




Echinacea Reduces Antibiotics by Preventing Respiratory Infections: A Meta-Analysis (ERA-PRIMA)

 ,
,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results
2.1. Study Characteristics
2.2. Risk of Bias
2.3. Results from Individual Studies
2.4. Results of Meta-Analysis
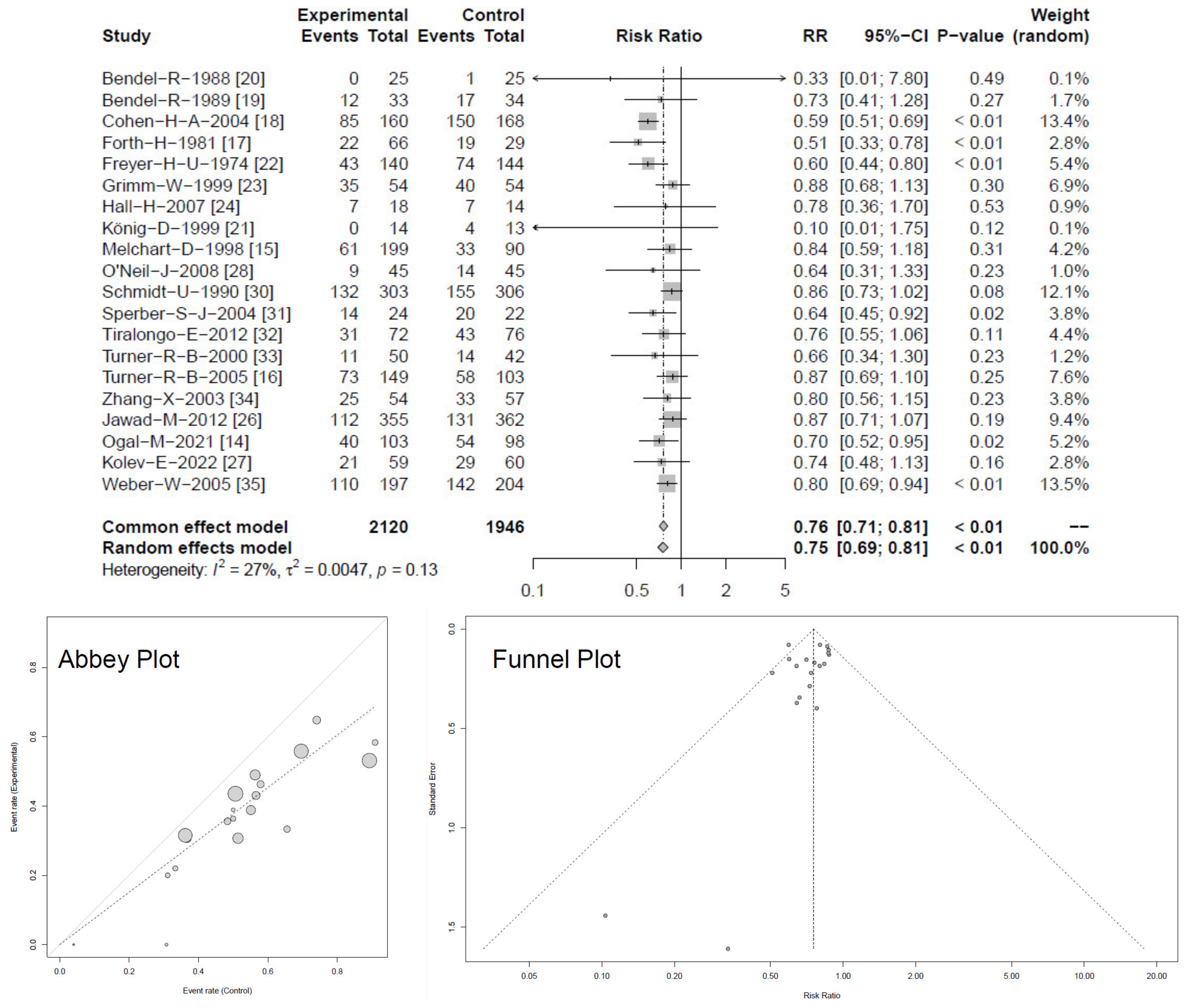
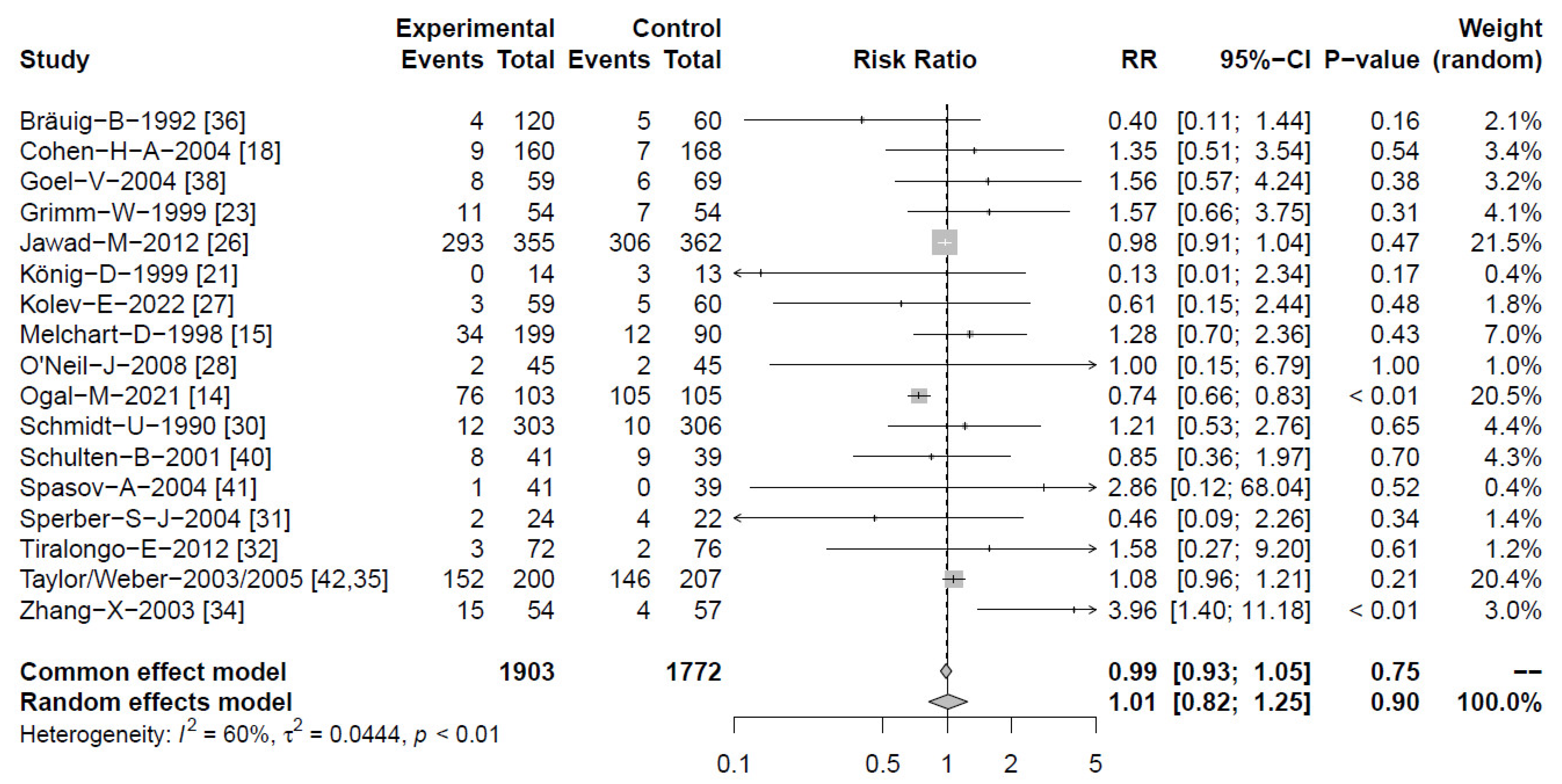
2.4.1. Prevention of Respiratory Tract Infections (RTIs)
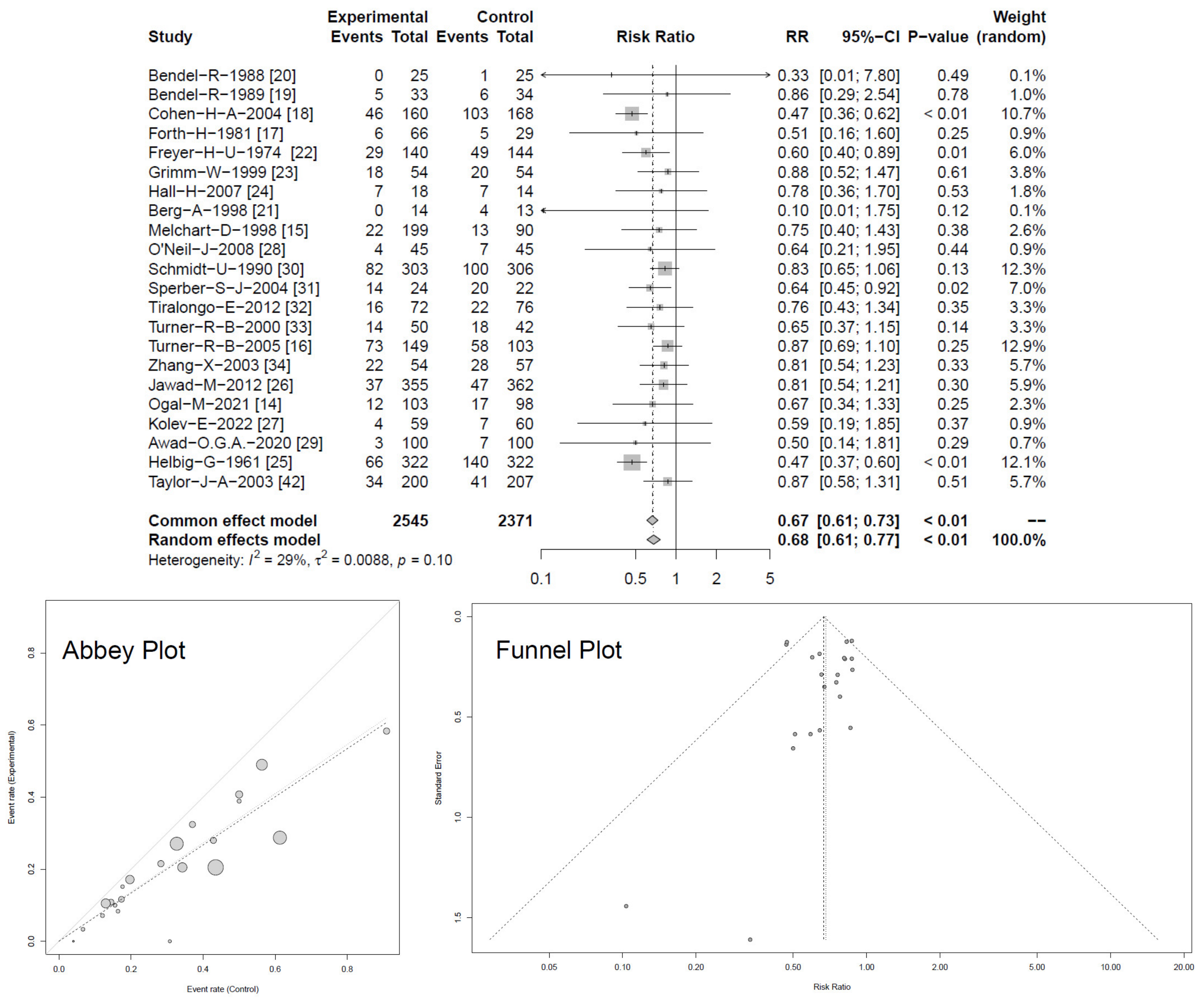
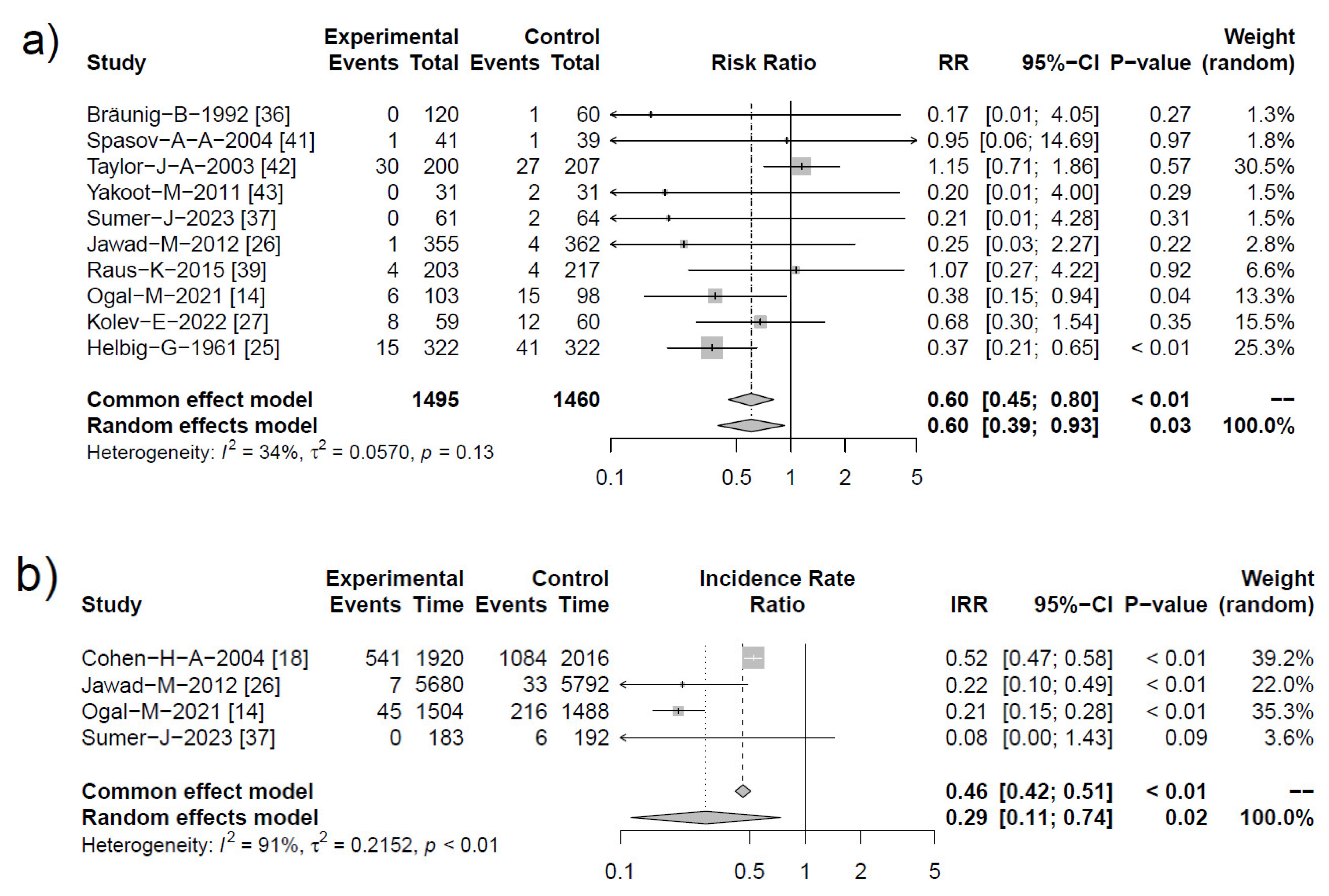
2.4.2. Reduction of RTI Complications
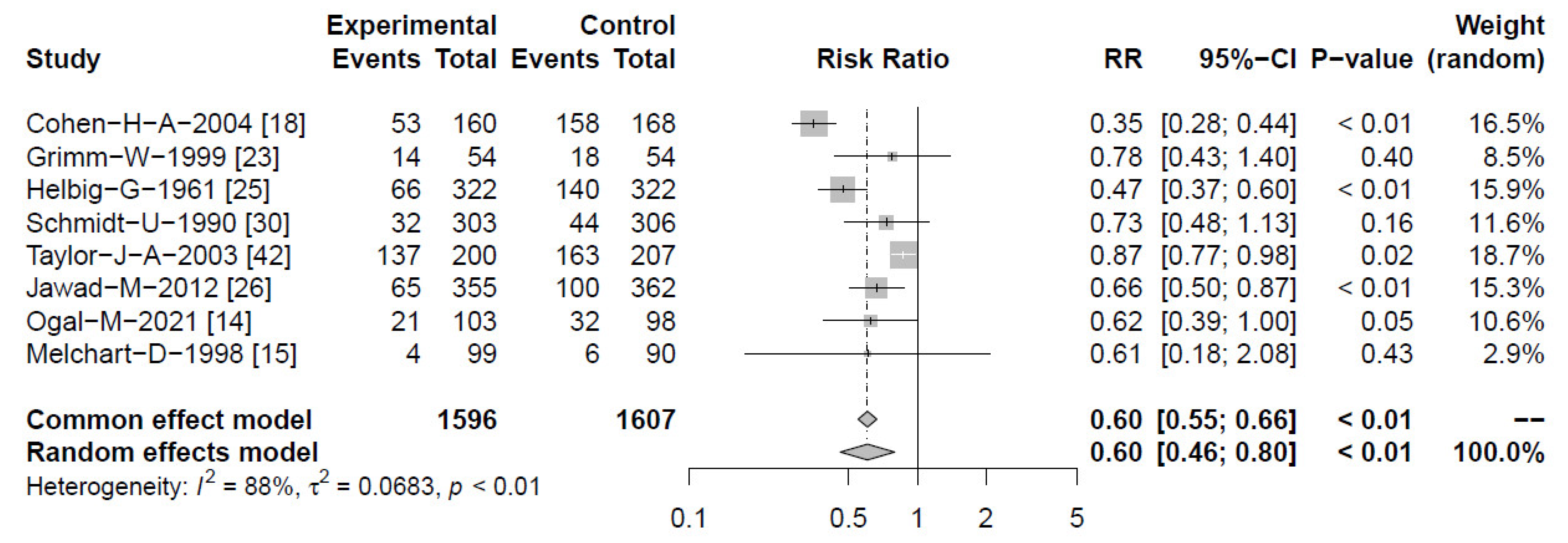
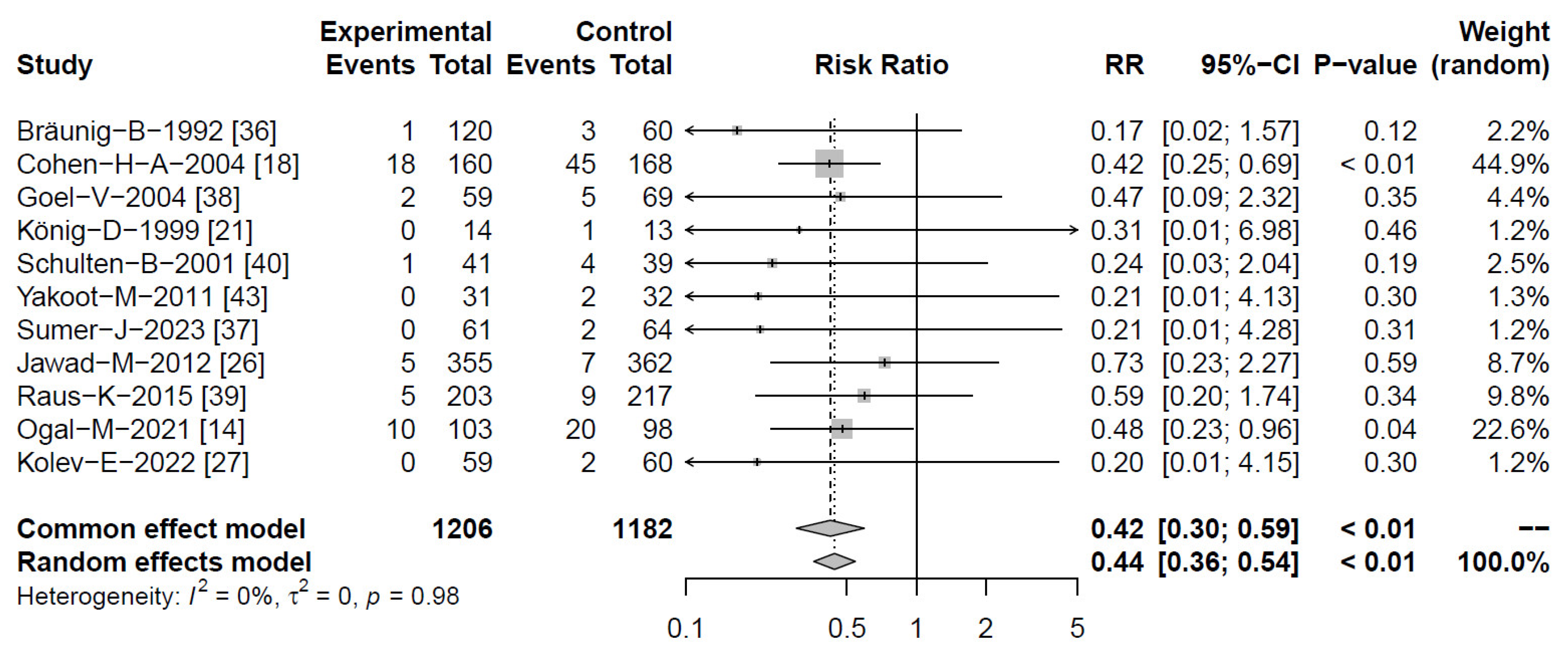
2.4.3. Antibiotic Prescriptions
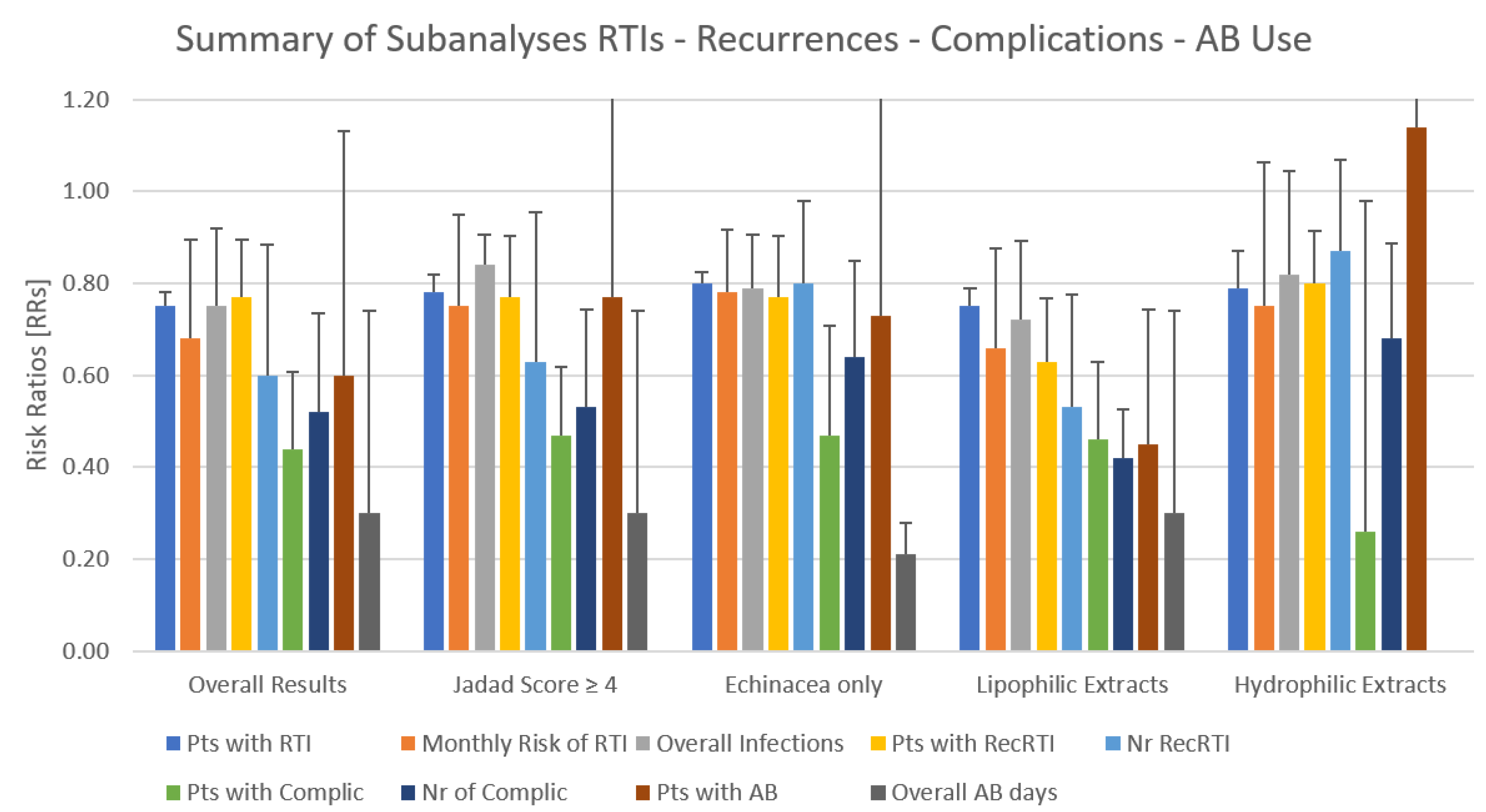
2.4.4. Subanalyses
2.4.5. Adverse Events
3. Discussion
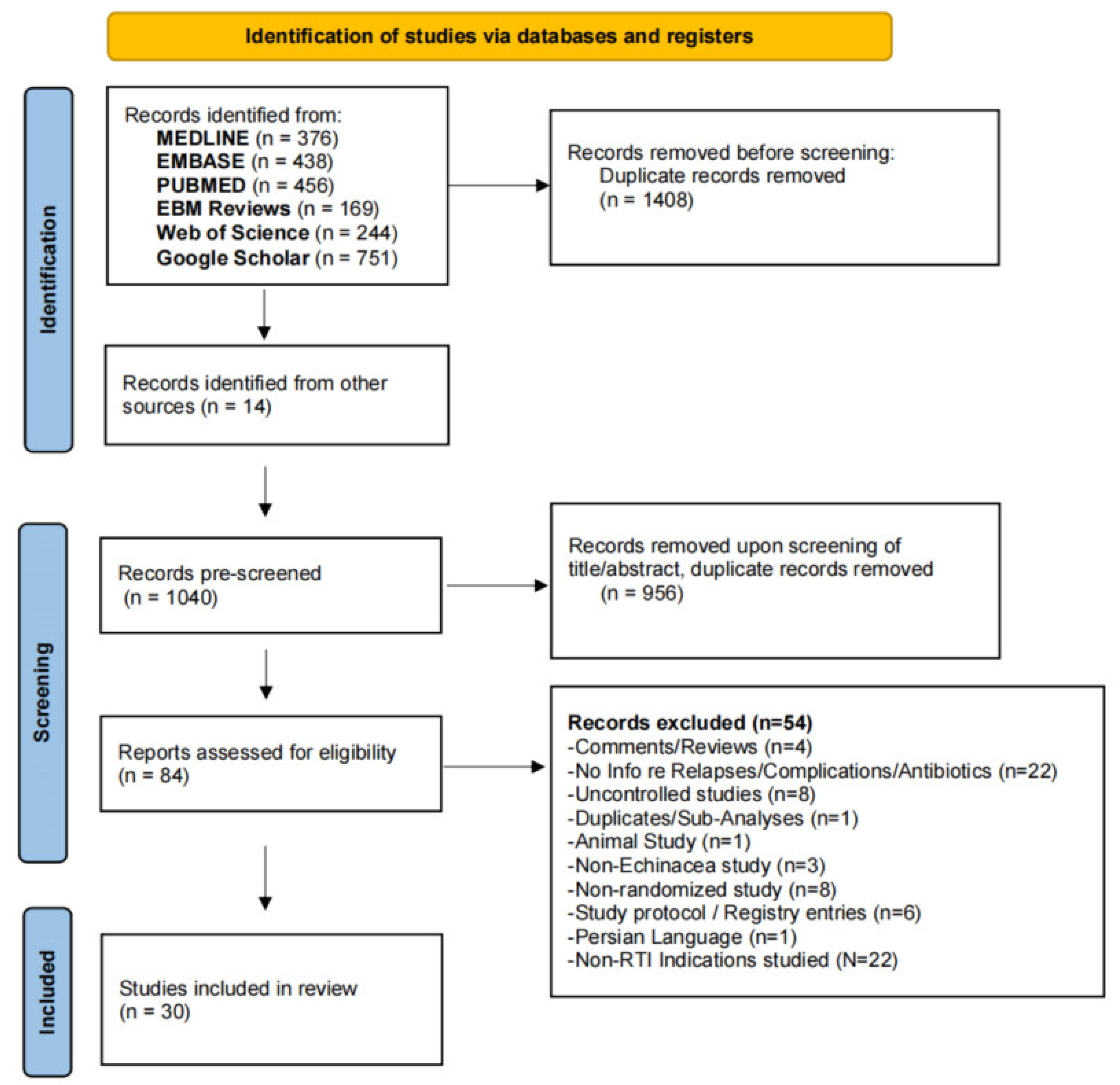
4. Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study/ Registry | Echinacea Species | Control | Extraction Method | Supplement | Duration of Treatment/Observation | Daily Dose/Amount of Echinacea [mg] | Participant Number (N, ITT) | Age [Years] | Cold Definition | Jadad Score [18] |
|---|---|---|---|---|---|---|---|---|---|---|
| Bendel R et al., 1988 [20] | EPAr + EPUr Esberitox | NT | Ethanolic Extract | Thuiae occid, Baptisia | 50 days in addition to Chemotherapy Prevention | 3 × 50 drops | 50 | >18 | Respiratory Infection induced Stop of Chemotherapy medically confirmed | 2 |
| Bendel R et al., 1989 [19] | EPAr + EPUr Esberitox | NT | Ethanolic Extract | Thuiae occid, Baptisia | 12 Chemotherapy Cycles à 14 days Prevention | 3 × 25 drops | 67 | >18 | Respiratory Infection induced Stop of Chemotherapy medically confirmed | 1 |
| Bräuning B et al., 1992 [36] | EPUr | Placebo | Ethanolic Extract | None | Therapy 8–10 days | Dosis 1 = 90 drops/450 mg Dosis 2 = 2 × 90 drops/900 mg | 180 | 18–60 | Flu-like Infections, clinically confirmed (virally vs. bacterial) | 1 |
| Cohen HA et al., 2004 [18] | EPU + EAN | Placebo | Glycerol extract | Propolis + Vitamin C | 3 mts Prevention | 2–4 × 5–7.5 mL 500–1500 mg | 328 | 1–5 | Patient reported- medically confirmed | 4 |
| Forth H, Beuscher N, 1981 [17] | EPAr + EPUr (Esberitox) | Placebo (20 mg Vit C) | Ethanolic extract | Thuiae occid, Baptisia | 3 × 14d cycles for up to 17 weeks Prevention | 3 × 25 drops or 3 × 1 tablet | 95 | >18 | Patient reported Rhinitis | 1 |
| Freyer HU, 1974 [22] | EPAr + EPUr | NT | Ethanolic extract | Thujae occid, Baptisia | 6 weeks Prevention | 3 × 20 drops | 284 | 6–17 | “infections” not further described | 1 |
| Goel V et al., 2004 [38] | EPU | Placebo | Ethanol | None | 7 days Therapy | 1st day: 10 × 4 mL 6 days: 4 × 4 mL | 128 ≥2 colds/y | 18–65 | Patient reported Confirmed by study nurse/physician | 5 |
| Grimm (1999)/Schoeneberger (1996) [23,62] | EPUh | Placebo | Pressed-juice | None | 2 mts Prevention | 2 × 4 mL 6200 mg 2) | 108 ≥3 colds/y | >11 | Patient reported- Confirmed by physician | 5 |
| Hall, H et al., 2007 [24] | EPUh | Placebo | Pressed Juice | none | 28 days Prevention | 4 × 2 capsules/8000 mg | 32 | >17 | Incidence of URTI Patient-reported outcome | 4 |
| Helbig (1961) [25] | EPUr + EANr (Esberitox) | NT | Ethanolic extract | Thujae occid/Baptisia | 1 mt Prevention | 3 × 20 drops | 644 | 1–3 | Infections of Upper Respiratory Tract | 0 |
| Jawad et al., 2012 [26] | EPU h + r (Echinaforce) | Placebo | Ethanolic extract | None | 4 mts Prevention | 3–5 × 0.9 mL 2.7–4.5 mL 2400–4000 mg | 717 | >17 | Patient reported–confirmed by Jackson method Virally confirmed infections | 5 |
| König D, 1999 or Berg A (1998) [21] | EPUh | Placebo/Magnesium | Pressed Juice i.c. placebo and Biomagnesin | None | 28 days Prevention | 3 × 40 drops/8000 mg | 42 (Athletes) | >17 | Incidence of URTI Infection, Training failures | 3 |
| Kolev E et al., 2022 [27] | EPU h + r (Echinaforce) | NT | Ethanolic extract | None | 5 months Prevention | 3–5 × 2 tablets (400 mg)/2400–4000 mg | 119 | 18–75 | Patient reported, physician and virally-confirmed infections | 2 |
| Melchart (1998) 3-arm study [15] | EPUr | Placebo | Ethanolic extract | None | 3 mts Prevention | 2 × 50 drops 1800 mg 3) | 99 (90 placebo) =/>3 colds/y | 18–65 | Patient reported- Confirmed by physician | 4 |
| Melchart (1998) 3-arm study [15] | EANr | Ethanolic extract | None | 3 mts Prevention | 2 × 50 drops 1800 mg 3) | 100 (90 placebo) | 18–65 | Patient reported- Confirmed by physician | ||
| O’Neil J et al., 2008 [28] | EPU | Placebo | Dried Echinacea, not specified | None | 8 weeks Prevention | 3 × 2 capsules/1800 mg | 90 | 18–65 | Patient reported- Study staff confirmed | 4 |
| Ogal M et al., 2021 NCT02971384 [14] | EPU h + r (Echinaforce) | Placebo (VitC) | Ethanolic extract | None | 4 months Prevention | 3–5 × 1 tablet (400 mg)/1200–2000 mg | 203 | 4–12 | Patient reported, physician and virally-confirmed infections | 5 |
| Awad OG, 2020 2015NBA5732814 [29] | EPU root | Azithromycin (AZT) vs. NTC | Powder | None | 6 × 10 days over 6 months Prevention | 3 × 5 mL (250 mg)/1500 mg + AZT I.c. no prevention/ATZ prevention | 300 | 5–16 | Recurrent tonsillitis, reported by parents | 1 |
| Schmidt U et al., 1990 [30] | EAN | Placebo | Ethanolic extract | Eupatorium/Baptisia | 2 month Prevention | 1 × 12 mL/1440 mg 1) | 609 | >17 | Patient reported- Confirmed by physician | 4 |
| Schulten B et al., 2001 [40] | EPUh (Echinacin®) | Placebo | Pressed Juice | None | 10 days Therapy | 2 × 5 mL (7750 mg) | 80 | >17 | Patient reported confirmed by Jackson method (full picture of cold) | 3 |
| Spasov AA et al., 2004 [41] | EPUh | NT (standard therapy) | Pressed Juice | None (i.a. std treatment) | 10 days Therapy | 3 × 10 drops | 80 | 4–11 | Patient reported, Physician confirmed uncomplicated RTIs | 2 |
| Sperber SJ et al., 2004 [31] | EPUh Echinaguard | Placebo | Pressed juice | None | 14d Prevention | 3 × 2.5 mL | 46 | 18–65 | Artificially Rhinovirus Infection, Jackson definition | 3 |
| Sumer J et al., 2023 [37] | EPU (h + r) (Echinaforce) | Ethanolic extract | None | 10 days Therapy | 1–5 tablets (3360 mg) or 2–7 sprays (1120 mg) 3360–16,800 mg | 246 | >17 | Patient reported, physician and virally-confirmed flu-like infections | 4 | |
| Tiralongo E et al., 2012 [32] | EPUr + EANr (MediHerb) | Placebo | Ethanolic extract | None | 5–9 weeks Prevention | Priming dose 2 × 1 tabs followed by exposition dose 2 × 2 tabs sick dose 3 × 2 tabs/3825 mg and 7650 mg | 148 | 18–65 | Natural exposition (air travel) | 5 |
| Turner RB et al., 2005 [16] 4-arm study | EANr | Placebo | 20% Ethanolic extract | None | 7 days Prevention 5 days Therapy | 3 × 1.5 mL (300 mg)/900 mg | 206 | >17 | Artificially Rhinovirus Infection, Jackson definition Patient reported, physician and virally-confirmed flu-like infections | 4 |
| Turner RB et al., 2005 [16] 4-arm study | EANr | Placebo | 60% Ethanolic extract | None | 7 days Prevention 5 days Therapy | 3 × 1.5 mL (300 mg)/900 mg | 203 | >17 | 4 | |
| Turner RB et al., 2005 [16] 4-arm study | EANr | Placebo | CO2 extract | None | 7 days Prevention 5 days Therapy | 3 × 1.5 mL (300 mg)/900 mg | 196 | >17 | 4 | |
| Turner RB et al., 2000 [33] | EPU | Placebo | Powder Almost no alkylamides | None | 19 days (14 days prevention + 5 days therapy) Prevention | 3 × 1 capsule/900 mg | 92 | >17 | Artificial Rhinovirus Infection, | 3 |
| Taylor (2003)/Weber (2005) [35,42] | EPUh (Echinacin®) | Placebo | Pressed juice | None- | 4/1 week Therapy | 2 × 3.75–5 mL 7.5–10 mL 7500–10,000 mg | 407/401 | 2–11 | Study staff confirmed | 5 |
| Yakoot M et al., 2011 [43] | E (Immumax) | Placebo | Extract | Garlic, Nigella sativa, Panax ginseng, Vitamin C, Zinc | 14 days Therapy | 2 × 1 capsule (120 mg)/240 mg | 63 | 38 (Mean) | Patient reported- Confirmed by physician | 5 |
| Zhang X et al., 2003 [34] | EPUr | Placebo | Powdered root | None | 8 weeks Prevention | 2 × 1 capsule (294 mg)/588 mg | 111 | 18–65 | Patient reported- Confirmed by physician | 3 |
| Study | Random Sequence Generation | Allocation Concealment | Blinding Patients/Personel | Blinding Outcome Assess | Incomplete Outcome | Select Reporting | Other Bias | Overall Jadad [0–5] | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Bendel, 1988 [20] | + | + | - | - | + | + | + | 2 | - | =High Risk |
| Bendel, 1989 [19] | ? | + | - | - | + | + | + | 1 | ||
| Bräunig, 1992 [36] | ? | ? | ? | ? | + | - | + | 1 | + | =Low Risk |
| Cohen, 2004 [18] | + | + | + | + | ? | + | + | 4 | ||
| Forth, 1981 [17] | + | - | - | ? | ? | - | ? | 1 | ? | =Unclear |
| Freyer, 1974 [22] | + | - | - | - | + | + | + | 1 | ||
| Goel, 2004 [38] | + | + | + | + | + | + | + | 5 | ||
| Grimm, 1996 [23] | + | ? | + | + | + | + | + | 5 | ||
| Hall, 2007 [24] | + | + | + | + | ? | ? | + | 4 | ||
| Helbig, 1961 [25] | ? | - | - | - | + | + | + | 1 | ||
| Jawad, 2012 [26] | + | + | + | + | ? | ? | + | 5 | ||
| Kolev, 2022 [27] | + | - | - | + | + | + | + | 2 | ||
| Berg, 1998 [21] | ? | + | + | ? | + | + | + | 3 | ||
| Melchart, 1998 [15] | + | + | - | ? | + | + | + | 4 | ||
| Ogal, 2021 [14] | + | + | ? | + | + | + | + | 5 | ||
| O’Neil, 2008 [28] | + | + | + | + | - | + | + | 4 | ||
| Osama 2020 [29] | + | + | - | - | - | + | ? | 1 | ||
| Raus, 2015 [39] | + | + | + | + | + | + | + | 5 | ||
| Schmidt 1990 [30] | ? | + | ? | ? | + | + | + | 4 | ||
| Schulten, 2001 [40] | + | - | + | + | + | ? | + | 3 | ||
| Spasov, 2004 [41] | + | - | - | - | ? | ? | ? | 2 | ||
| Sperber, 2004 [31] | ? | ? | + | + | + | + | + | 3 | ||
| Sumer, 2023 [37] | + | + | ? | ? | + | + | + | 4 | ||
| Taylor03-Weber05 [35,42] | + | + | + | + | + | + | + | 5 | ||
| Tiralongo, 2012 [32] | + | + | + | + | ? | + | + | 5 | ||
| Turner, 2000 [33] | ? | ? | ? | + | + | + | + | 3 | ||
| Turner, 2005 [16] | + | ? | + | + | + | + | + | 4 | ||
| Yakoot, 2011 [43] | + | + | + | + | + | ? | + | 5 | ||
| Zhang, 2003 [34] | + | + | - | - | ? | + | + | 3 |
| RTIs/Pts with RTIs | Recurrent RTIs/Pts with Recurrent RTIs | Complications/Pts with Complications | Pts with AB/AB Treatment Days/Mean Difference [Days] | Adverse Events (Number of Events) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study Registry | Echinacea (N) | Control (N) | Echinacea | Control | Echinacea | Control | Echinacea | Control | Echinacea | Control |
| Bendel R et al., 1988 [20] | 24/12 (33) | 30/17 (34) | - | - | - | - | - | - | Safety of Echinacea during Chemotherapy not assessed | |
| Bendel R et al., 1989 [19] | 0/0 (25) | 1/1 (25) | - | - | - | - | - | - | Safety of Echinacea during Chemotherapy not assessed | |
| Bräunig B et al., 1992 [36] | - | - | - | - | 1/2 (120) | 4/3 (60) | 0/0 | 1/- | 4 | 5 |
| Cohen HA et al., 2004 [18] | 138/85 (160) | 308/150 (168) | 53 | 158 | 54/18 (160) | 136/45 (168) | -/541/3.40 (160) | -/1084/6.50 (168) | 9 | 7 |
| Forth H, Beuscher N, 1981 [17] | 22/22 (66) | 19/19 (29) | None reported | None reported | ||||||
| Freyer HU, 1974 [22] | 43/43 (140) | 74/74 (144) | 0 | 0 | ||||||
| Goel V et al., 2004 [38] | - | - | - | - | 2/2 (59) | 5/5 (69) | - | - | 8 | 6 |
| Grimm (1999)/Schoeneberger (1996) [23,62] | 35/42 (54) | 40/50 (54) | 14/7 (54) | 18/8 (54) | 37 (54) | 54 (54) | - | - | 11 | 7 |
| Hall, H et al., 2007 [24] | 7/7 (18) | 7/7 (14) | - | - | - | - | - | - | Not reported | Not reported |
| Helbig 1961 [25] | 66/- (322) | 140/- (322) | 66 | 140 | - | - | 15 (322) | 41 (322) | 0 | 0 |
| Jawad (2012) [26] | 149/112 (355) | 188/131 (362) | 65/28 (355) | 100/43 (362) | 5/5 (355) | 7/7 (362) | 1/7/0.02 (355) | 4/33/0.09 (362) | 293 | 306 |
| König D, 1999 or Berg A (1998) [21] | 0/0 (14) | 4/4 (13) | - | - | 0/0 (14) | 1/1 (13) | - | - | 0 | 3 |
| Kolev E et al., 2022 [27] | 21/21 (59) | 29/29 (60) | - | - | 0/0 (59) | 2/2 (60) | 8 (59) | 12 (60) | 3 | 5 |
| Melchart (1998) 3-arm study [15] | - | - | 4/4 (EPUr) (99) | 6/6 (90) | - | - | - | - | 13 | 12 |
| Melchart (1998) 3-arm study [15] | - | - | 7/7 (EAN) (100) | - | - | - | - | 21 | ||
| O’Neil J et al., 2008 [28] | 9/9 (45) | 14/14 (45) | - | - | - | - | - | - | (8%) 2 | (7%) 2 |
| Ogal M et al., 2021 NCT02971384 [14] | 61/40 (103) | 86/54 (98) | 21/16 (103) | 32/22 (98) | 11/10 (103) | 30/20 (98) | 6/45/0.44 (103) | 15/216/2.20 (98) | 76 | 105 |
| Awad OG, 2020 2015NBA5732814 [29] | 2/- (100) | 4/- (100) | - | - | 2 (100) | 4 (100) | - | - | Not assessed as in combination with AZT | |
| Raus K et al., 2015 EUDRA-CT 2010-021571-88 [39] | - | - | - | - | 5/5 (203) | 9/9 (217) | 4 (203) | 4 (217) | Not assessed as in comparison with Oseltamivir | |
| Schmidt U et al., 1990 [30] | 164/132 (303) | 199/155 (306) | 32 | 44 | 12 | 10 | ||||
| Schulten B et al., 2001 [40] | - | - | 1/1 (41) | 4/4(39) | 8 | 9 | ||||
| Spasov AA et al., 2004 [41] | - | - | 1 (41) | 1 (39) | 1 | 0 | ||||
| Sperber SJ et al., 2004 [31] | 14/14 (24) | 20/20 (22) | 2 | 4 | ||||||
| Sumer J et al., 2023 [37] | - | - | 0/0 (61) | 2/2 (64) | 0/0/0 (61) | 2/6/0.09 (64) | Comparison of different Echinacea galenic forms, no non-Echinacea reference. | |||
| Tiralongo E et al., 2012 PHM0608HREC [32] | 31/31 (72) | 43//43 (76) | 3 | 2 | ||||||
| Turner RB et al., 2000 [33] | 11/11 (50) | 14/14 (42) | 0 No significant side effect seen | 0 | ||||||
| Turner RB et al., 2005 [16] | 73/73 (149) | 58/58 (103) | 2% (prevention phase) | 2% (prevention phase) | ||||||
| Taylor (2003) [42] Weber (2005) [35] | - - | - - | 137/110 (200) | 163/142 (207) | 30 (200) | 27 (207) | 152 | 146 | ||
| Yakoot M et al., 2011 [43] | - | - | 0/0 (31) | 2/2 (32) | 0 (31) | 2 (31) | No significant difference between groups but no listing of AEs | |||
| Zhang X et al., 2003 [34] | 25/44 (54) | 33/57 (57) | 15 | 4 | ||||||
| Subanalysis | Subjects with RTI | Monthly Risk of RTI | Overall Infections | Subjects with Recurrent RTI | Number of Recurrent RTI | Subjects with Complication | Number of Complications | Subjects with AB | Overall AB Days |
|---|---|---|---|---|---|---|---|---|---|
| Overall Result | 0.75 [0.69–0.81] I2 = 27% | 0.68 [0.61–0.77] I2 = 29% | 0.75 [0.69–0.82] I2 = 55% | 0.77 [0.68–0.88] I2 = 0% | 0.60 [0.46–0.80] I2 = 88% | 0.44 [0.36–0.54] I2 = 0% | 0.52 [0.43–0.64] I2 = 32% | 0.60 [0.39–0.93] I2 = 34% | 0.30 [0.12–0.73] I2 = 91% |
| Jadad Score ≥ 4 | 0.78 [0.71–0.86] I2 = 40% | 0.75 [0.64–0.87] I2 = 32% | 0.84 [0.80–0.88] I2 = 0% | 0.77 [0.68–0.88] I2 = 0% | 0.63 [0.46–0.87] I2 = 88% | 0.47 [0.37–0.58] I2 = 0% | 0.53 [0.41–0.68] I2 = 52% | 0.77 [0.34–1.45] I2 = 34% | 0.30 [0.12–0.73] I2 = 91% |
| Lipophilic Extracts | 0.75 [0.66–0.83] I2 = 47% | 0.66 [0.56–0.78] I2 = 50% | 0.72 [0.64–0.81] I2 = 68% | 0.63 [0.51–0.78] I2 = 0% | 0.53 [0.39–0.73] I2 = 72% | 0.46 [0.36–0.58] I2 = 0% | 0.42 [0.35–0.50] I2 = 0% | 0.45 [0.30–0.66] I2 = 0% | 0.30 [0.12–0.73] I2 = 91% |
| Hydrophilic Extracts | 0.79 [0.67–0.94] I2 = 0% |
0.75 [0.56–1.02] ns, 0% |
0.82 [0.66–1.02] ns, I2 = 15% | 0.80 [0.67–0.96] I2 = 0% |
0.87 [0.66–1.14] Ns, I2 = 0% |
0.26 [0.05–1.26] Ns, I2 = 0% | 0.68 [0.50–0.92] I2 = 0% | 1.14 [0.76–1.73] I2 = 0% | No study providing data |
| Echinacea only | 0.80 [0.75–0.85] I2 = 0% | 0.78 [0.71–0.85] I2 = 0% | 0.79 [0.74–0.85] I2 = 7% | 0.77 [0.68–0.88] I2 = 0% | 0.80 [0.67–0.96] I2 = 16% | 0.47 [0.34–0.65] I2 = 0% | 0.64 [0.54–0.77] I2 = 0% |
0.73 [0.41–1.33] Ns, I2 = 26% | 0.21 [0.15–0.29] I2 = 0% |

Appendix B




References
- Nunes-Silva, C.; Vilares, A.T.; Schweitzer, V.; Castanhinha, S.; Martins, A.; Lopes, M.J.; Ascoli-Bartoli, T.; Canelas, G.; Keir, H.R.; Cunha, F.; et al. Non-COVID-19 respiratory viral infection. Breathe 2022, 18, 210151. [Google Scholar] [CrossRef]
- Jin, X.; Ren, J.; Li, R.; Gao, Y.; Zhang, H.; Li, J.; Zhang, J.; Wang, X.; Wang, G. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. eClinicalMedicine 2021, 37, 100986. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602, Erratum in Lancet 2017, 389, e1. [Google Scholar] [CrossRef]
- WHO. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 1 February 2024).
- Lang, K. What do we know about covid in immunocompromised people? BMJ 2023, 383, 1612. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, J. 2023. Available online: https://coronavirus.jhu.edu/map.html (accessed on 1 February 2024).
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.J.; van der Linden, M.P.G.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370, Erratum in Lancet Digit. Health 2021, 3, e360–e370. [Google Scholar] [CrossRef] [PubMed]
- Nandi, A.; Pecetta, S.; Bloom, D.E. Global antibiotic use during the COVID-19 pandemic: Analysis of pharmaceutical sales data from 71 countries, 2020–2022. eClinicalMedicine 2023, 57, 101848. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Pleschka, S.; Stein, M.; Schoop, R.; Hudson, J.B. Anti-viral properties and mode of action of standardized Echinacea purpurea extract against highly pathogenic avian Influenza virus (H5N1, H7N7) and swine-origin H1N1 (S-OIV). Virol. J. 2009, 6, 197. [Google Scholar] [CrossRef] [PubMed]
- Declerck, K.; Novo, C.P.; Grielens, L.; Van Camp, G.; Suter, A.; Vanden Berghe, W. Echinacea purpurea (L.) Moench treatment of monocytes promotes tonic interferon signaling, increased innate immunity gene expression and DNA repeat hypermethyl-ated silencing of endogenous retroviral sequences. BMC Complement. Med. Ther. 2021, 21, 141. [Google Scholar] [CrossRef]
- Sharma, M.; Schoop, R.; Hudson, J.B. Echinacea as an antiinflammatory agent: The influence of physiologically relevant pa-rameters. Phytother. Res. 2009, 23, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Schapowal, A.; Klein, P.; Johnston, S.L. Echinacea Reduces the Risk of Recurrent Respiratory Tract Infections and Complications: A Meta-Analysis of Randomized Controlled Trials. Adv. Ther. 2015, 32, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Ogal, M.; Johnston, S.L.; Klein, P.; Schoop, R. Echinacea reduces antibiotic usage in children through respiratory tract infection prevention: A randomized, blinded, controlled clinical trial. Eur. J. Med. Res. 2021, 26, 33. [Google Scholar] [CrossRef] [PubMed]
- Melchart, D.; Walter, E.; Linde, K.; Brandmaier, R.; Lersch, C. Echinacea root extracts for the prevention of upper respiratory tract infections. Arch. Fam. Med. 1998, 7, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.B.; Bauer, R.; Woelkart, K.; Hulsey, T.C.; Gangemi, J.D. An evaluation of Echinacea angustifolia in experimental rhinovirus infections. N. Engl. J. Med. 2005, 353, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Forth, H.; Beuscher, N. Beeinflussung der Häufigkeit banaler Erkältungsinfekte durhc Esberitox. Z. Für Allg. 1981, 57, 2272–2275. [Google Scholar]
- Cohen, H.A.; Varsano, I.; Kahan, E.; Sarrell, M.; Uziel, Y. Effectiveness of an herbal preparation containing echinacea, propolis, and vitamin C in preventing respiratory tract infections in children: A randomized. Arch. Pediatr. Adolesc. Med. 2004, 158, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Bendel, R.; Bendel, V.; Renner, K.; Carstens, V.; Stolze, K. Zusatzbehandlung mit Esbertox N bei Patientinnen mit chemostrahlentherapeutischer Behandlung eines fortgeschrittenen Mammakarzinoms. Onkologie 1989, 12 (Suppl. S3), 32–38. [Google Scholar] [PubMed]
- Bendel, R.; Renner, K.; Stolze, K. Zusatzbehandlung mit Esberitox bei Patientinnen mit kurativer adjuvanter Bestrahlung nach Mammakarzinom. Strahlenther. Onkol. 1988, 164, 278–283. [Google Scholar] [PubMed]
- Berg, A.; Northoff, H.; Konig, D.; Weinstock, C.; Grathwohl, D.; Parnham, M.J.; Stuhlfauth, I.; Keul, J. Influence of Echinacin (EC31) treatment on the exercise-induced immune response in athletes. J. Clin. Res. 1998, 1, 367–380. [Google Scholar]
- Freyer, H.U. Häufigkeit banaler Infekte im Kindeslater und Möglichkeiten der Prophylaxe. Forschritte Med. 1974, 92, 165–168. [Google Scholar]
- Grimm, W.; Müller, H.-H. A randomized controlled trial of the effect of fluid extract of Echinacea purpurea on the incidence and severity of colds and respiratory infections. Am. J. Med. 1999, 106, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.; Fahlman, M.; Engels, H. Echinacea Purpurea and Mucosal Immunity. Int. J. Sports Med. 2007, 28, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Helbig, G. Unspezifische Reizkörpertherapie zur Infektionsprophylaxe. Med. Klin. 1961, 56, 1512–1514. [Google Scholar] [PubMed]
- Jawad, M.; Schoop, R.; Suter, A.; Klein, P.; Eccles, R. Safety and efficacy profile of Echinacea purpurea to prevent common cold episodes: A randomized, double-blind, placebo-controlled trial. Evid. Based Complement. Altern. Med. 2012, 2012, 841315. [Google Scholar] [CrossRef] [PubMed]
- Kolev, E.; Mircheva, L.; Edwards, M.R.; Johnston, S.L.; Kalinov, K.; Stange, R.; Gancitano, G.; Berghe, W.V.; Kreft, S. Echinacea Purpurea For the Long-Term Prevention of Viral Respiratory Tract Infections during COVID-19 Pandemic: A Randomized, Open, Controlled, Exploratory Clinical Study. Front. Pharmacol. 2022, 13, 856410. [Google Scholar] [CrossRef] [PubMed]
- O’neil, J.; Hughes, S.; Lourie, A.; Zweifler, J. Effects of echinacea on the frequency of upper respiratory tract symptoms: A randomized, double-blind, placebo controlled trial. Ann. Allergy Asthma Immunol. 2008, 100, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Awad, O.G.A.-N. Echinacea can help with Azithromycin in prevention of recurrent tonsillitis in children. Am. J. Otolaryngol. 2020, 41, 102344. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Albrecht, M.; Schenk, N. Pflanzliches Immunstimulans senkt Häufigkeit grippaler Infekt. Nat. Und Gan-Zheitsmedizin 1990, 3, 277–281. [Google Scholar]
- Sperber Steven, J.; Shah Leena, P.; Gilbert Richard, D.; Ritchey Thomas, W.; Monto, A.S. Echinacea purpurea for prevention of ex-perimental rhinovirus colds. Clin. Infect. Dis. 2004, 38, 1367–1371. [Google Scholar] [CrossRef]
- Tiralongo, E.; Lea, R.A.; Wee, S.S.; Hanna, M.M.; Griffiths, L.R. Randomised, double blind, placebo-controlled trial of Echinacea sup-plementation in air travellers. Evid Based Complement Altern. Med. 2012, 2012, 417267. [Google Scholar] [CrossRef] [PubMed]
- Turner Ronald, B.; Riker Donald, K.; Gangemi, J.D. Ineffectiveness of echinacea for prevention of experimental rhinovirus colds. Antimicrob. Agents Chemother. 2000, 44, 1708–1709. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lowe, D.; Badesha, G.; Ishaq, S.; Rai, H.; Williams, P. A Double-Blinded Placebo Controlled Trial Evaluating the Effectiveness of Echinacea in Countering Upper Respiratory Tract Infections. 2003. Unpublished Report. [Google Scholar]
- Weber, W.; Taylor, J.A.; Stoep, A.V.; Weiss, N.S.; Standish, L.J.; Calabrese, C. Echinacea purpureafor prevention of upper respiratory tract infections in children. J. Altern. Complement. Med. 2005, 11, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Bräuning, B.; Dorn, M.; Knick, E. Echinacea purpurea radix zur Stärkung der körpereigenen Abwehr bei grippalen Infekten. Z. Für Phytother. 1992, 13, 7–13. [Google Scholar]
- Sumer, J.; Keckeis, K.; Scanferla, G.; Frischknecht, M.; Notter, J.; Steffen, A.; Kohler, P.; Schmid, P.; Roth, B.; Wissel, K.; et al. Novel Echinacea formulations for the treatment of acute respiratory tract infections in adults—A randomized blinded controlled trial. Front. Med. 2023, 10, 948787. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.; Lovlin, R.; Barton, R.; Lyon, M.R.; Bauer, R.; Lee, T.D.G.; Basu, T.K. Efficacy of a standardized echinacea preparation (EchinilinTM) for the treatment of the common cold: A randomized, double-blind, placebo-controlled trial. J. Clin. Pharm. Ther. 2004, 29, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Rauš, K.; Pleschka, S.; Klein, P.; Schoop, R.; Fisher, P. Effect of an Echinacea-Based Hot Drink Versus Oseltamivir in Influenza Treatment: A Randomized, Double-Blind, Double-Dummy, Multicenter, Noninferiority Clinical Trial. Curr. Ther. Res. 2015, 77, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Schulten, B.; Bulitta, M.; Ballering-Brühl, B.; Köster, U.; Schäfer, M. Efficacy of echinacea purpurea in patients with a common cold. A placebo-controlled, randomised, doubleblind clinical trial. Arzneimittelforschung 2001, 51, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Spasov, A.A.; Ostrovskij, O.V.; Chernikov, M.V.; Wikman, G. Comparative controlled study of Andrographis paniculate fixed com-bination, Kan Jang and an Echinacea preparation as adjuvant, in the treatment of uncomplicated respiratory disease in children. Phytother. Res. 2004, 18, 47–53. [Google Scholar] [CrossRef]
- Taylor, J.A.; Weber, W.; Standish, L.; Quinn, H.; Jama, J.G. Efficacy and safety of Echinacea in treating upper respiratory tract infec-tions in children: A randomized controlled trial. JAMA 2003, 290, 2824–2830. [Google Scholar] [CrossRef] [PubMed]
- Yakoot, M.; Salem, A. Efficacy and safety of a multiherbal formula with vitamin C and zinc (Immumax) in the management of the common cold. Int. J. Gen. Med. 2011, 4, 45–51. [Google Scholar] [CrossRef] [PubMed]
- David, S.; Cunningham, R. Echinacea for the prevention and treatment of upper respiratory tract infections: A systematic review and meta-analysis. Complement. Ther. Med. 2019, 44, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Hróbjartsson, A.; Boutron, I.; Turner, L.; Altman, D.G.; Moher, D.; Cochrane Bias Methods Group. Assessing risk of bias in ran-domised clinical trials included in Cochrane Reviews: The why is easy, the how is a challenge. Cochrane Database Syst. Rev. 2013, 4, ED000058. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials:is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- A Wahl, R.; Aldous, M.B.; A Worden, K.; Grant, K.L. Echinacea purpurea and osteopathic manipulative treatment in children with recurrent otitis media: A randomized controlled trial. BMC Complement. Altern. Med. 2008, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Rahmati, M.B.; Safdarian, F.; Hamedi, Y.; Khadem, A.A.; Rezai, M.S. Efficacy and Safety of Echinacea Root Extracts in the Treatment of Pediatric Common Cold: A Randomized Clinical Trial. J. Maz. Univ. Med. Sci. 2012, 22, 12–18. [Google Scholar]
- Cars, T.; Eriksson, I.; Granath, A.; Wettermark, B.; Hellman, J.; Norman, C.; Ternhag, A. Antibiotic use and bacterial complications following upper respiratory tract infections: A population-based study. BMJ Open 2017, 7, e016221. [Google Scholar] [CrossRef] [PubMed]
- Nasrin, D.; Collignon, P.J.; Roberts, L.; Wilson, E.J.; Pilotto, L.S.; Douglas, R.M. Effect of beta lactam antibiotic use in children on pneumococcal resistance to penicillin: Prospective cohort study. BMJ 2002, 324, 28. [Google Scholar] [CrossRef] [PubMed]
- Lebanova, H.V.; Stoev, S.N.; Veleva, N.R.; Belcheva, S.P.; Madzharov, V.G.; Gueorguiev, S.R. Prevalence of Self-Medication with Antibiotics in Europe: A Scoping Review. J. Biomed. Clin. Res. 2023, 16, 5–16. [Google Scholar] [CrossRef]
- Karsch-Völk, M.; Barrett, B.; Kiefer, D.; Bauer, R.; Ardjomand-Woelkart, K.; Linde, K. Echinacea for preventing and treating the common cold. Emergencias 2014, 2014, CD000530. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Sander, S.; White, C.M.; Rinaldi, M.; Coleman, C. Evaluation of echinacea for the prevention and treatment of the common cold: A meta-analysis. Lancet Infect. Dis. 2007, 7, 473–480. [Google Scholar] [CrossRef] [PubMed]
- van Heuvel, L.; Paget, J.; Dückers, M.; Caini, S. The impact of influenza and pneumococcal vaccination on antibiotic use: An updated systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2023, 12, 70. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Rader, T.; Shokraneh, F.; Thomas, J.; et al. Technical Supplement to Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.1; Updated September 2020; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M.S., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2020; Available online: www.training.cochrane.org/handbook (accessed on 1 February 2024).
- Tjosvold, L. Randomized Controlled Trials/Controlled Clinical Trials: A Cut and Paste Search Strategy adapted from the Cochrane ENT Group for Web of Science. Adapted from “RCT Filters used by Cochrane ENT. Oxford (UK): Cochrane ENT Group; 2018.” John W. Scott Health Sciences Library, University of Alberta. Rev. 14 January 2021. Available online: https://docs.google.com/document/d/1aEVsIaeXVZY8_BND-sUB_19sTTMccgoxNUdznH54ilQ/edit (accessed on 1 February 2024).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Vonau, B.; Chard, S.; Mandalia, S.; Wilkinson, D.; Barton, S.E. Does the extract of the plant Echinacea purpurea influence the clinical course of recurrent genital herpes? Int. J. STD AIDS 2001, 12, 154–158. [Google Scholar] [CrossRef] [PubMed]
- PRISMA-P Group; Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Schoeneberger, C. The influence of the immuno stimulating effects of pressed juice from Echinacea purpurea on the course and severity of cold infections. Forum Immunol. 1992, 8, 18–22. [Google Scholar]







| Step | Search |
|---|---|
| 1 | Echinacea.mp. or exp Echinacea/ |
| 2 | coneflower.mp. |
| 3 | Black Sampson.mp. |
| 4 | 1 or 2 or 3 |
| 5 | (randomized controlled trial or controlled clinical trial).pt. or randomized.ab. or randomized.ab. or placebo.ab. or drug therapy.fs. or randomly.ab. or trial.ab. or groups.ab.) not (exp animals/ not humans.sh.) |
| 6 | 4 and 5 |
| 7 | Remove duplicates from 6 |
| 8 | limit to controlled, randomized human RTI studies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gancitano, G.; Mucci, N.; Stange, R.; Ogal, M.; Vimalanathan, S.; Sreya, M.; Booker, A.; Hadj-Cherif, B.; Albrich, W.C.; Woelkart-Ardjomand, K.; et al. Echinacea Reduces Antibiotics by Preventing Respiratory Infections: A Meta-Analysis (ERA-PRIMA). Antibiotics 2024, 13, 364. https://doi.org/10.3390/antibiotics13040364
Gancitano G, Mucci N, Stange R, Ogal M, Vimalanathan S, Sreya M, Booker A, Hadj-Cherif B, Albrich WC, Woelkart-Ardjomand K, et al. Echinacea Reduces Antibiotics by Preventing Respiratory Infections: A Meta-Analysis (ERA-PRIMA). Antibiotics. 2024; 13(4):364. https://doi.org/10.3390/antibiotics13040364
Chicago/Turabian StyleGancitano, Giuseppe, Nicola Mucci, Rainer Stange, Mercedes Ogal, Selvarani Vimalanathan, Mahfuza Sreya, Anthony Booker, Bushra Hadj-Cherif, Werner C. Albrich, Karin Woelkart-Ardjomand, and et al. 2024. "Echinacea Reduces Antibiotics by Preventing Respiratory Infections: A Meta-Analysis (ERA-PRIMA)" Antibiotics 13, no. 4: 364. https://doi.org/10.3390/antibiotics13040364
APA StyleGancitano, G., Mucci, N., Stange, R., Ogal, M., Vimalanathan, S., Sreya, M., Booker, A., Hadj-Cherif, B., Albrich, W. C., Woelkart-Ardjomand, K., Kreft, S., Vanden Berghe, W., Hoexter, G., Schapowal, A., & Johnston, S. L. (2024). Echinacea Reduces Antibiotics by Preventing Respiratory Infections: A Meta-Analysis (ERA-PRIMA). Antibiotics, 13(4), 364. https://doi.org/10.3390/antibiotics13040364