Abstract
A misunderstanding of the mechanism of action and bacterial targets of antibiotics by consumers may drive inappropriate antibiotic use and antimicrobial resistance (AMR). Tackling AMR requires an in-depth understanding of consumer beliefs and misconceptions. We explored consumer conversations on a number of social media platforms on antibiotic use and AMR in the context of sore throat and how coronavirus disease 2019 (COVID-19) affected online conversations between 1 January 2018 and 25 November 2021 across eight countries. Five distinct consumer groups were identified (antibiotic-preserving peer educators, antibiotic-cautious consumers, medication-resistant antibiotic opponents, believers in the strength of antibiotics, determined pro-antibiotic consumers) with a wide spectrum of beliefs around antibiotics in sore throat. Many opinions were based upon misconceptions, the most prominent of which was that antibiotics are strong medications that can treat all types of sore throat. COVID-19 had a multifaceted effect on the sore throat and AMR conversation. Sore throat triggered anxiety as consumers feared it may be a COVID-19 symptom while engagement in conversations around antibiotics for COVID-19 increased. Finally, consumers sought multiple routes to access antibiotics, such as directly from the pharmacy or by attempting to persuade physicians to prescribe. Knowledge obtained from this study could be used to develop focused approaches to dispel consumer misconceptions and mitigate AMR.
1. Introduction
Antimicrobial resistance (AMR) is one of the most urgent global health challenges of the 21st century [1] and the World Health Organization (WHO) has consistently listed AMR as one of the top ten global public health threats annually [2]. AMR is also a major source of mortality across the world [3]. In 2019, approximately 4.95 million deaths were associated with bacterial AMR and approximately 1.27 million deaths were directly attributable to AMR globally, positioning it as the third leading cause of death after stroke and ischemic heart disease [4].
Overuse and misuse of antimicrobials significantly contribute to AMR [2,5]. Despite the fact that antibiotics are only indicated for bacterial infections [6,7], common viral illnesses such as the common cold and the flu are frequently treated with antibiotics [6]. For example, a European survey among 26,511 respondents revealed that close to one-third of respondents took antibiotics for a common cold or the flu [6]. Pharyngitis, or sore throat, which is a common manifestation of viral illnesses [8], is also regularly treated with antibiotics. A European survey reported that 13% of respondents took antibiotics for a sore throat [6], while a UK study found that 59% of sore throat consultations resulted in an antibiotic prescription [9].
Inappropriate antibiotic use, whether obtained on prescription or over the counter (OTC), is likely to be influenced by consumer misunderstanding. Studies conducted prior to coronavirus disease 2019 (COVID-19) revealed that up to 71% of patients believed that viruses can be treated with antibiotics [10,11,12,13,14]. Studies conducted during or following the height of the pandemic showed that there was still substantial public misunderstanding, despite widespread public information campaigns around COVID-19 and far greater coverage of topics related to viral infection in the general media. For example, the Sore Throat and Antibiotic Resistance (STAR) study conducted in May 2022 across 12 countries determined behaviors and attitudes related to upper respiratory tract infections, and sought to understand how antibiotics were used for respiratory symptoms [15]. Overall, 55% of respondents (18–64 years) believed that antibiotics kill viruses, while this increased to 60% in 25–34-year-olds [15]. A European survey showed that approximately 40% of respondents incorrectly thought that antibiotics kill viruses and 11% were unsure [6].
It has also been shown that consumers have a poor understanding of AMR. A study using qualitative semi-structured interviews with patients or parents of children presenting with an acute respiratory infection to general practices in Australia, revealed a lack of understanding of what becomes resistant (the person or the bacteria), how patients contribute to AMR, and that resistance can spread between people in close proximity [16]. Furthermore, the STAR study revealed that 36% of consumers were not concerned about AMR [15].
Addressing the challenge of AMR as we move past the height of the COVID-19 pandemic requires an in-depth understanding of consumer perceptions and misconceptions around antibiotic use and AMR, so that targeted educational materials/messages and strategies (e.g., consumer engagement models) can be developed and delivered. Social media provides unprecedented communication opportunities between individuals, companies and organizations. In 2021, around one-half of the global population (approximately 4.26 billion people) used social media worldwide [17]. In addition, health organizations commonly use social media as a communication channel to engage their audiences [18]. For example, >80% of state health departments in the United States have social media accounts [19], while the Department of Health in South Africa had more than 100,000 Twitter followers as of March 2020 [20].
The extensive use of social media provides an opportunity to further explore consumer beliefs and conversations regarding antibiotics and AMR and offers opportunities to share appropriate messages through such platforms. The aim of this study was to explore consumer conversations on social media on antibiotic use and AMR in the context of sore throat using Brandwatch, a social listening platform that allows one to monitor and analyze online conversations [21], to determine beliefs and misconceptions and establish how the COVID-19 pandemic influenced online conversations related to sore throat and AMR. Knowledge obtained from this study will inform strategies and resources that can be developed and implemented to address consumer beliefs and misconceptions and help mitigate AMR.
2. Results
There were ~760,000 social media posts related to AMR and ~3,500,000 social media posts related to sore throat across the eight countries between 1 January 2018 and 25 November 2021. Table 1 shows the full volume of conversations by topic and country. However, this dataset was then sifted through a human-led qualitative analysis to exclude conversations that fell outside of the topics of interest. Twitter was the dominant platform for advice seeking and experience sharing by people experiencing sore throat, while country-specific healthcare forums where consumers seek advice from peers and healthcare professionals (HCPs) were prominent in some countries. In addition, parenting forums were popular sources where parents and pregnant women with sore throats went for advice about treatment and side effects.

Table 1.
Volume of conversations analyzed in the social listening exercise.
The social media listening exercise revealed three critical findings: (1) distinct consumer groups were involved in conversations on antibiotic use in sore throat with a substantial number of opinions based upon misconceptions; (2) COVID-19 impacted conversations on sore throat and AMR; and (3) COVID-19 impacted how the patient responded to early sore throat symptoms.
2.1. Consumer Profiles and Associated Misconceptions around Antibiotic Use in Sore Throat
Five distinct consumer profiles were identified with diverse opinions and beliefs on antibiotic use in sore throat (Table 2).
Table 2.
Consumer profiles deduced in the social media listening exercise and key beliefs observed for each profile.
The first two consumer profiles had the greatest understanding of antibiotics and AMR. Antibiotic-preserving peer educators shared knowledge of the difference between viral and bacterial infections manifesting in sore throat and had a strong opinion on if and when antibiotics should be taken. Consumers in this group tended to share advice only when asked, and while their posts were largely neutral and educational, they appeared to be strongly against antibiotic misuse. Antibiotic-cautious consumers were more hesitant to take antibiotics for a sore throat for different reasons. On one hand, reluctance was due to an awareness of AMR or the knowledge that antibiotics are not indicated for self-limiting sore throat of viral etiology. On the other hand, reluctance stemmed from the perception that antibiotics are ‘too strong’ a medication to take for something as trivial as sore throat; the tone of the conversation by these consumers made it seem that they had a moral reluctance to take antibiotics for sore throat (e.g., that it felt wrong or unethical for them to do so). These consumers often preferred home remedies and symptom relief; however, this was not driven by a belief that ‘natural’ solutions are superior, but rather by the knowledge that sore throat is self-limiting and will resolve over time with symptomatic management.
The third group were categorized as medication-resistant antibiotic opponents, who appeared to prefer home remedies and were reluctant to take antibiotics due to a misunderstanding of AMR. Consumers in this group believed that AMR could be ‘caught through antibiotics’ and believed that antibiotics make bacteria in their body stronger, which was partially reinforced by a concern about missing antibiotic doses and forgetting to finish the full course of treatment. This group also included pregnant women and parents who were hesitant to give/take antibiotics because of a perception that they could cause side effects or weaken the immune system of their child.
The final two consumer profiles appeared to be supporters of antibiotics with a lesser understanding of the mechanism of action of antibiotics. Consumers that were believers in the strength of antibiotics were typically keen to use antibiotics as they believed they are ‘strong medications’ that provide quick relief of symptoms. Consumers in this group were unable to make the distinction between viral and bacterial infections and often felt frustrated when their sore throat did not clear up with antibiotic treatment. Determined pro-antibiotic consumers were part of a smaller group. They often shared their beliefs that antibiotics are ‘strong medications’ and proactively attempted to source antibiotics by trying to persuade their physician. Some consumers even went directly to a pharmacy to obtain antibiotics OTC.
A number of consumer misconceptions were identified, with the most prevalent often being misinterpretations of the science behind AMR rather than outright fallacies. The most common consumer misconception was that antibiotics are strong medications that can treat all types of sore throat (Table 3).
Table 3.
Top four prevalent consumer misconceptions identified across the consumer profiles.
2.2. Impact of COVID-19 on the Sore Throat AMR Conversation
COVID-19 had a multifaceted effect on sore throat and AMR conversations. Firstly, sore throat triggered anxiety in consumers as they feared it may be a symptom of COVID-19, which prompted consumers to test for COVID-19. Secondly, the pandemic led to consumers engaging in conversations around antibiotics and the distinction between viral and bacterial infections in the context of COVID-19, and antibiotics not being effective against viral infections. Furthermore, early in the pandemic, commentary by consumers and HCPs was directed towards people being prescribed antibiotics for COVID-19. A minority of consumers suggested that antibiotic prescriptions for COVID-19 may play a role in the prevention of opportunistic bacterial infections. Finally, public interest in natural remedies for sore throat remained prominent, and possibly even increased during the pandemic, driven by a reluctance to visit healthcare centers for fear of contracting COVID-19 or overburdening the health system, as well as a desire to lead a healthy lifestyle focused on wellness.
In addition to consumers, the study found that other stakeholders played a larger part in conversations that included sore throat, AMR and COVID-19. For example, activities carried out during World Antibiotic Awareness Week (WAAW) by government agencies, health authorities, local branches of the WHO and regional healthcare bodies focused on raising awareness of AMR and the dangers it poses in general, and garnered significant coverage through online platforms. A small proportion of individual campaigners and consumers (largely made up of individuals who fit into peer educator and antibiotic-cautious consumer profile) joined the conversations. Supportive campaigns and conversations around AMR became less prominent during the height of the COVID-19 pandemic, as health authorities focused on tackling COVID-19. Furthermore, many stakeholders outside of government influenced the AMR conversation, including peer educators (e.g., practicing or former HCPs who have carved out a platform in social or traditional media and who publish their own content aimed at combatting antibiotic overuse) and non-healthcare figures in the public domain (e.g., models, TV presenters and politicians).
2.3. Impact of COVID-19 on Patient Response to Early Sore Throat Symptoms
Consumers sought advice for sore throat relief through multiple routes. Consumers seeking advice from people in an individual’s social network was common in online sore throat conversation. Some consumers frequently visited the pharmacy for OTC symptom relief if they did not already have this at home. Meanwhile, other consumers visited their physician or pharmacist immediately, especially when they were unsure if their symptoms were COVID-19-related. In some markets (Russian Federation, Romania, Brazil and Mexico), consumers with sore throat were more likely to demand specific antibiotics from their physician. In other markets (Germany and Italy), consumers attempted to persuade their physician to prescribe antibiotics by stating that they were necessary or exaggerating their symptoms. Antibiotics or antibiotic-containing products frequently mentioned by people experiencing sore throat included amoxicillin (Thailand), amoxicillin combined with clavulanic acid (Thailand), penicillin V (Germany), Benzetacil (benzyl penicillin) (Brazil), Grammidin (gramicidin) (Russian Federation), and Bioparox (fusafungine) spray (Romania). A trigger for visiting primary care/family physicians was when symptoms worsened or lingered for some time and depended on factors related to COVID-19, such as the desire to test and fear of infection, as well as factors related to the health systems (e.g., cost of services). In addition, in countries where antibiotics were more commonly available without a prescription directly from the pharmacy (even in situations where it is illegal), some consumers went directly to the pharmacy to access treatment.
3. Discussion
To our knowledge this is the first study to examine consumer beliefs and conversations on sore throat, antibiotics and AMR, and the impact that the COVID-19 pandemic has had on such conversations, using posts from multiple social platforms and forums. Our study assessed a large number of social media posts, which allowed us to unpack the diverse consumer beliefs related to antibiotic use. We found that consumer conservations were clustered, which allowed us to define five distinct groups, with many groups’ opinions based upon misconceptions. In addition, COVID-19 impacted conversations around sore throat and AMR and how patients respond to early sore throat symptoms.
Beliefs and misconceptions observed among the five groups aligned with previous studies. At one end of the scale were antibiotic-preserving peer educators and antibiotic-cautious consumers who had the greatest understanding of antibiotics and AMR. Other survey-based studies also found that there were a proportion of patients (between 36.5% and ~50%) who clearly understand that antibiotics are only effective against bacterial infections [6,11,13]. Previous studies have also revealed an understanding of AMR among patients. A large proportion of patients (73.7% to 85%) were aware that unnecessary use of antibiotics compromise their efficacy in the future [6,12,13], while 72% were aware that many infections are becoming increasingly resistant to treatment by antibiotics [10]. Furthermore, 84.1% of patients understood that bacteria can become resistant to antibiotics, while 61.5% understood that the prescribed course of antibiotics needed to be taken or they may not work in the future [13]. Meanwhile, determined pro-antibiotic consumers and believers in the strength of antibiotics who were in favor of antibiotics had the least understanding of how antibiotics work, believing that antibiotics are strong medications suitable for all types of sore throat (bacterial and viral). Survey-based studies have revealed that a substantial number of patients (36.5% to 71%) believe that antibiotics are effective in treating viral infections [6,10,11,12,13,14,15]. We also found that determined pro-antibiotic consumers proactively attempted to source antibiotics by trying to persuade their physician. Similarly, a study that utilized video recordings of adult primary care consultations found that many patients conveyed subtle forms of pressure towards their physician to obtain antibiotics [22]. Sitting between consumers with the greatest understanding of antibiotics and AMR and those in favor of antibiotics in our study were medication-resistant antibiotic opponents, who were reluctant to take antibiotics due to a misunderstanding of AMR. A questionnaire-based study also found that there was a reluctance among some patients to take antibiotics for reasons different to what was found in our study. In the questionnaire-based study, patients were reluctant to take antibiotics due to a concern about bacterial resistance, although it is important to note that patients who expressed this concern had experienced challenges with antibiotic treatment, thought that antibiotics were generally ineffective and did not hesitate to stop treatment inappropriately [23]. The belief that antibiotics are strong medications, capable of treating bacterial and viral infections was evident across all eight countries included in the study.
For HCPs to help address consumer misconceptions, we recommend a multifaceted approach. Firstly, we would suggest that HCPs become knowledgeable on the identified consumer profiles and the desired messages that should be conveyed to bring a shift in belief/behavior. Secondly, as it may be difficult to determine the beliefs of a consumer on first contact, we would suggest utilizing open-ended statements and questions to explore what consumers are looking for and identify any misconceptions. Once this information has been gathered, messages can be customized and relevant decision aids and knowledge bites on appropriate antibiotic use and symptomatic management can be provided, to address misconceptions and empower the consumer to make appropriate health decisions (Table 4). A simple call-to-action model, such as the ACE model for engagement developed by the Global Respiratory Infection Partnership, would be useful to ensure that HCPs are clear on the steps that should be taken to bring about a belief/behavior change. The ACE model recommends that HCPs: Ask questions to establish the understanding of AMR by the consumer and identify misconceptions; Customize messages according to the consumer profile; Empower consumers with the knowledge to understand the cause of their illness and why symptomatic relief can be effective.
Table 4.
Strategies to address misconceptions related to antibiotic strength and AMR.
The large number of social media posts analyzed in our study indicated that social media platforms are regularly used by various stakeholders to share opinions and perspectives and engage in discussions. Other studies have also found that social media is widely used by patients to source information and connect with their peers, healthcare organizations and HCPs [19,24,25,26]. The extensive use of social media provides opportunities to leverage such platforms to provide targeted education/messaging on public health issues such as AMR in a swift manner, which could help dispel misconceptions and translate into remedial action. When thinking about developing targeted education and messaging for use on social media, we would recommend the consideration of multiple factors. Firstly, it is important to consider the social platform that is used, whether there are any guidelines that should be considered, and if the message will translate as intended. For example, Twitter, which was the most commonly used platform in our study, has a maximum character limit of 280 [27]. Secondly, the format of social media content should be considered. By providing succinct content that is straightforward and visually engaging, the consumers’ attention can be captured and sustained. It is also critical to use language that consumers will understand versus more scientific language. Based on the number of misconceptions observed in our study, it could be argued that language and messaging on antibiotics and AMR may need to change. Furthermore, it is important that targeted education and messages are tailored according to the different profiles, to ensure that the appropriate misconceptions are being dispelled. Finally, the age group of the target audience should be considered and social media platforms that are more commonly used by these audiences should be utilized.
Along with the development of social media content to provide education and convey messages, consumers and HCPs that are less familiar with social media should not be overlooked. We recommend that targeted educational materials (e.g., short videos, easy-to-read booklets) remain available within the healthcare setting to ensure all consumers continue to receive relevant education. Notably, future HCPs (including community pharmacists and pharmacy counter assistants) are likely to be digitally native in their forms of communication and digital social engagement, meaning that they may not need as much training and education in this area. However, it is essential that future HCPs receive appropriate training on the different consumer profiles that have been identified in this study, along with AMR and antimicrobial stewardship [28], so that they can convey the correct information effectively to consumers, both in person and via social media.
Social media can be a useful tool for health promotion, providing communication opportunities between several stakeholders and audiences [29]. However, it can also be a source for misinformation [30]. Our study did not examine where consumer misconceptions originated from; however, social media could have played a part. We recommend that various stakeholders play a role in helping to mitigate the spread of misinformation and convey the correct messaging to consumers. Some stakeholders may need to work with social influencers, who are becoming more common in the healthcare space, as they have a greater understanding of the social media space and better reach. It is important to note that if stakeholders utilize influencers, they will not have the same control on content; therefore, it is important to educate influencers on the objective and the evidence that underpins the intended messaging and consider legal/regulatory frameworks.
COVID-19 had a multifaceted effect on sore throat and AMR conversations. For example, sore throat triggered anxiety in consumers as they feared it may be a symptom of COVID-19, which prompted them to carry out diagnostic testing. Interestingly, supportive campaigns and conversations around AMR became less prominent during the height of the COVID-19 pandemic, as health authorities focused on tackling COVID-19. Given that AMR remains a major health issue, we recommend that communications should be refocused on how inappropriate antibiotic use can contribute to AMR and the threat that it poses and should leverage our learnings from the COVID-19 pandemic.
In addition to targeted materials, messages and approaches to address consumer misconceptions on sore throat and antibiotic use, additional strategies could be employed to further help in the fight against AMR. Most cases of sore throat (up to 80%) are of viral etiology, meaning that antibiotics will not work [31]. Furthermore, as the symptoms of bacterial and viral infections are similar, it can be difficult to make a diagnosis from symptoms alone [32]. Therefore, point-of-care testing (POCT) could be implemented in primary care settings (e.g., pharmacy and general practice) to help distinguish between the cause of sore throat (viral or bacterial) in a rapid manner, enhance the quality of antibiotic prescribing decisions and help to guide self-care options for consumers [32]. Although there are challenges associated with POCT, such as the training required for HCPs, throat swab testing has become more familiar for patients following the COVID-19 pandemic. In addition, previous studies have demonstrated that POCT within the community pharmacy setting can reduce the number of inappropriate antibiotic prescriptions [33,34]. Bacterial microorganisms are capable of developing resistance to some antimicrobial agents through various mechanisms of resistance [3]. Most cases of sore throat with a bacterial etiology are caused by Streptococcus pyogenes (S. pyogenes) [35]. Penicillin resistance has not been reported for S. pyogenes; therefore, it is considered the antibiotic of choice for the treatment of group A streptococcal pharyngitis [36]. However, in cases where treatment fails (for example due to inadequate dosing), it is important to detect potential drug resistance and confirm susceptibility of the bacterial strain, to ensure that the most appropriate alternative antibiotic is prescribed [36,37,38]. Beyond POCT, antimicrobial susceptibility testing (AST) could be utilized to determine which antimicrobials will inhibit bacterial growth and ensure that the correct antibiotic regimen is provided to patients [37]. Various AST methods are available, which can provide accurate detection of antimicrobial resistance mechanisms when used correctly. However, it is important to note that they do come with some challenges, such as the speed in which results are produced from microbial culture and susceptibility testing; it is a two to three day process, which could in turn delay antibiotic administration [38,39]. It is important to also note the study limitations. Firstly, the study relied on qualitative rather than quantitative analysis. Therefore, future studies that assess the prevalence of different antibiotic consumer profiles and quantitatively characterize conversations across different social media platforms would be beneficial. In addition, as a qualitative approach was taken and the analysis looked at the totality of conversations within a defined timeframe, there was no ability to define a sample size. Secondly, the demographics present online in the discussion of antibiotics and sore throat may not be representative of the population. Thirdly, Brandwatch only has access to public social media accounts, meaning that there could have been significant conversations among people experiencing sore throat on private social media channels (e.g., individuals’ private Facebook accounts) that were not captured. Finally, it is important to note that retweets/reposts formed part of the overall dataset, and it is possible that automated posts/bot accounts could have formed part of the dataset. However, as analyzers focused on conversations by individuals first and foremost in the qualitative analysis, we do not expect retweets/reposts or bot accounts to have had a significant impact on our findings.
4. Materials and Methods
This was a multinational, observational, consumer content analysis study initiated and commissioned by Reckitt, the maker of Strepsils. The study was conducted across eight countries: Germany, Italy, Spain, Mexico, Brazil, Thailand, Romania and the Russian Federation. Social media searches were conducted between 1 January 2018 and 25 November 2021 to explore conversations around AMR and sore throat and the effect of COVID-19 on online conversations by contrasting the conversation before and after 1 January 2020. The master search terms in English are provided in Table 5 and Table 6. These terms were translated as appropriate. Social media posts from Twitter, Reddit, YouTube, forums, blogs, Facebook and Instagram posted by the general public, patients (people experiencing sore throat), healthcare organizations and HCPs in the main local language were included. Figure 1 provides an overview of the steps involved in the study.
Table 5.
Master English search terms for ‘Sore Throat’ used on Brandwatch.
Table 6.
Master English search terms for ‘AMR’ used on Brandwatch.
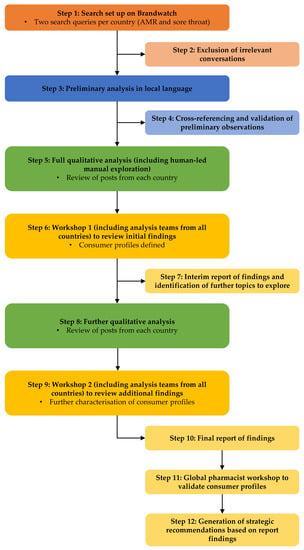
Figure 1.
Schematic of study methodology. AMR, antimicrobial resistance.
During Step 1, Brandwatch, a social listening platform that allows one to monitor and analyze what is being said online about brands, people and products [21], was utilized to set up two separate search queries that were translated into local language by individual analysts. The search queries captured relevant conversations across social media platforms around AMR (explicit and implicit references to this) and sore throat, and among the abovementioned stakeholders, which was followed by data cleaning to remove irrelevant conversations as Step 2. This iterative process involved the review of a portion of the dataset to identify any recurring unintended themes (e.g., the term ‘multidrug resistant’ pulled in many cancer-related conversations) and subsequent adjustment and refinement of the search terms. In addition, any records that were not geotagged to one of the eight countries of interest were removed from the data set at this stage.
Step 3 consisted of a preliminary analysis, which was conducted in local languages. During this step, social media conversations were reviewed by analysts to identify and summarize the most prevalent themes (‘conversation drivers’) of the conversations around antibiotics in the context of sore throat. Data were then distilled into an initial update by cross-referencing and validating the preliminary observations (Step 4).
The first qualitative analysis was conducted (Step 5) by a team of social media analysts who were proficient in the local language of each country. The analysis explored how antibiotics were being perceived and used by consumers within the context of sore throat. Data collection via Brandwatch was supplemented with extensive human-led manual identification and exploration of additional forums and data-limited channels. These additional country-specific sources were identified by analysts with local country knowledge, and through internet searches using the terms that had featured most prominently within the conversations identified via Brandwatch. The full qualitative analysis included the review of ~2500 posts per country and focused on the following topics: sore throat diagnosis; sore throat tests; sore throat self-treatment; sore throat hospital treatment; sore throat treatment with antibiotics; health literacy; AMR in the context of sore throat; consumer perception of antibiotic policy (in the context of the country stance on antibiotic use) and campaigns; antibiotic availability; key influencers (celebrities and public figures) discussing AMR; and the biggest changes in AMR conversations before and after the advent of the COVID-19 pandemic.
Following qualitative analysis, the first workshop was held to define the consumer profiles (Step 6). Workshop participants included analysis teams from all countries, Reckitt and Lumanity (the agency commissioned to carry out the study). Key beliefs and perceptions were summarized and organized along two axes: ‘in favor of antibiotics’ versus ‘opposed to antibiotics’ and ‘health literate’ versus ‘misinformed’. Where multiple individual beliefs were clustered together, these were grouped into different consumer profiles. An interim report was generated outlining the preliminary findings and identifying the additional key questions to explore (Step 7).
Step 8 consisted of a subsequent qualitative analysis to further refine and add detail to the consumer profiles, including discussions centering on consumer perceptions of interactions with HCPs in the path of receiving antibiotics; biggest changes in the sore throat conversations before and after the advent of the COVID-19 pandemic; sore throat channel breakdown analysis to determine which social media channels were used by different stakeholder groups and which were the most prominent types of conversation on these channels; WAAW; and Strepsils. During the second workshop (Step 9), analysis teams from each country, Reckitt and Lumanity assessed the prevalence of consumer profiles and shifts due to COVID-19. Key findings from the qualitative analyses and the workshops were distilled into a final report (Step 10) detailing the main areas of implications and the key messages from the study.
Key themes from the social media research were presented to a global group of pharmacists attending a Global Respiratory Infection Partnership workshop, which was held at an international pharmacy conference (80th International Pharmaceutical Federation (FIP) World Congress of Pharmacy and Pharmaceutical Sciences 2022). The workshop assessed whether consumer profiles and perceptions were recognized by pharmacists in their country. In addition, the workshop aimed to define the questions consumers in each profile should be asked and potential responses that could be provided to address misconceptions (Step 11). The analysis formed the basis for our recommended strategies and resources that could be implemented to address consumer misconceptions and help tackle AMR (Step 12).
5. Conclusions
Our social media listening study illustrated a number of misconceptions on sore throat, antibiotic use and AMR, and further showed that COVID-19 has impacted conversations and the patient response to early sore throat symptoms. The knowledge obtained from the study provides an opportunity to address the diverse consumer misconceptions through HCP interventions, both in person and in the social media space, and via other stakeholders, to effectively mitigate the challenge of AMR. One of the objectives of the WHO global action plan on AMR is to increase the awareness and understanding of AMR using strategies that focus on communication. Therefore, future efforts should focus on developing materials and messages that tackle identified misconceptions in a succinct and impactful way. In addition, finding the right people and channels to spread correct messaging to address misconceptions is of great importance.
Author Contributions
Conceptualization, S.E., J.B., D.B., K.E., W.T., T.M., A.S. and E.L.-P.; methodology, data curation, formal analysis and investigation, T.M. and A.S.; writing-original draft, S.E., J.B., D.B., K.E., W.T., T.M., A.S. and E.L.-P.; writing-reviewing and editing, S.E., J.B., D.B., K.E., W.T., T.M., A.S. and E.L.-P. All authors approved the final content and are wholly accountable for its content. All authors have read and agreed to the published version of the manuscript.
Funding
Funding for this manuscript was provided by Reckitt Benckiser Healthcare International Ltd., UK.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data are contained in the article.
Acknowledgments
Medical writing assistance was provided by Abby Armitt of Elements Communications Ltd., Westerham, UK and was funded by Reckitt Benckiser Healthcare International Ltd., UK.
Conflicts of Interest
D.B., E.L.P., J.B., K.E., S.E. and W.T. are members of the Global Respiratory Infection Partnership, which is supported by an unrestricted educational grant from Reckitt Benckiser Healthcare International Ltd., UK. T.M. is an employee of Lumanity, who received funding from Reckitt Benckiser Healthcare International Ltd., UK. A.S. is an employee of Reckitt Benckiser Healthcare International Ltd., UK.
References
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance: Key Facts. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 4 October 2022).
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018, 4, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. P&T 2015, 40, 277–283. [Google Scholar]
- European Commission. Special Eurobarometer 522 Report Antimicrobial Resistance. 2022. Available online: https://www.eunews.it/wp-content/uploads/2022/11/Antimicrobial_Resistance_ebs_522_report_en.pdf (accessed on 8 December 2022).
- Centers for Disease Control and Prevention. Be Antibiotics Aware: Smart Use, Best Care. 2021. Available online: https://www.cdc.gov/patientsafety/features/be-antibiotics-aware.html (accessed on 24 January 2023).
- Mustafa, Z.; Ghaffari, M. Diagnostic methods, clinical guidelines, and antibiotic treatment for group A Streptococcal pharyngitis: A narrative review. Front. Cell Infect. Microbiol. 2020, 10, 563627. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.; Robotham, J.V.; Smieszek, T. Actual versus ‘ideal’ antibiotic prescribing for common conditions in English primary care. J. Antimicrob. Chemother. 2018, 73, 19–26. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/194460/9789241509817_eng.pdf (accessed on 9 November 2022).
- Cals, J.W.; Boumans, D.; Lardinois, R.J.; Gonzales, R.; Hopstaken, R.M.; Butler, C.C.; Dinant, G.J. Public beliefs on antibiotics and respiratory tract infections: An internet-based questionnaire study. Br. J. Gen. Pract. 2007, 57, 942–947. [Google Scholar] [CrossRef]
- Widayati, A.; Suryawati, S.; de Crespigny, C.; Hiller, J.E. Knowledge and beliefs about antibiotics among people in Yogyakarta City Indonesia: A cross sectional population-based survey. Antimicrob. Resist. Infect. Control 2012, 1, 38. [Google Scholar] [CrossRef]
- Gaarslev, C.; Yee, M.; Chan, G.; Fletcher-Lartey, S.; Khan, R. A mixed methods study to understand patient expectations for antibiotics for an upper respiratory tract infection. Antimicrob. Resist. Infect. Control 2016, 5, 39. [Google Scholar] [CrossRef]
- Davis, M.E.; Liu, T.L.; Taylor, Y.J.; Davidson, L.; Schmid, M.; Yates, T.; Scotton, J.; Spencer, M.D. Exploring patient awareness and perceptions of the appropriate use of antibiotics: A mixed-methods study. Antibiotics 2017, 6, 23. [Google Scholar] [CrossRef]
- Altiner, A.; Duerden, M.; Kozlov, R.; López-Pintor, E.; Sessa, A.; Shephard, A.; van der Velden, A.W. Understanding attitudes and perceptions of consumers in relation to antibiotic use for respiratory illnesses and symptoms in Europe. In Proceedings of the 33rd European Congress of Clinical Microbiology & Infectious Diseases (P2298), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Bakhit, M.; Del Mar, C.; Gibson, E.; Hoffmann, T. Exploring patients’ understanding of antibiotic resistance and how this may influence attitudes towards antibiotic use for acute respiratory infections: A qualitative study in Australian general practice. BMJ Open 2019, 9, e026735. [Google Scholar] [CrossRef]
- Statista. Number of Social Media Users Worldwide from 2018 to 2027 (In Billions). 2023. Available online: https://www.statista.com/statistics/278414/number-of-worldwide-social-network-users/ (accessed on 10 November 2022).
- Gatewood, J.; Monks, S.L.; Singletary, C.R.; Vidrascu, E.; Moore, J.B. Social media in public health: Strategies to distill, package, and disseminate public health research. J. Public Health Manag. Pract. 2020, 26, 489–492. [Google Scholar] [CrossRef]
- Chen, J.; Wang, Y. Social media use for health purposes: Systematic review. J. Med. Internet Res. 2021, 23, e17917. [Google Scholar] [CrossRef]
- Kubheka, B.Z.; Carter, V.; Mwaura, J. Social media health promotion in South Africa: Opportunities and challenges. Afr. J. Prim. Health Care Fam. Med. 2020, 12, e1–e7. [Google Scholar] [CrossRef]
- Brandwatch. The Complete Social Listening Guide. 2022. Available online: https://www.brandwatch.com/blog/social-listening-guide/ (accessed on 8 December 2022).
- Stivers, T.; Timmermans, S. Arriving at no: Patient pressure to prescribe antibiotics and physicians’ responses. Soc. Sci. Med. 2021, 290, 114007. [Google Scholar] [CrossRef]
- Bagnulo, A.; Muñoz Sastre, M.T.; Kpanake, L.; Sorum, P.C.; Mullet, E. Why patients want to take or refuse to take antibiotics: An inventory of motives. BMC Public Health 2019, 19, 441. [Google Scholar] [CrossRef]
- Jha, A.; Lin, L.; Savoia, E. The use of social media by state health departments in the US: Analyzing health communication through Facebook. J. Community Health 2016, 41, 174–179. [Google Scholar] [CrossRef]
- Ranschaert, E.R.; Van Ooijen, P.M.; McGinty, G.B.; Parizel, P.M. Radiologists’ usage of social media: Results of the RANSOM survey. J. Digit. Imaging 2016, 29, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Smailhodzic, E.; Hooijsma, W.; Boonstra, A.; Langley, D.J. Social media use in healthcare: A systematic review of effects on patients and on their relationship with healthcare professionals. BMC Health Serv. Res. 2016, 16, 442. [Google Scholar] [CrossRef]
- Twitter. Counting Characters. 2023. Available online: https://developer.twitter.com/en/docs/counting-characters (accessed on 10 January 2023).
- Elmahi OK, O.; Uakkas, S.; Olalekan, B.Y.; Damilola, I.A.; Adedeji, O.J.; Hasan, M.M.; Costa, A.C.S.; Ahmad, S.; Essar, M.Y.; Thomson, D.J. Antimicrobial resistance and one health in the post COVID-19 era: What should health students learn? Antimicrob. Resist. Infect. Control 2022, 11, 58. [Google Scholar] [CrossRef]
- Zucco, R.; Lavano, F.; Anfosso, R.; Bianco, A.; Pileggi, C.; Pavia, M. Internet and social media use for antibiotic-related information seeking: Findings from a survey among adult population in Italy. Int. J. Med. Inform. 2018, 111, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Del Vicario, M.; Bessi, A.; Zollo, F.; Petroni, F.; Scala, A.; Caldarelli, G.; Stanley, H.E.; Quattrociocchi, W. The spreading of misinformation online. Proc. Natl. Acad. Sci. USA 2016, 113, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Wolford, R.W.G.; Syed, A.B.; Schaefer, S.T.J. Pharyngitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Essack, S.; Bell, J.; Burgoyne, D.; Tongrod, W.; Duerden, M.; Sessa, A.; Altiner, A.; Shephard, A. Point-of-Care Testing for Pharyngitis in the Pharmacy. Antibiotics 2020, 9, 743. [Google Scholar] [CrossRef]
- Demoré, B.; Tebano, G.; Gravoulet, J.; Wilcke, C.; Ruspini, E.; Birgé, J.; Boivin, J.-M.; Hénard, S.; Dieterling, A.; Munerol, L.; et al. Rapid antigen test use for the management of group A streptococcal pharyngitis in community pharmacies. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1637–1645. [Google Scholar] [CrossRef]
- Papastergiou, J.; Trieu, C.R.; Saltmarche, D.; Diamantouros, A. Community pharmacist-directed point-of-care group A Streptococcus testing: Evaluation of a Canadian program. J. Am. Pharm. Assoc. 2018, 58, 450–456. [Google Scholar] [CrossRef]
- Ogawa, T.; Terao, Y.; Sakata, H.; Okuni, H.; Ninomiya, K.; Ikebe, K.; Maeda, Y.; Kawabata, S. Epidemiological characterization of Streptococcus pyogenes isolated from patients with multiple onsets of pharyngitis. FEMS Microbiol. Lett. 2011, 318, 143–151. [Google Scholar] [CrossRef]
- Giovanetti, E.; Prenna, M.; Repetto, A.; Biavasco, F.; Romagnoli, M.; Ripa, S.; Varaldo, P.E. Susceptibility of Streptococcus pyogenes from throat cultures to macrolide antibiotics and influence of collection criteria. Clin. Microbiol. Infect. 1997, 3, 58–62. [Google Scholar] [CrossRef]
- Bayot, M.L.; Bragg, B.N. Antimicrobial Susceptibility Testing. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Jorgensen, J.H.; Ferraro, M.J. Antimicrobial susceptibility testing: A review of general principles and contemporary practices. Clin. Infect. Dis. 2009, 49, 1749–1755. [Google Scholar] [CrossRef]
- van Belkum, A.; Bachmann, T.T.; Lüdke, G.; Lisby, J.G.; Kahlmeter, G.; Mohess, A.; Becker, K.; Hays, J.P.; Woodford, N.; Mitsakakis, K.; et al. Developmental roadmap for antimicrobial susceptibility testing systems. Nat. Rev. Microbiol. 2019, 17, 51–62. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).