
Analysis of Bacterial Pathogens Causing Complicating HAP in Patients with Secondary Peritonitis

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients with Secondary Peritonitis
2.2. Patients with HAP
2.3. Isolation and Identification of Bacterial Pathogens Causing HAP
2.4. Determination of Resistance to Antibiotics
2.5. Genetic Analysis of Bacterial Pathogens
2.6. Statistical Methods
3. Results
3.1. Bacterial Pathogens Causing HAP
3.2. Resistance to Antibiotics
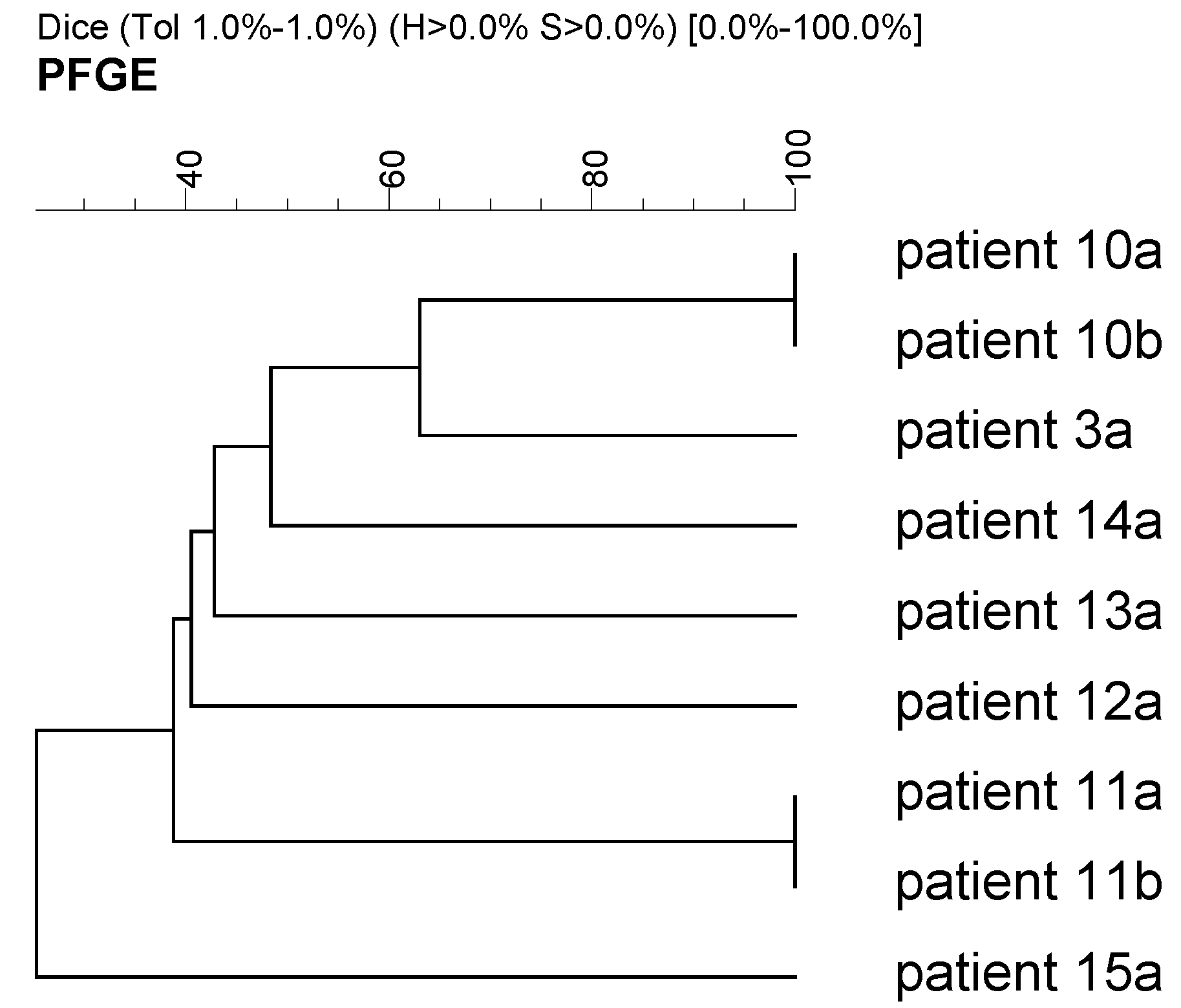
3.3. Clonality of Selected Bacterial Isolates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Skipworth, R.; Fearon, K. Acute abdomen: Peritonitis. Surgery 2008, 26, 98–101. [Google Scholar] [CrossRef]
- Lopez, N.; Kobayashi, L.; Coimbra, R. A Comprehensive review of abdominal infections. World J. Emerg. Surg. 2011, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clements, T.W.; Tolonen, M.; Ball, C.G.; Kirkpatrick, A.W. Secondary Peritonitis and Intra-Abdominal Sepsis: An Increasingly Global Disease in Search of Better Systemic Therapies. Scand. J. Surg. 2021, 110, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Mazuski, J.E.; Solomkin, J.S. Intra-abdominal infections. Surg. Clin. N. Am. 2009, 89, 421–437. [Google Scholar] [CrossRef]
- Eckmann, C.; Dryden, M.; Montravers, P.; Kozlov, R.; Sganga, G. Antimicrobial treatment of “complicated” intra-abdominal infections and the new IDSA guidelines—A commentary and an alternative European approach according to clinical definitions. Eur. J. Med. Res. 2011, 16, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Li, P.K.-T.; Szeto, C.C.; Piraino, B.; De Arteaga, J.; Fan, S.; Figueiredo, A.E.; Fish, D.N.; Goffin, E.; Kim, Y.-L.; Salzer, W.; et al. ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2016, 36, 481–508. [Google Scholar] [CrossRef] [Green Version]
- Gauzit, R.; Péan, Y.; Barth, X.; Mistretta, F.; Lalaude, O.; for the Top Study Team. Epidemiology, Management, and Prognosis of Secondary Non-Postoperative Peritonitis: A French Prospective Observational Multicenter Study. Surg. Infect. 2009, 10, 119–127. [Google Scholar] [CrossRef]
- Heredia-Rodríguez, M.; Peláez, M.T.; Fierro, I.; Gómez-Sánchez, E.; Gómez-Pesquera, E.; Lorenzo, M.; Álvarez-González, F.J.; Bustamante-Munguira, J.; Eiros, J.M.; Bermejo-Martin, J.F.; et al. Impact of ventilator-associated pneumonia on mortality and epidemiological features of patients with secondary peritonitis. Ann. Intensiv. Care 2016, 6, 34. [Google Scholar] [CrossRef] [Green Version]
- Koenig, S.M.; Truwit, J.D. Ventilator-Associated Pneumonia: Diagnosis, Treatment, and Prevention. Clin. Microbiol. Rev. 2006, 19, 637–657. [Google Scholar] [CrossRef] [Green Version]
- Uvizl, R.; Hanulik, V.; Husickova, V.; Sedlakova, M.H.; Adamus, M.; Kolar, M. Hospital-acquired pneumonia in icu patients. Biomed. Pap. 2011, 155, 373–378. [Google Scholar] [CrossRef] [Green Version]
- American Thoracic Society and the Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.D.; DeCamp, M.M.; Garrison, R.N.; Fry, D.E. Pulmonary infection complicating intra-abdominal sepsis: Clinical and experimental observations. Ann. Surg. 1982, 195, 732–738. [Google Scholar] [CrossRef]
- Mustard, R.A.; Bohnen, J.M.; Rosati, C.; Schouten, B.D. Pneumonia complicating abdominal sepsis. An independent risk factor for mortality. Arch. Surg. 1991, 126, 170–175. [Google Scholar] [CrossRef]
- Thompson, C.; Makary, M.A.; Dorman, T.; Pronovost, P.J. Clinical and Economic Outcomes of Hospital Acquired Pneumonia in Intra-Abdominal Surgery Patients. Ann. Surg. 2006, 243, 547–552. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Inf. Dis. 2016, 63, 61–111. [Google Scholar] [CrossRef] [Green Version]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the Management of Hospital-Acquired Pneumonia (HAP)/Ventilator-Associated Pneumonia (VAP) of the European. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef] [Green Version]
- Herkel, T.; Uvizl, R.; Doubravská, L.; Adamus, M.; Gabrhelik, T.; Sedlakova, M.H.; Kolar, M.; Hanulik, V.; Pudova, V.; Langova, K.; et al. Epidemiology of hospital-acquired pneumonia: Results of a Central European multicenter, prospective, observational study compared with data from the European region. Biomed. Pap. 2016, 160, 448–455. [Google Scholar] [CrossRef]
- Pudová, V.; Working Group; Sedláková, M.H.; Kolář, M. Clonality of Bacterial Pathogens Causing Hospital-Acquired Pneumonia. Curr. Microbiol. 2016, 73, 312–316. [Google Scholar] [CrossRef]
- Luna, C.M.; Vujacich, P.; Niederman, M.S.; Vay, C.; Gherardi, C.; Matera, J.; Jolly, E.C. Impact of BAL Data on the Therapy and Outcome of Ventilator-Associated Pneumonia. Chest 1997, 111, 676–685. [Google Scholar] [CrossRef]
- Jang, K.-S.; Kim, Y.H. Rapid and robust MALDI-TOF MS techniques for microbial identification: A brief overview of their diverse applications. J. Microbiol. 2018, 56, 209–216. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Available online: http://www.eucast.org (accessed on 10 February 2023).
- Sedlakova, M.H.; Hanulik, V.; Chroma, M.; Hricova, K.; Kolar, M.; Latal, T.; Schaumann, R.; Rodloff, A.C. Phenotypic detection of broad-spectrum beta-lactamases in microbiological practice. Med. Sci. Monit. 2011, 17, BR147–BR152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dallenne, C.; Da Costa, A.; Decré, D.; Favier, C.; Arlet, G. Development of a set of multiplex PCR assays for the detection of genes encoding important beta-lactamases in Enterobacteriaceae. J. Antimicrob. Chemother. 2010, 65, 490–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mlynarcik, P.; Dolejska, M.; Vagnerova, I.; Kutilová, I.; Kolar, M. Detection of clinically important β-lactamases by using PCR. FEMS Microbiol. Lett. 2021, 368, fnab068. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pérez, F.J.; Hanson, N.D. Detection of plasmid-mediated AmpC beta-lactamase genes in clinical isolates by using multiplex PCR. J. Clin. Microbiol. 2002, 40, 2153–2162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutka-Malen, S.; Evers, S.; Courvalin, P. Detection of glycopeptide resistance genotypes and identification to the species level of clinically relevant enterococci by PCR. J. Clin. Microbiol. 1995, 33, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Husickova, V.; Cekanova, L.; Chroma, M.; Htoutou-Sedlakova, M.; Hricova, K.; Kolar, M. Carriage of ESBL- and AmpC-positive Enterobacteriaceae in the gastrointestinal tract of community subjects and hospitalized patients in the Czech Republic. Biomed. Pap. 2012, 156, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, A.M.; Hassuna, N.A. Modified PFGE protocol for improving typeability of DNA degradation susceptible nosocomial Klebsiella pneumoniae. J. Med. Microbiol. 2019, 68, 1787–1792. [Google Scholar] [CrossRef]
- Špička, P.; Chudáček, J.; Řezáč, T.; Starý, L.; Horáček, R.; Klos, D. Prognostic significance of simple scoring systems in the prediction of diffuse peritonitis morbidity and mortality. Life 2022, 12, 487. [Google Scholar] [CrossRef]
- Boeck, L.; Eggimann, P.; Smyrnios, N.; Pargger, H.; Thakkar, N.; Siegemund, M.; Morgenthaler, N.G.; Rakic, J.; Tamm, M.; Stolz, D. The Sequential Organ Failure Assessment score and copeptin for predicting survival in ventilator-associated pneumonia. J. Crit. Care 2012, 27, 523.e1–523.e9. [Google Scholar] [CrossRef]
- Riché, F.C.; Dray, X.; Laisné, M.-J.; Matéo, J.; Raskine, L.; Pors, M.-J.S.-L.; Payen, D.; Valleur, P.; Cholley, B.P. Factors associated with septic shock and mortality in generalized peritonitis: Comparison between community-acquired and postoperative peritonitis. Crit. Care 2009, 13, R99. [Google Scholar] [CrossRef] [Green Version]
- Inui, T.; Haridas, M.; Claridge, J.A.; Malangoni, M.A. Mortality for intra-abdominal infection is associated with intrinsic risk factors rather than the source of infection. Surgery 2009, 146, 654–662. [Google Scholar] [CrossRef]
- Kolář, M. Bacterial Infections, Antimicrobial Resistance and Antibiotic Therapy. Life 2022, 12, 468. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with HAP (n = 40) | Patients without HAP (n = 234) | p-Value |
|---|---|---|---|
| age (mean years ± SD) | 63.9 ± 18.2 | 61.6 ± 16.4 | 0.191 a |
| male gender [n (%)] | 25 (62.5) | 129 (55.1) | 0.491 |
| comorbidities [n (%)] | |||
| diabetes mellitus | 8 (20.0) | 46 (19.7) | 1.000 |
| hypertension | 27 (67.5) | 126 (53.8) | 0.123 |
| malignancies | 17 (42.5) | 88 (37.6) | 0.599 |
| chronic kidney disease | 1 (2.5) | 26 (11.1) | 0.146 |
| liver disease | 6 (15.0) | 15 (6.4) | 0.098 |
| lung disease | 14 (35.0) | 50 (21.4) | 0.070 |
| two or more serious conditions | 29 (72.5) | 140 (59.8) | 0.159 |
| peritonitis type—etiology [n (%)] | 0.971 | ||
| 1 right colon | 5 (12.5) | 35 (15.0) | |
| 2 left colon | 13 (32.5) | 65 (27.7) | |
| 3 rectum | 3 (7.5) | 14 (6.0) | |
| 4 small intestine | 8 (20.0) | 48 (20.5) | |
| 5 biliary tract | 3 (7.5) | 26 (11.1) | |
| 6 upper GIT | 8 (20.0) | 46 (19.7) | |
| peritonitis type—effusion [n (%)] | 0.403 | ||
| serous, chemical, other | 5 (12.5) | 30 (12.8) | |
| purulent | 20 (50.0) | 142 (60.7) | |
| stercoral | 11 (27.5) | 50 (21.4) | |
| biliary | 4 (10.0) | 12 (5.1) | |
| qSOFA [n (%)] | 0.021 *,a | ||
| 0 | 14 (35.0) | 123 (52.6) | |
| 1 | 15 (37.5) | 76 (32.5) | |
| 2 | 9 (22.5) | 28 (12.0) | |
| 3 | 2 (5.0) | 7 (3.0) | |
| mortality [n (%)] | |||
| 30-day | 17 (42.5) | 45 (19.2) | 0.002 ** |
| 90-day | 21 (52.5) | 55 (23.5) | 0.0004 *** |
| overall morbidity [n(%)] | 38 (95.0) | 163 (69.7) | 0.0004 *** |
| surgery type [n (%)] | 0.774 | ||
| NPWT | 12 (30) | 54 (23.1) | |
| abdominal cavity closure with fabric | 3 (7.5) | 15 (6.4) | |
| primary closure with continuous flow | 11 (27.5) | 73 (31.2) | |
| primary closure with passive drain | 14 (35.0) | 92 (39.3) |
| Bacterial Species | No. of Isolates | Percentage |
|---|---|---|
| Pseudomonas aeruginosa | 9 | 20.0 |
| Klebsiella pneumoniae | 7 | 15.6 |
| Escherichia coli | 6 | 13.3 |
| Enterococcus faecalis | 5 | 11.1 |
| Enterobacter cloacae complex | 5 | 11.1 |
| Staphylococcus aureus | 4 | 8.9 |
| Klebsiella aerogenes | 2 | 4.4 |
| Acinetobacter baumannii | 2 | 4.4 |
| Serratia marcescens | 1 | 2.2 |
| Stenotrophomonas maltophilia | 1 | 2.2 |
| Burkholderia cepacia complex | 1 | 2.2 |
| Enterococcus faecium | 1 | 2.2 |
| Providencia rettgeri | 1 | 2.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chudáček, J.; Špička, P.; Kolar, M.; Stašek, M.; Kolcún, Š.; Klos, D.; Hricová, K.; Mlynarcik, P.; Pudová, V.; Klementová, O.; et al. Analysis of Bacterial Pathogens Causing Complicating HAP in Patients with Secondary Peritonitis. Antibiotics 2023, 12, 527. https://doi.org/10.3390/antibiotics12030527
Chudáček J, Špička P, Kolar M, Stašek M, Kolcún Š, Klos D, Hricová K, Mlynarcik P, Pudová V, Klementová O, et al. Analysis of Bacterial Pathogens Causing Complicating HAP in Patients with Secondary Peritonitis. Antibiotics. 2023; 12(3):527. https://doi.org/10.3390/antibiotics12030527
Chicago/Turabian StyleChudáček, Josef, Petr Špička, Milan Kolar, Martin Stašek, Štefan Kolcún, Dušan Klos, Kristýna Hricová, Patrik Mlynarcik, Vendula Pudová, Olga Klementová, and et al. 2023. "Analysis of Bacterial Pathogens Causing Complicating HAP in Patients with Secondary Peritonitis" Antibiotics 12, no. 3: 527. https://doi.org/10.3390/antibiotics12030527
APA StyleChudáček, J., Špička, P., Kolar, M., Stašek, M., Kolcún, Š., Klos, D., Hricová, K., Mlynarcik, P., Pudová, V., Klementová, O., & Horáček, R. (2023). Analysis of Bacterial Pathogens Causing Complicating HAP in Patients with Secondary Peritonitis. Antibiotics, 12(3), 527. https://doi.org/10.3390/antibiotics12030527