3.1. Antibiotic Consumption
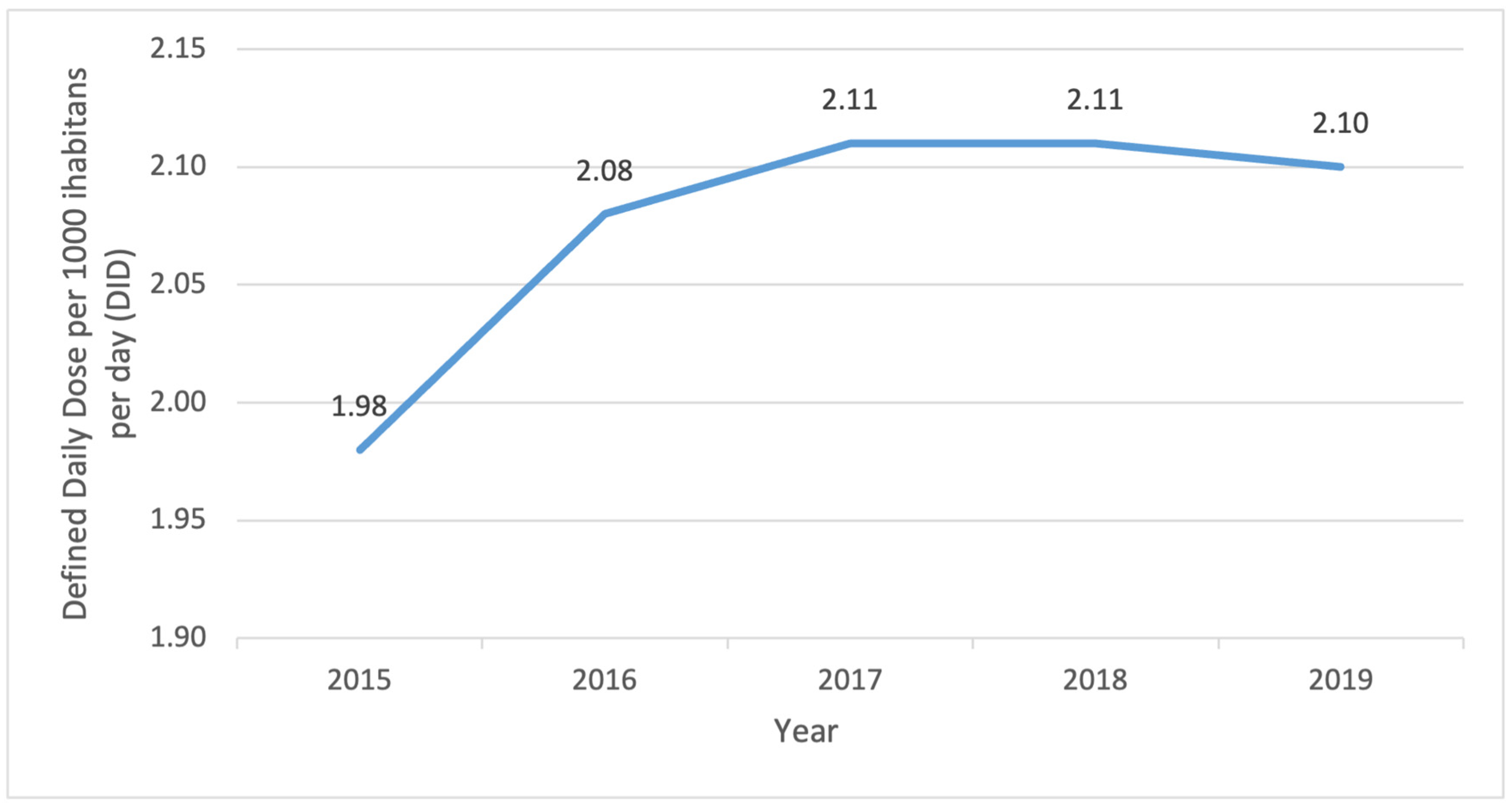
This national study showed an increase in antibiotic consumption in dentistry in an observed period. This is in accordance with a previous study from Croatia [
10]. In Croatia, the increase in antibiotic consumption in dentistry follows the trend of increased consumption of medication in general. During the period 2015 to 2019, there has been a trend of increased medication consumption measured in DID with an average increment of 6.6% a year [
11]. Klein et al. investigated global antibiotic consumption and came to the conclusion that there had been an increase of 65% between the years 2000 and 2015 [
12]. DDD grew from 21.1 billion to 34.8 billion while the rate of antibiotic consumption increased 39% from 11.3 to 15.7 DDD per 1000 inhabitants daily during the observation period. An increase in antibiotic consumption was noted even in the Czech Republic between the years 2006 and 2012 [
13]. Medication prescribed by dentists was increased even in Norway by 30% and Australia by 264% from 2005 to 2016 [
14,
15]. According to data from the European Antimicrobial Resistance Surveillance Network in systemic consumption from 2010 to 2019, total consumption of antibiotics was decreased, even though six countries (Bulgaria, Greece, Iceland, Ireland, Latvia, and Poland) showed a statistically significant increase in antibiotic consumption [
16]. Interestingly, in Croatia from 2015 to 2019, the number of prescribers increased while the population number decreased. On the other hand, different research that compared antibiotic prescription by dentists between England, Scotland, Norway, and Sweden showed a decrease in antibiotic prescribing trend from 2010 to 2016: in Sweden, it was lower by 19%, England by 18%, Scotland by 13% and Norway by 4% [
17]. Additionally, research conducted in Germany and Belgium showed the same trend [
18,
19]. Palmer et al. pointed out a possible explanation for an overprescription of antibiotics in dentistry
—inaccurate dental diagnoses (indications) with an aim to prevent the further spreading of infection, the pressure of time or postponed treatment [
20]. This could be related to a lack of patient cooperation, dentists’ work overload and prescribing an antibiotic “just in case” before the weekend or a vacation [
21,
22]. Yingling et al. investigated these reasons among the members of the American Association of Endodontists [
23]. Part of the members claimed that they prescribed antibiotics for “medical
–legal” reasons, so they would not lose a patient or their recommendation. One of the reasons for antibiotic prescription was pressure from the patient or general dentist who referred them to an endodontist specialist and required antibiotics to be prescribed for every endodontic treatment. Al-Khatib investigated, among Jordanian dentists, how their patients take antibiotics before dental procedures without even consulting them. Results of this study showed that 33.9% of dentists claimed that more than once a week they were pressured by patients to prescribe antibiotics even though there were no indications for it, and 22% of dentists claimed they were under pressure by parents who demanded an antibiotic for their children even though there were no indications for prescribing [
24].
3.2. Indications
In this study, most antibiotics were prescribed for the following diagnoses according to the ICD classification: Periapical abscess without sinus (K04.7), Diseases of pulp and periapical tissues (K04) and Chronic apical periodontitis (K04.5). Periapical abscess without sinus was one of the most often used diagnoses for antibiotic use in Turkey [
25]. Comparable results were seen in Belgium and Kosovo [
26,
27]. This study also revealed that diagnoses such as Acute periodontitis (K05.2) and Chronic periodontitis (K05.3) were used in less than 5% of cases when antibiotics were prescribed. However, studies showed that in Italy and France, pericoronitis was a diagnosis used in more than 50% of the cases in antibiotic prescriptions [
28,
29]. According to the guidelines of the European Society of Endodontology, indications for systemic antibiotic treatment in conjunction with endodontic therapy are indicated in: acute apical abscess in medically compromised patients, acute apical abscess with systemic involvement (localized fluctuant swellings, elevated body temperature > 38 °C, malaise, lymphadenopathy); trismus; progressive infections (rapid onset of severe infection in less than 24 h, cellulitis or a spreading infection, osteomyelitis) where onward referral to oral surgeons may be necessary; replantation of avulsed permanent teeth. In these cases, topical administration of antibiotics may also be indicated. Soft tissue trauma requiring treatment (e.g., sutures, debridement).
Clinical diagnoses where antibiotics are not indicated are: Symptomatic irreversible pulpitis (pain, with no other symptoms and signs of infection); Pulp necrosis; Symptomatic apical periodontitis (pain, pain to percussion and biting and widening of periodontal ligament space); Chronic apical abscess (teeth with sinus tract and periapical radiolucency); Acute apical abscess without systemic involvement (localized fluctuant swellings) [
30]. Considering the indication for correct prescription of antibiotics, their use for diagnoses such as caries (ICD K02), pulpitis (K04), retained dental root (K08.3), pulp necrosis (K04.1), dentofacial anomalies (K07), encounter for dental examination (Z01.2), deposits (accretions) on teeth (K03.6), presence of dental prosthetic device (Z97.2) points towards ignorance of dentists in Croatia on the correct use or prescription of antibiotics. This correlates with another national research, where results showed that antibiotics were prescribed in clinical situations where they were not supposed to like pulpitis in 25.6% of cases and cavity in 9.3% of cases [
9]. Similar results were seen in research in other countries such as D’Ambrosio et al., where antibiotics were used for pulpitis (19.4% of cases) [
28]. Meanwhile, in India, Malaysia, Saudi Arabia and Cambodia, antibiotics were given in 26.7% of the cases for pulpitis [
31]. Different research in the United Kingdom (UK) interestingly pointed out that in 75% of dental cases, antibiotics were prescribed incorrectly [
32]. Another piece of research conducted in Croatia investigated the attitudes of dentists towards antibiotic prescription and the results pointed out that their habits of prescribing are not in line with contemporary guidelines [
33]. Additionally, they showed ignorance when prescribing antibiotics for immunocompromised patients. It is alarming that there was an increase in antibiotic prescriptions for inaccurate diagnoses in Croatia in the observed period. Prescribed antibiotics in the observed period for diagnosis of pulpitis were increased by 4.1%, dental caries by 39.1%, caries of dentine by 13.5%, caries of cementum by 3.2%, other dental caries by 3.0%, retained dental root by 2.9%, dental examination 144.7%. This study revealed antibiotics were prescribed in 29.79% of cases for incorrect indications and in nearly 22% of cases for diagnoses where we cannot determine with certainty whether antibiotics were necessary or not. These indications depend greatly on the clinical situation, or a very broad indication was used instead of a specific clinical diagnosis.
In the period 2015 to 2019, diagnosis of acute apical periodontitis of pulpal origin was in the top five most used diagnoses for the prescription of antibiotics. According to the American Dental Association, antibiotics can be prescribed for this diagnosis only in cases when conservative treatment is not available within 24 h, or if symptoms progression is noted [
6]. Because we do not have data that could confirm if dental care was available within 24 h or not, we cannot verify if antibiotic use in these cases was appropriate. National guidelines and their implementation have an impact on the rational use of antibiotics, research from Sweden has shown [
34]. Since Croatia does not have national guidelines for prescribing antibiotics, that could potentially explain the reasoning for the incorrect use of antibiotics. Certain indications and guidelines for drug prescription published online from the Croatian Health Insurance Fund webpage do not fully correspond with the guidelines presented in the summary of products. Also, there are limitations within the computer software, where appropriate diagnosis could not be found, which could also lead to incorrect use of diagnosis for antibiotic prescription, even though clinical situation requires it. Furthermore, we do not have the data about if and when antibiotics were used for prophylactic purposes.
One of the problems when comparing data from different research is the fact that not all dentists use the same diagnosis classification. More unified classification would make comparison easier.
In this research, the most prescribed antibiotic in the observed period was amoxicillin with clavulanic acid (71%). This correlates with another national piece of research in Croatia [
9,
10,
35]. Following it are amoxicillin, clindamycin, metronidazole, cephalexin, and azithromycin. Their consumption accounted for 96% of the total consumption of all prescribed antibiotics by public health service dentists. The consumption of amoxicillin with clavulanic acid increased by 11.4% during the observed period, metronidazole by 15.5%, and azithromycin by 4.8%, while the consumption of amoxicillin decreased by 6%, clindamycin by 9.9%, cephalexin by 42.7%, and clindamycin by 9.9%. The study in the Czech Republic also showed an increased consumption of clindamycin and amoxicillin with clavulanic acid by 60% from 2006 to 2012 [
13]. Unlike the research in Croatia, where the use of amoxicillin with clavulanic acid is the first choice of antibiotics prescribed, in Belgium, during the period from 2000 to 2016, the most prescribed antibiotic was amoxicillin, followed by amoxicillin with clavulanic acid, clindamycin, clarithromycin, doxycycline, azithromycin, and metronidazole [
19]. Similar results were shown in a study conducted in Australia, where the most frequently prescribed antibiotic was amoxicillin, followed by amoxicillin with clavulanic acid and metronidazole [
15]. These three antibiotics accounted for more than 80% of all antibiotics prescribed by dentists. A study conducted in Germany also showed that amoxicillin is the first choice of antibiotic for treating dentoalveolar infections [
36]. A study conducted in the United States of America has shown that the most prescribed antibiotics were amoxicillin followed by penicillin V and clindamycin for individuals allergic to penicillin [
37]. Research indicated that amoxicillin remains the most used antibiotic in the treatment of odontogenic infections worldwide [
7,
20,
38,
39]. Dominguez et al. stated in their research that dentists with more experience prescribed amoxicillin with clavulanic acid as their first choice in treatment, while those with less experience prescribed only amoxicillin [
40]. According to the guidelines of the European Society of Endodontology, amoxicillin is the first-choice antibiotic for treating infections in non-allergic and non-immunocompromised patients [
30]. Choosing amoxicillin with clavulanic acid as the first choice in treating infections by dentists with more work experience could be associated with a lack of education and adherence to new guidelines. The research conducted in Croatia showed similar results. Dentists with less experience showed better knowledge of the proper use of antibiotics [
41]. A study by Smith et al. indicated that phenoxymethylpenicillin is more commonly prescribed in Norway and Sweden, while broad-spectrum amoxicillin is predominantly prescribed in England and Scotland [
17]. The previous guidelines in England had recommended amoxicillin as the first-choice antibiotic, unlike the recommendations of the Norwegian Institute of Public Health, which recommends the use of phenoxymethylpenicillin as the first-choice antibiotic in acute dentoalveolar processes. In the new guidelines in England, phenoxymethylpenicillin is now listed as the first-choice antibiotic [
42,
43,
44]. In Croatia, the consumption of phenoxymethylpenicillin prescribed by dentists amounted to less than 1%. Metronidazole is useful for treating anaerobes, and recommendations suggest its use in combination with penicillin for the treatment of odontogenic infections [
45]. Considering the use of metronidazole in combination with penicillin, the increase in metronidazole consumption parallels the increase in the consumption of amoxicillin with clavulanic acid. The highest prescription rates for antibiotics occur on Mondays and Fridays. The fact that the highest antibiotic consumption is on Mondays and Fridays could be linked to the availability of dental services. In addition to the mentioned availability of dental services, the reason could also be the pressure from patients to prescribe antibiotics “just in case”, especially if they are planning to travel, and in similar situations. Public dental offices in Croatia operate under specific contractual terms, including a designated number of working Saturdays, and they are closed on Sundays. This aligns with the observed trend of increased antibiotic prescriptions on Fridays and Mondays. The study conducted by Kuehlein et al. in Germany in 2010 also showed an increased prescription of antibiotics on Fridays and Mondays [
46].
This study shows increased consumption rates in both urban and rural areas of the Republic of Croatia in the period 2015 until the end of 2019. In urban areas, the consumption rate was 1.82 DID while in rural areas, it was 0.27 DID, indicating a 6% increase in urban areas and a 5% increase in rural areas during the observed period. The consumption of antibiotics was statistically higher in urban areas than in rural areas (
p < 0.05). The study conducted in Croatia in 2018 on parents’ knowledge regarding the use and resistance of antibiotics in rural and urban areas showed that, despite a higher level of knowledge about antibiotics among parents in urban areas, it did not influence antibiotic consumption levels [
47]. In contrast, a study in the UK has shown higher antibiotic prescriptions in less developed areas, indicating a higher incidence of caries and other dental diseases in those regions [
48]. Considering that untreated caries can lead to abscesses, prompting patients to visit a dentist, this could be a contributing factor to the higher antibiotic prescriptions in those areas [
49]. Manski et al., in their studies, emphasize that factors such as income, education, and health insurance could be correlated with individuals using dental care. However, they acknowledge that these factors alone cannot explain the usage patterns for all individuals [
50]. A study conducted in the United States of America (USA) has shown that adults in rural areas have a 65% lower chance of receiving adequate preventive dental care compared to those in urban areas. Contributing factors to this result may include a shortage of dentists in those areas, educational disparities, and the fact that health is not a priority due to other essential needs, such as food, particularly for individuals with lower socioeconomic status [
51]. One of the reasons that could explain the higher usage of antibiotics in urban areas could be the fact that more people live in urban areas rather than in rural areas.
3.3. Patients
In this research, from 2015 until the end of 2019, more antibiotics were prescribed to female patients. Similar results were noted in previous research by Peric et al. from 2015, wherein in 54 % of cases, antibiotics were prescribed to women and in 46% of cases to men [
35]. Such results are in accordance with research conducted in Norway (2010–2016) and the United States of America [
52,
53]. Similar results were also seen in a study in Sweden where women were prescribed more antibiotics than men in the age group 21–80 years [
34]. On the contrary, Lipsky et al., summarizing contemporary literature on differences in oral health in men and women, stated that men have poorer oral hygiene habits, a higher prevalence of periodontal diseases, and that they more often than women seek dental help for acute problems rather than for preventive reasons [
54]. Speaking of preventive dentistry, Lund et al. concluded that there is less chance for antibiotic prescription if a patient has a dental appointment once a year or more often [
34]. Considering that a study has shown that women have a more positive attitude towards oral health, better behavior related to oral health and visit dentists more frequently, it is not known why more antibiotics are prescribed to women [
54].
In this research, the highest consumption was recorded for the age group 18–65 years. Similar results could be found in another study in Turkey where most of the antibiotics prescribed were for the age group 18–64 years [
55]. However, in the age group 7–17 years, there was a statistically significant decrease in antibiotic consumption, while in the group 65+ years, there was a statistically significant increase. In 2017, a national program was implemented in the Republic of Croatia [
56]. The program consists of obligatory preventative dental exams before children are enrolled in kindergarten, first grade in elementary school (age 7) and sixth grade of elementary school (age 12). This could explain the decrease in antibiotic consumption in the age group 7–17 years because a written confirmation from a dentist is needed to enroll in school which obligates parents to bring their children to regular dental appointments thus giving them the opportunity to avoid clinical situations that would require antibiotic use. An increase in antibiotics in the age group 65+ years could be linked to other comorbidities and dentists’ decision to use antibiotics to prevent complications considering patients’ age, and whether there is an indication for antibiotic use or not.
Since the overuse of antibiotics is in direct connection with antimicrobial resistance, it is important to mention that in some works of research, the highest frequency of resistance was for amoxicillin, clindamycin, and metronidazole [
57]. Even though the resistance patterns were widely variable and have not yet reached critical levels, it is paramount for dentists to follow available guidelines on antibiotic use in certain clinical situations, as well as for patients to be educated on antibiotic use and resistance.

 ,
, 

{kind=link}