
Changes in the Prescription of Antibiotics and Phytopharmaceuticals in Children Treated for Acute Upper and Lower Respiratory Tract Infections in Pediatric Practices in Germany in 2013, 2018, and 2022

Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of the Study Sample
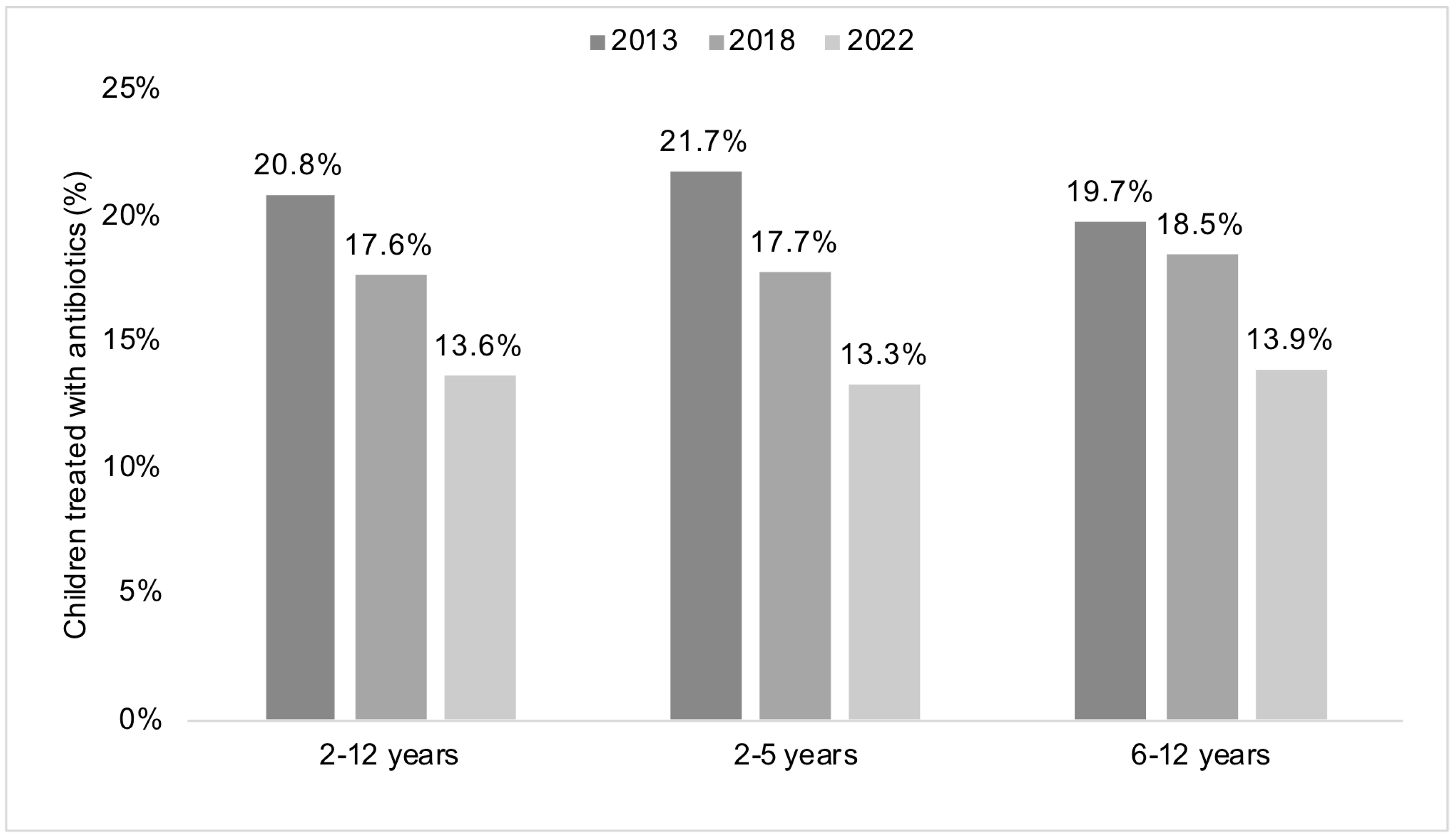
3.2. Changes in the Prescription of Antibiotics between 2013 and 2018 and between 2018 and 2022
3.3. Changes in the Prescription of Phytopharmaceuticals between 2013 and 2018 and between 2018 and 2022
3.4. Correlation between Antibiotic Prescription and Phytopharmaceutical Prescription per Pediatric Practice
4. Discussion
4.1. Main Findings
4.2. Interpretation of the Findings
4.3. Public Health Implications and Directions for Future Research
4.4. Strengths and Limitations
4.5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grief, S.N. Upper Respiratory Infections. Prim. Care 2013, 40, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Klig, J.E.; Chen, L. Lower Respiratory Infections in Children. Curr. Opin. Pediatr. 2003, 15, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Ren, J.; Li, R.; Gao, Y.; Zhang, H.; Li, J.; Zhang, J.; Wang, X.; Wang, G. Global Burden of Upper Respiratory Infections in 204 Countries and Territories, from 1990 to 2019. eClinicalMedicine 2021, 37, 100986. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. GBD 2019 Child and Adolescent Communicable Disease Collaborators The Unfinished Agenda of Communicable Diseases among Children and Adolescents before the COVID-19 Pandemic, 1990–2019: A Systematic Analysis of the Global Burden of Disease Study 2019. Lancet 2023, 402, 313–335. [Google Scholar] [CrossRef]
- Azor-Martínez, E.; Gonzalez-Jimenez, Y.; Seijas-Vazquez, M.L.; Cobos-Carrascosa, E.; Santisteban-Martínez, J.; Martínez-López, J.M.; Jimenez-Noguera, E.; Galan-Requena, M.d.M.; Garrido-Fernández, P.; Strizzi, J.M.; et al. The Impact of Common Infections on School Absenteeism during an Academic Year. Am. J. Infect. Control 2014, 42, 632–637. [Google Scholar] [CrossRef]
- Paalanne, M.; Honkila, M.; Paalanne, N.; Mattila, S.; Pokka, T.; Renko, M.; Tapiainen, T. Absence from Day Care or School and Parental Absence from Work during Children’s Respiratory Infections. Acta Paediatr. 2023, 112, 486–492. [Google Scholar] [CrossRef]
- Schot, M.J.C.; Dekker, A.R.J.; van Werkhoven, C.H.; van der Velden, A.W.; Cals, J.W.L.; Broekhuizen, B.D.L.; Hopstaken, R.M.; de Wit, N.J.; Verheij, T.J.M. Burden of Disease in Children with Respiratory Tract Infections in Primary Care: Diary-Based Cohort Study. Fam. Pract. 2019, 36, 723–729. [Google Scholar] [CrossRef]
- Buchholz, U.; Lehfeld, A.-S.; Tolksdorf, K.; Cai, W.; Reiche, J.; Biere, B.; Dürrwald, R.; Buda, S. Respiratory Infections in Children and Adolescents in Germany during the COVID-19 Pandemic. J. Health Monit. 2023, 8, 20–38. [Google Scholar] [CrossRef]
- Shin, S.M.; Shin, J.-Y.; Kim, M.H.; Lee, S.H.; Choi, S.; Park, B.-J. Prevalence of Antibiotic Use for Pediatric Acute Upper Respiratory Tract Infections in Korea. J. Korean Med. Sci. 2015, 30, 617–624. [Google Scholar] [CrossRef]
- Malo, S.; Bjerrum, L.; Feja, C.; Lallana, M.J.; Poncel, A.; Rabanaque, M.J. Antibiotic prescribing in acute respiratory tract infections in general practice. An. Pediatr. (Barc.) 2015, 82, 412–416. [Google Scholar] [CrossRef]
- Fletcher-Lartey, S.; Yee, M.; Gaarslev, C.; Khan, R. Why Do General Practitioners Prescribe Antibiotics for Upper Respiratory Tract Infections to Meet Patient Expectations: A Mixed Methods Study. BMJ Open 2016, 6, e012244. [Google Scholar] [CrossRef] [PubMed]
- Albayrak, A.; Karakaş, N.M.; Karahalil, B. Evaluation of Parental Knowledge, Attitudes and Practices Regarding Antibiotic Use in Acute Upper Respiratory Tract Infections in Children under 18 Years of Age: A Cross-Sectional Study in Turkey. BMC Pediatr. 2021, 21, 554. [Google Scholar] [CrossRef] [PubMed]
- Ndjadi Wembonyama Kasongo, A.; Mukuku, O.; A-Wakamb Kanteng, G.; Ya-Pongombo Shongo, M.; Kabamba Mutombo, A.; Mwembo-A-Nkoy Tambwe, A.; Tshikwej Ngwej, D.; Okitotsho Wembonyama, S.; Numbi Luboya, O. General Practitioners’ Knowledge, Attitudes and Practices on Antibiotic Prescribing for Acute Respiratory Infections in Children in Lubumbashi, Democratic Republic of Congo. J. Pulmonol. Respir. Res. 2020, 4, 011–017. [Google Scholar] [CrossRef]
- Gadomski, A.M. Potential Interventions for Preventing Pneumonia among Young Children: Lack of Effect of Antibiotic Treatment for Upper Respiratory Infections. Pediatr. Infect. Dis. J. 1993, 12, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Gillies, M.; Ranakusuma, A.; Hoffmann, T.; Thorning, S.; McGuire, T.; Glasziou, P.; Del Mar, C. Common Harms from Amoxicillin: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials for Any Indication. CMAJ 2015, 187, E21–E31. [Google Scholar] [CrossRef] [PubMed]
- Romandini, A.; Pani, A.; Schenardi, P.A.; Pattarino, G.A.C.; De Giacomo, C.; Scaglione, F. Antibiotic Resistance in Pediatric Infections: Global Emerging Threats, Predicting the Near Future. Antibiotics 2021, 10, 393. [Google Scholar] [CrossRef]
- European Scientific Cooperative on Phytotherapy ESCOP: 30 Years Building a Scientific Consensus on Herbal Medicines. Available online: https://escop.com/about-escop/ (accessed on 12 September 2023).
- Ajebli, M.; Eddouks, M. Phytotherapy of Hypertension: An Updated Overview. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 812–839. [Google Scholar] [CrossRef]
- Tumpang, M.A.; Ramli, N.A.; Hussain, Z. Phytomedicines Are Efficient Complementary Therapies for the Treatment of Atopic Dermatitis: A Review of Mechanistic Insight and Recent Updates. Curr. Drug Targets 2018, 19, 674–700. [Google Scholar] [CrossRef]
- Lee, G.; Bae, H. Therapeutic Effects of Phytochemicals and Medicinal Herbs on Depression. Biomed. Res. Int. 2017, 2017, 6596241. [Google Scholar] [CrossRef]
- Mancak Karakuş, M.; Tapısız, A.; Mutlu Karakaş, N.; Deniz, M.; Koca Çalışkan, U. Use of Herbal Tea/Herbal Preparations for Children with Symptoms of Viral Upper Respiratory Infections. Turk. J. Pharm. Sci. 2023, 20, 8–15. [Google Scholar] [CrossRef]
- Jund, R.; Mondigler, M.; Stammer, H.; Stierna, P.; Bachert, C. Herbal Drug BNO 1016 Is Safe and Effective in the Treatment of Acute Viral Rhinosinusitis. Acta Otolaryngol. 2015, 135, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Anheyer, D.; Cramer, H.; Lauche, R.; Saha, F.J.; Dobos, G. Herbal Medicine in Children with Respiratory Tract Infection: Systematic Review and Meta-Analysis. Acad. Pediatr. 2018, 18, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Kardos, P.; Lehmacher, W.; Zimmermann, A.; Brandes-Schramm, J.; Funk, P.; Matthys, H.; Kamin, W. Effects of Pelargonium Sidoides Extract EPs 7630 on Acute Cough and Quality of Life—A Meta-Analysis of Randomized, Placebo-Controlled Trials. Multidiscip. Respir. Med. 2022, 17, 868. [Google Scholar] [CrossRef] [PubMed]
- McCaig, L.F.; Besser, R.E.; Hughes, J.M. Trends in Antimicrobial Prescribing Rates for Children and Adolescents. JAMA 2002, 287, 3096–3102. [Google Scholar] [CrossRef]
- Mainous, A.G.; Hueston, W.J.; Davis, M.P.; Pearson, W.S. Trends in Antimicrobial Prescribing for Bronchitis and Upper Respiratory Infections among Adults and Children. Am. J. Public. Health 2003, 93, 1910–1914. [Google Scholar] [CrossRef]
- Grijalva, C.G.; Nuorti, J.P.; Griffin, M.R. Antibiotic Prescription Rates for Acute Respiratory Tract Infections in US Ambulatory Settings. JAMA 2009, 302, 758–766. [Google Scholar] [CrossRef]
- Meropol, S.B.; Chen, Z.; Metlay, J.P. Reduced Antibiotic Prescribing for Acute Respiratory Infections in Adults and Children. Br. J. Gen. Pract. 2009, 59, e321–e328. [Google Scholar] [CrossRef]
- Neumark, T.; Brudin, L.; Engstrom, S.; Molstad, S. Trends in Number of Consultations and Antibiotic Prescriptions for Respiratory Tract Infections between 1999 and 2005 in Primary Healthcare in Kalmar County, Southern Sweden. Scand. J. Prim. Health Care 2009, 27, 18–24. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Baddley, J.W.; Wang, H.E. Antibiotic Utilization for Acute Respiratory Tract Infections in U.S. Emergency Departments. Antimicrob. Agents Chemother. 2014, 58, 1451–1457. [Google Scholar] [CrossRef]
- Lee, M.-L.; Cho, C.-Y.; Hsu, C.-L.; Chen, C.-J.; Chang, L.-Y.; Lee, Y.-S.; Soong, W.-J.; Jeng, M.-J.; Wu, K.-G. Recent Trends in Antibiotic Prescriptions for Acute Respiratory Tract Infections in Pediatric Ambulatory Care in Taiwan, 2000–2009: A Nationwide Population-Based Study. J. Microbiol. Immunol. Infect. 2016, 49, 554–560. [Google Scholar] [CrossRef]
- Korppi, M.; Heikkilä, P.; Palmu, S.; Huhtala, H.; Csonka, P. Antibiotic Prescribing for Children with Upper Respiratory Tract Infection: A Finnish Nationwide 7-Year Observational Study. Eur. J. Pediatr. 2022, 181, 2981–2990. [Google Scholar] [CrossRef] [PubMed]
- Korppi, M.; Heikkilä, P.; Palmu, S.; Huhtala, H.; Csonka, P. Antibiotic Prescriptions for Children with Lower Respiratory Tract Infections Fell from 2014 to 2020, but Misuse Was Still an Issue. Acta Paediatr. 2022, 111, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.-J.; Kruppert, S.; Kostev, K. Basic Characteristics and Representativeness of the German Disease Analyzer Database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Andrew, J.D.; Tandon, O.P.; Turk, D.C. Acute Epiglottitis: Challenge of a Rarely Recognized Emergency. Br. Med. J. 1968, 3, 524–526. [Google Scholar] [CrossRef]
- Baillie, E.J.; Merlo, G.; Magin, P.; Tapley, A.; Mulquiney, K.J.; Davis, J.S.; Fielding, A.; Davey, A.; Holliday, E.; Ball, J.; et al. Antibiotic Prescribing for Upper Respiratory Tract Infections and Acute Bronchitis: A Longitudinal Analysis of General Practitioner Trainees. Fam. Pract. 2022, 39, 1063–1069. [Google Scholar] [CrossRef]
- Akmatov, M.K.; Kohring, C.; Dammertz, L.; Heuer, J.; Below, M.; Bätzing, J.; Holstiege, J. The Effect of the COVID-19 Pandemic on Outpatient Antibiotic Prescription Rates in Children and Adolescents—A Claims-Based Study in Germany. Antibiotics 2022, 11, 1433. [Google Scholar] [CrossRef] [PubMed]
- Linde, K.; Jonas, W.B.; Melchart, D.; Willich, S. The Methodological Quality of Randomized Controlled Trials of Homeopathy, Herbal Medicines and Acupuncture. Int. J. Epidemiol. 2001, 30, 526–531. [Google Scholar] [CrossRef]
- Kostev, K.; Völp, A.; Ludwig, F.; Strehl, C.; Seifert, G. Association between Ivy Leaves Dry Extract EA 575 Prescriptions and Antibiotic Use, Sick Leave Duration, and Repeated Infections in Adult Patients. Postgrad. Med. 2022, 134, 333–340. [Google Scholar] [CrossRef]
- Martin, D.; Konrad, M.; Adarkwah, C.C.; Kostev, K. Reduced Antibiotic Use after Initial Treatment of Acute Respiratory Infections with Phytopharmaceuticals—A Retrospective Cohort Study. Postgrad. Med. 2020, 132, 412–418. [Google Scholar] [CrossRef]
- Belongia, E.A.; Schwartz, B. Strategies for Promoting Judicious Use of Antibiotics by Doctors and Patients. BMJ 1998, 317, 668–671. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | 2013 | 2018 | 2022 | p-Value a |
|---|---|---|---|---|
| N | 120,894 | 116,844 | 127,821 | Not applicable |
| Age (in years) | ||||
| Median (interquartile range) | 5.0 (5.0) | 5.0 (5.0) | 5.0 (5.0) | <0.001 |
| 2–5 | 64,283 (53.2) | 63,902 (54.7) | 66,584 (52.1) | <0.001 |
| 6–12 | 56,611 (46.8) | 52,942 (45.3) | 61,237 (47.9) | |
| Sex | ||||
| Female | 58,248 (48.2) | 55,988 (47.9) | 60,817 (47.6) | 0.011 |
| Male | 62,646 (51.8) | 60,856 (52.1) | 67,004 (52.4) | |
| Diagnosis | ||||
| Acute nasopharyngitis (common cold) (ICD-10 code: J00) | 15,955 (13.2) | 18,105 (15.5) | 18,774 (14.7) | <0.001 |
| Acute sinusitis (ICD-10 code: J01) | 1680 (1.4) | 1202 (1.0) | 772 (0.6) | <0.001 |
| Acute pharyngitis (ICD-10 code: J02) b | 18,959 (15.7) | 16,845 (14.4) | 14,309 (11.2) | <0.001 |
| Acute tonsillitis (ICD-10 code: J03) c | 19,134 (15.8) | 15,016 (12.9) | 12,716 (9.9) | <0.001 |
| Acute laryngitis and tracheitis (ICD-10 code: J04) | 10,539 (8.7) | 9414 (8.1) | 10,491 (8.2) | <0.001 |
| Acute upper respiratory infections of multiple and unspecified sites (ICD-10 code: J06) | 79,099 (65.4) | 78,939 (67.6) | 90,845 (71.1) | <0.001 |
| Acute bronchitis (ICD-10 code: J20) | 25,761 (21.3) | 19,729 (16.9) | 19,224 (15.0) | <0.001 |
| Diagnosis | 2013 | 2018 | 2022 | p-Value for the Difference between 2013 and 2018 a | p-Value for the Difference between 2018 and 2022 a |
|---|---|---|---|---|---|
| In children aged 2–12 years | |||||
| Acute nasopharyngitis | 10.1 | 8.6 | 6.4 | <0.001 | <0.001 |
| Acute sinusitis | 32.9 | 29.1 | 27.1 | 0.030 | 0.325 |
| Acute pharyngitis | 21.6 | 19.7 | 18.1 | <0.001 | <0.001 |
| Acute tonsillitis | 72.1 | 72.2 | 66.7 | 0.936 | <0.001 |
| Acute laryngitis and tracheitis | 9.3 | 8.0 | 8.2 | 0.002 | 0.723 |
| Acute upper respiratory infections of multiple and unspecified sites | 9.0 | 8.1 | 6.6 | 0.508 | <0.001 |
| Acute bronchitis | 28.9 | 24.4 | 17.5 | <0.001 | <0.001 |
| In children aged 2–5 years | |||||
| Acute nasopharyngitis | 11.0 | 8.0 | 5.8 | <0.001 | <0.001 |
| Acute sinusitis | 26.8 | 25.6 | 19.4 | 0.714 | 0.112 |
| Acute pharyngitis | 24.0 | 20.7 | 19.8 | <0.001 | 0.163 |
| Acute tonsillitis | 73.5 | 72.4 | 67.3 | 0.108 | <0.001 |
| Acute laryngitis and tracheitis | 8.9 | 7.2 | 7.7 | <0.001 | 0.287 |
| Acute upper respiratory infections of multiple and unspecified sites | 9.8 | 8.7 | 5.9 | <0.001 | <0.001 |
| Acute bronchitis | 29.9 | 23.4 | 16.2 | <0.001 | <0.001 |
| In children aged 6–12 years | |||||
| Acute nasopharyngitis | 8.9 | 9.4 | 7.1 | 0.261 | <0.001 |
| Acute sinusitis | 35.2 | 30.2 | 30.0 | 0.015 | 0.927 |
| Acute pharyngitis | 19.5 | 18.8 | 16.7 | 0.196 | <0.001 |
| Acute tonsillitis | 70.6 | 71.9 | 65.9 | 0.078 | <0.001 |
| Acute laryngitis and tracheitis | 9.8 | 9.2 | 8.7 | 0.329 | 0.491 |
| Acute upper respiratory infections of multiple and unspecified sites | 8.0 | 9.5 | 7.3 | <0.001 | <0.001 |
| Acute bronchitis | 27.1 | 26.4 | 19.7 | 0.280 | <0.001 |
| Diagnosis | 2013 | 2018 | 2022 | p-Value for the Difference between 2013 and 2018 a | p-Value for the Difference between 2018 and 2022 a |
|---|---|---|---|---|---|
| In children aged 2–12 years | |||||
| Acute nasopharyngitis | 14.2 | 21.4 | 19.0 | <0.001 | <0.001 |
| Acute sinusitis | 45.8 | 57.0 | 55.1 | <0.001 | 0.397 |
| Acute pharyngitis | 4.8 | 7.8 | 7.7 | <0.001 | 0.721 |
| Acute tonsillitis | 2.8 | 4.0 | 3.9 | <0.001 | 0.510 |
| Acute laryngitis and tracheitis | 8.2 | 12.3 | 11.2 | <0.001 | 0.010 |
| Acute upper respiratory infections of multiple and unspecified sites | 12.5 | 17.9 | 17.3 | <0.001 | 0.003 |
| Acute bronchitis | 8.5 | 12.9 | 12.7 | <0.001 | 0.472 |
| In children aged 2–5 years | |||||
| Acute nasopharyngitis | 15.3 | 21.0 | 15.9 | <0.001 | <0.001 |
| Acute sinusitis | 46.4 | 54.4 | 52.1 | 0.038 | 0.623 |
| Acute pharyngitis | 5.3 | 7.5 | 6.2 | <0.001 | 0.002 |
| Acute tonsillitis | 2.7 | 3.7 | 3.5 | <0.001 | 0.370 |
| Acute laryngitis and tracheitis | 9.4 | 12.5 | 10.0 | <0.001 | <0.001 |
| Acute upper respiratory infections of multiple and unspecified sites | 13.6 | 17.5 | 15.0 | <0.001 | <0.001 |
| Acute bronchitis | 8.2 | 11.3 | 10.4 | <0.001 | 0.020 |
| In children aged 6–12 years | |||||
| Acute nasopharyngitis | 12.7 | 22.0 | 22.6 | <0.001 | 0.404 |
| Acute sinusitis | 45.6 | 57.8 | 56.2 | <0.001 | 0.543 |
| Acute pharyngitis | 4.3 | 8.1 | 9.1 | <0.001 | 0.034 |
| Acute tonsillitis | 2.8 | 4.4 | 4.4 | <0.001 | 0.974 |
| Acute laryngitis and tracheitis | 6.6 | 12.1 | 12.6 | <0.001 | 0.481 |
| Acute upper respiratory infections of multiple and unspecified sites | 11.2 | 18.4 | 19.9 | <0.001 | <0.001 |
| Acute bronchitis | 9.2 | 15.9 | 16.7 | <0.001 | 0.173 |
| Diagnosis | Pearson Correlation Coefficient | p-Value |
|---|---|---|
| Acute nasopharyngitis | −0.04 | 0.886 |
| Acute sinusitis | −0.27 | <0.001 |
| Acute pharyngitis | 0.05 | 0.310 |
| Acute tonsillitis | 0.03 | 0.587 |
| Acute laryngitis and tracheitis | −0.07 | 0.187 |
| Acute upper respiratory infections of multiple and unspecified sites | 0.03 | 0.477 |
| Acute bronchitis | −0.12 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostev, K.; van den Boom, L.; Tanislav, C.; Jacob, L. Changes in the Prescription of Antibiotics and Phytopharmaceuticals in Children Treated for Acute Upper and Lower Respiratory Tract Infections in Pediatric Practices in Germany in 2013, 2018, and 2022. Antibiotics 2023, 12, 1491. https://doi.org/10.3390/antibiotics12101491
Kostev K, van den Boom L, Tanislav C, Jacob L. Changes in the Prescription of Antibiotics and Phytopharmaceuticals in Children Treated for Acute Upper and Lower Respiratory Tract Infections in Pediatric Practices in Germany in 2013, 2018, and 2022. Antibiotics. 2023; 12(10):1491. https://doi.org/10.3390/antibiotics12101491
Chicago/Turabian StyleKostev, Karel, Louisa van den Boom, Christian Tanislav, and Louis Jacob. 2023. "Changes in the Prescription of Antibiotics and Phytopharmaceuticals in Children Treated for Acute Upper and Lower Respiratory Tract Infections in Pediatric Practices in Germany in 2013, 2018, and 2022" Antibiotics 12, no. 10: 1491. https://doi.org/10.3390/antibiotics12101491