
Impact of Adding a Rapid PCR-Based Blood Culture Identification Panel to the Antimicrobial Stewardship Program of Patients with Febrile Neutropenia in a Peruvian Referral Hospital
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klastersky, J.; de Naurois, J.; Rolston, K.; Rapoport, B.; Maschmeyer, G.; Aapro, M.; Herrstedt, J.; on behalf of the ESMO Guidelines Committee. Management of febrile neutropaenia: ESMO Clinical Practice Guidelines. Ann. Oncol. 2016, 27 (Suppl. 5), v111–v118. [Google Scholar] [CrossRef]
- Carvalho, A.S.; Lagana, D.; Catford, J.; Shaw, D.; Bak, N. Bloodstream infections in neutropenic patients with haematological malignancies. Infect. Dis. Health 2020, 25, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Lalaoui, R.; Javelle, E.; Bakour, S.; Ubeda, C.; Rolain, J.-M. Infections Due to Carbapenem-Resistant Bacteria in Patients With Hematologic Malignancies. Front. Microbiol. 2020, 11, 1422. [Google Scholar] [CrossRef] [PubMed]
- Nesher, L.; Rolston, K.V.I. The current spectrum of infection in cancer patients with chemotherapy related neutropenia. Infection 2014, 42, 5–13. [Google Scholar] [CrossRef]
- Trecarichi, E.M.; Pagano, L.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Caira, M.; Spadea, A.; Busca, A.; et al. Current epidemiology and antimicrobial resistance data for bacterial bloodstream infections in patients with hematologic malignancies: An Italian multicentre prospective survey. Clin. Microbiol. Infect. 2015, 21, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, Y.; Fan, X.; Tang, W.; Hu, J. Prevalence of Resistant Gram-Negative Bacilli in Bloodstream Infection in Febrile Neutropenia Patients Undergoing Hematopoietic Stem Cell Transplantation. Medicine 2015, 94, e1931. [Google Scholar] [CrossRef]
- Kara, Ö.; Zarakolu, P.; Aşçioğlu, S.; Etgül, S.; Uz, B.; Büyükaşik, Y.; Akova, M. Epidemiology and emerging resistance in bacterial bloodstream infections in patients with hematologic malignancies. Infect. Dis. 2015, 47, 686–693. [Google Scholar] [CrossRef]
- El-Mahallawy, H.; Samir, I.; Fattah, R.A.; Kadry, D.; El Kholy, A. Source, pattern and antibiotic resistance of blood stream infections in hematopoietic stem cell transplant recipients. J. Egypt. Natl. Cancer Inst. 2014, 26, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Garzón, J.R.; Isaza, N.; Posada, A.; Mendez, R.; Arenas, J.; Ardila, M.P.; Cárdenas, A.; Barrera, V.; Moreno, P.; Córdoba, I.; et al. Clinical and microbiological characteristics of patients with febrile neutropenia in one Colombian Universitary Hospital. Infectio 2019, 23, 347–351. [Google Scholar] [CrossRef]
- Klastersky, J.; Ameye, L.; Maertens, J.; Georgala, A.; Muanza, F.; Aoun, M.; Ferrant, A.; Rapoport, B.; Rolston, K.; Paesmans, M. Bacteraemia in febrile neutropenic cancer patients. Int. J. Antimicrob. Agents 2007, 30, 51–59. [Google Scholar] [CrossRef]
- Righi, E.; Peri, A.M.; Harris, P.N.A.; Wailan, A.M.; Liborio, M.; Lane, S.W.; Paterson, D.L. Global prevalence of carbapenem resistance in neutropenic patients and association with mortality and carbapenem use: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2017, 72, 668–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinojosa-Andía, L.J.; del Carpio-Jayo, D. Bacteremia associated with febrile neutropenia in hematology-oncology patients, bacterial spectrum and antibiotic susceptibility pattern. Rev. Med. Hered. 2014, 25, 22–29. [Google Scholar] [CrossRef]
- Nouér, S.A.; Nucci, M.; Anaissie, E. Tackling antibiotic resistance in febrile neutropenia: Current challenges with and recommendations for managing infections with resistant Gram-negative organisms. Expert Rev. Hematol. 2015, 8, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D.; Neugut, A.I.; Ananth, C.V.; Lewin, S.N.; Wilde, E.T.; Lu, Y.-S.; Herzog, T.J.; Hershman, D.L. Deviations From Guideline-Based Therapy for Febrile Neutropenia in Cancer Patients and Their Effect on Outcomes. JAMA Intern. Med. 2013, 173, 559–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baugh, C.W.; Wang, T.J.; Caterino, J.M.; Baker, O.N.; Brooks, G.A.; Reust, A.C.; Pallin, D.J. Emergency Department Management of Patients with Febrile Neutropenia: Guideline Concordant or Overly Aggressive? Acad. Emerg. Med. 2017, 24, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Horo, J.C.; Marcelin, J.; Abu Saleh, O.M.; Barwise, A.K.; Odean, P.M.; Rivera, C.; Tande, A.J.; Wilson, J.W.; Osmon, D.R.; Tosh, P.K. Standardizing Febrile Neutropenia Management: Antimicrobial Stewardship in the Hematologic Malignancy Population. J. Oncol. Pract. 2019, 15, e843–e848. [Google Scholar] [CrossRef]
- Rosa, R.G.; Goldani, L.Z.; Dos Santos, R.P. Association between adherence to an antimicrobial stewardship program and mortality among hospitalised cancer patients with febrile neutropaenia: A prospective cohort study. BMC Infect. Dis. 2014, 14, 286. [Google Scholar] [CrossRef] [Green Version]
- Madran, B.; Keske, Ş.; Tokça, G.; Dönmez, E.; Ferhanoğlu, B.; Çetiner, M.; Mandel, N.M.; Ergönül, Ö. Implementation of an antimicrobial stewardship program for patients with febrile neutropenia. Am. J. Infect. Control 2018, 46, 420–424. [Google Scholar] [CrossRef]
- Hernández-Gómez, C.; Hercilla, L.; Mendo, F.; Pérez-Lazo, G.; Contreras, E.; Ramírez, E.; Flores, W.; Julca, Á.; Chuquiray, N.; Arenas, B.; et al. Antimicrobial Stewardship programs in Peru: A fundamental agreement. Rev. Chil. Infectología 2019, 36, 565–575. [Google Scholar] [CrossRef] [Green Version]
- CDC. Core Elements of Hospital Antibiotic Stewardship Programs; US Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 12 December 2022).
- Patel, R.; Fang, F.C. Diagnostic Stewardship: Opportunity for a Laboratory–Infectious Diseases Partnership. Clin. Infect. Dis. 2018, 67, 799–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peri, A.M.; Ling, W.; Furuya-Kanamori, L.; Harris, P.N.A.; Paterson, D.L. Performance of BioFire Blood Culture Identification 2 Panel (BCID2) for the detection of bloodstream pathogens and their associated resistance markers: A systematic review and meta-analysis of diagnostic test accuracy studies. BMC Infect. Dis. 2022, 22, 794. [Google Scholar] [CrossRef]
- MacVane, S.H.; Nolte, F.S. Benefits of Adding a Rapid PCR-Based Blood Culture Identification Panel to an Established Antimicrobial Stewardship Program. J. Clin. Microbiol. 2016, 54, 2455–2463. [Google Scholar] [CrossRef] [Green Version]
- Egli, A.; Osthoff, M.; Goldenberger, D.; Halter, J.; Schaub, S.; Steiger, J.; Weisser, M.; Frei, R. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF) directly from positive blood culture flasks allows rapid identification of bloodstream infections in immunosuppressed hosts. Transpl. Infect. Dis. 2015, 17, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Szymankiewicz, M.; Nakonowska, B. Rapid Detection of Bloodstream Pathogens in Oncologic Patients with a FilmArray Multiplex PCR Assay: A Comparison with Culture Methods. Pol. J. Microbiol. 2018, 67, 103–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buss, B.A.; Baures, T.J.; Yoo, M.; Hanson, K.E.; Alexander, D.P.; Benefield, R.J.; Spivak, E.S. Impact of a Multiplex PCR Assay for Bloodstream Infections with and without Antimicrobial Stewardship Intervention at a Cancer Hospital. Open Forum Infect. Dis. 2018, 5, ofy258. [Google Scholar] [CrossRef]
- Rosa, R.; Suarez, J.F.; Bravo, G.; A Morillas-Rodriguez, J.; Anderson, A.D.; Camargo, J.F.; Abbo, L. Challenges in Antimicrobial Stewardship: Rapid Diagnostics and Optimization of Therapy Among Immunocompromised Patients. Open Forum Infect. Dis. 2019, 6, ofz239. [Google Scholar] [CrossRef] [PubMed]
- Foster, R.A.; Kuper, K.; Lu, Z.K.; Bookstaver, P.B.; Bland, C.M.; Mahoney, M.V. Pharmacists’ Familiarity with and Institutional Utilization of Rapid Diagnostic Technologies for Antimicrobial Stewardship. Infect. Control Hosp. Epidemiol. 2017, 38, 863–866. [Google Scholar] [CrossRef]
- Nathwani, D.; Varghese, D.; Stephens, J.; Ansari, W.; Martin, S.; Charbonneau, C. Value of hospital antimicrobial stewardship programs [ASPs]: A systematic review. Antimicrob. Resist. Infect. Control 2019, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Carbajal, P.; Salvatierra, G.; Yareta, J.; Pino, J.; Vásquez, N.; Diaz, P.; Martínez, I.; Asmat, P.; Peralta, C.; Huamani, C.; et al. Microbiological and molecular characterization of antimicrobial resistance in uropathogenic Escherichia coli from peruvian public hospitals. Rev. Peru. Med. Exp. Salud Publica 2021, 38, 119–123. [Google Scholar] [CrossRef]
- Al Sulayyim, H.J.; Ismail, R.; Al Hamid, A.; Ghafar, N.A. Antibiotic Resistance during COVID-19: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11931. [Google Scholar] [CrossRef]
- Gudiol, C.; Aguilar-Guisado, M.; Azanza, J.R.; Candel, F.J.; Cantón, R.; Carratalà, J.; Garcia-Vidal, C.; Jarque, I.; Lizasoain, M.; Gil-Bermejo, J.M.; et al. Executive summary of the consensus document of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC), the Spanish Network for Research in Infectious Diseases (REIPI) and the Spanish Society of Haematology and Haemotherapy (SEHH) on the management of febrile neutropenia in patients with hematological malignancies. Enferm. Infecc. Microbiol. Clínica 2020, 38, 174–181. [Google Scholar] [CrossRef]
- Jaiswal, S.R.; Gupta, S.; Kumar, R.S.; Sherawat, A.; Rajoreya, A.; Dash, S.K.; Bhagwati, G.; Chakrabarti, S. Gut Colonization with Carbapenem Resistant Enterobacteriaceae Adversely Impacts the Outcome in Patients with Hematological Malignancies: Results of a Prospective Surveillance Study. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Nadal, G.; Puerta-Alcalde, P.; Gudiol, C.; Cardozo, C.; Albasanz-Puig, A.; Marco, F.; Laporte-Amargós, J.; Moreno-García, E.; Domingo-Doménech, E.; Chumbita, M.; et al. Inappropriate Empirical Antibiotic Treatment in High-risk Neutropenic Patients With Bacteremia in the Era of Multidrug Resistance. Clin. Infect. Dis. 2020, 70, 1068–1074. [Google Scholar] [CrossRef]
- Chumbita, M.; Puerta-Alcalde, P.; Yáñez, L.; Cuesta, M.A.; Chinea, A.; Morales, I.E.; Abellán, P.F.; Gudiol, C.; Guerreiro, M.; González-Sierra, P.; et al. Resistance to empirical β-lactams recommended in febrile neutropenia guidelines in Gram-negative bacilli bloodstream infections in Spain: A multicentre study. J. Antimicrob. Chemother. 2022, 77, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- Satlin, M.J.; Weissman, S.J.; Carpenter, P.A.; Seo, S.K.; Shelburne, S.A. American Society of Transplantation and Cellular Therapy Series, 1: Enterobacterales Infection Prevention and Management after Hematopoietic Cell Transplantation. Transplant. Cell. Ther. 2021, 27, 108–114. [Google Scholar] [CrossRef]
- Clerici, D.; Oltolini, C.; Greco, R.; Ripa, M.; Giglio, F.; Mastaglio, S.; Lorentino, F.; Pavesi, F.; Farina, F.; Liberatore, C.; et al. The place of ceftazidime/avibactam and ceftolozane/tazobactam for therapy of haematological patients with febrile neutropenia. Int. J. Antimicrob. Agents 2021, 57, 106335. [Google Scholar] [CrossRef]
- Karlowsky, J.A.; Kazmierczak, K.M.; de Figueiredo Valente, M.L.N.; Luengas, E.L.; Baudrit, M.; Quintana, A.; Irani, P.; Stone, G.G.; Sahm, D.F. In vitro activity of ceftazidime-avibactam against Enterobacterales and Pseudomonas aeruginosa isolates collected in Latin America as part of the ATLAS global surveillance program, 2017–2019. Braz. J. Infect. Dis. 2021, 25, 101647. [Google Scholar] [CrossRef] [PubMed]
- Naomi-Matsuoka, A.; Vargas, M.; Ymaña, B.; Soza, G.; Pons, M.J. Colistin resistance in multidrug-resistant klebsiella pneumoniae strains at a perinatal maternal institute in Lima, Peru, 2015–2018. Rev. Peru. Med. Exp. Salud Publica 2020, 37, 716–720. [Google Scholar] [CrossRef]
- Sahitya, D.S.K.; Jandiyal, A.; Jain, A.; Senapati, J.; Nanda, S.; Aggarwal, M.; Kumar, P.; Mohapatra, S.; Ray, P.; Malhotra, P.; et al. Prevention and management of carbapenem-resistant Enterobacteriaceae in haematopoietic cell transplantation. Ther. Adv. Infect. Dis. 2021, 8, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Lazo, G.; Abarca-Salazar, S.; Lovón, R.; Rojas, R.; Ballena-López, J.; Morales-Moreno, A.; Flores-Paredes, W.; Arenas-Ramírez, B.; Illescas, L.R. Antibiotic Consumption and Its Relationship with Bacterial Resistance Profiles in ESKAPE Pathogens in a Peruvian Hospital. Antibiotics 2021, 10, 1221. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Castro-Sanchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the potential long-term impact on antimicrobial resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, M.; Averbuch, D.; Tissot, F.; Cordonnier, C.; Akova, M.; Calandra, T.; Ceppi, M.; Bruzzi, P.; Viscoli, C.; Aljurf, M.; et al. Fluoroquinolone prophylaxis in haematological cancer patients with neutropenia: ECIL critical appraisal of previous guidelines. J. Infect. 2018, 76, 20–37. [Google Scholar] [CrossRef] [PubMed]
- Freifeld, A.G.; Bow, E.J.; Sepkowitz, K.A.; Boeckh, M.J.; Ito, J.I.; Mullen, C.A.; Raad, I.I.; Rolston, K.V.; Young, J.-A.H.; Wingard, J.R. Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2011, 52, e56–e93. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Characteristic | Before ASP Intervention n = 32 | After ASP Intervention n = 30 | After ASP Intervention Plus BCID2 n = 31 | p Value | |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 20 (62.5%) | 20 (66.7%) | 10 (32.3%) | 0.013 | |
| Age, mean (IQR) | 46.7 (38–57.5) | 45.3 (37–56) | 50 (40–62) | 0.279 | |
| Comorbidities | |||||
| Diabetes mellitus | 2 (6.3%) | 1 (3.3%) | 1 (3.2%) | 1.000 | |
| Liver disease | 2 (6.3%) | 0 | 2 (6.5%) | 0.541 | |
| Renal replacement therapy | 1 (3.1%) | 0 | 3 (9.7%) | 0.216 | |
| HIV/AIDS | 0 | 1 (3.3%) | 0 | 0.323 | |
| Cerebrovascular disease | 1 (3.1%) | 1 (3.3%) | 1 (3.2%) | 1.000 | |
| Peripheral vascular disease | 0 | 2 (6.7%) | 0 | 0.102 | |
| Chronic heart failure | 1 (3.1%) | 0 | 0 | 1.000 | |
| Hypertension | 1 (3.1%) | 2 (6.7%) | 4 (12.9%) | 0.341 | |
| Connective tissue disease | 0 | 2 (6.7%) | 0 | 0.102 | |
| Hematological malignancy | |||||
| Acute myeloid leukemia | 13 (40.6%) | 12 (40%) | 16 (51.6%) | 0.585 | |
| Acute lymphocytic leukemia | 13 (40.6%) | 14 (46.7%) | 10 (32.2%) | 0.513 | |
| Non-Hodgkin’s lymphoma | 3 (9.4%) | 4 (13.3%) | 1 (3.2%) | 0.386 | |
| Aplastic anemia | 1 (3.1%) | 0 | 2 (6.5%) | 0.652 | |
| Autologous stem cell transplant | 0 | 0 | 2 (6.5%) | 0.21 | |
| Multiple myeloma | 2 (6.3%) | 0 | 0 | 0.326 | |
| Suspected source of infection | |||||
| Urine | 3 (9.4%) | 4 (13.3%) | 1 (3.2%) | 0.386 | |
| Catheter related | 11 (34.4%) | 6 (20%) | 5 (16.1%) | 0.199 | |
| Respiratory | 6 (18.8%) | 5 (16.7%) | 5 (16.1%) | 0.958 | |
| Intra-abdominal | 5 (15.6%) | 4 (13.3%) | 6 (19.4%) | 0.811 | |
| Skin and soft tissue | 2 (6.2%) | 2 (6.7%) | 9 (29.1%) | 0.021 | |
| Others | 0 | 0 | 1 (3.2) | 0.656 | |
| Unidentified | 5 (15.6%) | 9 (30%) | 4 (12.9%) | 0.193 | |
| MASCC score < 21 (high risk) | 23 (71.9%) | 25 (83.3%) | 28 (90.3%) | 0.161 | |
| Charlson Comorbidity Index, mean (IQR) | 2.8 (2–3.5) | 3.1 (2–4) | 3.5 (3–4) | 0.02 | |
| Pitt bacteremia score (PBS), mean (IQR) | 1.5 (0–2) | 1.8 (1–2) | 1.8 (0–3) | 0.693 | |
| Mechanic ventilation | 4 (12.5%) | 3 (10%) | 6 (19.4%) | 0.569 | |
| Admission to ICU within 48 h of the episode of BSI | 3 (9.4%) | 2 (6.7%) | 2 (6.5%) | 1.000 | |
| Polymicrobial infection | 8 (25%) | 7 (23.3%) | 8 (25.8%) | 0.974 | |
| Antibacterial prophylaxis | 20 (62.5%) | 4 (13.3%) | 9 (29.1%) | <0.001 | |
| Antifungal prophylaxis | 10 (31.3%) | 13 (43.3%) | 19 (61.3%) | 0.055 | |
| Parameter | Before ASP Intervention | After ASP Intervention | After ASP Intervention Plus BCID2 | p Value |
|---|---|---|---|---|
| Microbiology-related outcomes | ||||
| Time to blood culture positivity, h, median (IQR) | 18 (15.5–20) | 18 (15–21) | 11.14 (9.4–15.7) b,c | <0.001 |
| Time to organism identification, h, median (IQR) | 55 (50–58) | 48 (43–56) b | 19.5 (17.8–25.2) b,c | <0.001 |
| Time to in vitro susceptibility results, h, median (IQR) | 64 (58–67.5) | 62 (56–68) | 59.1 (56–64.6) | 0.317 |
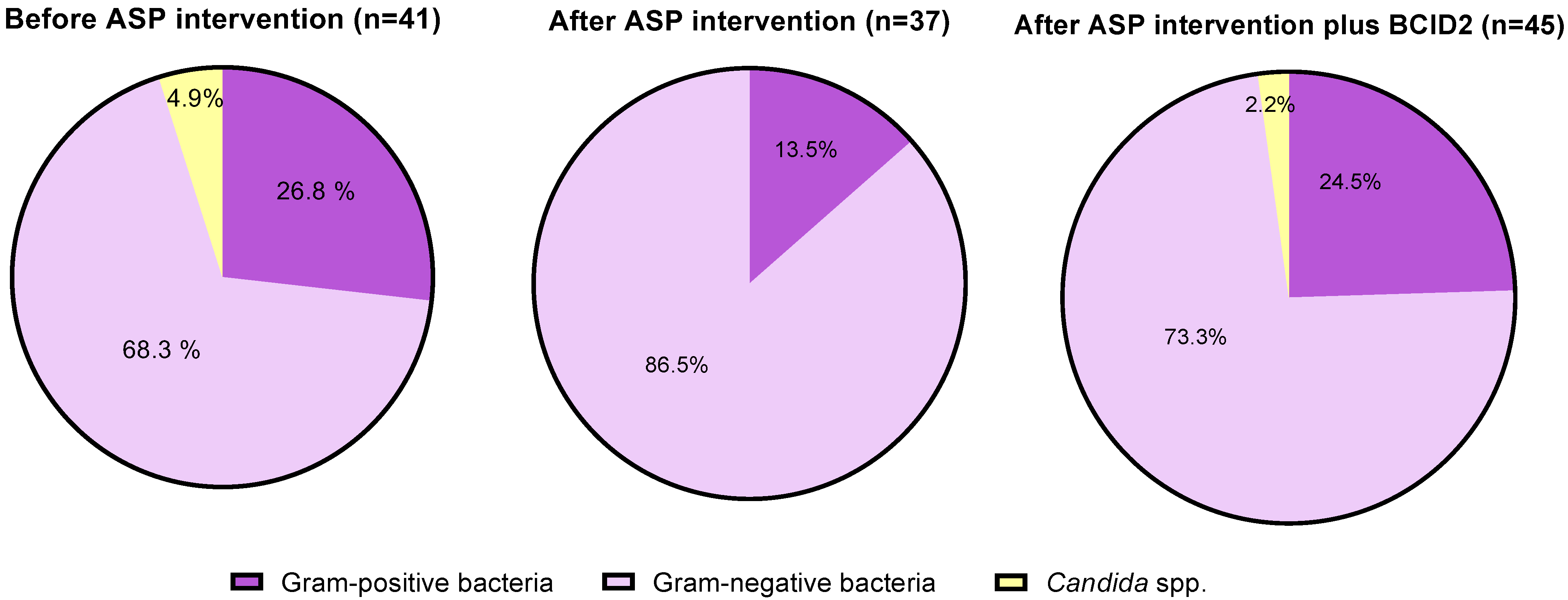
| Blood culture pathogens a | ||||
| Gram-positive bacteria (n = 27) | 11/41 (26.8%) | 5/37 (13.5%) | 11/45 (24.5%) | 0.321 |
| Staphylococcus spp. (coagulase negative) | 5 | 4 | 8 | |
| Staphylococcus aureus | 3 | 1 | 0 | |
| Enterococcus faecium | 2 | 0 | 1 | |
| Streptococcus spp. | 1 | 0 | 2 | |
| Gram-negative bacteria (n = 93) | 28/41 (68.3%) | 32/37 (86.5%) | 33/45 (73.3%) | 0.158 |
| E. coli | 8 | 10 | 10 | |
| Klebsiella pneumoniae | 6 | 5 | 10 | |
| Pseudomonas aeruginosa | 7 | 7 | 5 | |
| Acinetobacter baumannii | 2 | 1 | 1 | |
| Citrobacter freundii | 1 | 0 | 0 | |
| Enterobacter cloacae | 1 | 2 | 0 | |
| Acinetobacter lwoffii | 1 | 3 | 1 | |
| Pseudomonas putida | 1 | 0 | 1 | |
| Aeromonas hydrophila | 0 | 1 | 0 | |
| Serratia marcescens | 0 | 1 | 2 | |
| Klebsiella oxytoca | 1 | 0 | 2 | |
| Leminorella richardii | 0 | 1 | 0 | |
| Stenotrophomonas maltophilia | 0 | 1 | 0 | |
| Proteus spp. | 0 | 0 | 1 | |
| Candida spp. (n = 3) | 2/41 (4.9%) | 0/0 (0%) | 1/45 (2.2%) | 0.64 |
| Candida albicans | 1 | 0 | 0 | |
| Candida tropicalis | 1 | 0 | 0 | |
| Candida kefyr | 0 | 0 | 1 |
| Patient | BCID2 Result | Conventional Culture and Phenotypic Susceptibility Testing Result(s) |
|---|---|---|
| Polymicrobial cultures | ||
| Patient #3 | Klebsiella pneumoniae, Acinetobacter calcoaceticus-baumannii complex, E. coli, Streptococcus spp. | Klebsiella pneumoniae |
| Patient #11 | Staphylococcus epidermidis (gen mec A/C), Streptococcus spp. | Methicillin-resistant Staphylococcus epidermidis |
| Patient #31 | E. coli/Klebsiella pneumoniae (CTX-M), Proteus spp., Serratia marcescens | ESBL-producing E. coli, Serratia marcescens |
| Discrepancies between resistance genes identified by BCID2 panel and phenotypic antimicrobial susceptibility test results | ||
| Patient #4 | Klebsiella oxytoca | ESBL-producing Klebsiella oxytoca |
| Patient # 25 | Staphylococcus epidermidis | Methicillin-resistant Staphylococcus epidermidis |
| Discrepancy in organism identification | ||
| Patient #10 | Non-identified | Acinetobacter lwoffii |
| Patient #15 | Non-identified | Pseudomonas putida |
| Patient #27 | Staphylococcus epidermidis (gen mec A/C) | Candida kefyr |
| Parameter | Before ASP Intervention | After ASP Intervention | After ASP Intervention Plus BCID2 | |
|---|---|---|---|---|
| Blood culture pathogens | ||||
| Staphylococcus spp. (coagulase negative) meticillin-resistance | ||||
| 4/4 (100%) | 3/4 (75%) | 7/8 (87.5%) * | ||
| Staphylococcus aureus meticillin-resistance | ||||
| 3/3 (100%) | 1/1 (100%) | 0 | ||
| Enterobacteriaceae ESBL CPE | ||||
| 8/17 (47.1%) | 8/19 (42.1%) | 9/25 (36%) ** | ||
| 0 | 0 | 5/25 (20%) *** | ||
| Pseudomonas aeruginosa MDR XDR DTR Susceptible | ||||
| 3/7 (42.9%) | 0 | 0 | ||
| 4/7 (57.1%) | 2/7 (28.6%) | 0 | ||
| 0 | 1/7 (14.3%) | 0 | ||
| 0 | 4/7 (57.1%) | 5/5 (100%) | ||
| Acinetobacter baumannii MDR XDR Susceptible | ||||
| 1/2 (50%) | 0 | 0 | ||
| 0 | 0 | 0 | ||
| 1/2 (50%) | 1/1 (100%) | 1/1(100%) | ||
| Enterococcus faecium Vancomycin resistant | ||||
| 2/2 (100%) | 0 | 1/1 (100%) **** | ||
| Candida Resistant to azoles | ||||
| 1/2 (50%) | 0 | 1/1 (100%) | ||
| Before ASP Intervention | After ASP Intervention | After ASP Intervention Plus BCID2 | p Value | |
|---|---|---|---|---|
| Appropriateness of antimicrobials a | ||||
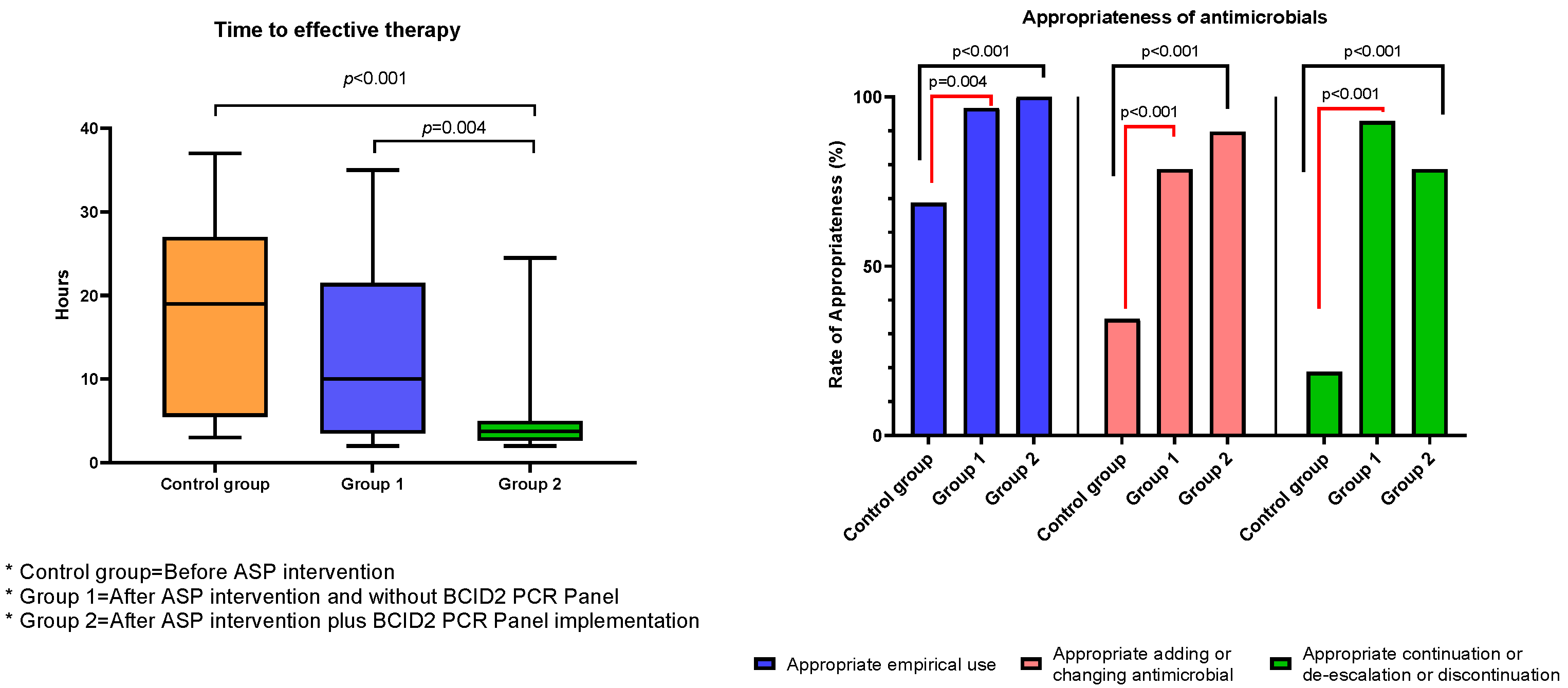
| Appropriate empirical use | 22/32 (68.7%) | 29/30 (96.7%) b | 31/31 (100%) b | <0.001 |
| Appropriate adding or changing antimicrobial | 11/32 (34.4%) | 22/28 (78.6%) b | 26/29 (89.7%) b | <0.001 |
| Appropriate continuation or de-escalation or discontinuation | 6/32 (18.8%) | 26/28 (92.8%) b | 22/28 (78.6%) b | <0.001 |
| Parameter | Before ASP Intervention n = 32 | After ASP Intervention n= 30 | After ASP Intervention Plus BCID2 n= 31 | p Value |
|---|---|---|---|---|
| Treatment-related outcomes | ||||
| Time to effective therapy, h, median (IQR) (n = 78) | 19 (6–27) | 10 (4–20) b | 3.75 (2.75–5) b,c | <0.001 |
| Relapse of bacteremia a | 5 (15.6%) | 0 | 5 (16.1%) | 0.051 |
| Clinical outcomes | ||||
| Hospital length of stay (LOS), number of days, median (IQR) | 33 (27–50) | 27 (23–37) | 28 (23–32) b | 0.042 |
| LOS, number of days, following first positive blood culture, median (IQR) | 10 (6.5–12) | 11 (6–19) | 11 (8–18) | 0.281 |
| In-hospital mortality (all cause)a | 9 (28.1%) | 5 (16.7%) | 11 (35.5%) | 0.248 |
| 30-day all-cause hospital readmission (n = 68) a | 12 (52.1%) | 9 (36%) | 7 (35%) | 0.419 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Lazo, G.; del Valle-Mendoza, J.; Sandoval-Ahumada, R.; Soto-Febres, F.; Castillo-Córdova, R.; Zárate-Tantaleán, M.; Morales-Castillo, L.; Páucar-Miranda, C.J.; Altamirano-Molina, M.; Pacheco-Modesto, I.; et al. Impact of Adding a Rapid PCR-Based Blood Culture Identification Panel to the Antimicrobial Stewardship Program of Patients with Febrile Neutropenia in a Peruvian Referral Hospital. Antibiotics 2023, 12, 648. https://doi.org/10.3390/antibiotics12040648
Pérez-Lazo G, del Valle-Mendoza J, Sandoval-Ahumada R, Soto-Febres F, Castillo-Córdova R, Zárate-Tantaleán M, Morales-Castillo L, Páucar-Miranda CJ, Altamirano-Molina M, Pacheco-Modesto I, et al. Impact of Adding a Rapid PCR-Based Blood Culture Identification Panel to the Antimicrobial Stewardship Program of Patients with Febrile Neutropenia in a Peruvian Referral Hospital. Antibiotics. 2023; 12(4):648. https://doi.org/10.3390/antibiotics12040648
Chicago/Turabian StylePérez-Lazo, Giancarlo, Juana del Valle-Mendoza, Roxana Sandoval-Ahumada, Fernando Soto-Febres, Raúl Castillo-Córdova, Melissa Zárate-Tantaleán, Liliana Morales-Castillo, Celia Joanna Páucar-Miranda, Milagros Altamirano-Molina, Iván Pacheco-Modesto, and et al. 2023. "Impact of Adding a Rapid PCR-Based Blood Culture Identification Panel to the Antimicrobial Stewardship Program of Patients with Febrile Neutropenia in a Peruvian Referral Hospital" Antibiotics 12, no. 4: 648. https://doi.org/10.3390/antibiotics12040648