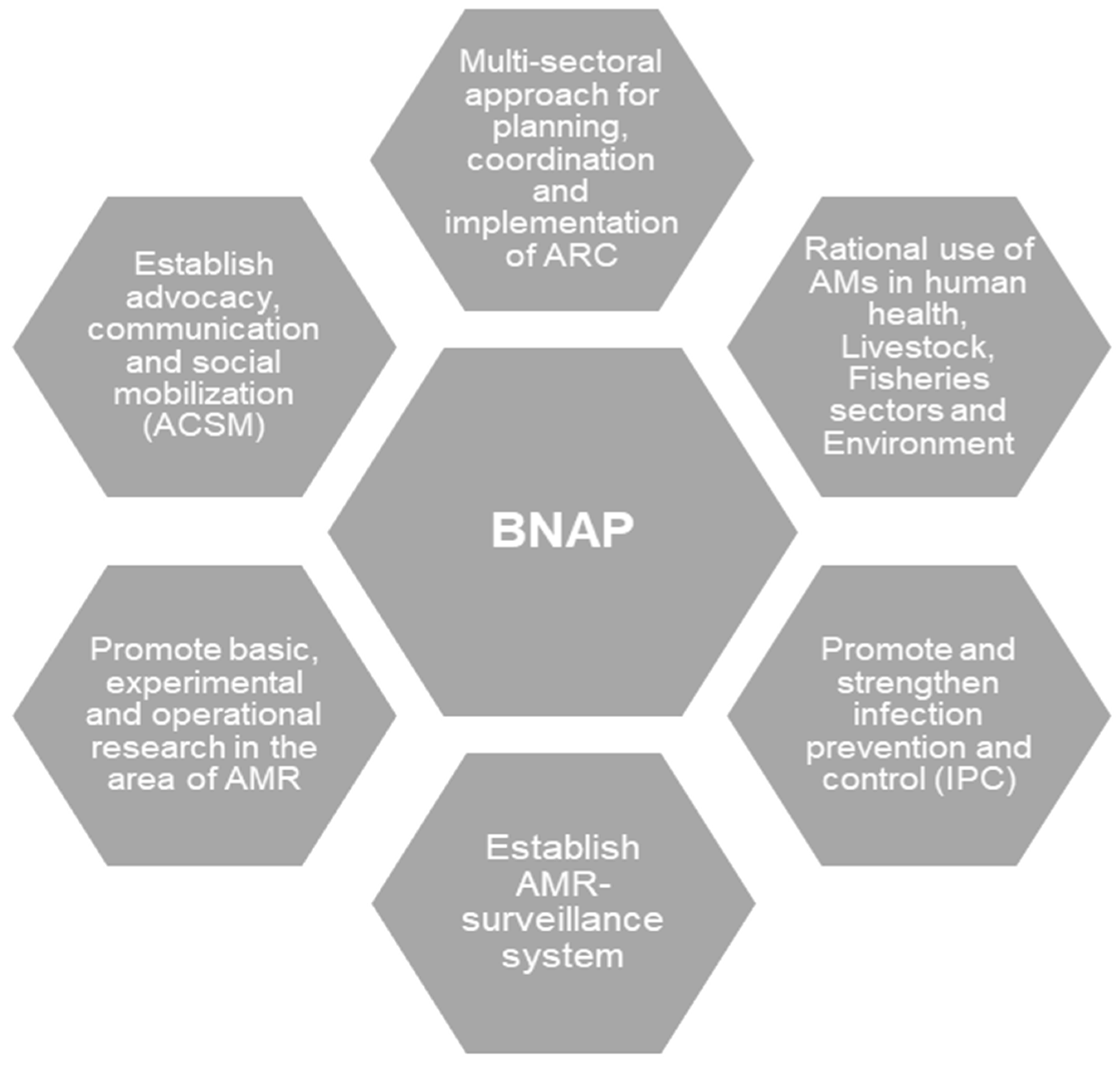
3.2. Development and Implementation of NAP
“During the policy design of NAP, various sectors were involved. But only the three sectors which were actively working for NAP designing were the human health, animal (livestock), and fisheries sectors.”(R2)
“All the meetings are organised by CDC, DGHS since the design of NAP began, which used to hold on a regular basis—due to COVID-19 pandemic, no sectorial meetings were arranged regularly…only the virtual meetings held once/twice during the whole pandemic.”(R4)
3.2.1. Implementation Tool
Awareness-Building
“As per my knowledge, there is no national guidelines/protocol to be followed in the hospitals for AMR containment…few of the hospitals follow guidelines prepared by their respective facility experts.”(R3)
Awareness-Building among Hospital Patients and Attendants
“Awareness on AMR containment usually held during the AMR weeks… as per my knowledge, no such programmes to aware the community people regarding the AMR issues.”(R11)
Infection Prevention and Control in Health Facilities
“IPC is an important component to reduce the AMR …some small scales on-going IPC programmes are running in the country, however, these need to be done on a large scale.”(R1)
“I think, the workforce from livestock sectors also need to be trained on IPC… they also lack knowledge…due to lack of training on AMR-related issues.”(R2)
3.2.2. Monitoring and Evaluation
We are trying to maintain the M&E indicators in our implementation. We have a team for this. Though we could not start the work indicator-wise, we are still trying to follow the indicators.(R7)
“To understand the effectiveness of the programmes, we need to wait for a few more years…”(R15)
“Stewardship is part of NAP, but no one has any idea about it. Drug sellers don’t follow guidelines to prescribe medicines; our people are also not aware of the disadvantages of antibiotics use.”(R16)
3.2.3. Feedback Mechanisms and Reporting
Feedback mechanism and reporting arevery crucial… without these two, we can’t understand the status of surveillance or other activities.(R6)
3.2.4. Sustainability
“Sustainability of the NAP is not ensured because it depends on funding.”(R2)
3.2.5. One Health Engagement
“One health approach is a must to achieve the goals of NAP… environment sector in Bangladesh is yet to take any initiative for containing AMR… so I would say, all sectors should come forward…”(R3)
3.3. Constraints in Implementing NAP
3.3.1. Shortage of Health Workforce
“Shortage of workforce is a common scenario for all sectors… need more people to engage in AMR-related work; otherwise, relevant tasks would not be accomplished on time…”(R11)
“We have only three dedicated staff for AMR-related activities…we can’t achieve our goals with this small workforce.”(R1)
3.3.2. High Turnover
“Staff is switching (some are retired, some are being transferred to other departments, so new employees keep joining all the time… they may not even be interested in AMR containment activities. Some of them also take time to adapt with the NAP on AMR activities.”(R2)
3.3.3. Engagement in COVID-19 Emergency Management
“Most of our staff are involved with COVD-19 related tasks. We have staff shortage even in normal days… now the number of dedicated staff for AMR activities is too less like 2 or 3 persons are working dedicatedly, but it’s not enough.”(R1)
3.3.4. Financial Constraints
“We have financial constraints in almost all sectors… more budgets needed to implement the NAP activities … funds should not depend on donors, our government. should provide funds for AMR-related activities…”(R7)
“The budget is minimal for AMR-related activities in many sectors… no dedicated fund for AMR containment in our department… we will submit a budget soon.”(R2)
3.4. Stakeholders Recommendations
3.4.1. Strengthening Multi-Sectorial Coordination
“We (all sectors) are not working together to implement the NAP on AMR…active participation/involvement from all sectors are important. Otherwise, the implementation plan would be useless.”(R7)
3.4.2. Revision/Update of the NAP Strategy in the Context of COVID-19 Pandemic
“The current version of NAP is old… We need to revise the version soon… the next version is under development although.”(R4)
3.4.3. Proper Documentation for Tracking the Progress of NAP on AMR Activities
“Even our policymakers don’t know about the NAP for containment of AMR-related work progress. Without proper documentation, none of them can understand the current situation, neither can decide the next steps.”(R6)
4. Discussion
Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation (WHO). Worldwide Country Situation Analysis: Response to Antimicrobial Resistance; WHO Document Production Services: Geneva, Switzerland, 2015.
- United Nations (UN). No Time to Wait: Securing the Future from Drug-Resistant Infections. Interagency Collaboration Group on Antimicrobial Resistance. 2019. Available online: https://www.who.int/docs/default-source/documents/no-time-to-wait (accessed on 17 May 2022).
- World Health Organisation (WHO). Antimicrobial resistance: A top ten global public health threat. EClinicalMedicine 2021, 41, 101221. [Google Scholar] [CrossRef] [PubMed]
- Pruden, A.; Arabi, M.; Storteboom, H.N. Correlation between upstream human activities and riverine antibiotic resistance genes. Environ. Sci. Technol. 2012, 46, 11541–11549. [Google Scholar] [CrossRef] [PubMed]
- Uchil, R.R.; Kohli, G.S.; KateKhaye, V.M.; Swami, O.C. Strategies to combat antimicrobial resistance. J. Clin. Diagn. Res. 2014, 8, ME01–ME04. [Google Scholar] [CrossRef] [PubMed]
- Gillings, M.R. Evolutionary consequences of antibiotic use for the resistome, mobilome and microbial pangenome. Front. Microbiol. 2013, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsonage, B.; Hagglund, P.K.; Stephaine, J.D. Control of Antimicrobial Resistance Requires an Ethical Approach. Front. Microbiol. 2017, 8, 2124. [Google Scholar] [CrossRef] [Green Version]
- Dar, O.A.; Hasan, R.; Schlundt, J.; Harbarth, S.; Caleo, G.; Dar, F.K.; Littmann, J.; Rweyemamu, M.; Buckley, E.; Shahid, M.; et al. Exploring the evidence base for national and regional policy interventions to combat resistance. Lancet 2016, 387, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Laxminarayan, R.; Chaudhury, R.R. Antibiotic resistance in India: Drivers and opportunities for action. PLoS Med. 2016, 13, e1001974. [Google Scholar] [CrossRef] [Green Version]
- Mtenga, A.; Emanuel, M.; Mabula, J.; Peter, R. Consumer and Practitioner Education: Status of Antibiotic Resistance; Alliance for the Prudent use of Antibiotics (APUA): Boston, MA, USA, 2011. [Google Scholar]
- World Health Organization. Global Action Plan on Antimicrobial Resistance; WHO Document Production Services: Geneva, Switzerland, 2015.
- Lim, M.J.; Singh, S.R.; Duong, H.L.Q.; Hsu, L.Y.; Tam, C.C. National Interventions To Reduce Inappropriate Antibiotic Use In Humans: A Systematic Review. J. Antimicrob. Chemother. 2019, 75, 14–29. [Google Scholar] [CrossRef] [Green Version]
- Chereau, F.; Opatowski, L.; Tourdjman, M.; Vong, S. Risk assessment for antibiotic resistance in South East Asia. BMJ 2017, 358, j3393. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Situation Analysis of Antimicrobial Resistance in the South East Asia Region; WHO Document Production Services: Geneva, Switzerland, 2015.
- Ahmed, S.M.; Naher, N.; Hossain, T.; Rawal, L.B. Exploring the status of retail private drug shops in Bangladesh and action points for developing an accredited drug shop model: A facility based cross-sectional study. J. Pharm. Pol. Prac. 2017, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Hoque, R.; Ahmed, S.M.; Naher, N.; Islam, M.A.; Rousham, E.K.; Ismal, B.Z.; Hassan, S. Tackling antimicrobial resistance in Bangladesh: A scoping review of policy and practice in human, animal and environment sectors. PLoS ONE 2020, 15, e0227947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohiuddin, M.; Rashid, S.F.; Shuvro, M.I.; Nahar, N.; Ahmed, S.M. Qualitative insights into promotion of pharmaceutical products in Bangladesh: How ethical are the practices? BMC Med. Ethics 2015, 16, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.M.; Hossain, M.A.; Chowdhury, M.R. Informal sector providers in Bangladesh: How equipped are they to provide rational health care? Health Policy Plan. 2009, 24, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Government of Bangladesh (GoB). Strategic Framework and Action Plan for the Application of a One Health Approach in Bangladesh (2017–2021); Final Draft; GoB: Dhaka, Bangladesh, 2018. Available online: http://www.iedcr.org/ (accessed on 17 May 2022).
- Chua, A.Q.; Verma, M.; Hsu, L.Y.; Legido-Quigley, H. An analysis of national action plans on antimicrobial resistance in Southeast Asia using a governance framework. Lancet Reg. Health-West. Pac. 2021, 7, 100084. [Google Scholar] [CrossRef]
- GoB (Disease Control Unit, Communicable Disease Control Program (CDC), Directorate General of Health Services, MoHFW). National Action Plan: Antimicrobial Resistance Containment in Bangladesh 2017–2022; WHO Press: Geneva, Switzerland, 2017.
- Johra, S.T. Fleming’s Warning and the future pandemic (editorial). Bangladesh J. Med. Microbiol. 2021, 15, 1–4. [Google Scholar] [CrossRef]
- World Health Organisation, Bangladesh. Training of Trainers on WHO Bangladesh Package of Essential Noncommunicable Disease Interventions in Primary Health Care Settings. Available online: https://www.google.com/search?client=firefox-b-d&q=Training+of+Trainers+on+WHO+Bangladesh+Package+of+Essential+Noncommunicable+Disease+Interventions+in+Primary+Health+Care+Settings+ (accessed on 17 May 2022).
- Orubu, E.S.F.; Zaman, M.H.; Rahman, M.T.; Wirtz, V.J. Veterinary antimicrobial resistance containment in Bangladesh: Evaluating the national action plan and scoping the evidence on implementation. J. Glob. Antimicrob. Resist. 2020, 21, 105–115. [Google Scholar] [CrossRef]
- Rapid Review. The Implementation of National Action Plan on Antimicrobial Resistance in Bangladesh. unpublished work.
- Lucas, P.J.; Uddin, M.R.; Khisa, N.; Akter, S.M.A.; Unicomb, L.; Nahar, P.; Islam, M.A.; Alam Nizame, F.; Rousham, E.K. Pathways to antibiotics in Bangladesh: A qualitative study investigating how and when households access medicine including antibiotics for humans or animals when they are ill. PLoS ONE 2019, 14, e0225270. [Google Scholar] [CrossRef] [Green Version]
- Adebisi, Y.A.; Jimoh, N.D.; Ogunkola, I.O.; Uwizeyimana, T.; Olayemi, A.H.; Ukor, N.A.; Lucero-Prisno, D.E. The use of antibiotics in COVID-19 management: A rapid review of national treatment guidelines in 10 African countries. Trop. Med. Health 2021, 49, 51. [Google Scholar] [CrossRef]
- Popp, M.; Stegemann, M.; Riemer, M.; Metzendorf, M.I.; Romero, C.S.; Mikolajewska, A.; Kranke, P.; Meybohm, P.; Skoetz, N.; Weibel, S. Antibiotics for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 10, CD015025. [Google Scholar] [CrossRef]
- Khan, M.S.; Bagale, A.D.; Mateus, A.; Sultana, Z.; Hasan, R.; Hanefeld, J. What are the barriers to implementing national antimicrobial resistance action plans? A novel mixed-methods policy analysis in Pakistan. Health Policy Plan. 2020, 35, 973–982. [Google Scholar] [CrossRef]
- Kakkar, A.K.; Shafiq, N.; Singh, G.; Ray, P.; Gautum, V.; Agarwal, R.; Muralidharan, J.; Arora, P. Antimicrobial stewardship programs in resource constrained environments: Understanding and addressing the need of the systems. Front. Public Health 2020, 8, 140. [Google Scholar] [CrossRef] [PubMed]
- Harant, A. Assessing transparency and accountability of national action plans on antimicrobial resistance in 15 African countries. Antimicrob. Resist. Infect. Control. 2022, 11, 15. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, S.M.; Naher, N.; Tune, S.N.B.K.; Islam, B.Z. The Implementation of National Action Plan (NAP) on Antimicrobial Resistance (AMR) in Bangladesh: Challenges and Lessons Learned from a Cross-Sectional Qualitative Study. Antibiotics 2022, 11, 690. https://doi.org/10.3390/antibiotics11050690
Ahmed SM, Naher N, Tune SNBK, Islam BZ. The Implementation of National Action Plan (NAP) on Antimicrobial Resistance (AMR) in Bangladesh: Challenges and Lessons Learned from a Cross-Sectional Qualitative Study. Antibiotics. 2022; 11(5):690. https://doi.org/10.3390/antibiotics11050690
Chicago/Turabian StyleAhmed, Syed Masud, Nahitun Naher, Samiun Nazrin Bente Kamal Tune, and Bushra Zarin Islam. 2022. "The Implementation of National Action Plan (NAP) on Antimicrobial Resistance (AMR) in Bangladesh: Challenges and Lessons Learned from a Cross-Sectional Qualitative Study" Antibiotics 11, no. 5: 690. https://doi.org/10.3390/antibiotics11050690