Abstract
Background: A correct approach to recurrent urinary tract infections (rUTIs) is an important pillar of antimicrobial stewardship. We aim to define an Artificial Neural Network (ANN) for predicting the clinical efficacy of the empiric antimicrobial treatment in women with rUTIs. Methods: We extracted clinical and microbiological data from 1043 women. We trained an ANN on 725 patients and validated it on 318. Results: The ANN showed a sensitivity of 87.8% and specificity of 97.3% in predicting the clinical efficacy of empirical therapy. The previous use of fluoroquinolones (HR = 4.23; p = 0.008) and cephalosporins (HR = 2.81; p = 0.003) as well as the presence of Escherichia coli with resistance against cotrimoxazole (HR = 3.54; p = 0.001) have been identified as the most important variables affecting the ANN output decision predicting the fluoroquinolones-based therapy failure. A previous isolation of Escherichia coli with resistance against fosfomycin (HR = 2.67; p = 0.001) and amoxicillin-clavulanic acid (HR = 1.94; p = 0.001) seems to be the most influential variable affecting the output decision predicting the cephalosporins- and cotrimoxazole-based therapy failure. The previously mentioned Escherichia coli with resistance against cotrimoxazole (HR = 2.35; p < 0.001) and amoxicillin-clavulanic acid (HR = 3.41; p = 0.007) seems to be the most influential variable affecting the output decision predicting the fosfomycin-based therapy failure. Conclusions: ANNs seem to be an interesting tool to guide the antimicrobial choice in the management of rUTIs at the point of care.
1. Introduction
Antibiotic resistance is one of the biggest public health challenges for clinicians and health care systems worldwide, with high costs and a high risk of death due to antibiotic-resistant infection [1,2]. Antibiotic resistance is a particular challenge in urology, due to the high prevalence of bacterial infections among urological patients, and because many urological conditions increase the risk of infections [3,4,5]. In this sense, several authors have demonstrated that ascertaining a correct approach to the management of symptomatic recurrences is a key step towards improving adherence to antimicrobial stewardship principles, due to the rate of rUTIs’ treatment failure (about 35%) [6]. The management of UTIs and the prescription of antibiotics in urology should be performed in accordance with international guidelines’ recommendations and the accurate evaluation of all risk factors impacting on the risk of antimicrobial resistance [7,8]. During the last decade, we have witnessed raised interest in tools able to process large datasets and perform cognitive tasks that facilitate clinical decision-making in urology [7]. In recent years, artificial intelligence (AI) has been progressively applied in different medical specialties, improving either performance of major clinical diagnostic procedures or adherence to recommended treatments [9]. Several authors have demonstrated the efficacy of AI in predicting clinical outcomes in oncological as well as non-oncological diseases [7,10,11,12]. An Artificial Neural Network (ANN) is a machine learning model that allows a computer system to learn from clinical experiences and predict an event from raw data or independent variables. The ANN is based on connections between nodes (the so-called artificial neurons) analogous to brain synapses. ANNs may identify non-linear relationship variables, representing the ideal tool for bridging the gap between linear statistical models and human factors. In brief, ANNs are based on a collection of connected units called “artificial neurons”; each connection, as well as the synapses in a biological brain model, can transmit signals to other neurons. The signal transmission is controlled by the interconnections between the artificial neurons. Artificial neurons may have a threshold such that a signal is sent from one to the other only if the aggregated signal crosses that threshold [10]. In this scenario, we hypothesized that ANNs could be applied as a guide for antimicrobial choice in patients with recurrent UTIs (rUTIs). The aim of this study is to evaluate a neural network made to predict the clinical efficacy of the empirical antibiotic treatment of symptomatic UTI episodes in a large cohort of women affected by rUTIs.
2. Results
Of 1234 patients, 1043 patients were finally selected and enrolled in this study, while 191 were excluded for missing data. The patients’ mean age was 39.6 years (SD ± 7.1). All patients’ demographics, clinical and microbiological data at baseline are described in Table 1.

Table 1.
Patient anamnestic, clinical and microbiological characteristics.
2.1. Clinical and Microbiological Data
The mean number of episodes per year was 5.1 (SD ± 1.2). The mean rate of treatment failure was 42% in the 3 month period before enrollment. No differences in terms of anamnestic, clinical or microbiological data have been reported between the two groups (Table 1). Among 1043 patients included in the analysis, 1912 strains were isolated. The most common isolated strains at the baseline evaluation were Escherichia coli (1202; 62.9%), followed by Klebsiella spp. (374; 19.6%) and Enterococcus spp. (199; 10.4%). All microbiological data are displayed in Table 1.
2.2. Antibiotic Susceptibility Profiles and Antibiotic Resistance Patterns
The overall mean resistance rate among Escherichia coli to ciprofloxacin was 34.7% (418/1202), to cephalexin 8.9% (108/1202) and to fosfomycin 6.6% (80/1202). Finally, 513 out of the 1912 (26.8%) strains were considered as cefpodoxime-resistant and belonged to the ‘ESBL subgroup’. All data about antibiotic susceptibility profiles are detailed in Table 2.
Table 2.
Antibiotic resistance of the most common isolated strains to the tested antibiotics.
2.3. Univariate and Multivariate Analyses
Multivariate analysis identified the following parameters as the most important variables affecting the output decision in predicting fluoroquinolones-based therapy failure: previous use of fluoroquinolones (yes, HR = 4.23, p = 0.008) and cephalosporins (yes, HR = 2.81, p = 0.003) in the last three months, and the presence of Escherichia coli with resistance against cotrimoxazole (yes, HR = 3.54, p = 0.001). Finally, the previously mentioned Escherichia coli with resistance against cotrimoxazole (yes, HR = 2.35, p < 0.001) and amoxicillin-clavulanic acid (yes, HR = 3.41, p = 0.007) was the most influential variable affecting the output decision in predicting the fosfomycin-based therapy failure. The previous use of fosfomycin in the last 3 months was not identified as a variable affecting the output decision in predicting fosfomycin therapy failure. No significant differences are reported stratifying data in terms of isolated strains. All univariate and multivariate analysis results are displayed in Table 3.
Table 3.
Univariate and multivariate analysis results of laboratory and clinical factors affecting the output decision in predicting treatment outcome and treatment failure.
2.4. Artificial Neural Network Analysis
After the completion of the ANN learning and prediction processes, our neural network showed a sensitivity of 87.8% and specificity of 97.3% in predicting the clinical efficacy of empirical therapy. The area under the ROC curve was 0.867 (Figure 1). The calibration plot of predicted probabilities compared with actual probabilities is displayed in Figure 2. ANN analysis reported a high correlation between expected and observed data (train phase: Pearson’s coefficient, 81.5—Root Mean Square error, 1.3; test phase: Pearson’s coefficient, 79.7—Root Mean Square error, 1.2). Moreover, the ANN analysis shows a prediction with an overall accuracy of 83.63%, and the previous use of fluoroquinolones and cephalosporins in the last three months as well as the presence of E. coli with resistance against cotrimoxazole to be the most influential variables affecting the fluoroquinolone-based therapy failure. The presence of Escherichia coli with resistance to fosfomycin and amoxicillin-clavulanic acid has not been confirmed to be an influential variable affecting the output decision in predicting the cephalosporins and cotrimoxazole-based therapy failure in the ANN analysis. Finally, the previously mentioned Escherichia coli with resistance against cotrimoxazole (yes, HR = 2.35, p < 0.001) and resistance against amoxicillin-clavulanic acid (yes, HR = 3.41, p = 0.007) have been identified as the most important variables affecting the ANN output decision predicting the fosfomycin-based therapy failure.
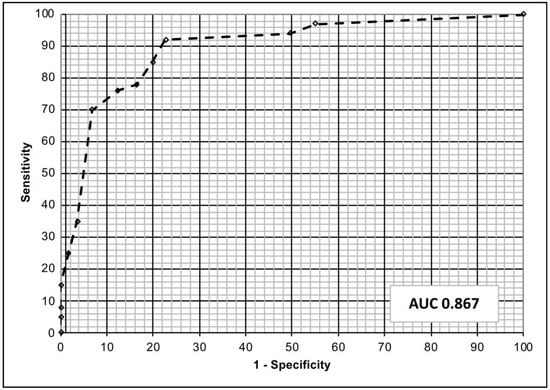
Figure 1.
The figure shows the discriminatory performance of our model for predicting the outcome of empirical antibiotic treatment of uncomplicated cystitis. The area under the receiver operating curve (ROC) was 0.867.
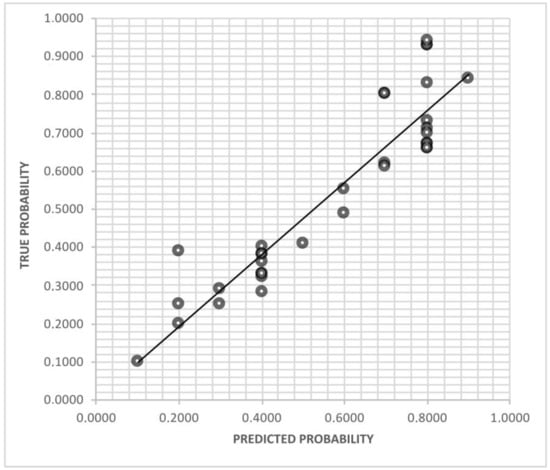
Figure 2.
The figure shows the calibration plot of predicted probabilities compared with actual probabilities.
3. Discussion
Here, we demonstrated the feasibility and reliability of ANN applications to guide antimicrobial choice in the empiric treatment of uncomplicated cystitis in everyday clinical practice. The ANN’s performance was good when predicting recurrence in patients with rUTIs. We showed that the previous use of a specific class of antibiotic is not a risk factor for developing bacterial resistance to the same class (except for the fluoroquinolones), but instead the most important risk factor for predicting resistance is the use of other classes of antibiotics. This is a new approach to the treatment of rUTIs.
3.1. Results in the Light of Current Knowledge: Nomogram and ANN
Proper data classification and critical management analysis represent an exponentially growing, unmet need in the area of rUTIs. Advances in pharmacological treatment, microbiological pathways and increased antibiotic resistance have contributed to the generation of Big Data in this complex scenario. Due to this increased availability of representative variables, urologists continuously face new challenges when synthesizing information in order to develop accurate diagnosis, tailored treatment plans and outcome prediction in patients affected by rUTIs [5]. Nevertheless, the development of computer-based prediction and decision support models has boosted improvements in the management of rUTIs across different healthcare profiles [13]. Current examples are nomograms or calculators that have been introduced in the clinical management of patients with rUTIs [13,14,15,16]. Recently, Ozkan et al. demonstrated that a model based on an ANN is also a successful medical decision-support system [13] for UTIs with complex symptoms, and the use of this tool is associated with a lower diagnosis cost and shorter diagnosis time [13]. In this context, our study showed promising findings. By using ANN software, the AI showed a sensitivity of 87.8% and specificity of 97.3% in predicting clinical and microbiological efficacy of prescribed antimicrobial medication at a 1 month follow-up.
3.2. Results in the Light of Current Knowledge: Previous Antibiotic Exposure and Resistances
Following Cox regression analysis, previous use of fluoroquinolones or cephalosporins were the only significant variables affecting the output decision predicting the fluoroquinolones-based therapy failure in the last three-month period of the identification of Escherichia coli strain resistance to cotrimoxazole. Moreover, the presence of a previous Escherichia coli infection resistant to either fosfomycin or amoxicillin-clavulanic acid in at least one antibiogram were both indicators of cephalosporins- and cotrimoxazole-based therapy failure. Based on Cox regression analysis, we demonstrated that among all standard clinical and microbiological variables, only the previous use of different antibiotic types was an independent predictor of clinical failure. These data are comparable with the results of a previously published series. Evident disparities between linear statistical or mathematical analysis may justify results obtained in our model, as either rUTIs or a progression to more severe infectious diseases (e.g., pyelonephritis or sepsis) may be related to a complex network of anatomical or clinical variables not available in our dataset. Despite this, the ANN showed the ability to analyze a non-linear relationship, by using multiple layers of interconnected nodes with an adequate accuracy. According to our series, previous microbiological data results seem to have a significant prognostic role in the determination of antibiotic selection. Among rUTIs, only patients prone to multiple resistances to a single Escherichia coli strain could benefit from a follow-up with strict observations. The optimal follow-up schedule of rUTIs should not be planned only on the basis of clinical and microbiological variables, rather it should consider the complex interactions between multiple features included in our system. We previously believed that only a small number of rUTIs which reported multiple previous antibiotic treatments should undergo a restrictive follow-up with frequent and more invasive instrumental diagnostic methodologies. However, future studies with a closer follow-up control to check microbiological eradication should be planned to test this hypothesis. The decision to include only adult women in this study is based on a higher incidence of rUTIs in this specific population. Considering their intrinsic anatomical predisposition, adult women must be treated properly to avoid recurrences, severe complications and unnecessary morbidity. Moreover, as highlighted by Cai et al., clinical management shows poor adherence to current antibiotic stewardship, with a subsequent high rate of overdiagnosis and overtreatment [5]. We argue that the use of an ANN enhances antibiotic stewardship adherence in follow-up decision making for this population of patients. Recently, Schinkel et al. developed a machine learning model for predicting blood culture outcomes highlighting the usefulness of learning machines for improving antimicrobial stewardship in a hospital setting [17]. Finally, Yelin et al. demonstrated that the combination of clinical and microbiological parameters by using a learning machine reduced the risk of mismatched treatment when compared with the current standard of care [18]. However, several legal issues should be considered and discussed in the future [19]. In analogy to previous reports, our findings encourage the use of mathematical applications to improve the management of rUTIs in everyday clinical practice [11,20]. We demonstrated the feasibility and reliability of ANN applications in rUTIs, reporting good accuracy in antibiotic selection and hence an improved antibiotic stewardship. If our findings are confirmed in future studies, ANNs should be regarded as a valuable tool to improve the management of patients with uncomplicated UTIs, prevent antimicrobial resistance and improve antimicrobial stewardship. Finally, the findings of this research provide an easy-to-use and low-cost tool for improving our adherence to the principles of antibiotic stewardship in everyday clinical practice. The costs are associated with the software use and the ANN application, as reported by other authors [21].
3.3. Strengths and Limitations of This Study
The ANN represented a quick methodology to support the management of patients with rUTIs by computing a combination of established prognostic factors, e.g., previous use of any antibiotics in the last three months and urinary culture results that are used in everyday urological practice. Although it is supported by a large cohort of women, this study has some limitations. Firstly, the characteristics of the patient population. We enrolled only women affected by a recurrent and uncomplicated UTI. This cohort of patients is, however, very common in everyday clinical practice and these patients undergo several antimicrobial treatments and have a high risk of recurrence. We believe this feature explains the prevalence of ESBL strains, which is 26.8%. The suboptimal follow-up timeframe in this specific patients’ cohort remains to be resolved in future studies.
4. Materials and Methods
4.1. Study Design, Population and Data Source
We conducted a retrospective study including 1043 consecutive patients who had undergone antimicrobial treatment for uncomplicated cystitis between January 2012 and December 2020, at two referral urological centers. Each patient underwent antimicrobial therapy in accordance with the recommendations of EAU guidelines on urological infections [7]. All data were prospectively collected in a dedicated database. All data about previous use of antibiotics and antibiograms were included in the analysis together with clinical follow-up data. We analyzed the importance of bacterial strain, susceptibility and previous antibiotic use for clinical efficacy. Data were analyzed by using the commercially available software program NeuralWorks (NeuralWare, version 3.2, ©Solvusoft Corporation, Carnegie, PA, USA, 2011–2022), as reported by Cai et al. [11]. The results of the ANN were compared with the follow-up data in order to test the feasibility and reliability of AI applications to guide antimicrobial choice in patients with recurrent cystitis.
4.2. Inclusion and Exclusion Criteria
We considered all women >18 years affected by clinically and microbiologically confirmed recurrent cystitis for the enrolment. Recurrent cystitis was defined as three episodes of a UTI in the previous 12 months, or two episodes in the previous six months [7]. Only women who tested positive for uropathogens in two or more consecutive cultures (colony-forming units ≥105/mL) were included and analyzed. In line with Cai et al., the following characteristics were considered as exclusion criteria: major concomitant diseases, upper urinary tract congenital abnormalities or stones and sexually transmitted infections [22].
4.3. Microbiological Considerations, Follow-Up Evaluation and Outcome
All microbiological and laboratory analyses were performed as previously described [22,23,24]. In particular, the cut-off for significant pathogenic growth was considered ≥105 CFU/mL for the microbiological diagnosis of UTIs [22,24]. Fosfomycin susceptibilities were determined using both the CLSI agar dilution and disk diffusion reference methods as well as using an E-test, in line with Karlowsky J.A. [25] and Tutone M. [26]. Moreover, in line with Tutone et al., isolates resistant to cefpodoxime were inferred to be ESBL-producers [26]. Here, we considered data of the first follow-up (T1). In line with Cai et al., all patients underwent a clinical assessment and microbiological analyses at baseline (T0) and during a follow-up at 1 month (T1) [22]. At the follow-up evaluation, all women underwent urological and midstream urine culture evaluation. The outcome of interest was clinical cure, defined as symptom relief and return to a pre-UTI performance status. Treatment failure was defined as evidence of microbiological colonization with at least 105 Colony Forming Units per milliliter (CFUs/mL) of a single uropathogen in the midstream urine culture associated with the persistence of lower urinary tract symptoms [22,27,28].
4.4. Statistical Analysis and Artificial Neural Networks
To evaluate the correlation between the different parameters we used Pearson’s coefficient and Fisher’s exact test to assess the statistical significance with p < 0.05 accepted as significant. Moreover, we used Bonferroni’s correction as well as an ANOVA test for a univariate analysis and the log-rank test (Mantel Cox) for a multivariate analysis. We used the Cox proportional hazard regression model to calculate the hazard ratio (HR) with the 95% confidence interval (95% CI). The best cut-off value, in the ANN analysis, was tested by the receiver operating characteristic curve (ROC). The efficacy of the ANN in guiding the antimicrobial choice in the management of recurrent cystitis was tested with accuracy, sensitivity, specificity, positive predictive value and negative predictive value. The error between corresponding pairs of values in two series of values has been evaluated by the Root Mean Square. The ANN methodology and data analysis were described by Cai et al. [11]. All statistical analyses were performed using SPSS 22 for Apple-Macintosh (SPSS, Inc. Chicago, IL, USA). In the present study we evaluated the impact of previous use of antibiotics (all antibiotic classes) in the last three months and the previous resistance (all antibiotic classes) extracted by the last microbiological analysis (antibiogram). All factors were finally used as input parameters (input neurons) to the ANN. All characteristics of the ANN structure were the same as described by Cai et al. [11]. Of 1043 selected patients, 725 (69.5%) were used to train the system, while 318 (30.5%) were used for the testing phase. We did not perform the re-training of the network after the first training phase. No standard logistic regression was performed to compare these results to those of the ANN analysis, because the ANN analysis produces more accurate results than the LR and other standard statistical analyses [29].
4.5. Ethical Considerations
This study was planned with a retrospective design; for this reason, Ethical Committee approval was not required in accordance with Italian law. However, all anamnestic, clinical and laboratory data containing sensitive information about patients were de-identified to ensure the analysis of anonymous data only. The de-identification process was performed by non-medical staff by means of dedicated software [30]. The study was conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki.
5. Conclusions
We demonstrated that an ANN is a feasible and reliable instrument to guide antimicrobial choice in the empiric treatment of uncomplicated cystitis in clinical urological practice, and to predict the recurrence of a UTI. Compared to traditional linear statistical approaches, the ANN provided, in terms of decision-making and prediction accuracy, a significant benefit in terms of adherence to antibiotic stewardship principles in the management of rUTIs in adult women. The ANN enables the clinician to consider more variables of importance for antimicrobial stewardship and has the potential to become an important aid in the management of rUTIs. The isolation of Escherichia coli with resistance against cotrimoxazole is the most influential variable for predicting the fluoroquinolones-based therapy failure, and the resistance against cotrimoxazole and amoxicillin-clavulanic acid predicts fosfomycin-based therapy failure.
Author Contributions
T.C., M.R. and G.L. conceptualized this study; T.C., S.M. and A.B. curated the data; T.C., U.A. and F.P. collectively investigated the data and decided on the methodology to be used; T.C. and S.M. conducted the formal analyses; T.C., U.A., L.C., L.M. and C.T. drafted the original manuscript; L.G., C.T., F.M.E.W., T.E.B.J. and A.P. reviewed, edited, and agreed the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was planned with a retrospective design; for this reason, Ethical Committee approval was not required in accordance with Italian law. However, all anamnestic, clinical and laboratory data containing sensitive information about patients were de-identified to ensure analysis of anonymous data only. The study was, however, conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki.
Informed Consent Statement
Not applicable.
Data Availability Statement
Due to ethical restrictions, clinical data are not available.
Acknowledgments
We want to thank all members of Santa Chiara regional Hospital Department of Urology and the Department of Microbiology for their support in data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wagenlehner, F.M.E.; Bjerklund Johansen, T.E.; Cai, T.; Koves, B.; Kranz, J.; Pilatz, A.; Tandogdu, Z. Epidemiology, definition and treatment of complicated urinary tract infections. Nat. Rev. Urol. 2020, 17, 586–600. [Google Scholar] [CrossRef] [PubMed]
- Batista, A.D.; Rodrigues, D.A.; Figueiras, A.; Zapata-Cachafeiro, M.; Roque, F.; Herdeiro, M.T. Antibiotic Dispensation without a Prescription Worldwide: A Systematic Review. Antibiotics 2020, 9, 786. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Stamm, W.E. Increasing antimicrobial resistance and the management of uncomplicated community-acquired urinary tract infections. Ann. Intern. Med. 2001, 135, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Urinary tract infection syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. N. Am. 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Cai, T.; Tamanini, I.; Collini, L.; Brugnolli, A.; Migno, S.; Mereu, L.; Tateo, S.; Pilatz, A.; Rizzo, M.; Liguori, G.; et al. Management of Recurrent Cystitis in Women: When Prompt Identification of Risk Factors Might Make a Difference. Eur. Urol. Focus 2022, 8, 1476–1482. [Google Scholar] [CrossRef]
- Tandan, M.; Thapa, P.; Maharjan, P.; Bhandari, B. Impact of Antimicrobial Stewardship Program on Antimicrobial Resistant and Prescribing in Nursing Home: A Systematic Review and Meta-analysis. J. Glob. Antimicrob. Resist. 2022, 29, 74–87. [Google Scholar] [CrossRef]
- EAU. European Association of Urology Guidelines on Urological Infections, Update 2019. Available online: http://uroweb.org/guideline/urological-infections/ (accessed on 3 March 2022).
- Kwok, M.; McGeorge, S.; Mayer-Coverdale, J.; Graves, B.; Paterson, D.L.; Harris, P.N.; Esler, R.; Dowling, C.; Britton, S.; Roberts, M.J. Guideline of guidelines: Management of recurrent urinary tract infections in women. BJU Int. 2022, 130 (Suppl. S3), 11–22. [Google Scholar] [CrossRef]
- Dai, J.C.; Johnson, B.A. Artificial intelligence in endourology: Emerging technology for individualized care. Curr. Opin. Urol. 2022, 32, 379–392. [Google Scholar] [CrossRef]
- Chowdhury, A.S.; Lofgren, E.T.; Moehring, R.W.; Broschat, S.L. Identifying predictors of antimicrobial exposure in hospitalized patients using a machine learning approach. J. Appl. Microbiol. 2019, 128, 688–696. [Google Scholar] [CrossRef]
- Cai, T.; Conti, G.; Nesi, G.; Lorenzini, M.; Mondaini, N.; Bartoletti, R. Artificial intelligence for predicting recurrence-free probability of non-invasive high-grade urothelial bladder cell carcinoma. Oncol. Rep. 2007, 18, 959–964. [Google Scholar]
- Catto, J.W.F.; Linkens, D.A.; Abbod, M.F.; Chen, M.; Burton, J.L.; Feeley, K.M.; Hamdy, F.C. Artificial intelligence in predicting bladder cancer outcome: A comparison of neurofuzzy modeling and artificial neural networks. Clin. Cancer Res. 2003, 9, 4172–4177. [Google Scholar] [CrossRef]
- Ozkan, I.A.; Koklu, M.; Sert, I.U. Diagnosis of urinary tract infection based on artificial intelligence methods. Comput. Methods Programs Biomed. 2018, 166, 51–59. [Google Scholar] [CrossRef]
- Cai, T.; Mazzoli, S.; Migno, S.; Malossini, G.; Lanzafame, P.; Mereu, L.; Tateo, S.; Wagenlehner, F.M.; Pickard, R.S.; Bartoletti, R. Development and validation of a nomogram predicting recurrence risk in women with symptomatic urinary tract infection. Int. J. Urol. 2014, 21, 929–934. [Google Scholar] [CrossRef]
- Lisboa, P.J.; Taktak, A.F. The use of artificial neural networks in decision support in cancer: A systematic review. Neural Netw. 2006, 19, 408–415. [Google Scholar] [CrossRef]
- Fang, N.W.; Chiou, Y.H.; Chen, Y.S.; Hung, C.W.; Yin, C.H.; Chen, J.S. Nomogram for diagnosing acute pyelonephritis in pediatric urinary tract infection. Pediatr. Neonatol. 2022, 63, 380–387. [Google Scholar] [CrossRef]
- Schinkel, M.; Boerman, A.W.; Bennis, F.C.; Minderhoud, T.C.; Lie, M.; Peters-Sengers, H.; Holleman, F.; Schade, R.P.; de Jonge, R.; Wiersinga, W.J.; et al. Diagnostic stewardship for blood cultures in the emergency department: A multicenter validation and prospective evaluation of a machine learning prediction tool. EBioMedicine 2022, 82, 104176. [Google Scholar] [CrossRef]
- Yelin, I.; Snitser, O.; Novich, G.; Katz, R.; Tal, O.; Parizade, M.; Chodick, G.; Koren, G.; Shalev, V.; Kishony, R. Personal clinical history predicts antibiotic resistance of urinary tract infections. Nat. Med. 2019, 25, 1143–1152. [Google Scholar] [CrossRef]
- Hejrati, B.; Fathi, A.; Abdali-Mohammadi, F. A new near-lossless EEG compression method using ANN-based reconstruction technique. Comput. Biol. Med. 2017, 87, 87–94. [Google Scholar] [CrossRef]
- Goździkiewicz, N.; Zwolińska, D.; Polak-Jonkisz, D. The Use of Artificial Intelligence Algorithms in the Diagnosis of Urinary Tract Infections-A Literature Review. J. Clin. Med. 2022, 11, 2734. [Google Scholar] [CrossRef]
- Aznan, A.; Gonzalez Viejo, C.; Pang, A.; Fuentes, S. Rapid Detection of Fraudulent Rice Using Low-Cost Digital Sensing Devices and Machine Learning. Sensors 2022, 22, 8655. [Google Scholar] [CrossRef]
- Cai, T.; Tamanini, I.; Cocci, A.; Maida, F.D.; Caciagli, P.; Migno, S.; Mereu, L.; Tateo, S.; Malossini, G.; Palmieri, A.; et al. Xyloglucan, hibiscus and propolis to reduce symptoms and antibiotics use in recurrent UTIs: A prospective study. Future Microbiol. 2019, 14, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Hooton, T.M.; Scholes, D.; Gupta, K.; Stapleton, A.E.; Roberts, P.L.; Stamm, W.E. Amoxicillin-clavulanate vs ciprofloxacin for the treatment of uncomplicated cystitis in women: A randomized trial. JAMA 2005, 293, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Mazzoli, S.; Cai, T.; Rupealta, V.; Gavazzi, A.; Pagliai, R.C.; Mondaini, N.; Bartoletti, R. Interleukin 8 and anti-Chlamydia trachomatis mucosal IgA as urogenital immunologic markers in patients with C. trachomatis prostatic infection. Eur. Urol. 2007, 51, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Karlowsky, J.A.; Baxter, M.R.; Golden, A.R.; Adam, H.J.; Walkty, A.; Lagacé-Wiens, P.R.; Zhanel, G.G. Use of Fosfomycin Etest to Determine In Vitro Susceptibility of Clinical Isolates of Enterobacterales Other than Escherichia coli, Nonfermenting Gram-Negative Bacilli, and Gram-Positive Cocci. J. Clin. Microbiol. 2021, 59, e0163521. [Google Scholar] [CrossRef] [PubMed]
- Tutone, M.; Bjerklund Johansen, T.E.; Cai, T.; Mushtaq, S.; Livermore, D.M. SUsceptibility and Resistance to Fosfomycin and other antimicrobial agents among pathogens causing lower urinary tract infections: Findings of the SURF study. Int. J. Antimicrob. Agents 2022, 59, 106574. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef]
- Warren, J.W.; Abrutyn, E.; Hebel, J.R.; Johnson, J.R.; Schaeffer, A.J.; Stamm, W.E. Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America (IDSA). Clin. Infect. Dis. 1999, 29, 745–758. [Google Scholar] [CrossRef]
- Abbod, M.F.; Linkens, D.A.; Catto, J.W.; Hamdy, F.C. Comparative study of intelligent models for the prediction of bladder cancer progression. Oncol. Rep. 2006, 15, 1019–1022. [Google Scholar] [CrossRef]
- Neamatullah, I.; Douglass, M.M.; Lehman, L.-W.H.; Reisner, A.; Villarroel, M.; Long, W.J.; Szolovits, P.; Moody, G.B.; Mark, R.G.; Clifford, G.D. Automated de-identification of free-text medical records. BMC Med. Inform. Decis. Mak. 2008, 8, 32. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).