Abstract
Background: The presence of extended-spectrum β-lactamase (ESBL)-producing bacteria among uropathogens is significantly increasing in children all over the world. Thus, this research was conducted to investigate the prevalence of E. coli and their antimicrobial susceptibility pattern, and both genes of ESBL-producing E. coli resistant and virulence factor in UTIs patients among children in Duhok Province, Kurdistan, Iraq. Method: a total of 67 E. coli were identified from 260 urine samples of pediatric patients diagnosed with UTIs aged (0–15 years) which were collected from Heevi Pediatric Teaching Hospital, from August 2021 to the end of February 2022. Result: a high proportion of UPEC infections at ages <5 years and the rates among girls (88%) were significantly higher than those among the boys. A wide variety of E. coli are resistant to most antibiotics, such as Amoxicillin, Ampicillin and Tetracycline, and 64% of them were positive for ESBL. Interestingly, the presence of both the ESBL marker genes (blaTEM, and blaCTX-M) as well as both virulence marker genes (pai and hly) were detected in above 90% of E. coli. Conclusion: the data illustrate an alarming increase in UPEC with ESBL production and the emergence of multidrug-resistant drugs in the early age of children. The public health sectors should further monitor the guidelines of using antibiotics in Kurdistan, Iraq.
1. Introduction
Urinary tract infections (UTIs) are the most common severe bacterial infections seen in clinical settings worldwide [1,2]. It is estimated that annually there are over 150 million occurrences of UTIs, which are medically expensive [3,4]. On yearly basis, the total healthcare cost of UTIs in the USA, whether for its management or treatment, is over 3.5 billion USD [5], and around 630 million USD for pediatrics UTIs [6]. Pediatric UTIs are estimated to impact 2.4 to 3 % of all American children each year, resulting in more than 1.5 million doctor visits [7], of which 5–14% are dedicated to emergency visits [8]. The incidence of UTIs is common during childhood, and affects in both boys and girls equally during the first year of life [9]. UTIs are considered the second most frequent bacterial infection in children throughout the first seven years of life, and girls account for the majority of infections, approximately 8.4% and less than 1.7% for boys [10,11,12].
It is known that Escherichia coli (E. coli) is the most prevalent bacterial pathogen that causes UTIs and is responsible for 80% of UTIs that occur in children [13]. Numerous virulence factors, such as adhesins, toxins, and siderophores, are present in uropathogenic Escherichia coli (UPEC) strains and contribute to the spread of infection [14,15]. The ability of bacteria to adhere to the host cells in the urinary system and prevent quick clearance by the bulk flow of urine is one of the most crucial virulence factors [16]. The most significant virulence component released by uropathogenic E. coli is a lipoprotein known as α-hemolysin (hlyA), which is connected to higher UTIs that result in pyelonephritis [17]. In addition, E. coli that has colonized the body may produce toxins that create an inflammatory reaction, which is one potential cause of the symptoms of UTIs [18].
The majority of enzymes that can break down penicillins, third-generation cephalosporins, and monobactams are known as extended-spectrum β-lactamases (ESBLs) [19]. Because antibiotics hydrolyzed the β-lactam ring and bound covalently to their carbonyl moiety, they were ineffective as a therapy [20]. There are very few antibiotic choices for treating a bacterium that generates ESBL. For serious infections caused by ESBL-producing organisms, carbapenems are the drug of choice [21]. However, studies reported that carbapenem-resistant isolates do exist [21,22].
The prevalence of ESBL in Enterobacteriaceae with UTIs patients is increasing and has become a significant cause of morbidity and a major problem all over the world [23]. The World Health Organization declared in 2021 [24] that the category of Enterobacteriaceae that produce ESBL offers the greatest danger of infection to the health of the global population. One of the most prevalent bacteria carrying ESBL genes is E. coli, which belongs to the Enterobacteriaceae family. Due to its rapid growth, this bacterium represents a threat to both sexes in the community at different phases of life [25,26].
It has been reported that the prevalence of E. coli with ESBL in UTIs varies greatly between different nations [27,28,29,30,31]. In the Kurdistan Region, Iraq, several studies have been conducted on the prevalence of UTIs among adults [32,33,34] and reporting the antibiotics susceptibility test only in children [35,36,37]. Therefore, this study is undertaken to identify ESBL-producing E. coli, to detect their ESBL resistant marker genes and five virulence factors marker genes, and to determine their antimicrobial susceptibility pattern among children in Duhok Province, Kurdistan Region, Iraq.
2. Results
2.1. E. coli Isolation with Phenotypic and Genotypic Detection
In this current study, a total of 260 out- and in-patient children (<15 years) were recruited, from August 2021 and February 2022. From these cultures, 150 (57.7%) were phylogenetic positive bacterial cultures. From 150 samples, E. coli was the predominant pathogenic bacteria, and 67 (44.7%) of them were confirmed phenotypically and molecularly by the species-specific gene (uidA). Phenotypically, E. coli was identified on MacConkey and EMB agars as well as Gram stain and biochemical tests (Oxidas, IMViC, TSI). In addition, all isolated E. coli were genotypically confirmed by the species-specific gene (uidA) (Figure 1a).
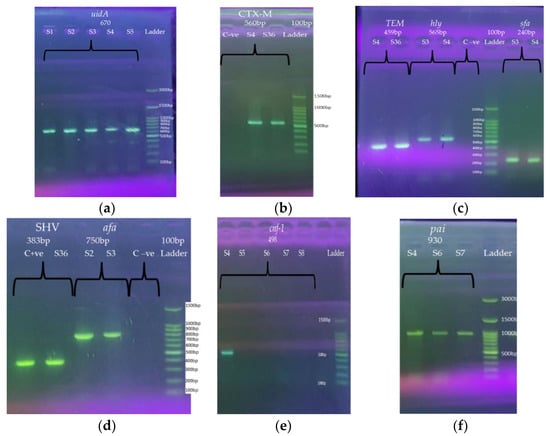
Figure 1.
Gel electrophoresis of PCR products for E. coli-specific primers uidA (a) marker genes (blaTEM, blaCTX-M, and blaSHV) (b–d) and five virulence factors marker genes (pai, hly, cnf-1, sfa and afa) (c–f). The amplified DNA fragments produce of various E. coli strains with these marker primers: species-specific primer uidA (lanes 1–5 for strains 1–5) (a), CTX-M (lanes 1, 2 and 3 for control negative and strains 4 and 36, respectively) (b), TEM (lanes 1 and 2 for strains 4 and 36), hly (lanes 3 and 4 for strains 3 and 4 and lane 5 for control negative), and sfa (lanes 7 and 8, for strains 3 and 4) (c), SHV (lanes 1 and 2, for strains control positive and S36), afa (lanes 3 and 4, for strains 2 and 3) (d), cnf-1 (lanes 1, 2, 3, 4, 5 and 6 for strains 4, 5, 6, 7, 8 and control-ve) (e), and pai (lanes 1, 2, and 3, for strains 4, 6 and 7) (f), and lane 100 bp Ladder (GDSBio Marker) (b–e) and 300 bp (GeneDireX, Marker) as shown in (a,f). A 7 µL of the PCR products and ladder were pipetted into a prepared 1.5% agarose gel stained with 5 µL of Safe Gel Stain Dye. Key: pai; pathogenicity island; hly; hemolysin, sfa; S-fimbrial adhesion, cnf-1; cytotoxic necrotizing factor-1, and afa; a fimbrial adhesion and S = strain.
2.2. Antimicrobial Susceptibility Pattern
All the isolated E. coli underwent an antimicrobial susceptibility test, and the results of the 19 antibiotics and their percentage (yellow colors) are shown in Figure 2. Isolated E. coli were resistant to Tetracycline around (97%) and approximately 85% of them were highly resistant to Amoxicillin and Ampicillin. Furthermore, around 70% of isolated E. coli were resistant to Nalidixic acid, Cefotaxime, Cefixime, Trimethoprim/ Sulfamethoxazole, Gentamicin and Ceftriaxone. In addition, around (57%) of these E. coli were resistant to Amikacin, (51%) to Ciprofloxacin and (45%) to Aztreonam. In contrast, over 85% of E. coli were highly susceptible to Chloramphenicol, Nitrofurantoin and Imipenem.
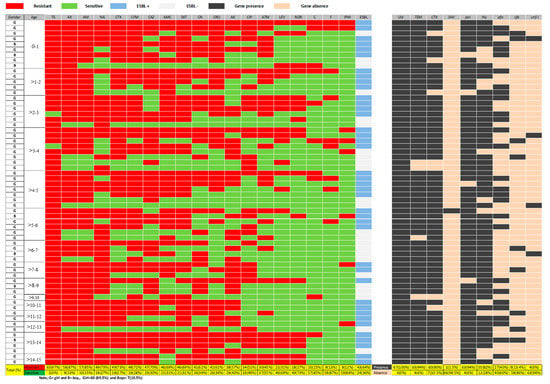
Figure 2.
The prevalence of isolated E. coli and details of each strain for antibiotic resistance profiles and genes of both ESBL production and virulence factor. The red color of cells indicates that E. coli strains are resistant to antibiotics while the green color refers to E. coli strains that are sensitive to antibiotics. Furthermore, the blue color cells indicate that E. coli are ESBL producers by the DDST, whereas the white-darker color cells are for non-ESBL producer E. coli. Moreover, the black color cells indicate that E. coli strains have the marker genes while orange colors refer to E. coli strains which do not possess the marker. In addition, the yellow colors refer to the total and percentage for these above parameters. Each cell is for the individual bacteria. Keys: antibiotics include; TE: Tetracycline, AK: Amikacin, CAZ: Ceftazidime, AX: Amoxicillin, CTX: Cefotaxime, F: Nitrofurantoin, CN: Gentamicin, IPM: Imipenem, AM: Ampicillin, SXT: Trimethoprim/Sulphamethoxazole, CIP: Ciprofloxacin, LEV: Levofloxacin, AMC: Amoxicillin/Clavulanic acid, ATM: Aztreonam, CRO: Ceftriaxone, C: Chloramphenicol, CFM: Cefixime, NOR: Norfloxacin, NA: Nalidixic acid, and ESBL: ESBL-producing E. coli. Gene markers include pai: pathogenicity island, hly: hemolysin, sfa: S-fimbrial adhesion, cnf-1: cytotoxic necrotizing factor-1, and afa: a fimbrial adhesion, and β-lactamase genes: blaCTX-M, blaTEM and blaSHV.
2.3. Phenotypic and Molecular Detection of ESBL Production
All E. coli were subjected to detect the presence of the production of ESBLs by the double disc synergy test (DDST), shown in Figure 2 and Appendix A. The results show that 43 (64%) of E. coli were positive for ESBLs production by DDST. They were also tested for whether they were harboring ESBL genes or not by PCR amplifications as shown in Figure 1. Figure 2 presents individual and collective detecting of marker genes. The fragments which produced ESBL genes include TEM, CTX-M, and SHV, confirmed by agarose gels (Figure 1). Among the ESBL marker genes, TEM and CTX-M were more abundant 63 (94%) and 60 (90%), respectively, and the SHV had the lowest abundance of 1 (1.4%). It is interesting to note that only 3 out of the already-decided 24 non-producer ESBLs E. coli turned out to be non-ESBL, the rest were ESBL (Figure 2). Table 1 illustrates the presence of these ESBL marker genes in all of the isolated E. coli strains and 58 of the isolated strains harboring both TEM and CTX-M genes. Furthermore, the TEM gene was found in the four of the E. coli strains while only one strain harbored three TEM, CTX-M, SHV genes and another strain has only the CTX-M gene.

Table 1.
Representation of the antibiotic resistance of ESBL-producing E. coli and the virulence gene distribution pattern among of isolates UPEC.
2.4. Molecular Detection of Virulence Factors Genes
The isolated E. coli strains were also tested for the presence of the five virulence factor genes and their PCR product size on agarose gels, and these are shown in Figure 1. The total number and prevalence rate of the five virulence factor genes in E. coli isolates are also shown in Figure 2 and Appendix A. Of the 67 E. coli isolates, 63 (94%), 55 (82%), 27 (40%) 9 (13%) and 4 (6%) of isolates possess pathogenicity island (pai), hemolysin (hly), a fimbrial adhesion (afa), S-fimbrial adhesion (sfa), and cytotoxic necrotizing factor-1 (cnf-1), respectively. Table 1 illustrates the details of virulence factor genes that existed in all of the isolated E. coli strains. The main point of interest is that 21 of the isolated E. coli strains had both pai and hly genes, and 18 strains had three genes, pai, hly and afa. Furthermore, five strains possess three genes, pai, hly, and sfa and, the other five strains possess both pai, and afa. Moreover, two of these E. coli strains possess pai, hly, afa and sfa, one possesses pai, hly, sfa and cnf-1, two possess hly and afa, three possess pai, hly and cnf-1, one possesses pai and sfa, five possess pai, and one possesses hly and afa.
2.5. Relationship between UTIs by E. coli and Children Age
The total number of children with UTIs is overwhelming, at earlier ages than the pre- and school aged children. The Spearman’s correlation coefficient indicates that there was a significant negative correlation between the UTIs with UPEC and age of children; (r = −0.830, p-value = 0.0003) (Figure 3).
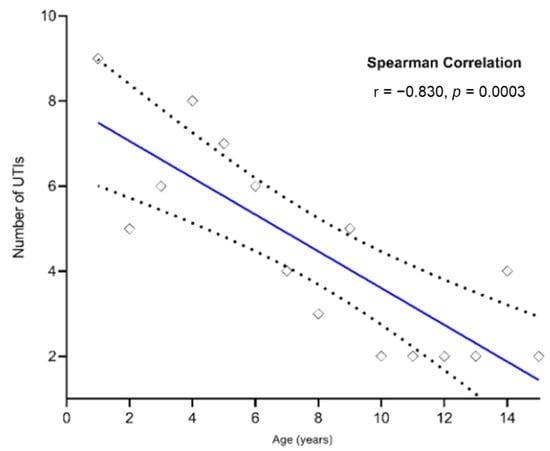
Figure 3.
Correlation analysis between the children of all ages and UTIs by UPEC. The correlation analysis indicates that the number of UTIs reduces with children’s age, and hence this figure uses a number so that the relationship is evident across ages from 0 to 15 years. Each marker denotes a sum observation of UTIs for a particular age of the children. Spearman’s correlation was performed by GraphPad Prism, and significance was considered to be established when p < 0.05.
2.6. Relationship between Antibiotic Resistance and Marker Genes of E. coli and Children Ages Having UTIs
Figure 4 illustrates the total number of antibiotics resisted and the marker genes (i.e., antibiotics resistance and virulence factors) of E. coli, in pediatric patients of all ages. It highlights the fact that they are significantly higher in early ages than pre- and school age groups. Figure 4a shows the Spearman’s correlation coefficient, indicating that there was a significant negative correlation between the children of all ages and UPEC resistant to antibiotics. The findings of the significant relationships are as follows: Tetracycline (TE; r = −0.8156, p-value = 0.0004), Amoxicillin (AX; r = −0.8266, p-value = 0.0003), Ampicillin (AM; r = −0.8266, p-value = 0.0003), Nalidixic acid (NA; r = −0.5399, p-value = 0.0404), Nitrofurantoin (F; r = −0.5399, p-value = 0.0404), Cefotaxime (CTX; r = −0.665, p-value = 0.0084), Cefixime (CFM; r = −0.7456, p-value = 0.002), Trimethoprim/Sulphamethoxazole (SXT; r = −0.629, p-value = 0.0138), Amoxicillin/Clavulanic acid (AMC; r = −0.7961, p-value = 0.0007), Ceftazidime (CAZ; r = −0.6443, p-value = 0.0112), Ceftriaxone (CRO; r = −0.5617, p-value = 0.0316), Amikacin (AK; r = −0.63, p-value = 0.0137), Aztreonam (ATM; r = −0.6228, p-value = 0.0151), Chloramphenicol (C; r = −0.5838, p-value = 0.0251), and F (r = −0.8295, p-value = 0.0003). In addition, a similar trend (although statistically not so significant) was observed in the other antibiotics; Gentamicin (CN; r = −0.3393, p-value = 0.2145), Ciprofloxacin (CIP; r = −0.4155, p-value = 0.1242), Levofloxacin (LEV; r = −0.2894, p-value = 0.2924), Norfloxacin (NOR; r = −0.2337, p-value = 0.398) and Imipenem (IPM; r = −0.3334, p-value = 0.2239). In addition, there was a significant negative correlation between the ESBL-producing E. coli and the age of children (ESBL; r = −0.5624, p-value = 0.0313) (Figure 3).
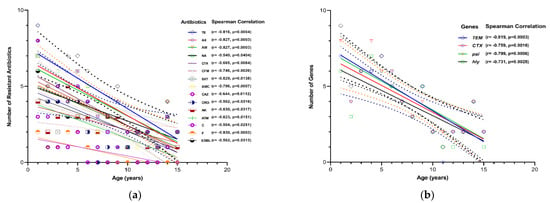
Figure 4.
Correlation analysis between the children of all ages and antibiotic resistance to (a) and both the marker genes of ESBL-producing and virulence factors (b) of UPEC infection. This figure depicts the relationship between the antibiotic resistance to UPEC and the age of the children, where antibiotic resistance and gene markers for UPEC are illustrated in number terms. Each marker denotes a specific observation for antibiotics resistance and the age (years) of a particular child. This figure depicts the relationship between the UTIs with UPEC and the age of children, where UTIs are illustrated in number terms. Spearman’s correlation was performed by GraphPad Prism and a significance was considered to be established when p < 0.05. Spearman’s correlation method was carried out by GraphPad Prism, and significance was considered to be established when p < 0.05. Keys: TE: Tetracycline, AK: Amikacin, CAZ: Ceftazidime, AX: Amoxicillin, CTX: Cefotaxime, F: Nitrofurantoin, AM: Ampicillin, SXT: Trimethoprim/Sulphamethoxazole, AMC: Amoxicillin/Clavulanic acid, ATM: Aztreonam, CRO: Ceftriaxone, C: Chloramphenicol, CFM: Cefixime, NA: Nalidixic acid, and ESBL: ESBL-producing E. coli. Gene markers include pai: pathogenicity island, hly: hemolysin.
Furthermore, the Spearman’s correlation coefficient which indicated there was a significant negative correlation between the children’s age and both marker genes of ESBL-producing and virulence factors of UPEC infection (Figure 4b). The findings of the significant relationship are as follows: TEM (r = −0.8189, p-value = 0.0003), CTX (r = −0.7594, p-value = 0.0016), pai (r = −0.7986, p-value = 0.0006) and hly (r = −0.7311, p-value = 0.0028). In addition, a similar trend (although statistically not so significant) was observed in the other marker genes, SHV (r = −0.1237, p-value = 0.8), afa (r = −0.4368, p-value = 0.1077), sfa (r = −0.04953, p-value = 0.8617) and cnf-1 (r = −0.5234, p-value = 0.0557).
2.7. Relationship between Antibiotics Resistance and Virulence Factors Genes
Figure 5 illustrates the relationship between the antibiotic-resistant genes and virulence factors of UPEC infection, using Spearman’s correlation coefficient. There were highly significant positive correlations between TEM and CTX (r = 0.98, p-value < 0.0001), pai (r = 0.96, p-value < 0.0001) and hly (r = 0.94, p-value < 0.0001), and also between CTX, and pai (r = 0.96, p-value < 0.0001) and hly (r = 0.95, p-value < 0.0001). Furthermore, despite the very low prevalence of cnf-1, it was also found that cnf-1 was a significant positive correlation with TEM (r = 0.60, p-value = 0.023), CTX (r = 0.60, p-value = 0.021), pai (r = 0.63, p-value = 0.016), and hly (r = 0.62, p-value = 0.018).
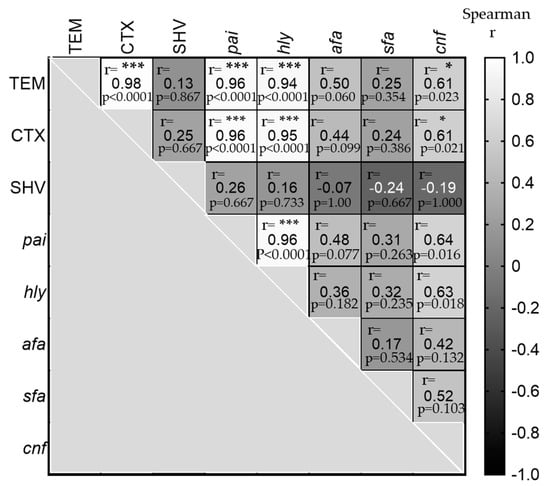
Figure 5.
Correlation analysis among the antibiotic-resistant genes with virulence factors of UPEC infection. The heatmap shows the relationship among the antibiotic-resistant genes and virulence factors of UPEC infection, using computed nonparametric Spearman correlation. The white cells are highly positively correlated between these genes, r > 0.90 and significance were considered when the p-value was <0.0001 (***). At the same time, the light gray colors are moderate positively correlated, with r between 0.60–065 and a p-value < 0.05 (*). On the other hand, the darker gray cells are not significant found. Keys: Gene markers include pai: pathogenicity island, hly: hemolysin, sfa: S-fimbrial adhesion, cnf-1: cytotoxic necrotizing factor-1, and afa: a fimbrial adhesion.
3. Discussion
The incidence of pediatric UTIs has increased dramatically in recent years worldwide, which is caused by a variety of pathogens, particularly Gram-negative bacteria. This study revealed that E. coli was the predominant uropathogen in children in our community, where the prevalence of the infected girls was higher than in boys. These findings were in agreement with the recent results obtained by several studies in Iraq, in Duhok city [35], Erbil city [36,37], and Baghdad city [38], as well as a Child Cohort Study in Taiwan with UTIs between 2004 and 2018 [39]. In fact, there are many factors that can affect the interpretation of UTIs in girls, particularly E. coli. Among these factors are the anatomical structure of the urogenital system, and girls have a shorter distance between the urethral and anal opening [40]. It has been previously suggested that there is a relationship between the arising of the dominant fecal flora, coliform bacteria, colonizing the perineum which enters and ascends to the urinary tract in girls [41,42,43]. In fact, studies have demonstrated that the UPEC strains possess specific properties. For instance, both pili and fimbriae can mediate bacterial attachment and invasion to the uroepithelial cell surface, allowing them to overcome the host defenses [16,42]. In addition, the majority of pathogenic bacteria in UTIs are the commensal bacteria and their pathogenicity might result from microbiota dysbiosis [42].
In this current study, the frequency of UTIs by E. coli was widely reduced in older children. It showed high infection rates in children aged between 0–3 years and during toilet training for 4–5 years, particularly in girls. The increase in the incidence rate of UTIs at these ages may be due to the use of diapers and the wet tissues for infants and during toilet training for 4–5 years [44]. Boys with UTIs have rarely been detected in this study and this is due to the fact that almost all boys have undergone circumcision in their first week after birth [45]. Thus, this finding is dissimilar to Western studies and highlights the notion that uncircumcision in boys is the main reason for the higher UTIs proportion than girls, which is inverse in our communities [46,47].
In this study, the antimicrobial susceptibility testing of E. coli showed that 97% of them were highly resistant to Tetracycline. This finding is higher than previous studies conducted with different child age groups in Iraq: 63% [48], 83% [33] and 80% [49]. High resistance may primarily be attributed to the diversity of genes in various bacteria that regulate the efflux of Tetracyclines from the cell [50]. Furthermore, this study demonstrated around 85% higher resistance to Penicillin agents, including Amoxicillin and Ampicillin. This may be due to the misuse of older antimicrobials that have made it a less acceptable choice, such as Penicillins agent [51]. Although it has been suggested that certain Penicillins, when taken with β-lactamase inhibitors (clavulanic acid), are useful in treating some infections caused by bacteria that produce ESBLs [50], in this study, 64% of E. coli were resistant to Amoxicillin-clavulanic acid. This finding is in agreement with a similar laboratory-based recent study conducted in Turkey [52], while half of it was found in a study conducted in a European country such as Poland [53].
It has been emphasized that Imipenem is considered a stable antibiotic against the enzyme ESBLs produced by Enterobacteriaceae as well as preferred for treating serious infections caused by bacteria producing β-lactamase [54]. In the current study, approximately 88% of E. coli were sensitive to Imipenem. This finding was slightly lower when compared with other results from studies in Iraq, roughly 95.2% in Erbil city [36,37], and 100% in Baghdad [38]. It is surprising that the very recent data estimated that E. coli have not been observed to be resistant to Imipenem in UTIs patients under 12 old in Iran [55], and in the various ages in Iraqi studies, such as those in Duhok city [56] and Erbil city [57], as well as in Saudi Arabia [58]. In other words, E. coli resistance to Imipenem is steadily increasing when compared with studies of UTIs in various age groups, and this is due to the use of over-the-counter antibiotics and the ease of finding and buying antibiotics without a prescription. The public health sector has not verified the guidelines for how to control the selling of antibiotics. In addition, both Nitrofurantoin and chloramphenicol are considered the second most effective antibiotic against these isolates, roughly 85% in this present study. A similar result was found for Nitrofurantoin in a study conducted in Ethiopia for children under 15 years [59], while a dissimilar finding for E. coli resistance to chloramphenicol was recorded in a study in Iran, accounting for about 72% [60].
It has been previously noted that E. coli which produce extended-spectrum β-lactamase (ESBL) are becoming more common in the community worldwide [61]. In this study, all isolates of E. coli were subjected to detect ESBLs phenotypically in a clinical microbiology laboratory and approximately 64% of E. coli were positive for ESBLs production. The prevalence rate ESBL-producing E. coli was higher compared with several studies from Middle Eastern countries, approximately 30% in both Qatar [27] and Iran [28], about 41% in Turkey [29], and also in European countries, about 16.8% in Sweden [31] and around 2% in Spain [30]. According to Rupp [19], the DDST is much more sensitive and specific. The DDST, however, can produce false-positive or false-negative results [22,62]. Therefore, all isolates of E. coli were subjected to PCR using TEM, CTX-M, and SHV-specific primers for the detection of ESBL genes. Approximately 64% of E. coli were positive for the DDST, while 94% and 89% of them were identified as possessing ESBL genes, TEM and CTX-M, respectively. However, a total of 19 E. coli strains have the ESBL marker genes from 24 non-ESBL producer E. coli, and they were identified by DDST. This finding suggests that the detection of ESBL by PCR is more sensitive than the DDST.
In this study, all isolated E. coli were confirmed by the PCR amplification of E. coli-specific marker gene (uidA). As is known, this gene is widely used in the identification of E. coli from clinical samples [63,64,65,66]. Evidence demonstrated that the presence of pai in pathogenic strains carries genes encoding more virulence factors, such as adhesins, toxins (cnf-1 and hly), invasions, and iron absorption systems [67,68]. Altogether, these bacterial virulence factors enhance their ability to adhere, invade and colonize a host and increase the pathogenicity [69,70]. These virulence factors also help pathogenic bacteria to become resistant to immune defenses, such as phagocytosis, the complement system, or adaptive immune responses [69,70,71]. Altogether, these gene factors in UPEC contribute to urinary virulence associated with severe UTIs [18]. Thus, in this study, the high prevalence of virulence factors in the UPEC strain are major causative agents for UTIs in children in Iraq, with a high prevalence rate of both pai (94%) and hly (82%) in almost UPEC strains. The hly gene finding was similar (81%) to a very recent study of uropathogenic E. coli in Egyptian patients (age range 23–56) [72]. These findings were dissimilar to several recent studies among various age groups with UTIs, for pai virulence gene, approximately 72% higher when compared to a study in Zakho City [48] and around 20% higher in three different cities in Kurdistan [33], and the hly virulence gene was found to be 60% higher by [48] and 45% higher by [33]. Whereas afa was roughly similar when compared with a study in Duhok City.
In addition, further analysis was conducted to answer whether the virulence genes have a role in increasing antibiotic-resistant genes or not. Only one study was reported in Egypt by Abd El-Baky et al. [72] which found a significant positive correlation between CTX and hly, similar to this study. Thus, further molecular studies of whole genome sequencing are recommended to highlight the relationship between the virulence factors and antibiotic-resistant genes of these pathogenic E. coli.
Regarding the age, it is noteworthy in this study that the negative correlation between the age of pediatrics and UTIs by UPEC with their resistance to antibiotics and both genes of resistance and virulence factors. This finding has not been previously reported in Iraq. A recently reviewed study has highlighted the reduction in UTIs in children, particularly after age 6 [10]. In addition, the high prevalence of UTIs with E. coli in pediatrics depends on other factors as well. These factors together can cause more UTI outcomes in children than in adolescents. A study by Pärnänen et al. [73] reported that although infants were not exposed to antibiotics, their gut microbiome contains a higher abundance of antibiotic resistance genes than adults. Pärnänen and their colleagues found that the features of infants’ fecal antibiotic resistance genes and mobile genetic element profiles were inherited from their mother’s gut and breast milk microbiota.
The limitation of this study is the lack of molecular characterization, 16s rRNA gene and whole genome sequencing of E. coli for the phylogenetic analysis might help understand the epidemiology and clinical microbial infection of UPEC in our community.
4. Materials and Methods
4.1. Sample Collection
The current study was conducted in the microbiology Laboratory of Heevi Pediatric Teaching Hospital in Duhok Governorate, Iraq, from August 2021 to the end of February 2022. A total 260 urine samples were collected from in-patient and out-patient children 0–15 years old with clinical suspicion of UTIs and not receiving antimicrobial treatment.
4.2. E. coli Isolation and Identification
Collected urine samples were cultured on MacConkey agar and Blood agar (containing 5% human blood) and aerobically incubated overnight at 37 °C. A growth of a single organism with a count of ≥105 colony-forming unit (CFU)/mL was considered to represent the UTIs [74,75,76]. The lactose-fermenting colonies were selected and sub-cultured on both MacConkey and Eosin methylene Blue (EMB) agar to obtain a pure culture and to identify E. coli by green metallic sheen on EMB and Pink colonies on MacConkey agar. Based on the morphological and biochemical characteristics of these pure colonies was identified according to study by [77].
4.3. Antimicrobial Susceptibility Test and ESBLs Detection
All isolated E. coli were subjected to antibiotic susceptibility test using Kirby–Bauer disk diffusion method by spreading the inoculated sterile swab on Muller–Hinton agar incubated overnight aerobically at 37 °C according to [78]. Nineteen antibiotics were used, supplied by (Bioanalyses, Turkey), Amikacin (AK; 10 mg), Ceftazidime (CAZ; 30 mg), Amoxicillin (AX; 25 mg), Cefotaxime (CTX; 30 mg), Nitrofurantoin (F; 100 mg), Gentamicin (CN; 10 mg), Imipenem (IPM; 10 mg), Trimethoprim/ Sulphamethoxazole (SXT; 25 mg), Tetracycline (TE; 10 mg), Ciprofloxacin (CIP; 10 mg), Levofloxacin (LEV; 5 mg), Amoxicillin/Clavulanic acid (AMC; 30 mg), Aztreonam (ATM; 30 mg), Ampicillin (AM; 25 mg), Ceftriaxone (CRO; 10 mg), Chloramphenicol (C; 10 mg), Cefixime (CFM; 5 mg), Nalidixic acid (NA; 30 mg) and Norfloxacin (NOR; 30 mg). The diameter of the inhibition zone around antibiotic disks was measured according to the Clinical and Laboratory Standards Institute [79].
A double-disk synergy test was used to identify E. coli ESBL producer and five antibiotic disks (Cefotaxime, Ceftazidime, Ceftriaxone and Aztreonam were placed 30 mm from an amoxicillin/clavulanate in the center) were used on Muller–Hinton agar according to the method described by [80].
4.4. Bacterial DNA Extraction from E. coli
Bacterial DNA was extracted from isolated E. coli using the Quick DNA Extraction kit (Guangzhou Dongsheng Biotech Co., Ltd.) following the manufacturer’s protocol. Bacterial DNA quality was achieved by (NanoDrop™ One UV-Vis Spectrophotometer, Thermo Fisher Scientific, Waltham, MA, USA) and then stored at −20 °C for DNA amplification. Different primers were used for amplification of these marker genes (Macrogen, Seoul, Korea) as described in Table 2. Purified DNA was used for PCR amplification of 9 genes (Table 3). A species-specific primer for E. coli, uidA gene. After confirming E. coli, 3 primers were used to detect ESBL genotypes, blaCTX-M, blaTEM and blaSHV β-lactamase genes. In addition, five primers were used for detecting the five virulence genes, including pathogenicity island (pai), hemolysin (hly), S-fimbrial adhesion (sfa), cytotoxic necrotizing factor-1 (cnf-1), and a fimbrial adhesion (afa).
Table 2.
Primer names and sequences for different gene markers in this study.
Table 3.
The PCR amplification condition for detecting different gene markers in this study.
The amplifications of DNA for each gene were carried out in PCR tubes containing master mix and consisting of 7 µL Tag master (Guangzhou Dongsheng Biotech Co., Ltd., Guangzhou, China), 1 µL of each forward and reverse primers (10 pmol/µL), 2 µL pure DNA (25–50 ng/µL), and adding 9µL of free-nuclease water to make a final volume of 20 µL. The amplification conditions of each gene are described in Table 2.
The DNA lengths of each fragment produced with these 9 primers were confirmed by running 7 µL of each PCR products on 1.2 % agarose gels in 1× TAE buffer and added 5 µL of Safe Gel stain Dye (Guangzhou Dongsheng Biotech Co., Ltd., Guangzhou, China) and the electrophoresis was performed at 85 V for 35 min. The agarose gel was visualized under the UV radiation (Cleaver Scientific Ltd., Rugby, UK). The images of DNA bands were captured, and the estimated amplicon size were compared with the 100 pb DNA ladder (Guangzhou Dongsheng Biotech Co., Ltd., Guangzhou, China) and 300 bp (GeneDirex, Inc, Taoyuan, Taiwan).
4.5. Statistical Analysis
GraphPad Prism 9.4.1 was used to analyze the data. Spearman’s method was used for nonparametric correlation between the children age and the frequency of UPEC, antibiotics resistance patterns and genes of both ESBL production and virulence factors. Significance was considered to be established when p < 0.05.
4.6. Ethical Approval
The approval for conducting this study was given by the Ethical Committee of Duhok Directorate General of Health (ethical code n 18082021-8-15) and the Ethical and Protocol Review Committee of the Biological Sciences Committee (BSCZ) at the University of Zakho (ID: “BSCZ/28/7/2021”).
5. Conclusions
In conclusion, the data illustrates that E. coli remain the most predominant bacteria among pediatrics with UTIs, particularly for girls. They also state an alarming increase in E. coli with ESBL production of UTIs in children of ages younger than the pre- and school age group of children. The E. coli ESBL-producer was more resistant to antibiotics than the non-producer. Moreover, Imipenem and Nitrofurantoin are considered to be the most effective antibiotic choices for the treatment of pediatric UPEC infections. UPEC resistance to antibiotics decreases with children of the older age group. As well as this, molecular detections of ESBL-producing E. coli were more accurate than phenotypic identification. In addition, ESBL colonization and infection are increased in the urinary tract because of these genes’ products, pai and hly, as well as two β-lactamase genes, blaCTX-M and blaTEM. The public health sectors would be better if they monitored the guidelines for the use of antibiotics and the careful use of antibiotics as recommended by physicians only. Furthermore, doctors need to give more advice about accurate hygiene, especially cleaning toddlers and pre-school children during toilet training to avoid UTIs. Hence, further molecular studies of different clinical specimens and different ages would achieve a confirmed database for ESBL-producing E. coli in Kurdistan, Iraq.
Author Contributions
Conceptualization, K.S.I.; methodology, S.M.H.; formal analysis, K.S.I. and S.M.H.; investigation, K.S.I. and S.M.H.; resources, K.S.I. and S.M.H.; data curation, K.S.I. and S.M.H.; writing—original draft preparation, S.M.H.; writing—review and editing, K.S.I.; visualization, K.S.I.; supervision, K.S.I.; project administration, K.S.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the Ethical Committee Approval of Duhok Directorate General of Health (ethical code n 18082021-8-15) and approved by the Biological Sciences Committee (BSCZ) at the University of Zakho (ID: BSCZ/28/7/2021).
Informed Consent Statement
Patient’s parent informed consent was obtained from all participants children involved in the study.
Data Availability Statement
All material information described in the manuscript and all relevant primary data, is openly accessible.
Acknowledgments
The authors are thankful to the Heevi Pediatric Teaching Hospital, Department of Biology, Faculty of Science, University of Zakho and Scientific Research Center Department of the Science college, University of Duhok, in (Duhok governorate Kurdistan region of Iraq), for providing some of the research facilities.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
The total of antibiotic resistance profiles and genes, ESBL production and virulence factor genes of all isolated E. coli in different pediatric ages.

References
- Núñez-Samudio, V.; Pecchio, M.; Pimentel-Peralta, G.; Quintero, Y.; Herrera, M.; Landires, I. Molecular Epidemiology of Escherichia coli Clinical Isolates from Central Panama. Antibiotics 2021, 10, 899. [Google Scholar] [CrossRef] [PubMed]
- Kresken, M.; Pfeifer, Y.; Wagenlehner, F.; Werner, G.; Wohlfarth, E.; Study Group ‘Antimicrobial Resistance’ of the Paul Ehrlich Society for Infection Therapy. Resistance to Mecillinam and Nine Other Antibiotics for Oral Use in Escherichia coli Isolated from Urine Specimens of Primary Care Patients in Germany, 2019/20. Antibiotics 2022, 11, 751. [Google Scholar] [CrossRef] [PubMed]
- Sahu, R.; Sahoo, R.K.; Prusty, S.K.; Sahu, P.K. Urinary Tract Infection and Its Management. Syst. Rev. Pharm. 2019, 10, 42–48. [Google Scholar] [CrossRef]
- Stamm, W.E.; Norrby, S.R. Urinary Tract Infections: Disease Panorama and Changes. J. Infect. Dis. 2001, 183, S1–S4. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary Tract Infections: Epidemiology, Mechanisms of Infection and Treatment Options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Millner, R.; Becknell, B. Urinary Tract Infections. Pediatr. Clin. N. Am. 2019, 66, 1–13. [Google Scholar] [CrossRef]
- Schmidt, B.; Copp, H.L. Work-up of Pediatric Urinary Tract Infection. Urol. Clin. 2015, 42, 519–526. [Google Scholar] [CrossRef]
- Freedman, A.L.; Urologic Diseases in America Project. Urologic Diseases in North America Project: Trends in Resource Utilization for Urinary Tract Infections in Children. J. Urol. 2005, 173, 949–954. [Google Scholar] [CrossRef]
- Nibhanipudi, K.V. A Study to Determine the Incidence of Urinary Tract Infections in Infants and Children Ages 4 Months to 6 Years with Febrile Diarrhea. Glob. Pediatr. Health 2016, 3, 2333794X16667175. [Google Scholar] [CrossRef]
- Tullus, K.; Shaikh, N. Urinary Tract Infections in Children. Lancet 2020, 395, 1659–1668. [Google Scholar] [CrossRef]
- Ismaili, K.; Wissing, K.M.; Lolin, K.; Le, P.Q.; Christophe, C.; Lepage, P.; Hall, M. Characteristics of First Urinary Tract Infection with Fever in Children: A Prospective Clinical and Imaging Study. Pediatr. Infect. Dis. J. 2011, 30, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Montini, G.; Tullus, K.; Hewitt, I. Febrile Urinary Tract Infections in Children. N. Engl. J. Med. 2011, 365, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Morone, N.E.; Bost, J.E.; Farrell, M.H. Prevalence of Urinary Tract Infection in Childhood: A Meta-Analysis. Pediatr. Infect. Dis. J. 2008, 27, 302–308. [Google Scholar] [CrossRef]
- Johnson, J.R.; Kuskowski, M.A.; O’bryan, T.T.; Colodner, R.; Raz, R. Virulence Genotype and Phylogenetic Origin in Relation to Antibiotic Resistance Profile among Escherichia Coli Urine Sample Isolates from Israeli Women with Acute Uncomplicated Cystitis. Antimicrob. Agents Chemother. 2005, 49, 26–31. [Google Scholar] [CrossRef]
- Wiles, T.J.; Kulesus, R.R.; Mulvey, M.A. Origins and Virulence Mechanisms of Uropathogenic Escherichia coli. Exp. Mol. Pathol. 2008, 85, 11–19. [Google Scholar] [CrossRef]
- Mulvey, M.A.; Schilling, J.D.; Martinez, J.J.; Hultgren, S.J. Bad Bugs and Beleaguered Bladders: Interplay between Uropathogenic Escherichia coli and Innate Host Defenses. Proc. Natl. Acad. Sci. USA 2000, 97, 8829–8835. [Google Scholar] [CrossRef]
- Marrs, C.F.; Zhang, L.; Foxman, B. Escherichia coli Mediated Urinary Tract Infections: Are There Distinct Uropathogenic E. coli (UPEC) Pathotypes? FEMS Microbiol. Lett. 2005, 252, 183–190. [Google Scholar] [CrossRef]
- Bien, J.; Sokolova, O.; Bozko, P. Role of Uropathogenic Escherichia coli Virulence Factors in Development of Urinary Tract Infection and Kidney Damage. Int. J. Nephrol. 2012, 2012, 681473. [Google Scholar] [CrossRef]
- Rupp, M.E.; Fey, P.D. Extended Spectrum β-Lactamase (ESBL)-Producing Enterobacteriaceae. Drugs 2003, 63, 353–365. [Google Scholar] [CrossRef]
- Toussaint, K.A.; Gallagher, J.C. β-Lactam/β-Lactamase Inhibitor Combinations: From Then to Now. Ann. Pharmacother. 2015, 49, 86–98. [Google Scholar] [CrossRef]
- Paterson, D.L. Recommendation for Treatment of Severe Infections Caused by Enterobacteriaceae Producing Extended-Spectrum β-Lactamases (ESBLs). Clin. Microbiol. Infect. 2000, 6, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L.; Bonomo, R.A. Extended-Spectrum β-Lactamases: A Clinical Update. Clin. Microbiol. Rev. 2005, 18, 657–686. [Google Scholar] [CrossRef] [PubMed]
- Ngoi, S.T.; Teh, C.S.J.; Chong, C.W.; Abdul Jabar, K.; Tan, S.C.; Yu, L.H.; Leong, K.C.; Tee, L.H.; AbuBakar, S. In Vitro Efficacy of Flomoxef against Extended-Spectrum Beta-Lactamase-Producing Escherichia coli and Klebsiella Pneumoniae Associated with Urinary Tract Infections in Malaysia. Antibiotics 2021, 10, 181. [Google Scholar] [CrossRef]
- World Health Organization. Global Priority Pathogens List of Antibiotic-Resistant Bacteria; WHO: Geneva, Switzerland, 2021; Volume 500. Available online: https://www.doherty.edu.au/news-events/news/who-global-priority-pathogens-list-of-antibiotic-501resistant-bacteria (accessed on 30 June 2022).
- Raphael, E.; Glymour, M.M.; Chambers, H.F. Trends in Prevalence of Extended-Spectrum Beta-Lactamase-Producing Escherichia coli Isolated from Patients with Community-and Healthcare-Associated Bacteriuria: Results from 2014 to 2020 in an Urban Safety-Net Healthcare System. Antimicrob. Resist. Infect. Control 2021, 10, 118. [Google Scholar] [CrossRef] [PubMed]
- Yasir, M.; Ajlan, A.M.; Shakil, S.; Jiman-Fatani, A.A.; Almasaudi, S.B.; Farman, M.; Baazeem, Z.M.; Baabdullah, R.; Alawi, M.; Al-Abdullah, N. Molecular Characterization, Antimicrobial Resistance and Clinico-Bioinformatics Approaches to Address the Problem of Extended-Spectrum β-Lactamase-Producing Escherichia coli in Western Saudi Arabia. Sci. Rep. 2018, 8, 14847. [Google Scholar] [CrossRef]
- Awean, G.Z.A.; Salameh, K.; Elmohamed, H.; Alshmayt, H.; Omer, M.R.B. Prevalence of ESBL Urinary Tract Infection in Children. J Adv. Pediatr. Child Health 2019, 2, 4–7. [Google Scholar] [CrossRef]
- Rezai, M.S.; Salehifar, E.; Rafiei, A.; Langaee, T.; Rafati, M.; Shafahi, K.; Eslami, G. Characterization of Multidrug Resistant Extended-Spectrum Beta-Lactamase-Producing Escherichia coli among Uropathogens of Pediatrics in North of Iran. Biomed Res. Int. 2015, 2015, 309478. [Google Scholar] [CrossRef]
- Kizilca, O.; Siraneci, R.; Yilmaz, A.; Hatipoglu, N.; Ozturk, E.; Kiyak, A.; Ozkok, D. Risk Factors for Community-acquired Urinary Tract Infection Caused by ESBL-producing Bacteria in Children. Pediatr. Int. 2012, 54, 858–862. [Google Scholar] [CrossRef]
- Rodríguez-Bano, J.; Navarro, M.D.; Romero, L.; Martínez-Martínez, L.; Muniain, M.A.; Perea, E.J.; Pérez-Cano, R.; Pascual, A. Epidemiology and Clinical Features of Infections Caused by Extended-Spectrum Beta-Lactamase-Producing Escherichia coli in Nonhospitalized Patients. J. Clin. Microbiol. 2004, 42, 1089–1094. [Google Scholar] [CrossRef]
- Kaarme, J.; Riedel, H.; Schaal, W.; Yin, H.; Nevéus, T.; Melhus, Å. Rapid Increase in Carriage Rates of Enterobacteriaceae Producing Extended-Spectrum β-Lactamases in Healthy Preschool Children, Sweden. Emerg. Infect. Dis. 2018, 24, 1874. [Google Scholar] [CrossRef]
- Ibrahim, M.; Khalid, H.M.; Mer, W.M.S. The Prevalence of Uropathogenic Escherichia coli Strains among Outpatients with Urinary Tract Infection in Zakho Hospitals-Zakho City, Duhok Province/Iraq. Al-Qadisiyah J. Pure Sci. 2021, 26, 26–40. [Google Scholar] [CrossRef]
- Merza, N.S.; Jubrael, J.M.S. The Prevalence of Virulence Factors among Uropathogenic Escherichia coli Strains Isolated from Different Hospitals in Kurdistan Region-Iraq. Int. J. Bioinforma Biomed. Eng. 2015, 1, 338–343. [Google Scholar]
- Naqid, I.A.; Balatay, A.A.; Hussein, N.R.; Ahmed, H.A.; Saeed, K.A.; Abdi, S.A. Bacterial Strains and Antimicrobial Susceptibility Patterns in Male Urinary Tract Infections in Duhok Province, Iraq. Middle East J. Rehabil. Health Stud. 2020, 7, e103529. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Mohamed, D.A.; Suleman, S.K. Microbial Causes of Urinary Tract Infection and Its Sensitivity to Antibiotics at Heevi Pediatric Teaching Hospital/Duhok City. Med. J. Babylon 2020, 17, 109. [Google Scholar]
- Saeed, C.H.; AL-Otraqchi, K.I.B.; Mansoor, I.Y. Prevalence of Urinary Tract Infections and Antibiotics Susceptibility Pattern among Infants and Young Children in Erbil City. Zanco J. Med. Sci. 2015, 19, 915–922. [Google Scholar] [CrossRef]
- Alkhateeb, N.E.R. Antibiotic Resistance of Urinary Tract Pathogens and Rationale for Empirical Antibiotic Therapy in Children with Urinary Tract Infection. Zanco J. Med. Sci. 2016, 20, 1458_1466. [Google Scholar]
- Hussein, N.H. Prevalence and Antimicrobial Susceptibility Patterns of Bacteria Isolated from Urinary Tract Infections (UTIs) in Children at Children Hospital in Baghdad. Al-Kindy Coll. Med. J. 2017, 13, 102–107. [Google Scholar] [CrossRef]
- Chen, H.E.; Tain, Y.L.; Kuo, H.C.; Hsu, C.N. Trends in Antimicrobial Susceptibility of Escherichia coli Isolates in a Taiwanese Child Cohort with Urinary Tract Infections between 2004 and 2018. Antibiotics 2020, 9, 501. [Google Scholar] [CrossRef]
- Foxman, B. Urinary Tract Infection Syndromes: Occurrence, Recurrence, Bacteriology, Risk Factors, and Disease Burden. Infect. Dis. Clin. 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Moreno, E.; Andreu, A.; Perez, T.; Sabaté, M.; Johnson, J.R.; Prats, G. Relationship between Escherichia coli Strains Causing Urinary Tract Infection in Women and the Dominant Faecal Flora of the Same Hosts. Epidemiol. Infect. 2006, 134, 1015–1023. [Google Scholar] [CrossRef]
- Morand, A.; Cornu, F.; Dufour, J.-C.; Tsimaratos, M.; Lagier, J.-C.; Raoult, D. Human Bacterial Repertoire of the Urinary Tract: A Potential Paradigm Shift. J. Clin. Microbiol. 2019, 57, e00675-18. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C.; Wong, A.H.C.; Leung, A.A.M.; Hon, K.L. Urinary Tract Infection in Children. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Fahimzad, A.; Taherian, M.; Dalirani, R.; Shamshiri, A. Diaper Type as a Risk Factor in Urinary Tract Infection of Children. Iran. J. Pediatr. 2010, 20, 97–100. [Google Scholar] [PubMed]
- Banieghbal, B. Optimal Time for Neonatal Circumcision: An Observation-Based Study. J. Pediatr. Urol. 2009, 5, 359–362. [Google Scholar] [CrossRef] [PubMed]
- To, T.; Agha, M.; Dick, P.T.; Feldman, W. Cohort Study on Circumcision of Newborn Boys and Subsequent Risk of Urinary-Tract Infection. Lancet 1998, 352, 1813–1816. [Google Scholar] [CrossRef]
- Singh-Grewal, D.; Macdessi, J.; Craig, J. Circumcision for the Prevention of Urinary Tract Infection in Boys: A Systematic Review of Randomised Trials and Observational Studies. Arch. Dis. Child. 2005, 90, 853–858. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Khalid, H.M.; Mero, W.M. Molecular Characterization of Some Virulence Genes and Antibiotics Resistance of Uropathogenic Escherichia coli Isolated from Patients in Zakho City, Kurdistan Region/Iraq. Zanco J. of Pure and Appl. Sci. 2020, 32, 167–177. [Google Scholar] [CrossRef]
- Al- Barzinji, R.; Esmahil, S.; Sulaiman, S.; Raheem, S. Effect of Some Antimicrobial Agents on Isolated Bacteria from Patients with Urinary Tract Infection in Kurdistan Region. Zanco J. Med. Sci. 2010, 14, 61–67. [Google Scholar] [CrossRef]
- Murray, P.R.; Rosenthal, K.S.; Pfaller, M.A. Antimicrobial Agents; Elsevier: Amsterdam, The Netherlands, 2016; pp. 183–190. [Google Scholar]
- Nicolle, L.E. Complicated Urinary Tract Infection in Adults. Can. J. Infect. Dis. Med. Microbiol. 2005, 16, 349–360. [Google Scholar] [CrossRef]
- Demir, M.; Kazanasmaz, H. Uropathogens and Antibiotic Resistance in the Community and Hospital-Induced Urinary Tract Infected Children. J. Glob. Antimicrob. Resist. 2020, 20, 68–73. [Google Scholar] [CrossRef]
- Kot, B.; Grużewska, A.; Szweda, P.; Wicha, J.; Parulska, U. Antibiotic Resistance of Uropathogens Isolated from Patients Hospitalized in District Hospital in Central Poland in 2020. Antibiotics 2021, 10, 447. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L. Resistance in Gram-Negative Bacteria: Enterobacteriaceae. Am. J. Infect. Control 2006, 34, S20–S28. [Google Scholar] [CrossRef] [PubMed]
- Sharif, M.; Nori, S. The Frequency and Antibiotic Resistance of Urinary Tract Infection Organisms in Hospitalized Children Shahid Beheshti Hospital, Kashan 2012–2013. Iran. J. Infect. Dis. Trop. Med. 2014, 65, 47–51. [Google Scholar]
- Assafi, M.S.A.; Ibrahim, N.M.R.; Hussein, N.R.; Taha, A.A.; Balatay, A.A. Urinary Bacterial Profile and Antibiotic Susceptibility Pattern among Patients with Urinary Tract Infection in Duhok City, Kurdistan Region, Iraq. Int. J. Pure Appl. Sci. Technol. 2015, 30, 54. [Google Scholar]
- Aka, S.T.; Haji, S.H. Evaluation of Multi Drug Resistance among Extended Spectrum β-Lactamase-Producing Escherichia coli Causing Urinary Tract Infection in Erbil City. Zanco J. Med. Sci. 2015, 19, 998–1004. [Google Scholar] [CrossRef][Green Version]
- Alqasim, A.; Abu Jaffal, A.; Alyousef, A.A. Prevalence of Multidrug Resistance and Extended-Spectrum β-Lactamase Carriage of Clinical Uropathogenic Escherichia coli Isolates in Riyadh, Saudi Arabia. Int. J. Microbiol. 2018, 2018, 3026851. [Google Scholar] [CrossRef]
- Agegnehu, A.; Worku, M.; Nigussie, D.; Lulu, B.; Tadesse, B.T. Pediatric Febrile Urinary Tract Infection Caused by ESBL Producing Enterobacteriaceae Species. Biomed Res. Int. 2020, 2020, 6679029. [Google Scholar] [CrossRef]
- Mortazavi-Tabatabaei, S.A.R.; Ghaderkhani, J.; Nazari, A.; Sayehmiri, K.; Sayehmiri, F.; Pakzad, I. Pattern of Antibacterial Resistance in Urinary Tract Infections: A Systematic Review and Meta-Analysis. Int. J. Prev. Med. 2019, 10, 169. [Google Scholar]
- Calbo, E.; Romaní, V.; Xercavins, M.; Gómez, L.; Vidal, C.G.; Quintana, S.; Vila, J.; Garau, J. Risk Factors for Community-Onset Urinary Tract Infections Due to Escherichia coli Harbouring Extended-Spectrum β-Lactamases. J. Antimicrob. Chemother. 2006, 57, 780–783. [Google Scholar] [CrossRef]
- Rawat, D.; Nair, D. Extended-Spectrum β-Lactamases in Gram Negative Bacteria. J. Glob. Infect. Dis. 2010, 2, 263. [Google Scholar] [CrossRef]
- Cleuziat, P.; Robert-Baudouy, J. Specific Detection of Escherichia coli and Shigella Species Using Fragments of Genes Coding for β-Glucuronidase. FEMS Microbiol. Lett. 1990, 72, 315–322. [Google Scholar] [CrossRef]
- Feng, P.; Lum, R.; Chang, G.W. Identification of UidA Gene Sequences in Beta-D-Glucuronidase-Negative Escherichia coli. Appl. Environ. Microbiol. 1991, 57, 320–323. [Google Scholar] [CrossRef]
- Farnleitner, A.H.; Kreuzinger, N.; Kavka, G.G.; Grillenberger, S.; Rath, J.; Mach, R.L. Simultaneous Detection and Differentiation of Escherichia coli Populations from Environmental Freshwaters by Means of Sequence Variations in a Fragment of the β-D-Glucuronidase Gene. Appl. Environ. Microbiol. 2000, 66, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Brons, J.K.; Vink, S.N.; de Vos, M.G.J.; Reuter, S.; Dobrindt, U.; van Elsas, J.D. Fast Identification of Escherichia coli in Urinary Tract Infections Using a Virulence Gene Based PCR Approach in a Novel Thermal Cycler. J. Microbiol. Methods 2020, 169, 105799. [Google Scholar] [CrossRef] [PubMed]
- Karaolis, D.K.R. Pathogenicity Islands. In Encyclopedia of Genetics; Academic Press (Elsevier): Amsterdam, The Netherlands, 2001; pp. 1422–1424. [Google Scholar]
- Tarchouna, M.; Ferjani, A.; Ben-Selma, W.; Boukadida, J. Distribution of Uropathogenic Virulence Genes in Escherichia coli Isolated from Patients with Urinary Tract Infection. Int. J. Infect. Dis. 2013, 17, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, M.; Brooks, B.D.; Brooks, A.E. The Complex Relationship between Virulence and Antibiotic Resistance. Genes 2017, 8, 39. [Google Scholar] [CrossRef]
- Giaouris, E.; Heir, E.; Desvaux, M.; Hébraud, M.; Møretrø, T.; Langsrud, S.; Doulgeraki, A.; Nychas, G.-J.; Kačániová, M.; Czaczyk, K. Intra-and Inter-Species Interactions within Biofilms of Important Foodborne Bacterial Pathogens. Front. Microbiol. 2015, 6, 841. [Google Scholar] [CrossRef]
- Srivastava, N.; Srivastava, M.; Mishra, P.K.; Ramteke, P.W.; Singh, R.L. New and Future Developments in Microbial Biotechnology and Bioengineering: From Cellulose to Cellulase: Strategies to Improve Biofuel Production; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Abd El-Baky, R.M.; Ibrahim, R.A.; Mohamed, D.S.; Ahmed, E.F.; Hashem, Z.S. Prevalence of Virulence Genes and Their Association with Antimicrobial Resistance among Pathogenic E. coli Isolated from Egyptian Patients with Different Clinical Infections. Infect. Drug Resist. 2020, 13, 1221. [Google Scholar] [CrossRef]
- Pärnänen, K.; Karkman, A.; Hultman, J.; Lyra, C.; Bengtsson-Palme, J.; Larsson, D.G.; Rautava, S.; Isolauri, E.; Salminen, S.; Kumar, H. Maternal Gut and Breast Milk Microbiota Affect Infant Gut Antibiotic Resistome and Mobile Genetic Elements. Nat. Commun. 2018, 9, 3891. [Google Scholar] [CrossRef]
- Zwane, T.; Shuping, L.; Perovic, O. Etiology and Antimicrobial Susceptibility of Pathogens Associated with Urinary Tract Infections among Women Attending Antenatal Care in Four South African Tertiary-Level Facilities, 2015–2019. Antibiotics 2021, 10, 669. [Google Scholar] [CrossRef]
- Roberts, K.B.; Downs, S.M.; Finnell, S.M.E.; Hellerstein, S.; Shortliffe, L.D.; Wald, E.R.; Zerin, J.M. Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Larcombe, J. Urinary tract infection in children. Am. Fam. Physician 2010, 82, 1252–1256. [Google Scholar] [PubMed]
- Leboffe, M.J.; Pierce, B.E. A Photographic Atlas for the Microbiology Laboratory, 4th ed.; Morton Pub. Co: Englewood, CO, USA, 2011. [Google Scholar]
- Hudzicki, J. Kirby-Bauer Disk Diffusion Susceptibility Test Protocol. Am. Soc. Microbiol. 2009, 15, 55–63. [Google Scholar]
- CLSI (Clinical and Laboratory Standards Institute). Performanc Standards for Antimicrobial 409 Susceptibility testing; Seventeeth Informational Supplement. M100-17; Clinical and Laboratory Standards 410 Institute: Wayne, PA, USA, 2007. [Google Scholar]
- Jarlier, V.; Nicolas, M.-H.; Fournier, G.; Philippon, A. Extended Broad-Spectrum β-Lactamases Conferring Transferable Resistance to Newer β-Lactam Agents in Enterobacteriaceae: Hospital Prevalence and Susceptibility Patterns. Clin. Infect. Dis. 1988, 10, 867–878. [Google Scholar] [CrossRef]
- Adamus-Bialek, W.; Wojtasik, A.; Majchrzak, M.; Sosnowski, M.; Parniewski, P. (CGG) 4-Based PCR as a Novel Tool for Discrimination of Uropathogenic Escherichia coli Strains: Comparison with Enterobacterial Repetitive Intergenic Consensus-PCR. J. Clin. Microbiol. 2009, 47, 3937–3944. [Google Scholar] [CrossRef]
- Oliveira, F.A.; Paludo, K.S.; Arend, L.; Farah, S.; Pedrosa, F.O.; Souza, E.M.; Surek, M.; Picheth, G.; Fadel-Picheth, C.M. Virulence Characteristics and Antimicrobial Susceptibility of Uropathogenic Escherichia coli Strains. Genet. Mol. Res. 2011, 10, 4114–4125. [Google Scholar] [CrossRef]
- Le Bouguenec, C.; Archambaud, M.; Labigne, A. Rapid and Specific Detection of the Pap, Afa, and Sfa Adhesin-Encoding Operons in Uropathogenic Escherichia coli Strains by Polymerase Chain Reaction. J. Clin. Microbiol. 1992, 30, 1189–1193. [Google Scholar] [CrossRef]
- Mladin, C.; Usein, C.-R.; Chifiriuc, M.-C.; Palade, A.; Slavu, C.L.; Negut, M.; Damian, M. Genetic Analysis of Virulence and Pathogenicity Features of Uropathogenic Escherichia coli Isolated from Patients with Neurogenic Bladder. Rom. Biotechnol. Lett. 2009, 14, 4906–4911. [Google Scholar]
- Chapman, T.A.; Wu, X.-Y.; Barchia, I.; Bettelheim, K.A.; Driesen, S.; Trott, D.; Wilson, M.; Chin, J.J.-C. Comparison of Virulence Gene Profiles of Escherichia coli Strains Isolated from Healthy and Diarrheic Swine. Appl. Environ. Microbiol. 2006, 72, 4782–4795. [Google Scholar] [CrossRef]
- Pandit, R.; Awal, B.; Shrestha, S.S.; Joshi, G.; Rijal, B.P.; Parajuli, N.P. Extended-Spectrum β-Lactamase (ESBL) Genotypes among Multidrug-Resistant Uropathogenic Escherichia coli Clinical Isolates from a Teaching Hospital of Nepal. Interdiscip. Perspect. Infect. Dis. 2020, 2020, 6525826. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).