
Health Information Orientation Profiles and Their Association with Knowledge of Antibiotic Use in a Population with Good Internet Access: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling Frame
2.2. Survey Data Collection
2.3. Dependent Variable—Poor Knowledge of Antibiotic Use
2.4. Data Analysis
3. Results
3.1. Demographics of Survey Respondents
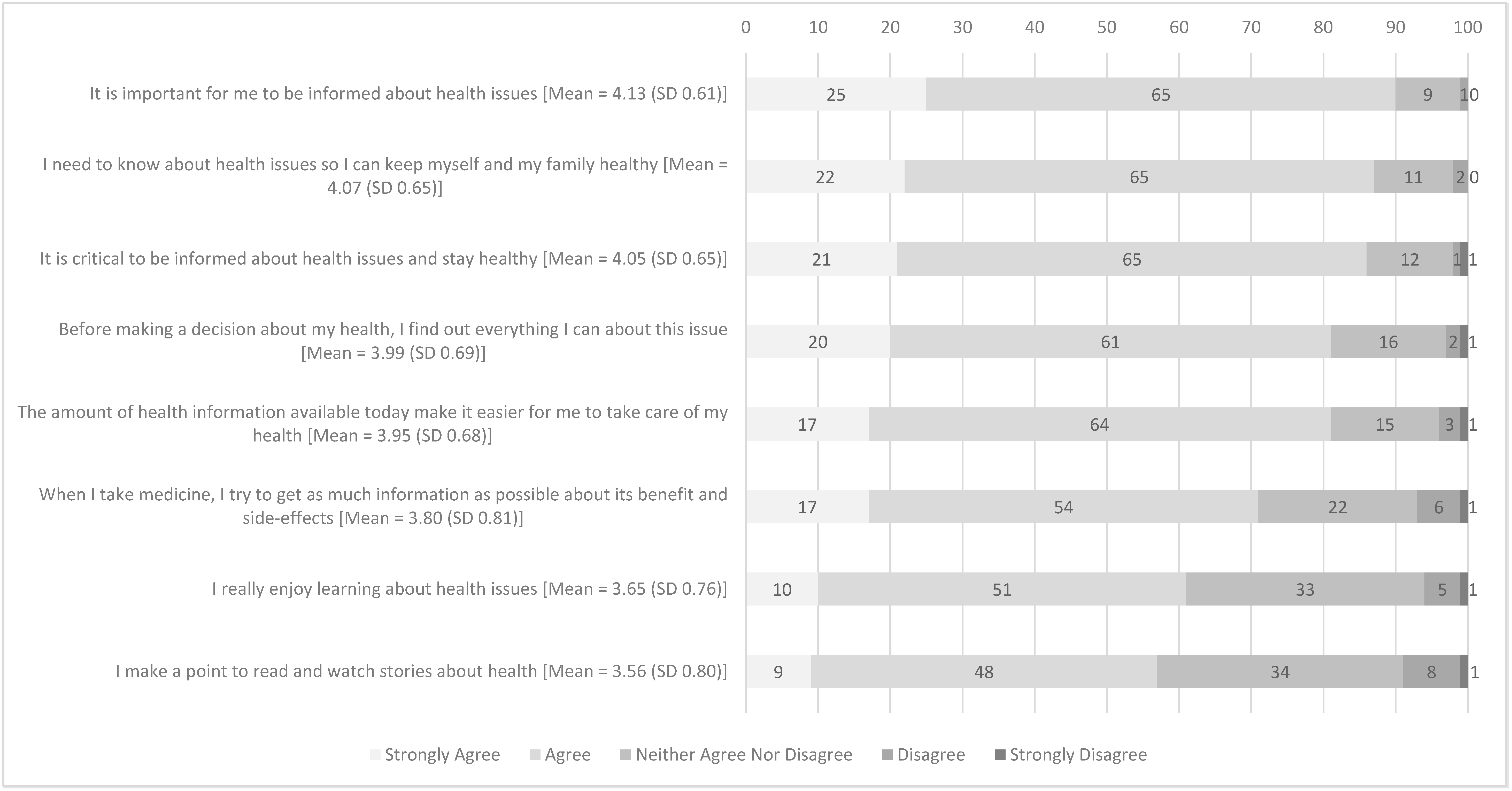
3.2. Health Information Orientation
3.3. Characteristics of Respondents with High Level of HIO vs. Low Level of HIO
3.4. Factors Associated with Poor Knowledge of Antibiotic Use
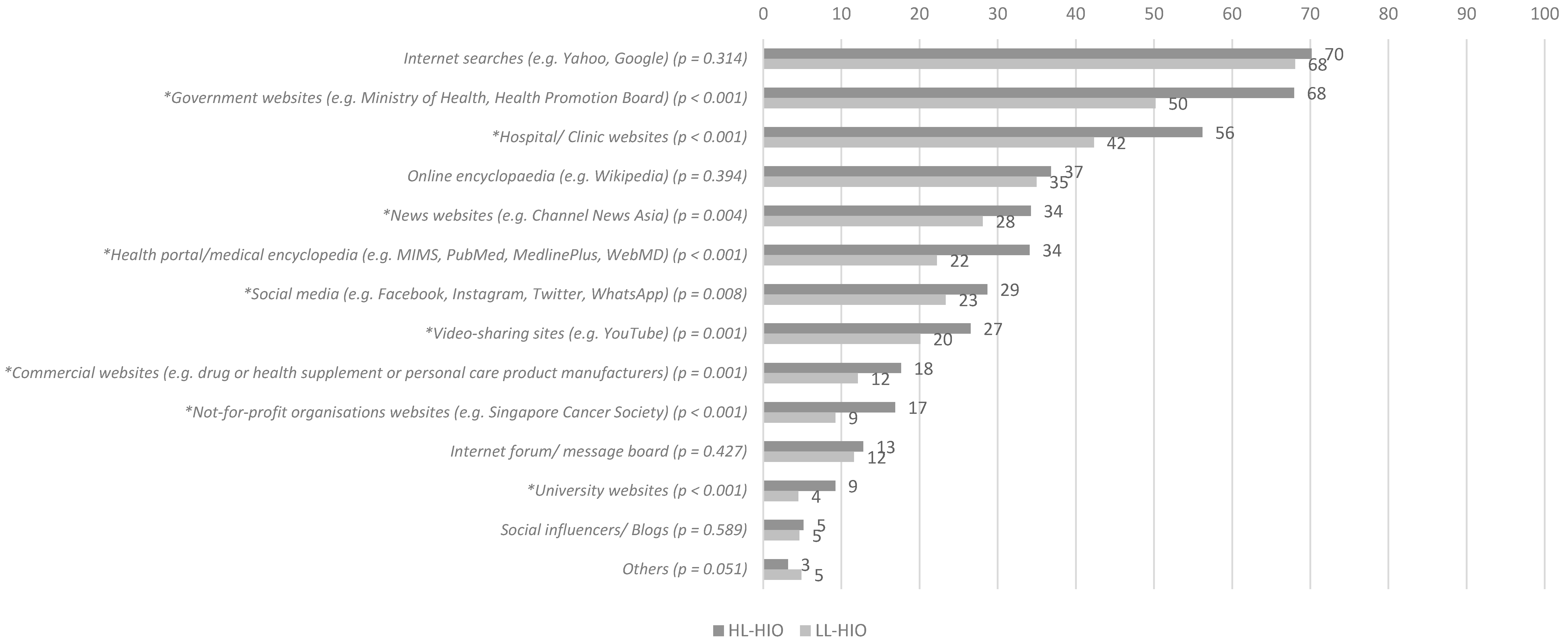
3.5. Online Health Information-Seeking Behaviours (HISBs) among Respondents with High and Low Levels of HIO
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hutching, M.; Truman, A.W.; Wilkinson, B. Antibiotics: Past, present and future. Curr. Opin. Microbiol. 2019, 51, 72–80. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 26 April 2022).
- Review on Antimicrobial Resistance. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014. Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 26 April 2022).
- Pan, D.S.T.; Huang, J.H.; Lee, M.H.M.; Yu, Y.; Chen, M.I.-C.; Goh, E.H.; Jiang, L.; Chong, J.W.C.; Leo, Y.S.; Lee, T.H.; et al. Knowledge, attitudes, and practices towards antibiotic use in upper respiratory tract infections among patients seeking primary health care in Singapore. BMC Fam. Pract. 2016, 17, 148. [Google Scholar] [CrossRef] [Green Version]
- Shaikhan, F.; Rawaf, S.; Majeed, A.; Hassounah, S. Knowledge, attitude, perception and practice regarding antimicrobial use in upper respiratory tract infections in Qatar: A systematic review. J. R. Soc. Med. 2018, 9, 2054270418774971. [Google Scholar] [CrossRef] [PubMed]
- Choo, S.J.; Chang, C.T.; Lee, J.C.-Y.; Munisamy, V.; Tan, C.K.; Raj, J.D.; Taib, R.I.M.; Thong, K.S.; A Shafie, A. A cross-sectional study on public belief, knowledge and practice towards antibiotic use in the state of Perak, Malaysia. J. Infect. Dev. Ctries. 2018, 12, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.M.; Chhoun, P.; Tuot, S.; Om, C.; Krang, S.; Ly, S.; Hsu, L.Y.; Yi, S.; Tam, C.C. Public knowledge, attitudes and practices surrounding antibiotic use and resistance in Cambodia. JAC Antimicrob. Resist. 2021, 3, dlaa115. [Google Scholar] [CrossRef] [PubMed]
- Gillani, A.H.; Chang, J.; Aslam, F.; Saeed, A.; Shukar, S.; Khanum, F.; Jairoun, A.; Nicholson, A.; Ibrahim, M.I.M.; Fang, Y. Public knowledge, attitude, and practice regarding antibiotics use in Punjab, Pakistan: A cross-sectional study. Expert Rev. Anti-Infect. Ther. 2021, 19, 399–411. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 26 April 2022).
- Mortazhejri, S.; Hong, P.J.; Yu, A.M.; Hong, B.Y.; Stacey, D.; Bhatia, R.S.; Grimshaw, J.M. Systematic review of patient-oriented interventions to reduce unnecessary use of antibiotics for upper respiratory tract infections. Syst. Rev. 2020, 9, 106. [Google Scholar] [CrossRef]
- Castro-Sánchez, E.; Chang, P.W.; Candel, R.V.; Escobedo, A.A.; Holmes, A.H. Health literacy and infectious diseases: Why does it matter? Int. J. Infect. Dis. 2016, 43, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Price, L.; Gozdzielewska, L.; Young, M.; Smith, F.; Macdonald, J.; McParland, J.; Williams, L.; Langdridge, D.; Davis, M.D.M.; Flowers, P. Effectiveness of interventions to improve the public’s antimicrobial resistance awareness and behaviours associated with prudent use of antimicrobials: A systematic review. J. Antimicrob. Chemother. 2018, 73, 1464–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.M.; Singh, S.R.; Duong, M.C.; Legido-Quigley, H.; Hsu, L.Y.; Tam, C.C. Impact of national interventions to promote responsible antibiotic use: A systematic review. J. Antimicrob. Chemother. 2020, 75, 14–29. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Hildon, Z.J.-L.; Lye, D.C.B.; Straughan, P.T.; Chow, A. The Associations between Poor Antibiotic and Antimicrobial Resistance Knowledge and Inappropriate Antibiotic Use in the General Population Are Modified by Age. Antibiotics 2022, 11, 47. [Google Scholar] [CrossRef]
- Jia, X.; Pang, Y.; Liu, L.S. Online Health Information Seeking Behavior: A Systematic Review. Healthcare 2021, 9, 1740. [Google Scholar] [CrossRef] [PubMed]
- Dutta-Bergman, M.J. Primary Sources of Health Information: Comparisons in the Domain of Health Attitudes, Health Cognitions, and Health Behaviors. Health Commun. 2004, 16, 273–288. [Google Scholar] [CrossRef]
- Dutta-Bergman, M.J. Health attitudes, health cognitions, and health behaviors among Internet health information seekers: Population-based survey. J. Med. Internet Res. 2004, 6, e15. [Google Scholar] [CrossRef]
- Sheng, X.; Simpson, P.M. Seniors, health information, and the Internet: Motivation, ability, and Internet knowledge. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 740–746. [Google Scholar] [CrossRef]
- Lee, S.T.; Dutta, M.J.; Luk, P.; Kaur-Gill, S.; Lin, J. Health Orientation as a Psychographic Framework for Understanding Physical Exercise Behavior. Health Commun. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. 2015. Available online: https://apps.who.int/iris/handle/10665/194460 (accessed on 26 April 2022).
- The University of Hong Kong. General Public’s Knowledge, Attitude and Practice Survey on Antimicrobial Resistance. 2017. Available online: http://chp.gov.hk/files/pdf/kap_on_amr_main_report.pdf (accessed on 26 April 2022).
- Jiang, S.; Street, R.L. Pathway Linking Internet Health Information Seeking to Better Health: A Moderated Mediation Study. Health Commun. 2017, 32, 1024–1031. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth literacy scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singapore Health Promotion Board. FIGHT the Spread of Infectious Diseases. 2017. Available online: https://www.healthhub.sg/programmes/52/Fight_The_Spread (accessed on 26 April 2022).
- Kim, K.; Lee, I. The Influence of Health Information Orientation, E-Health Literacy, and Anxiety on Health Behaviour among Parents with School Age Children: Focusing on MERS Prevention Behaviour. J. Nurs. Health Care 2015, 3, 2. [Google Scholar]
- Cho, J.; Park, D.; Lee, H.E. Cognitive Factors of Using Health Apps: Systematic Analysis of Relationships Among Health Consciousness, Health Information Orientation, eHealth Literacy, and Health App Use Efficacy. J. Med. Internet Res. 2014, 16, e125. [Google Scholar] [CrossRef]
- Wrzus, C.; Hänel, M.; Wagner, J.; Neyer, F.J. Social network changes and life events across the life span: A meta-analysis. Psychol. Bull. 2013, 139, 53–80. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.L. Socioemotional selectivity theory: Social activity in life-span context. Annu. Rev. Gerontol. Geriatr. 1991, 11, 195–217. [Google Scholar]
- Carstensen, L.L. Social and emotional patterns in adulthood: Support for socioemotional selectivity theory. Psychol. Aging 1992, 7, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.L. Evidence for a life-span theory of socioemotional selectivity. Curr. Dir. Psychol. Sci. 1995, 4, 151–156. [Google Scholar] [CrossRef]
- Rutgers University-Camden. Camden Barbers Become Messengers of COVID-19 Vaccine Importance, Thanks to Innovative Collaboration. 2021. Available online: https://news.camden.rutgers.edu/2021/07/camden-barbers-become-trusted-messengers-of-covid-19-vaccine-importance-thanks-to-innovative-collaboration/ (accessed on 9 May 2022).
- Eley, N.T.; Namey, E.; McKenna, K.; Johnson, A.C.; Guest, G. Beyond the Individual: Social and Cultural Influences on the Health-Seeking Behaviours of African American Men. Am. J. Mens Health 2019, 13, 1557988319829953. [Google Scholar] [CrossRef] [Green Version]
- Victor, R.G.; Lynch, K.; Li, N.; Blyler, C.; Muhammad, E.; Handler, J.; Brettler, J.; Rashid, M.; Hsu, B.; Foxx-Drew, D.; et al. A Cluster-Randomized Trial of Blood-Pressure Reduction in Black Barbershops. N. Engl. J. Med. 2018, 378, 1291–1301. [Google Scholar] [CrossRef]
- Berglund, E.; Lytsy, P.; Westerling, R. Living environment, social support, and informal caregiving are associated with healthcare seeking behaviour and adherence to medication treatment: A cross-sectional population study. Health Soc. Care Community 2019, 27, 1260–1270. [Google Scholar] [CrossRef]
- Parveen, S.; Garzon-Orjuela, N.; Amin, D.; McHugh, P.; Vellinga, A. Public Health Interventions to Improve Antimicrobial Resistance Awareness and Behavioural Change Associated with Antimicrobial Use: A Systematic Review Exploring the Use of Social Media. Antibiotics 2022, 11, 669. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Dutta, M.J. The Relationship Between Health Information Seeking and Community Participation: The Roles of Health Information Orientation and Efficacy. Health Commun. 2008, 21, 70–79. [Google Scholar] [CrossRef]
- Van Rijn, M.; Haverkate, M.; Achterberg, P.; Timen, A. The public uptake of information about antibiotic resistance in the Netherlands. Public Underst. Sci. 2019, 28, 486–503. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Hildon, Z.J.-L.; Loh, V.W.K.; Sundram, M.; Bin Ibrahim, M.A.; Tang, W.E.; Chow, A. Exploring antibiotic prescribing in public and private primary care settings in Singapore: A qualitative analysis informing theory and evidence-based planning for value-driven intervention design. BMC Fam. Pract. 2021, 22, 205. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Survey Respondents, % | Singapore Residents in Census 2020 a, % |
|---|---|---|
| Residency Status, N(%) | ||
| Singapore Citizen | 87 | 86 |
| Permanent Resident | 13 | 14 |
| Age, N(%) | ||
| 21–34 years old | 31 | 26 |
| 35–49 years old | 33 | 28 |
| ≥50 years old | 36 | 46 |
| Gender, N(%) | ||
| Male | 48 | 48 |
| Female | 52 | 52 |
| Race, N(%) | ||
| Chinese | 72 | 76 |
| Non-Chinese | 28 | 24 |
| Highest Educational Level, N(%) | ||
| Lower Educated (Post-Secondary and Below) | 35 | 51 |
| Higher Educated (Diploma and Above) | 65 | 49 |
| Marital Status, N(%) | ||
| Currently Married | 62 | 63 |
| Currently Not Married | 38 | 37 |
| Employment Status, N(%) | ||
| Currently Employed | 70 | NA |
| Currently Not Employed | 30 | NA |
| Self-Reported Influence of Religion on Health-Seeking Behaviour, N(%) | ||
| Yes | 27 | NA |
| Have Family Members or Friends Working in Healthcare Sector, N(%) | ||
| Yes | 54 | NA |
| Have At Least One Chronic Disease, N(%) | ||
| Yes | 32 | NA |
| Self-Reported Health Rating, N(%) | ||
| Below Average | 3 | NA |
| Average | 33 | NA |
| Above Average | 65 | NA |
| Adoption of Healthy Lifestyle, N(%) | ||
| High | 16 | NA |
| Low | 84 | NA |
| Continuity of Care with a Regular Doctor, N(%) | ||
| Yes | 62 | NA |
| Adherence to Infection Prevention Measures, N(%) | ||
| High | 18 | NA |
| Low | 83 | NA |
| Characteristics | High Level of Health Information Orientation (N = 1203) | Low Level of Health Information Orientation (N = 801) | p-Value * |
|---|---|---|---|
| Residency Status, N(%) | |||
| Singapore Citizen | 1048 (87) | 690 (86) | 0.529 |
| Permanent Resident | 155 (13) | 111 (14) | |
| Age, N(%) | |||
| 21–34 years old | 334 (28) | 281 (35) | 0.001 |
| 35–49 years old | 402 (33) | 256 (32) | |
| ≥50 years old | 467 (39) | 264 (33) | |
| Gender, N(%) | |||
| Male | 558 (46) | 396 (49) | 0.180 |
| Female | 645 (54) | 405 (51) | |
| Race, N(%) | |||
| Chinese | 838 (70) | 600 (75) | 0.011 |
| Non-Chinese | 365 (30) | 201 (25) | |
| Highest Educational Level, N(%) | |||
| Lower Educated (Post-Secondary and Below) | 418 (35) | 278 (35) | 0.985 |
| Higher Educated (Diploma and Above) | 785 (65) | 523 (65) | |
| Marital Status, N(%) | |||
| Currently Married | 790 (66) | 462 (58) | <0.001 |
| Currently Not Married | 413 (34) | 339 (42) | |
| Employment Status, N(%) | |||
| Currently Employed | 372 (31) | 228 (28) | 0.239 |
| Currently Not Employed | 831 (69) | 573 (72) | |
| Self-Reported Influence of Religion on Health-Seeking Behaviour, N(%) | |||
| Yes | 363 (30) | 176 (22) | <0.001 |
| Have Family Members or Friends Working in Healthcare Sector, N(%) | |||
| Yes | 702 (58) | 374 (47) | <0.001 |
| Have At Least One Chronic Disease, N(%) | |||
| Yes | 404 (34) | 244 (30) | 0.143 |
| Self-Reported Health Rating, N(%) | |||
| Below Average | 30 (2) | 20 (3) | <0.001 |
| Average | 342 (28) | 319 (40) | |
| Above Average | 831 (69) | 462 (58) | |
| Adoption of Healthy Lifestyle, N(%) | |||
| High | 245 (20) | 85 (11) | <0.001 |
| Low | 958 (80) | 716 (89) | |
| Continuity of Care with a Regular Doctor, N(%) | |||
| Yes | 784 (65) | 449 (56) | <0.001 |
| Adherence to Infection Prevention Measures, N(%) | |||
| High | 247 (21) | 106 (13) | <0.001 |
| Low | 956 (79) | 965 (87) | |
| Variables | Good Knowledge of Antibiotic Use (N = 1188) | Poor Knowledge of Antibiotic Use (N = 816) | p-Value * | Univariate Analysis (N = 2004) | Model 1: without Interaction Terms (N = 2004) | Model 2: with Interaction Terms (N = 2004) | |||
|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value * | Adjusted Odds Ratio (95% CI) | p-Value * | Adjusted Odds Ratio (95% CI) | p-Value * | ||||
| Level of Health Information Orientation, N(%) | |||||||||
| Low | 438 (37) | 363 (44) | 0.001 | 1.37 (1.14–1.65) | 0.001 | 1.36 (1.12–1.65) | 0.002 | 1.82 (1.32–2.51) | <0.001 |
| High Adherence to Infection Prevention Measures, N(%) | |||||||||
| Yes | 191 (16) | 162 (20) | 0.029 | 1.29 (1.03–1.63) | 0.030 | 1.22 (0.96–1.56) | 0.109 | 1.21 (0.95–1.55) | 0.123 |
| Residency Status, N(%) | |||||||||
| Permanent Resident | 172 (14) | 94 (12) | 0.055 | Ref | - | - | - | - | - |
| Singapore Citizen | 1016 (86) | 722 (88) | 1.30 (0.99–1.70) | 0.056 | - | - | - | - | |
| Age, N(%) | |||||||||
| ≥50 years old | 446 (38) | 285 (35) | 0.001 | Ref | - | Ref | - | Ref | - |
| 35–49 years old | 416 (35) | 242 (30) | 0.91 (0.73–1.13) | 0.397 | 1.08 (0.85–1.37) | 0.535 | 1.27 (0.94–1.72) | 0.124 | |
| 21–34 years old | 326 (27) | 289 (35) | 1.39 (1.12–1.72) | 0.003 | 1.47 (1.12–1.92) | 0.006 | 1.80 (1.29–2.52) | 0.001 | |
| Gender, N(%) | |||||||||
| Male | 529 (45) | 425 (52) | 0.001 | 1.35 (1.13–1.62) | 0.001 | 1.36 (1.13–1.64) | 0.001 | 0.90 (0.56–1.44) | 0.651 |
| Race, N(%) | |||||||||
| Non-Chinese | 267 (22) | 299 (37) | <0.001 | 1.99 (1.64–2.43) | <0.001 | 1.77 (1.43–2.20) | <0.001 | 1.76 (1.42–2.19) | <0.001 |
| Highest Educational Level, N(%) | |||||||||
| Higher Educated (Diploma and Above) | 838 (71) | 470 (58) | <0.001 | Ref | - | Ref | - | Ref | - |
| Lower Educated (Post-Secondary and Below) | 350 (29) | 346 (42) | 1.76 (1.46–2.12) | <0.001 | 1.90 (1.53–2.36) | <0.001 | 1.86 (1.50–2.31) | <0.001 | |
| Employment Status, N(%) | |||||||||
| Currently Not Employed | 344 (29) | 256 (31) | 0.246 | 1.12 (0.92–1.36) | 0.246 | - | - | - | - |
| Marital Status, N(%) | |||||||||
| Currently Not Married | 409 (34) | 343 (42) | 0.001 | 1.38 (1.15–1.66) | 0.001 | 1.28 (1.05–1.58) | 0.017 | 1.28 (1.04–1.57) | 0.019 |
| Self-Reported Influence of Religion on Health-Seeking Behaviour, N(%) | |||||||||
| Yes | 293 (25) | 246 (30) | 0.007 | 1.32 (1.08–1.61) | 0.007 | 1.20 (0.97–1.49) | 0.100 | 1.03 (0.79–1.35) | 0.814 |
| Have Family Members or Friends Working in Healthcare Sector, N(%) | |||||||||
| No | 531 (45) | 397 (49) | 0.081 | 1.17 (0.98–1.40) | 0.081 | - | - | - | - |
| Have At Least One Chronic Disease, N(%) | |||||||||
| Yes | 381 (32) | 267 (33) | 0.760 | 1.03 (0.85–1.25) | 0.760 | - | - | - | - |
| Self-Reported Health Rating, N(%) | |||||||||
| Below Average | 36 (3) | 14 (2) | 0.170 | Ref | - | - | - | - | - |
| Average | 393 (33) | 268 (33) | 1.75 (0.93–3.31) | 0.084 | - | - | - | - | |
| Above Average | 759 (64) | 534 (65) | 1.81 (0.97–3.39) | 0.064 | - | - | - | - | |
| Adoption of Healthy Lifestyle, N(%) | |||||||||
| Low | 973 (82) | 701 (86) | 0.018 | 1.35 (1.05–1.72) | 0.018 | 1.09 (0.84–1.41) | 0.516 | 0.90 (0.56–1.44) | 0.414 |
| Continuity of Care with a Regular Doctor, N(%) | |||||||||
| No | 418 (35) | 353 (43) | <0.001 | 1.40 (1.17–1.69) | <0.001 | 1.32 (1.09–1.61) | 0.005 | 1.17 (0.93–1.46) | 0.171 |
| Interaction between Health Information Orientation and Age | |||||||||
| Low health information orientation and 35–49 years old | - | - | - | 0.63 (0.40–0.99) | 0.044 | - | - | 0.67 (0.42–1.06) | 0.084 |
| Low health information orientation and 21–34 years old | - | - | - | 0.58 (0.37–0.91) | 0.016 | - | - | 0.61 (0.39–0.97) | 0.035 |
| Interaction between Adoption of Healthy Lifestyle and Gender | |||||||||
| Low adoption of healthy lifestyle and male gender | - | - | - | 1.72 (1.05–2.82) | 0.033 | - | - | 1.62 (0.97–2.70) | 0.067 |
| Interaction between Continuity of Care with a Regular Doctor and Self-Reported Influence of Religion on Health-Seeking Behaviour | |||||||||
| Lack of continuity of care with a regular doctor and self-reported influence of religion on health-seeking behaviour | - | - | - | 1.87 (1.22–2.86) | 0.004 | - | - | 1.61 (1.04–2.51) | 0.034 |
| Poor Knowledge of Antibiotic Use | ≥50 Years Old(N = 731) | 35–49 Years Old(N = 658) | 21–34 Years Old(N = 615) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Interaction a,* | OR | 95% CI | p-Interaction a | OR | 95% CI | p-Interaction a | |
| Unadjusted analysis | |||||||||
| High health information orientation | Ref | - | <0.001 | Ref | - | 0.332 | Ref | - | 0.632 |
| Low health information orientation | 1.86 | 1.37–2.53 | 1.17 | 0.85–1.62 | 1.08 | 0.79–1.49 | |||
| Adjusted analysis b | |||||||||
| High health information orientation | Ref | - | <0.001 | Ref | - | 0.265 | Ref | - | 0.534 |
| Low health information orientation | 1.81 | 1.32–2.51 | 1.21 | 0.87–1.69 | 1.11 | 0.80–1.55 | |||
| Poor Knowledge of Antibiotic Use | Lack of Self-Reported Influence of Religion on Health-Seeking Behaviour(N = 539) | Presence of Self-Reported Influence of Religion on Health-Seeking Behaviour(N = 1465) | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Interaction a | OR | 95% CI | p-Interaction a,* | |
| Unadjusted analysis | ||||||
| With continuity of care with a regular doctor | Ref | - | 0.065 | Ref | - | <0.001 |
| Without continuity of care with a regular doctor | 1.22 | 0.99–1.51 | 2.29 | 1.58–3.30 | ||
| Adjusted analysis b | ||||||
| With continuity of care with a regular doctor | Ref | - | 0.171 | Ref | - | 0.001 |
| Without continuity of care with a regular doctor | 1.17 | 0.93–1.46 | 1.89 | 1.28–2.77 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, H.; Lim, H.Y.; Chow, A. Health Information Orientation Profiles and Their Association with Knowledge of Antibiotic Use in a Population with Good Internet Access: A Cross-Sectional Study. Antibiotics 2022, 11, 769. https://doi.org/10.3390/antibiotics11060769
Guo H, Lim HY, Chow A. Health Information Orientation Profiles and Their Association with Knowledge of Antibiotic Use in a Population with Good Internet Access: A Cross-Sectional Study. Antibiotics. 2022; 11(6):769. https://doi.org/10.3390/antibiotics11060769
Chicago/Turabian StyleGuo, Huiling, Huai Yang Lim, and Angela Chow. 2022. "Health Information Orientation Profiles and Their Association with Knowledge of Antibiotic Use in a Population with Good Internet Access: A Cross-Sectional Study" Antibiotics 11, no. 6: 769. https://doi.org/10.3390/antibiotics11060769
APA StyleGuo, H., Lim, H. Y., & Chow, A. (2022). Health Information Orientation Profiles and Their Association with Knowledge of Antibiotic Use in a Population with Good Internet Access: A Cross-Sectional Study. Antibiotics, 11(6), 769. https://doi.org/10.3390/antibiotics11060769