
Treatment of Pediatric Helicobacter pylori Infection

Abstract
:1. Introduction
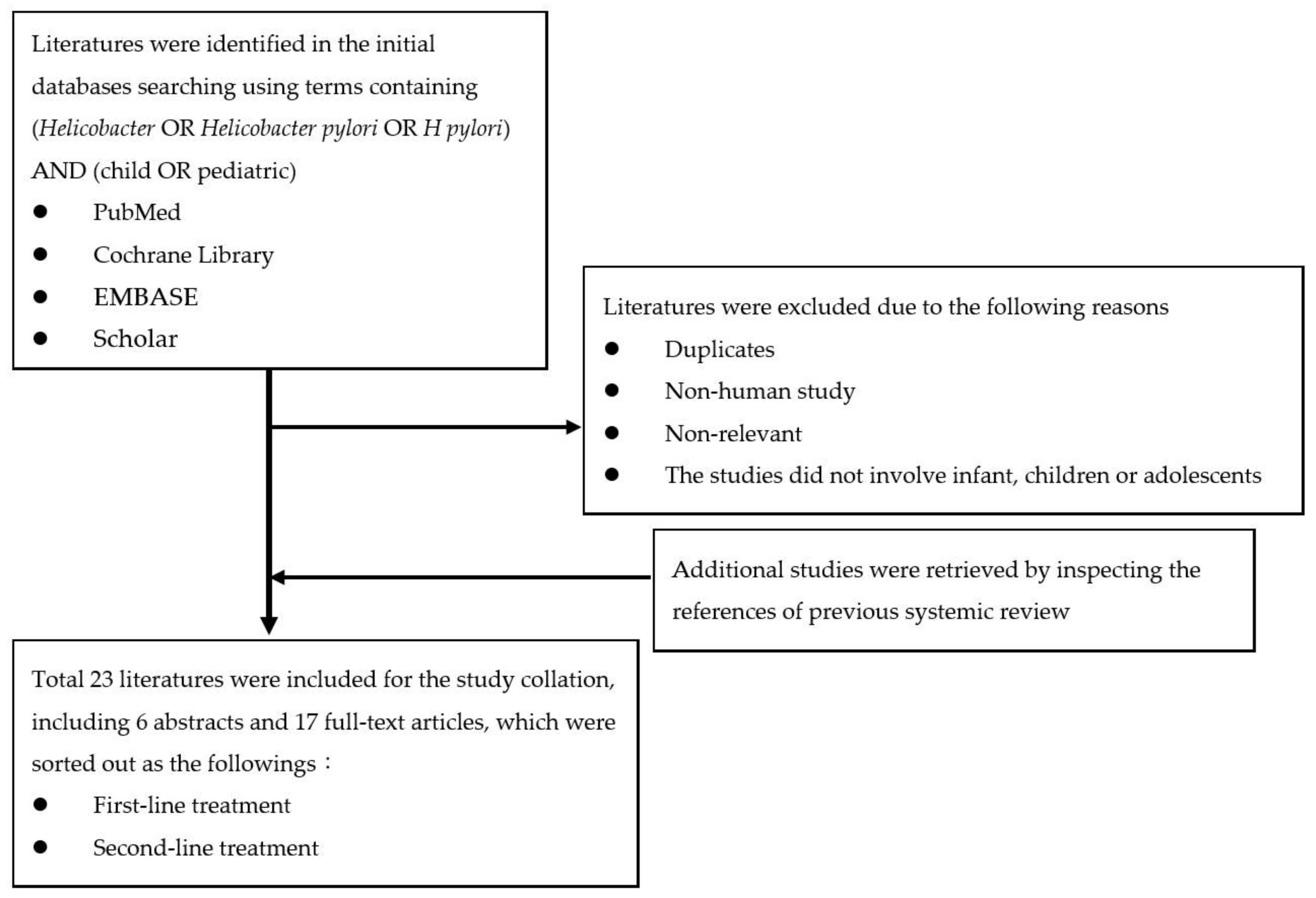
2. Methods
3. Results
3.1. First-Line Treatment

{kind=link}
| Published Year | Region | Helicobacter pylori Antimicrobial Susceptibility | ||||
|---|---|---|---|---|---|---|
| Susceptible to CLA and MET | Resistant to MET, Susceptible to CLA | Resistant to CLA, Susceptible to MET | Resistant to CLA and MET | Unknown | ||
| 2016 [10] | Europe | PPI-AMO-CLA 14 d | PPI-AMO-MET 14 d | PPI-high dose AMO-MET 14 d | ||
| Sequential therapy 10 d # | BIS-PPI-AMO-MET * 14 d # | BIS-PPI-AMO-MET * 14 d # | BIS-PPI-AMO-MET 14 d # | |||
| Concomitant therapy for 14 d *# | ||||||
| Doses (morning dose/evening dose) of PPI and antibiotics are calculated based on the body weight and age: | ||||||
| Body weight | 15–24 kg | 25–34 kg | >35 kg | |||
| PPI | 20 mg/20 mg | 30 mg/30 mg | 40 mg/40 mg | |||
| The PPI dose refers to esomeprazole and omeprazole and should be adapted if other PPIs are used. | ||||||
| AMO | 500 mg/500 mg | 750 mg/750 mg | 1000 mg/1000 mg | |||
| High dose AMO | 750 mg/750 mg | 1000 mg/1000 mg | 1500 mg/1500 mg | |||
| CLA | 250 mg/250 mg | 500 mg/250 mg | 500 mg/500 mg | |||
| MET | 250 mg/250 mg | 500 mg/250 mg or 375 mg/375 mg | 500 mg/500 mg | |||
| Age | <10 years | >10 years | ||||
| BIS | 262 mg QID | 524 mg QID | ||||
| Bismuth in the United States and Canada comes as bismuth subsalicylate. | ||||||
| 2019 [18] | Korea | PPI-AMO-CLA 14 d | PPI-AMO-MET 14 d | PPI-high dose AMO-MET 14 d | ||
| Sequential therapy 10 d # | BIS-PPI-AMO (TET)-MET 14 d *# | BIS-PPI-AMO (TET)-MET 14 d *# | BIS-PPI-AMO (TET)-MET 14 d *# | |||
| Concomitant therapy 14 d *# | ||||||
| The doses of PPI, Amoxicillin, Clarithromycin, Metronidazole, and Bismuth are the same as stated above except for esomeprazole or omeprazole (1.5–2.5 mg/kg/d) are also mentioned. | ||||||
| TET | 500 mg QID (>12 years old, >40 kg) | |||||
| 2020 [5] | Japan | PPI-AMO-CLA 7–14 d | PPI -AMO-MET 7–14 d | PPI-AMO-CLA 7–14 d | ||
| Twice daily | Maximum daily dose (mg/day) | |||||
| PPI | ||||||
| Lansoprazole | 1.5 mg/kg/day | 60 | ||||
| Omeprazole | 1.0 mg/kg/day | 40 | ||||
| Rabeprazole | 0.5 mg/kg/day | 20 | ||||
| Esomeprazole | ≥4 years old Body weight < 30 kg | 20 mg/day | 40 | |||
| Bodyweight ≥ 30 kg | 40 mg/day | |||||
| AMO | 50 mg/kg/day | 1500 | ||||
| CLA | 15–20 mg/kg/day | 800 | ||||
| MET | 10–20 mg/kg/day | 500 | ||||
| Study | Region | Study Period | Follow-Up Case Number | Treatment | Eradication Rate |
|---|---|---|---|---|---|
| Francavilla et al., 2005 [21] | Italy | 2002 to 2004 | 74 (Age 3.3–18 years; median age 12.3 years) | Triple therapy for 7 days OME + AMO + MET | 75.7% (28/37) |
| Sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA + TIN for 5 days | 97.3% (36/37) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, at least 4 weeks after the end of therapy | |||||
| Lerro et al., 2006 [26] (abstract) | Italy | Not available | 25 (Median age 12.3 years) | Triple therapy for 7 days OME + AMO + TIN | 80% (20/25) |
| 25 (Median age 11.9 years) | Sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA + TIN for 5 days | 92% (23/25) | |||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 6 weeks after the end of therapy | |||||
| Hurduc et al., 2007 | Romania | Not available | 135 | Triple therapy for 7–14 days * PPI + 2 antibiotics (type of medication was not reported) | 80% (36/45) |
| Sequential therapy for 10 days * OME + AMO for 5 days followed by OME + CLA + TIN for 5 days | 86.7% (39/45) | ||||
| Lu et al., 2010 [27] | China | 2006 to 2009 | 33 (Mean age 10.2 ± 2.8 years) | Standard triple therapy for 10 days OME + AM + CLA | 78.8% (26/33) |
| 38 (Mean age 10.7 ± 2.4 years) | Sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA+ TIN for 5 days | 94.7% (36/38) | |||
| The method that detects the eradication of H. pylori: 13C-urea breath test, at least 4 weeks after the end of therapy | |||||
| Anania et al., 2011 [23] (abstract) | Italy | Not available | 15 (Age 5.8–16.7 years; median age 11 years) | Concomitant therapy for 5 days * OME + AMO + CLA + TIN | 93.3% (14/15) |
| 15 (Age 4.8–14.1 years; median age 7.6 years) | Sequential therapy for 10 days * OME + AMO for 5 days followed by OME + CLA + TIN for 5 days | 86.7% (13/15) | |||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 8 weeks after the end of therapy | |||||
| Bontems et al., 2011 [28] | Belgian, France, Italy | 2007 to 2009 | 150 (Median age 10.4 years) | Standard triple therapy for 7 days OME + AMO + CLA or MET for CLA-resistant strains | 80.8% (59/73) |
| Standard sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA + MET for 5 days | 88.3% (68/77) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, at least 8 weeks after the end of therapy | |||||
| Albrecht et al., 2011 [29] | Poland | 2006 to 2009 | 103 (Age 3 to 18 years) | Standard triple therapy for 7 days + Placebo for 3 days OME + AMO + CLA for 7 days followed by placebo for 3 days | 68.6% (35/51) |
| Sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA + TIN for 5 days | 86.5% (45/52) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 6–8 weeks after the end of therapy | |||||
| Liu et al., 2011 [30] (abstract) | China | Not available | 100 | Standard triple therapy for 10 days * OME + AMO + CLA | 69.0% (33) |
| Triple therapy for 10 days * OME + AMO + MET | 76.7% (33) | ||||
| Standard sequential therapy for 10 days * OME + AMO for 5 days followed by OME + CLA + MET for 5 days | 91.2% (34) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 4 weeks after the end of therapy | |||||
| Hong et al., 2012 [31] | Seoul, Korea | 2004 to 2012 | 62 (Age 3.1–16.6 years; mean age 11.0±3.2 years) | Standard triple therapy for 14 days OME + AMO + CLA | 67.7% (42/62) |
| 56 (Age 2.7–18.6; mean age 11.0±3.3 years) | Bismuth-based quadruple therapy for 7 days OME + AMO + MET + BIS citrate | 83.9% (47/56) | |||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 4 weeks after the end of therapy | |||||
| Huang et al., 2012 [32] (abstract) | Not available | Not available | 199 | Triple therapy for 7 days OME + AMC + CLA | 71.4% |
| Triple therapy for 10 days | 67.3% | ||||
| Triple therapy for 14 days | 82.0% | ||||
| Sequential therapy for 10 days OME + AMC for 5 days followed by OME + CLA + MET for 5 days | 90.2% | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 4 weeks after the end of therapy | |||||
| Hojsak, et al., 2012 [33] | Croatia | 2001 to 2010 | 186 (Age 1.08–18.8 years; median age 12.9 years) | Triple therapy for 7–10 days PPI 1–2 mg/kg/day + AMO + MET or CLA | 81.2% (151/186) |
| The method that detects the eradication of H. pylori: urea breath test or repeated endoscopy with culture | |||||
| Huang et al., 2013 [34] | China | 2008 to 2010 | 318 (Age 3–16 years) | Standard triple therapy for 7 days OME + AMO + CLA | 70.9% (73/103) |
| Standard triple therapy for 10 days | 77.8% (84/108) | ||||
| Standard sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA + MET for 5 days | 89.7% (96/107) | ||||
| The method that detects the eradication of H. pylori: stool antigen test, 4 weeks after the end of therapy | |||||
| Ali Habib HS et al., 2013 [35] | Jeddah, Saudi Arabia | Not available | 16 (Age 12–15 years, male) | Standard triple therapy for 10 days rabeprazole + AMO + CLA | 55.6% (5/9) |
| Sequential therapy for 10 days rabeprazole + AMO for 5 days followed by rabeprazole + CLA + TIN for 5 days | 57.1% (4/7) | ||||
| The method that detects the eradication of H. pylori: 14C-urea breath test, 6 weeks after the end of therapy | |||||
| Laving et al., 2013 [36] | Kenya | 2007 | 71 (Age 2–16 years; mean age 8.9 years) | Standard triple therapy for 10 days OME + AMO + CLA | 48.9% (22/45) |
| Sequential therapy for 10 days OME + AMO for 5 days followed by OME + CLA + TIN for 5 days | 84.6% (22/26) | ||||
| The method that detects the eradication of H. pylori: a stool antigen test and/or a repeat histology obtained at repeat endoscopy, 6 weeks after the end of therapy | |||||
| Baysoy et al., 2013 [37] | Turkey | 2008 to 2010 | 61 (Age 4–18 years) | Standard triple therapy for 14 days LAN + AMO + CLA | 54.2% (13/24) |
| Sequential therapy for 10 days LAN + AMO for 5 days followed by LAN + CLA+ ORN for 5 days | 48.6% (18/37) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 6–8 weeks after the end of therapy | |||||
| Kutluk et al., 2014 [38] | Turkey | 2011 | 136 (Age 3–18 years) | Standard triple therapy for 10 days LAN + AMO + CLA | 55.7% (39/70) |
| Standard sequential therapy for 10 days LAN + AMO for 5 days followed by LAN + CLA and MET for 5 days | 56.1% (37/66) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, 4–6 weeks after the end of therapy | |||||
| Schwarzer, et al., 2016 [39] | European, a registry from nine European centers | 2009 to 2011 | 209 (Age 3.1– 17.9 years) | Standard sequential therapy for 10 days ESO + AMO for 5 days followed by ESO + CLA + MET for 5 days (Dosage was chosen depending on weight: 15–24 kg, 25–34 kg, >35 kg) | 80.4% (168/209) |
| The method that detects the eradication of H. pylori: 13C-urea breath test, by upper endoscopy with culture and histology, and/or by a monoclonal stool antigen test, 8–12 weeks after the end of therapy | |||||
| Zhou et al., 2020 [40] | China | 2017 to 2018 | 228 (Age 6– 18 years) | Standard triple therapy for 14 days OME + AMO + CLA | 74.1% (43/58) |
| Sequential therapy for 14 days OME + AMO for 7 days followed by OME + CLA + MET for 7 days | 69.5% (41/59) | ||||
| Bismuth-based quadruple therapy for 14 days OME + AMO + MET + elemental BIS | 89.8% (53/59) | ||||
| Standard concomitant therapy for 14 days OME + AMO + CLA + MET | 84.6% (44/52) | ||||
| The method that detects the eradication of H. pylori: 13C-urea breath test, at least 4 weeks after the end of therapy | |||||
3.1.1. Triple Therapy
3.1.2. Sequential Therapy
3.1.3. Concomitant Therapy
3.1.4. Bismuth-Based Quadruple Therapy
3.1.5. Adjuvant Therapy with Probiotics
3.2. Second-Line Treatment
3.3. Adverse Event
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vakil, N.; Malfertheiner, P.; Chey, W.D. Helicobacter pylori infection. N. Engl. J. Med. 2010, 363, 595–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, J.R.; Marshall, B. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983, 1, 1273–1275. [Google Scholar] [PubMed]
- Salama, N.R.; Hartung, M.L.; Müller, A. Life in the human stomach: Persistence strategies of the bacterial pathogen Helicobacter pylori. Nat. Rev. Microbiol. 2013, 11, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic review with meta-analysis: The worldwide prevalence of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Kato, S.; Shimizu, T.; Toyoda, S.; Gold, B.D.; Ida, S.; Ishige, T.; Fujimura, S.; Kamiya, S.; Konno, M.; Kuwabara, K.; et al. The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2020, 62, 1315–1331. [Google Scholar] [CrossRef]
- Dror, G.; Muhsen, K. Helicobacter pylori Infection and Children’s Growth: An Overview. J. Pediatr. Gastroenterol. Nutr. 2016, 62, e48–e59. [Google Scholar] [CrossRef]
- Roka, K.; Roubani, A.; Stefanaki, K.; Panayotou, I.; Roma, E.; Chouliaras, G. The prevalence of Helicobacter pylori gastritis in newly diagnosed children with inflammatory bowel disease. Helicobacter 2014, 19, 400–405. [Google Scholar] [CrossRef]
- Ren, S.; Cai, P.; Liu, Y.; Wang, T.; Zhang, Y.; Li, Q.; Gu, Y.; Wei, L.; Yan, C.; Jin, G. Prevalence of Helicobacter pylori infection in China: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2021, 37, 464–470. [Google Scholar] [CrossRef]
- Yeung, C.-Y.; Lee, H.-C. Paediatric Helicobacter pylori infection in Taiwan: Current status and perspectives. Gastroenterology 2017, 6, 90–97. [Google Scholar]
- Jones, N.L.; Koletzko, S.; Goodman, K.; Bontems, P.; Cadranel, S.; Casswall, T.; Czinn, S.; Gold, B.D.; Guarner, J.; Elitsur, Y.; et al. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 991–1003. [Google Scholar] [CrossRef]
- Sierra, M.S.; Hastings, E.V.; Goodman, K.J. What do we know about benefits of H. pylori treatment in childhood? Gut Microbes 2013, 4, 549–567. [Google Scholar] [CrossRef] [Green Version]
- Kalach, N.; Bontems, P.; Cadranel, S. Advances in the treatment of Helicobacter pylori infection in children. Ann. Gastroenterol. 2015, 28, 10–18. [Google Scholar]
- Perri, F.; Pastore, M.; Clemente, R.; Festa, V.; Quitadamo, M.; Niro, G.; Conoscitore, P.; Rutgeerts, P.; Andriulli, A. Helicobacter pylori infection may undergo spontaneous eradication in children: A 2-year follow-up study. J. Pediatr. Gastroenterol. Nutr. 1998, 27, 181–183. [Google Scholar] [CrossRef]
- van Zanten, S.V. Knowledge Translation Action is Needed to Address Problems in Adherance to Pediatric Helicobacter Consensus Guidelines in Clinical Practice. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 138–139. [Google Scholar] [CrossRef]
- Ertem, D. Clinical practice: Helicobacter pylori infection in childhood. Eur. J. Pediatr. 2013, 172, 1427–1434. [Google Scholar] [CrossRef]
- Bonilla, S.; Mitchell, P.D.; Mansuri, I. Low Adherence to Society Guidelines for the Management of Helicobacter pylori among Pediatric Gastroenterologists. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 178–183. [Google Scholar] [CrossRef]
- Eren, M.; Dinleyici, E.Ç.; Hekim, S. Third-line rescue therapy with Levofloxacin based protocol for H. pylori eradication in children. Cocuk Enfeksiyon Derg. 2009, 3, 98–103. [Google Scholar]
- Jun, J.S.; Seo, J.H.; Park, J.S.; Rhee, K.H.; Youn, H.S. Changes in the Treatment Strategies for Helicobacter pylori Infection in Children and Adolescents in Korea. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 417–430. [Google Scholar] [CrossRef]
- Huang, Y.; Zhan, X. Sequential Therapy is Superior to Triple Therapy for Helicobacter pylori Infection in Children: A Meta-Analysis. Indian J. Pediatr. 2016, 83, 307–315. [Google Scholar] [CrossRef]
- Horvath, A.; Dziechciarz, P.; Szajewska, H. Meta-analysis: Sequential therapy for Helicobacter pylori eradication in children. Aliment. Pharmacol. Ther. 2012, 36, 534–541. [Google Scholar] [CrossRef]
- Francavilla, R.; Lionetti, E.; Castellaneta, S.P.; Magistà, A.M.; Boscarelli, G.; Piscitelli, D.; Amoruso, A.; Di Leo, A.; Miniello, V.L.; Francavilla, A.; et al. Improved efficacy of 10-Day sequential treatment for Helicobacter pylori eradication in children: A randomized trial. Gastroenterology 2005, 129, 1414–1419. [Google Scholar] [CrossRef] [PubMed]
- Nyssen, O.P.; McNicholl, A.G.; Megraud, F.; Savarino, V.; Oderda, G.; Fallone, C.A.; Fischbach, L.; Bazzoli, F.; Gisbert, J.P. Sequential versus standard triple first-line therapy for Helicobacter pylori eradication. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Anania, C.; Di Nardo, G.; Olivero, G.; Ferraro, F.; Olivero, O.; Pacifico, L. Sequential versus concomitant therapy for Helicobacter pylori infection in children: A pilot study. J. Pediatr. Gastroenterol. Nutr. 2011, 52, E170–E171. [Google Scholar]
- Hurduc, V.; Dragomir, D.; Leseanu, G.; Sajin, M. Comparison of sequential and triple therapies in the eradication of H. pylori infection in symptomatic children. Gut 2007, 56, A243. [Google Scholar]
- Gatta, L.; Vakil, N.; Leandro, G.; Di Mario, F.; Vaira, D. Sequential therapy or triple therapy for Helicobacter pylori infection: Systematic review and meta-analysis of randomized controlled trials in adults and children. Am. J. Gastroenterol. 2009, 104, 3069–3079. [Google Scholar] [CrossRef]
- Lerro, P.; Kuvidi, M.; Baldi, M.; Calvo, P.; Barbera, C. A 10-day sequential therapy: New option for Helicobacter pylori eradication in children. Dig. Liver Dis. 2006, 38, A104–A105. [Google Scholar] [CrossRef]
- Lu, J.H.; Xu, M.Y.; Sheng, Y.; Yang, W.X. Comparison of the efficacy of 10-day sequential therapy and conventional triple therapy for Helicobacter pylori eradication in children. Zhongguo Dang Dai Er Ke Za Zhi Chin. J. Contemp. Pediatr. 2010, 12, 988–990. [Google Scholar]
- Bontems, P.; Kalach, N.; Oderda, G.; Salame, A.; Muyshont, L.; Miendje, D.Y.; Raymond, J.; Cadranel, S.; Scaillon, M. Sequential therapy versus tailored triple therapies for Helicobacter pylori infection in children. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 646–650. [Google Scholar] [CrossRef]
- Albrecht, P.; Kotowska, M.; Szajewska, H. Sequential therapy compared with standard triple therapy for Helicobacter pylori eradication in children: A double-blind, randomized, controlled trial. J. Pediatr. 2011, 159, 45–49. [Google Scholar] [CrossRef]
- Liu, F.-L.; Zhen, L.-N.; Zhao, Y.; Xia, Z.-W.; Situ, A.-M.; Zhang, S.-H. The efficacy of sequential therapy and standard triple therapy for eradication of Helicobacter pylori infection in children. J. Clin. Pediatr. 2011, 29, 925–928. [Google Scholar]
- Hong, J.; Yang, H.R. Efficacy of Proton Pump Inhibitor-based Triple Therapy and Bismuth-based Quadruple Therapy for Helicobacter pylori Eradication in Korean Children. Pediatr. Gastroenterol. Hepatol. Nutr. 2012, 15, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Gong, S.T.; Ou, W.J.; Pan, R.F.; Geng, L.L.; Huang, H.; He, W.E.; Chen, P.Y.; Liu, L.Y.; Zhou, L.Y. A 10-day sequential therapy for eradication of Helicobacter pylori infection in children. Zhonghua Er Ke Za Zhi Chin. J. Pediatr. 2012, 50, 563–567. [Google Scholar]
- Hojsak, I.; Kos, T.; Dumančić, J.; Mišak, Z.; Jadrešin, O.; Jaklin Kekez, A.; Lukić Grlić, A.; Kolaček, S. Antibiotic resistance of Helicobacter pylori in pediatric patients—10 years’ experience. Eur. J. Pediatr. 2012, 171, 1325–1330. [Google Scholar] [CrossRef]
- Huang, J.; Zhou, L.; Geng, L.; Yang, M.; Xu, X.W.; Ding, Z.L.; Mao, M.; Wang, Z.L.; Li, Z.L.; Li, D.Y.; et al. Randomised controlled trial: Sequential vs. standard triple therapy for Helicobacter pylori infection in Chinese children-a multicentre, open-labelled study. Aliment. Pharmacol. Ther. 2013, 38, 1230–1235. [Google Scholar] [CrossRef]
- Ali Habib, H.S.; Murad, H.A.; Amir, E.M.; Halawa, T.F. Effect of sequential versus standard Helicobacter pylori eradication therapy on the associated iron deficiency anemia in children. Indian J. Pharmacol. 2013, 45, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Laving, A.; Kamenwa, R.; Sayed, S.; Kimang’a, A.N.; Revathi, G. Effectiveness of sequential v. standard triple therapy for treatment of Helicobacter pylori infection in children in Nairobi, Kenya. S. Afr. Med. J. Suid-Afrik. Tydskr. Vir Geneeskd. 2013, 103, 921–924. [Google Scholar] [CrossRef] [Green Version]
- Baysoy, G.; Saltık Temızel, İ.N.; Uslu, N.; Balamtekın, N.; Demır, H.; Gürkan, F.; Özen, H.; Akyön, Y.; Yüce, A. Ornidazole-based sequential therapy is not effective in Helicobacter pylori eradication in children. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2013, 24, 382–386. [Google Scholar] [CrossRef]
- Kutluk, G.; Tutar, E.; Bayrak, A.; Volkan, B.; Akyon, Y.; Celikel, C.; Ertem, D. Sequential therapy versus standard triple therapy for Helicobacter pylori eradication in children: Any advantage in clarithromycin-resistant strains? Eur. J. Gastroenterol. Hepatol. 2014, 26, 1202–1208. [Google Scholar] [CrossRef]
- Schwarzer, A.; Bontems, P.; Urruzuno, P.; Kalach, N.; Iwanczak, B.; Roma-Giannikou, E.; Sykora, J.; Kindermann, A.; Casswall, T.; Cadranel, S.; et al. Sequential Therapy for Helicobacter pylori Infection in Treatment-naïve Children. Helicobacter 2016, 21, 106–113. [Google Scholar] [CrossRef]
- Zhou, Y.; Ye, Z.; Wang, Y.; Zhang, Y.; Tang, Z.; Yan, W.; Jiang, Y.; Huang, Y. Comparison of four different regimens against Helicobacter pylori as a first-line treatment: A prospective, cross-sectional, comparative, open trial in Chinese children. Helicobacter 2020, 25, e12679. [Google Scholar] [CrossRef] [Green Version]
- Homan, M.; Orel, R. Are probiotics useful in Helicobacter pylori eradication? World J. Gastroenterol. 2015, 21, 10644–10653. [Google Scholar] [CrossRef] [PubMed]
- Sgouras, D.; Maragkoudakis, P.; Petraki, K.; Martinez-Gonzalez, B.; Eriotou, E.; Michopoulos, S.; Kalantzopoulos, G.; Tsakalidou, E.; Mentis, A. In vitro and in vivo inhibition of Helicobacter pylori by Lactobacillus casei strain Shirota. Appl. Environ. Microbiol. 2004, 70, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacifico, L.; Osborn, J.F.; Bonci, E.; Romaggioli, S.; Baldini, R.; Chiesa, C. Probiotics for the treatment of Helicobacter pylori infection in children. World J. Gastroenterol. 2014, 20, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.; Fatemeh, F.; Mehri, N.; Maryam, S. Probiotics for the treatment of pediatric helicobacter pylori infection: A randomized double blind clinical trial. Iran J. Pediatr. 2013, 23, 79–84. [Google Scholar]
- Fang, H.R.; Zhang, G.Q.; Cheng, J.Y.; Li, Z.Y. Efficacy of Lactobacillus-supplemented triple therapy for Helicobacter pylori infection in children: A meta-analysis of randomized controlled trials. Eur. J. Pediatr. 2019, 178, 7–16. [Google Scholar] [CrossRef]
- Seo, J.H.; Park, J.S.; Youn, H.S. Recent changes in the treatment of helicobacter pylori infection in children and adolescents. Korean J. Helicobacter Up. Gastrointest. Res. 2021, 21, 188–193. [Google Scholar] [CrossRef]
- Genis, N.; Salame, A.; Lenga, E.; Mahler, T.; Scaillon, M.; Cadranel, S.; Bontems, P. LOW efficacy of rescue treatments for H. pylori eradication in children after failure of a first sequential regimen. Helicobacter 2013, 18, 81–82. [Google Scholar] [CrossRef]
- Kallirroi, K.; Salame, A.; Lenga, E.; Mahler, T.; Miendje-Deyi, V.Y.; Urbanowicz, M.; Cadranel, S.; Bontems, P. Low efficacy of second line treatments for H. pylori eradication in children. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 668. [Google Scholar] [CrossRef]
- Aguilera Matos, I.; Diaz Oliva, S.E.; Escobedo, A.A.; Villa Jiménez, O.M.; Velazco Villaurrutia, Y.D.C. Helicobacter pylori infection in children. BMJ Paediatr. Open 2020, 4, e000679. [Google Scholar] [CrossRef]
- Jansson, L.; Agardh, D. Prevalence of clarithromycin-resistant Helicobacter pylori in children living in South of Sweden: A 12-year follow-up. Scand. J. Gastroenterol. 2019, 54, 838–842. [Google Scholar] [CrossRef] [Green Version]
- Yousefi-Avarvand, A.; Vaez, H.; Tafaghodi, M.; Sahebkar, A.H.; Arzanlou, M.; Khademi, F. Antibiotic Resistance of Helicobacter pylori in Iranian Children: A Systematic Review and Meta-Analysis. Microb. Drug Resist. 2018, 24, 980–986. [Google Scholar] [CrossRef]
- Nguyen, T.V.; Bengtsson, C.; Yin, L.; Nguyen, G.K.; Hoang, T.T.; Phung, D.C.; Sörberg, M.; Granström, M. Eradication of Helicobacter pylori in children in Vietnam in relation to antibiotic resistance. Helicobacter 2012, 17, 319–325. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e1317. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.H.; Lai, F.P.; Lo, H.Y.; Sheu, B.S.; Yang, Y.J. Increasing antimicrobial resistance to clarithromycin and metronidazole in pediatric Helicobacter pylori infection in southern Taiwan: A comparison between two decades. Helicobacter 2019, 24, e12633. [Google Scholar] [CrossRef]
- Osaki, T.; Konno, M.; Yonezawa, H.; Hojo, F.; Zaman, C.; Takahashi, M.; Fujiwara, S.; Kamiya, S. Analysis of intra-familial transmission of Helicobacter pylori in Japanese families. J. Med. Microbiol. 2015, 64, 67–73. [Google Scholar] [CrossRef]
- Zhao, J.B.; Yuan, L.; Yu, X.C.; Shao, Q.Q.; Ma, J.; Yu, M.; Wu, Y.; Qi, Y.B.; Hu, R.B.; Wei, P.R.; et al. Whole family-based Helicobacter pylori eradication is a superior strategy to single-infected patient treatment approach: A systematic review and meta-analysis. Helicobacter 2021, 26, e12793. [Google Scholar] [CrossRef]

| Medication | Dosage | Study | Maximum Dose | |
|---|---|---|---|---|
| PPI | OME | 1 mg/kg/day | Francavilla et al., 2005 Lerro et al., 2006 Albrecht et al., 2011 Hong et al., 2012 Laving et al., 2013 Zhou et al., 2020 | 40 mg/day |
| 0.8 mg/kg/day | Lu et al., 2010 | |||
| 0.8–1.0 mg/kg/day | Huang et al., 2012 Huang et al., 2013 | |||
| 10 mg twice a day below 30 kg | Bontems et al., 2011 | |||
| 20 mg twice a day above 30 kg | ||||
| LAN | 1 mg/kg/day | Baysoy et al., 2013 Kutluk et al., 2014 | 30 mg/day | |
| Rabeprazole | 40 mg/day | Ali Habib HS et al., 2013 | ||
| Antibiotics | AMO | 50 mg/kg/day | Francavilla et al., 2005 Lerro et al., 2006 Bontems et al., 2011 Albrecht et al., 2011 Hojsak, et al., 2012 Hong et al., 2012 Baysoy et al., 2013 Laving et al., 2013 Kutluk et al., 2014 Zhou et al., 2020 | 2 g/day |
| 40 mg/kg/day | Lu et al., 2010 | |||
| 30 mg/kg/day | Huang et al., 2013 | |||
| 1 g/day | Ali Habib HS et al., 2013 | |||
| AMC | 50 mg/kg/day | Huang et al., 2012 | ||
| CLA | 15 mg/kg/day | Francavilla et al., 2005 Lerro et al., 2006 Lu et al., 2010 Bontems et al., 2011 Hong et al., 2012 Baysoy et al., 2013 Laving et al., 2013 | 1 g/day | |
| 20 mg/kg/day | Albrecht et al., 2011 Hojsak, et al., 2012 Huang et al., 2012 Huang et al., 2013 Kutluk et al., 2014 Zhou et al., 2020 | |||
| 500 mg/day | Ali Habib HS et al., 2013 | |||
| MET | 15 mg/kg/day | Francavilla et al., 2005 | ||
| 20 mg/kg/day | Kutluk et al., 2014 Zhou et al., 2020 | 1 g/day | ||
| Bontems et al., 2011 Hojsak, et al., 2012 Hong et al., 2012 Huang et al., 2012 Huang et al., 2013 | 1.5 g/day | |||
| TIN | 20 mg/kg/day | Francavilla et al., 2005 Lerro et al., 2006 Albrecht et al., 2011 Laving et al., 2013 | 1 g/day | |
| 15 mg/kg/day | Lu et al., 2010 | |||
| 1 g/day | Ali Habib HS et al., 2013 | |||
| ORN | 30 mg/kg/day | Baysoy et al., 2013 | ||
| BIS | bismuth citrate 8 mg/kg/day | Hong et al., 2012 | ||
| elemental bismuth 6–8 mg/kg/day | Zhou et al., 2020 | 330 mg/day |
| Published Year | Region | Helicobacter pylori Antimicrobial Susceptibility | ||||
|---|---|---|---|---|---|---|
| Past Treatment Regimen | Susceptible to CLA and MET | Resistant to MET, Susceptible to CLA | Resistant to CLA, Susceptible to MET | Unknown | ||
| 2016 [10] | Europe | PPI-AMO-CLA | PPI-AMO-MET | ◎ | - | ◎ |
| PPI-AMO-MET | PPI-AMO-CLA | - | Treatment like double resistance (#) | |||
| Sequential therapy | ◎ | - | - | |||
| Doses (morning dose/evening dose) of PPI and antibiotics are calculated based on the body weight and age: | ||||||
| Body weight | 15–24 kg | 25–34 kg | >35 kg | |||
| PPI | 20 mg/20 mg | 30 mg/30 mg | 40 mg/40 mg | |||
| The PPI dose refers to esomeprazole and omeprazole and should be adapted if other PPIs are used. | ||||||
| AMO | 500 mg/500 mg | 750 mg/750 mg | 1000 mg/1000 mg | |||
| High dose AMO | 750 mg/750 mg | 1000 mg/1000 mg | 1500 mg/1500 mg | |||
| CLA | 250 mg/250 mg | 500 mg/250 mg | 500 mg/500 mg | |||
| MET | 250 mg/250 mg | 500 mg/250 mg or 375 mg/375 mg | 500 mg/500 mg | |||
| Age | <10 years | >10 years | ||||
| BIS | 262 mg QID | 524 mg QID | ||||
| Bismuth in the United States and Canada comes as bismuth subsalicylate. | ||||||
| 2019 [18] | Korea | PPI-AMO-CLA | PPI-AMO-MET | ◎ | - | ◎ |
| PPI-AMO-MET | PPI-AMO-CLA | - | Treatment like double resistance (#) | |||
| Sequential therapy | ◎ | - | - | |||
| The doses of PPI, Amoxicillin, Clarithromycin, Metronidazole, and Bismuth are the same as stated above except for esomeprazole or omeprazole (1.5–2.5 mg/kg/d) are also mentioned. | ||||||
| TET | 500 mg QID (>12 years old, >40 kg) | |||||
| 2020 [5] | Japan | PPI-AMO-CLA | PPI-AMO-MET for 7 days | |||
| Twice daily | Maximum daily dose (mg/day) | |||||
| PPI | ||||||
| Lansoprazole | 1.5 mg/kg/day | 60 | ||||
| Omeprazole | 1.0 mg/kg/day | 40 | ||||
| Rabeprazole | 0.5 mg/kg/day | 20 | ||||
| Esomeprazole | ≥4 years old Body weight < 30 kg | 20 mg/day | 40 | |||
| Bodyweight ≥ 30 kg | 40 mg/day | |||||
| AMO | 50 mg/kg/day | 1500 | ||||
| CLA | 15–20 mg/kg/day | 800 | ||||
| MET | 10–20 mg/kg/day | 500 | ||||
| Study | Region | Study Period | Follow-Up Case Number | Past Treatment Regimen | Treatment | Eradication Rate |
|---|---|---|---|---|---|---|
| Genis et al., 2013 [47] (abstract) | Belgium | 2007 to 2011 | 25 | Sequential regimen | Tailored triple therapy for 10–14 days | 3/5 (60%) |
| Repeated sequential regimen | 13/20 (65%) | |||||
| Kallirroi et al., 2019 [48] (abstract) | Belgium | 2011 to 2018 | 52 | Not available | Sequential treatment either a triple therapy (tailored when secondary antimicrobial susceptibility was available) with duration and dosage per local treatment protocols (which were changing over time) | 35/52 (67.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, H.-H.; Lai, M.-W. Treatment of Pediatric Helicobacter pylori Infection. Antibiotics 2022, 11, 757. https://doi.org/10.3390/antibiotics11060757
Lai H-H, Lai M-W. Treatment of Pediatric Helicobacter pylori Infection. Antibiotics. 2022; 11(6):757. https://doi.org/10.3390/antibiotics11060757
Chicago/Turabian StyleLai, Hung-Hsiang, and Ming-Wei Lai. 2022. "Treatment of Pediatric Helicobacter pylori Infection" Antibiotics 11, no. 6: 757. https://doi.org/10.3390/antibiotics11060757
APA StyleLai, H.-H., & Lai, M.-W. (2022). Treatment of Pediatric Helicobacter pylori Infection. Antibiotics, 11(6), 757. https://doi.org/10.3390/antibiotics11060757