
National Level Cross-Sectional Study on Antibiotic Use in Children during the Pre- and Early COVID-19 Eras


Abstract
:1. Introduction
2. Results
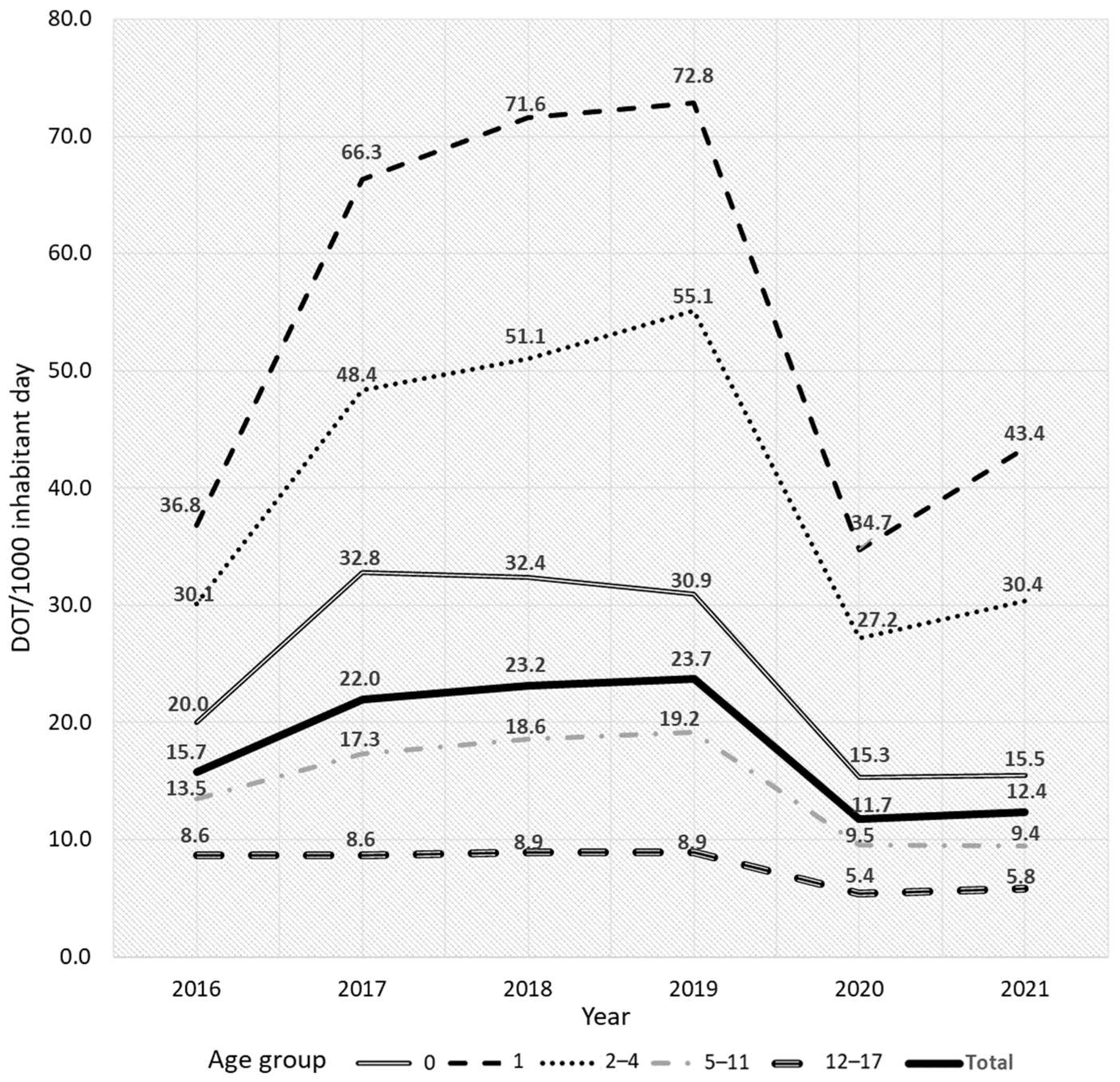
2.1. Demographics and Analyses by Age Group and Year
2.2. Patterns of Prescribed Classes of Antibiotics by Age Group
2.3. Temporal Trends in Antibiotic Prescription
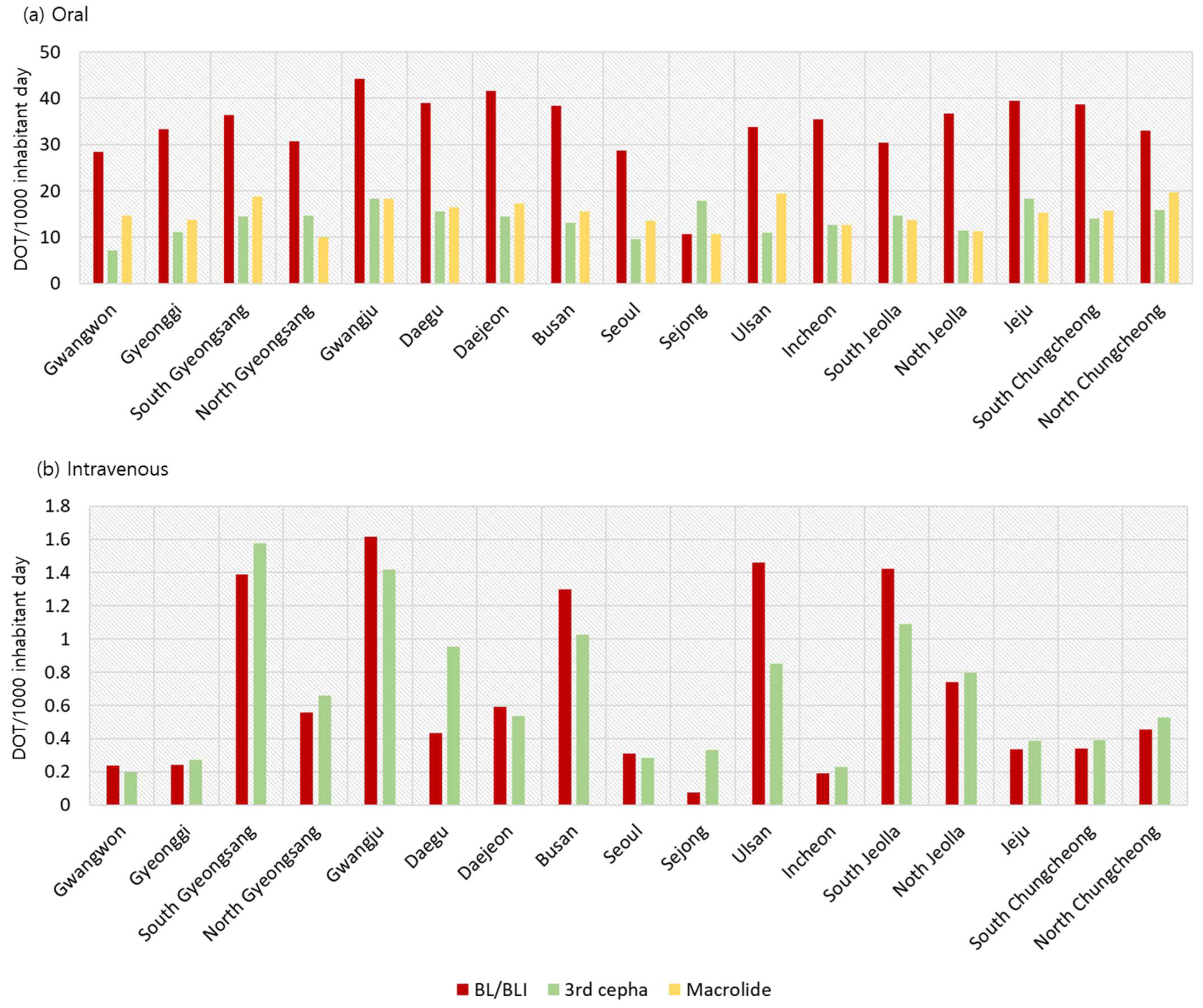
2.4. Analyses of Antibiotic Prescriptions by Region
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCaig, L.F.; Hughes, J.M.J.J. Trends in antimicrobial drug prescribing among office-based physicians in the United States. JAMA 1995, 273, 214–219. [Google Scholar] [CrossRef]
- Park, J.; Han, E.; Lee, S.O.; Kim, D.S. Antibiotic use in South Korea from 2007 to 2014: A health insurance database-generated time series analysis. PLoS ONE 2017, 12, e0177435. [Google Scholar] [CrossRef]
- Park, J.Y.; Kang, H.M.; Kwak, E.M.; Rhim, J.W.; Ahn, Y.H.; Lee, H.; Jeong, D.C.; Kang, J.H. Impact of Antibiotic Prescribing Patterns on Susceptibilities of Uropathogens in Children below 24 Months Old. Antibiotics 2020, 9, 915. [Google Scholar] [CrossRef]
- Belongia, E.A.; Sullivan, B.J.; Chyou, P.-H.; Madagame, E.; Reed, K.D.; Schwartz, B.J.P. A community intervention trial to promote judicious antibiotic use and reduce penicillin-resistant Streptococcus pneumoniae carriage in children. Pediatrics 2001, 108, 575–583. [Google Scholar] [CrossRef]
- Finkelstein, J.A.; Davis, R.L.; Dowell, S.F.; Metlay, J.P.; Soumerai, S.B.; Rifas-Shiman, S.L.; Higham, M.; Miller, Z.; Miroshnik, I.; Pedan, A.J.P. Reducing antibiotic use in children: A randomized trial in 12 practices. Pediatrics 2001, 108, 1–7. [Google Scholar] [CrossRef]
- Holstiege, J.; Schulz, M.; Akmatov, M.K.; Steffen, A.; Bätzing, J. Marked reductions in outpatient antibiotic prescriptions for children and adolescents—A population-based study covering 83% of the paediatric population, Germany, 2010 to 2018. Euro. Surveill. 2020, 2, 1900599. [Google Scholar] [CrossRef]
- Park, K.H.; Choe, S.A.; Shin, J.Y.; Choe, Y.J. Trend of Antibiotic Use in Children with Acute Otitis Media in Korea. J. Korean Med. Sci. 2021, 36, e317. [Google Scholar] [CrossRef]
- Yum, S.; Hong, K.; Sohn, S.; Kim, J.; Chun, B.C. Trends in Viral Respiratory Infections During COVID-19 Pandemic, South Korea. Emerg. Infect. Dis. 2021, 27, 1685–1688. [Google Scholar] [CrossRef]
- Choe, Y.J.; Shin, J.Y. Trends in the use of antibiotics among Korean children. Korean J. Pediatr. 2019, 62, 113–118. [Google Scholar] [CrossRef]
- Truong, J.; Cointe, A.; Le Roux, E.; Bidet, P.; Michel, M.; Boize, J.; Mariani-Kurkdjian, P.; Caseris, M.; Hobson, C.A.; Desmarest, M.; et al. Clinical impact of a gastrointestinal PCR panel in children with infectious diarrhoea. Arch. Dis. Child 2022, 107, 601–605. [Google Scholar] [CrossRef]
- Zanichelli, V.; Sharland, M.; Cappello, B.; Moja, L.; Getahun, H.; Pessoa-Silva, C.; Sati, H.; van Weezenbeek, C.; Balkhy, H.; Simão, M.; et al. The WHO AWaRe (Access, Watch, Reserve) antibiotic book and prevention of antimicrobial resistance. Bull. World Health Organ 2023, 101, 290–296. [Google Scholar] [CrossRef]
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M.; et al. Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef]
- Youngster, I.; Avorn, J.; Belleudi, V.; Cantarutti, A.; Díez-Domingo, J.; Kirchmayer, U.; Park, B.J.; Peiró, S.; Sanfélix-Gimeno, G.; Schröder, H.; et al. Antibiotic Use in Children—A Cross-National Analysis of 6 Countries. J. Pediatr 2017, 182, 239–244.e231. [Google Scholar] [CrossRef]
- Song, Y.K.; Han, N.; Kim, M.G.; Chang, H.J.; Sohn, H.S.; Ji, E.; Oh, J.M. A national pharmacoepidemiological study of antibiotic use in Korean paediatric outpatients. Arch. Dis. Childh. 2017, 102, 660–666. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef]
- Kinoshita, N.; Morisaki, N.; Uda, K.; Kasai, M.; Horikoshi, Y.; Miyairi, I. Nationwide study of outpatient oral antimicrobial utilization patterns for children in Japan (2013–2016). J. Infect. Chemother. 2019, 25, 22–27. [Google Scholar] [CrossRef]
- Petersen, M.R.; Cosgrove, S.E.; Quinn, T.C.; Patel, E.U.; Kate Grabowski, M.; Tobian, A.A.R. Prescription Antibiotic Use Among the US population 1999-2018: National Health and Nutrition Examination Surveys. Open. Forum. Infect. Dis. 2021, 8, ofab224. [Google Scholar] [CrossRef]
- Ryu, S.; Kim, S.; Kim, B.I.; Klein, E.Y.; Yoon, Y.K.; Chun, B.C. Temporal relationship between antibiotic use and respiratory virus activities in the Republic of Korea: A time-series analysis. Antimicrob. Resist. Infect. Control 2018, 7, 56. [Google Scholar] [CrossRef]
- Yoon, Y.K.; Park, G.C.; An, H.; Chun, B.C.; Sohn, J.W.; Kim, M.J. Trends of Antibiotic Consumption in Korea According to National Reimbursement Data (2008–2012): A Population-Based Epidemiologic Study. Medicine 2015, 94, e2100. [Google Scholar] [CrossRef]
- Kim, Y.A.; Park, Y.S.; Youk, T.; Lee, H.; Lee, K. Changes in Antimicrobial Usage Patterns in Korea: 12-Year Analysis Based on Database of the National Health Insurance Service-National Sample Cohort. Sci. Rep. 2018, 8, 12210. [Google Scholar] [CrossRef]
- Lieberthal, A.S.; Carroll, A.E.; Chonmaitree, T.; Ganiats, T.G.; Hoberman, A.; Jackson, M.A.; Joffe, M.D.; Miller, D.T.; Rosenfeld, R.M.; Sevilla, X.D.; et al. The Diagnosis and Management of Acute Otitis Media. Pediatrics 2013, 131, e964–e999. [Google Scholar] [CrossRef]
- Kim, B.; Lee, M.J.; Moon, S.M.; Park, S.Y.; Song, K.H.; Lee, H.; Park, J.S.; Lee, M.S.; Choi, S.M.; Yeom, J.S.; et al. Current status of antimicrobial stewardship programmes in Korean hospitals: Results of a 2018 nationwide survey. J. Hosp. Infect. 2020, 104, 172–180. [Google Scholar] [CrossRef]
- Park, S.; Soumerai, S.B.; Adams, A.S.; Finkelstein, J.A.; Jang, S.; Ross-Degnan, D. Antibiotic use following a Korean national policy to prohibit medication dispensing by physicians. Health Policy Plan 2005, 20, 302–309. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Patients | p | No. of Prescriptions | p | |||
|---|---|---|---|---|---|---|
| N = 170,309,944 | % | N = 257,088,265 | % | |||
| Prescribed place | <0.001 | <0.001 | ||||
| Outpatient department | 161,087,148 | 94.58 | 247,633,761 | 96.32 | ||
| Ward | 9,222,796 | 5.42 | 9,454,504 | 3.68 | ||
| Type of medical care center | <0.001 | <0.001 | ||||
| Tertiary general hospital | 2,465,394 | 1.45 | 2,716,220 | 1.06 | ||
| General hospital | 9,097,375 | 5.34 | 11,510,181 | 4.48 | ||
| Hospital | 25,487,538 | 14.97 | 36,939,583 | 14.37 | ||
| Primary care clinic | 131,411,559 | 77.16 | 203,832,791 | 79.29 | ||
| Others | 1,848,078 | 1.09 | 2,089,490 | 0.81 | ||
| Administered route | <0.001 | <0.001 | ||||
| Oral | 162,634,775 | 95.49 | 248,272,470 | 96.57 | ||
| Intravenous | 7,675,169 | 4.51 | 8,815,795 | 3.43 | ||
| Age group | ||||||
| 0 | 8,190,624 | 4.81 | 13,409,391 | 5.22 | ||
| 1 | 20,130,364 | 11.82 | 34,373,178 | 13.37 | ||
| 2–4 | 53,420,071 | 31.37 | 86,923,974 | 33.81 | ||
| 5–11 | 57,894,436 | 33.99 | 83,205,024 | 32.36 | ||
| 12–17 | 30,674,449 | 18.01 | 39,176,698 | 15.24 | ||
| Age Group (Years Old) | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|
| 0 | 393,674 | 345,786 | 317,685 | 295,132 | 265,087 | 253,946 |
| 1 | 441,720 | 409,814 | 361,625 | 330,970 | 304,651 | 274,633 |
| 2–4 | 1,368,877 | 1,323,515 | 1,294,934 | 1,219,020 | 1,107,285 | 1,001,890 |
| 5–11 | 3,248,187 | 3,302,078 | 3,293,789 | 3,239,207 | 3,215,416 | 3,180,414 |
| 12–17 | 3,283,593 | 3,099,254 | 2,908,302 | 2,844,578 | 2,818,507 | 2,773,061 |
| Total | 8,736,051 | 8,480,447 | 8,176,335 | 7,928,907 | 7,710,946 | 7,483,944 |
| Newborns | 406,243 | 357,771 | 326,822 | 302,676 | 272,337 | 260,562 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.Y.; Kang, H.M. National Level Cross-Sectional Study on Antibiotic Use in Children during the Pre- and Early COVID-19 Eras. Antibiotics 2024, 13, 249. https://doi.org/10.3390/antibiotics13030249
Park JY, Kang HM. National Level Cross-Sectional Study on Antibiotic Use in Children during the Pre- and Early COVID-19 Eras. Antibiotics. 2024; 13(3):249. https://doi.org/10.3390/antibiotics13030249
Chicago/Turabian StylePark, Ji Young, and Hyun Mi Kang. 2024. "National Level Cross-Sectional Study on Antibiotic Use in Children during the Pre- and Early COVID-19 Eras" Antibiotics 13, no. 3: 249. https://doi.org/10.3390/antibiotics13030249
APA StylePark, J. Y., & Kang, H. M. (2024). National Level Cross-Sectional Study on Antibiotic Use in Children during the Pre- and Early COVID-19 Eras. Antibiotics, 13(3), 249. https://doi.org/10.3390/antibiotics13030249