Knowledge, Perceptions and Practices of Community Pharmacists Towards Antimicrobial Stewardship: A Systematic Scoping Review



Abstract
:1. Introduction
2. Methods
2.1. Research Objectives
- To identify the breadth and scope of existing AMS surveys targeting CPs.
- To assess the quality of and gaps in AMS survey tools measuring knowledge, perceptions and practices of CPs regarding AMS.
- To identify and analyse the types and range of outcomes reported in AMS surveys.
- To identify the evidence gaps and recommend future directions of research in relation to improving AMS in community pharmacy.
2.2. Reviewing Data Sources and Search Strategies
2.3. Study Selection
2.3.1. Inclusion Criteria
- 1
- A national or cross-sectional survey that explored AMS at community pharmacy context.
- 2
- Survey participants were limited to CPs of any age and level of experiences.
- 3
- Surveys that employed a single or multiple outcome measure related to CPs’ knowledge, perceptions, practices, barriers and facilitators concerning AMS.
- 4
- Full text articles are available.
2.3.2. Exclusion Criteria
- 1
- Qualitative interviews, editorials, reports, case studies and case series;
- 2
- Any survey that did not include AMS as a topic;
- 3
- Study conducted in other than primary care;
- 4
- Articles not written in English language.
2.4. Data Extraction
2.5. Assessing the Quality of Included Survey Studies
2.6. Collating, Summarising and Analysing Outcome Measures
3. Results
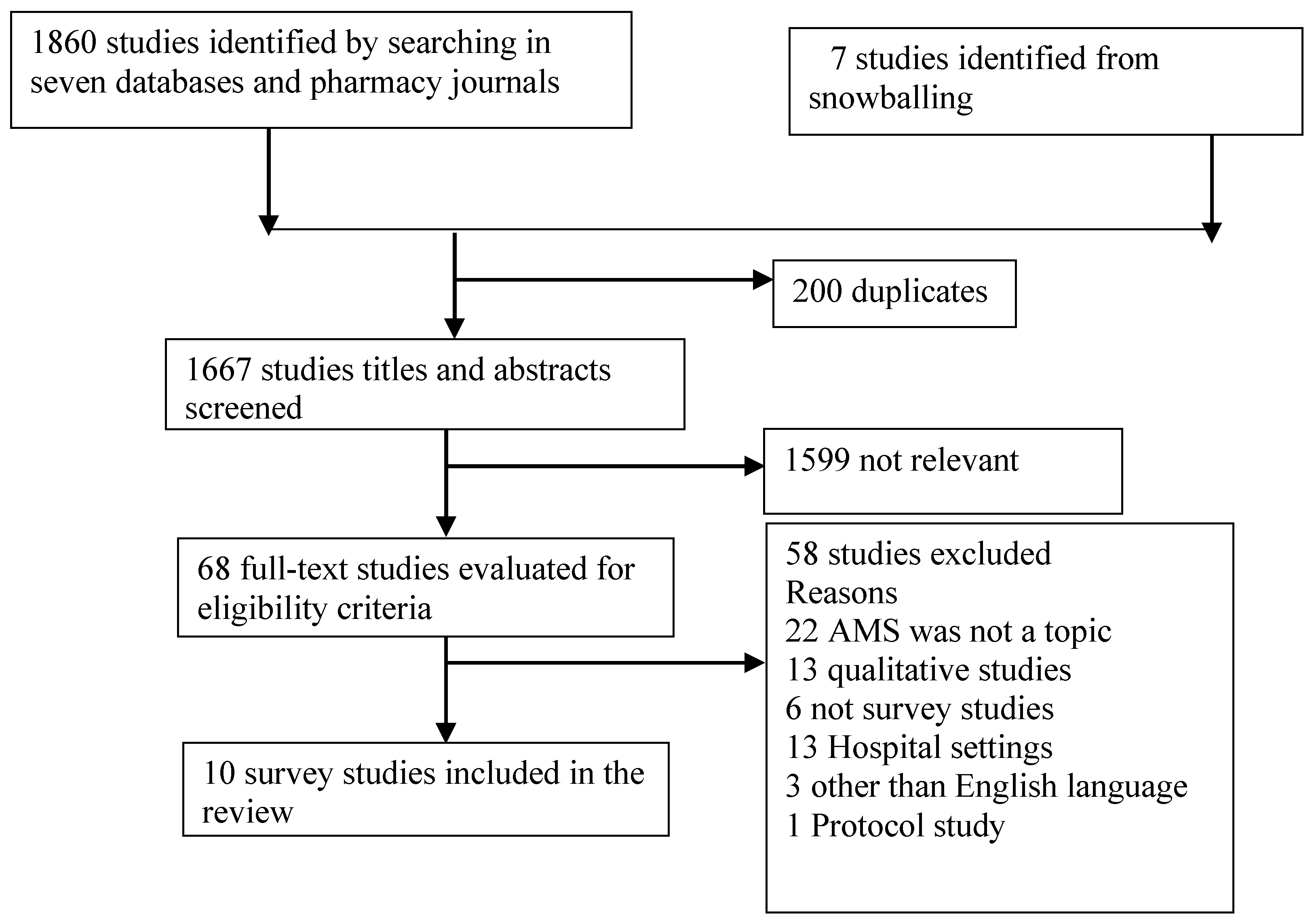
3.1. Breadth of Survey Studies
3.2. Study Demographics and Description of Survey Tools
3.3. Quality Assessment
3.4. Reported Survey Outcomes
3.4.1. Knowledge about AMS
3.4.2. Perceptions of AMS
3.4.3. AMS Practices
Communication with the Prescribers
Patient Education
AMS Compliant Dispensing Process
Participation in AMS Campaign
3.4.4. Barriers and Facilitators to Implementing AMS
Barriers to Undertaking AMS
Facilitators of Conducting AMS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Antibiotic Resistance. Available online: http://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 10 February 2019).
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Anthierens, S.; Tonkin-Crine, S.; Cals, J.W.; Coenen, S.; Yardley, L.; Brookes-Howell, L.; Fernandez-Vandellos, P.; Krawczyk, J.; Godycki-Cwirko, M.; Llor, C.; et al. Clinicians’ views and experiences of interventions to enhance the quality of antibiotic prescribing for acute respiratory tract infections. J. Gen. Intern. Med. 2015, 30, 408–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, G.V.; Fleming-Dutra, K.E.; Roberts, R.M.; Lauri, A.; Hicks, D.O. Core elements of outpatient antibiotic stewardship. MMWR Recomm. Rep. 2016, 65, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Rodis, J.L.; Green, C.G.; Cook, S.C.; Pedersen, C.A. Effects of a pharmacist-initiated educational intervention on patient knowledge about the appropriate use of antibiotics. Am. J. Health Syst. Pharm. 2004, 61, 1385–1389. [Google Scholar] [CrossRef]
- Booth, J.L.; Mullen, A.B.; Thomson, D.A.; Johnstone, C.; Galbraith, S.J.; Bryson, S.M.; McGovern, E.M. Antibiotic treatment of urinary tract infection by community pharmacists: A cross-sectional study. Br. J. Gen. Pract. 2013, 63, e244–e249. [Google Scholar] [CrossRef]
- Klepser, M.E.; Adams, A.J.; Klepser, D.G. Antimicrobial stewardship in outpatient settings: Leveraging innovative physician-pharmacist collaborations to reduce antibiotic resistance. Health Secur. 2015, 13, 166–173. [Google Scholar] [CrossRef]
- World Health Organization. The Role of Pharmacist in Encouraging Prudent Use of Antibiotics and Averting Antimicrobial Resistance: A Review of Policy and Experience in Europe. WHO Regional Office for Europe Publications: Geneva, Switzerland, 2014. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance/publications/2014/the-role-of-pharmacist-in-encouraging-prudent-use-of-antibiotic-medicines-and-averting-antimicrobial-resistance-a-review-of-current-policies-and-experiences-in-europe-2014 (accessed on 10 January 2019).
- The Global Respiratory Infection Partnership Declaration. Available online: https://www.grip-initiative.org/media/1295/grip_meeting_report_2014_web.pdf (accessed on 5 September 2019).
- Buckland, L.; Merrett, G.; Bloom, G.; Wilkinson, A.; MacGregor, H. Towards the just and sustainable use of antibiotics. J. Pharm. Policy Pract. 2016, 9, 31. [Google Scholar]
- Jones, L.F.; Owens, R.; Sallis, A.; Ashiru-Oredope, D.; Thornley, T.; Francis, N.A.; Butler, C.; McNulty, C.A. Qualitative study using interviews and focus groups to explore the current and potential for antimicrobial stewardship in community pharmacy informed by the Theoretical Domains Framework. BMJ Open 2018, 8, e025101. [Google Scholar] [CrossRef] [Green Version]
- Keijsers, C.J.; Leendertse, A.J.; Faber, A.; Brouwers, J.R.; de Wildt, D.J.; Jansen, P.A. Pharmacists’ and general practitioners’ pharmacology knowledge and pharmacotherapy skills. J. Clin. Pharmacol. 2015, 55, 936–943. [Google Scholar] [CrossRef]
- Essack, S.; Bell, J.; Shephard, A. Community pharmacists—Leaders for antibiotic stewardship in respiratory tract infection. J. Clin. Pharm. Ther. 2018, 43, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Res, R.; Hoti, K.; Charrois, T.L. Pharmacists’ perceptions regarding optimization of antibiotic prescribing in the community. J. Pharm. Pract. 2017, 30, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Coleman, C.L. Examining influences of pharmacists’ communication with consumers about antibiotics. Health Commun. 2003, 15, 79–99. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Hawes, L.; Mazza, D. Effectiveness of interventions involving pharmacists on antibiotic prescribing by general practitioners: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2019, 74, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Dobson, E.L.; Klepser, M.E.; Pogue, J.M.; Labreche, M.J.; Adams, A.J.; Gauthier, T.P.; Turner, R.B.; Su, C.P.; Jacobs, D.M.; Suda, K.J.; et al. Outpatient antibiotic stewardship: Interventions and opportunities. J. Am. Pharm. Assoc. 2017, 57, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Kallen, M.C.; Ten Oever, J.; Prins, J.M.; Kullberg, B.J.; Schouten, J.A.; Hulscher, M.E.J.L. A survey on antimicrobial stewardship prerequisites, objectives and improvement strategies: Systematic development and nationwide assessment in Dutch acute care hospitals. J. Antimicrob. Chemother. 2018, 73, 3496–3504. [Google Scholar] [CrossRef]
- Weier, N.; Tebano, G.; Thilly, N.; Demoré, B.; Pulcini, C.; Zaidi, S.T.R. Pharmacist participation in antimicrobial stewardship in Australian and French hospitals: A cross-sectional nationwide survey. J. Antimicrob. Chemother. 2017, 73, 804–813. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, R.; Hall, B.J.; Doyle, J.; Waters, E. ‘Scoping the scope’ of a cochrane review. Int. J. Public Health 2011, 33, 147–150. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellerman, S.E.; Herold, J. Physician response to surveys: A review of the literature. Am. J. Prev. Med. 2001, 20, 61–67. [Google Scholar] [CrossRef]
- Draugalis, J.R.; Coons, S.J.; Plaza, C.M. Best practices for survey research reports: A synopsis for authors and reviewers. Am. J. Pharm. Educ. 2008, 72, 11. [Google Scholar] [CrossRef] [PubMed]
- Mays, N.; Roberts, E.; Popay, J. Synthesising research evidence. In Studying the Organisation and Delivery of Health Services: Research Methods; Fulop, N., Allen, P., Clarke, A., Black, N., Eds.; Routlege, Tailor and Francis Group: London, UK; New York, NY, USA, 2001; Volume 220. [Google Scholar]
- Elder, J.P.; Lytle, L.; Sallis, J.F.; Young, D.R.; Steckler, A.; Simons-Morton, D.; Stone, E.; Jobe, J.B.; Stevens, J.; Lohman, T.; et al. A description of the social–ecological framework used in the trial of activity for adolescent girls (TAAG). Health Educ. Res. 2006, 22, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, T.; Thompson, A.; Williams, M.; Zaidi, S.T.R. Perceptions and current practices of community pharmacists regarding antimicrobial stewardship in Tasmania. Int. J. Clin. Pharm. 2018, 40, 1380–1387. [Google Scholar] [CrossRef] [Green Version]
- Avent, M.L.; Fejzic, J.; van Driel, M.L. An underutilised resource for Antimicrobial Stewardship: A ‘snapshot’ of the community pharmacists’ role in delayed or ‘wait and see’ antibiotic prescribing. Int. J. Pharm. Pract. 2018, 26, 373–375. [Google Scholar] [CrossRef]
- Hancock, L.J.; Mellor, C. An evaluation of antimicrobial stewardship in community pharmacy. Fields J. Hudders. Stud. Res. 2016, 2, e23. [Google Scholar] [CrossRef]
- Wilcock, M.; Lee, F. Community Pharmacists and Antimicrobial Stewardship—What is Their Role? J. Med. Optim. 2017, 3, 47–50. Available online: https://www.pharman.co.uk/uploads/imagelib/pdfs/Journal_articles_by_issue/JoMO%20Sep%202017/Community%20Pharmacists.pdf (accessed on 18 September 2019).
- Erku, D.A. Antimicrobial stewardship: A cross-sectional survey assessing the perceptions and practices of community pharmacists in Ethiopia. Interdiscip. Perspect. Infect. Dis. 2016, 2016, 5686752. [Google Scholar] [CrossRef]
- Rehman, I.; Asad, M.; Bukhsh, A.; Ali, Z.; Ata, H.; Dujaili, J.; Blebil, A.; Khan, T. Knowledge and practice of pharmacists toward antimicrobial stewardship in Pakistan. Pharmacy 2018, 6, 116. [Google Scholar] [CrossRef] [Green Version]
- Pawluk, S.; Black, E.; El-Awaisi, A. Strategies for improving antibiotic use in Q atar: A survey of pharmacists’ perceptions and experiences. Int. J. Pharm. Pract. 2015, 23, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.R.; Saqib, A.; Iftikhar, S.; Sadiq, T. Knowledge of community pharmacists about antibiotics, and their perceptions and practices regarding antimicrobial stewardship: A cross-sectional study in Punjab, Pakistan. Infect. Drug Resist. 2018, 11, 133–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.U.; Hassali, M.A.A.; Ahmad, A.; Elkalmi, R.M.; Zaidi, S.T.R.; Dhingra, S. Perceptions and practices of community pharmacists towards antimicrobial stewardship in the State of Selangor, Malaysia. PLoS ONE 2016, 11, e0149623. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Phillips, C.; Vanstone, J.R. Knowledge and Attitudes of Community Health Care Professionals Towards an Antimicrobial Stewardship Program: Post-Survey Report. 2017. Regina Qu’Appelle Health Region. Saskatchewan. Available online: http://www.rqhealth.ca/service-lines/master/files/9003768_8_Community%20HCW%20Knowledge%20and%20Attitudes%20Towards%20ASP%20Survey%20-%20Final%20Report.pdf (accessed on 12 October 2018).
- Klepser, M.E.; Dobson, E.L.; Pogue, J.M.; Labreche, M.J.; Adams, A.J.; Gauthier, T.P.; Turner, R.B.; Su, C.P.; Jacobs, D.M.; Suda, K.J.; et al. A call to action for outpatient antibiotic stewardship. J. Am. Pharm. Assoc. 2017, 57, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.A.; Karami, N.A.; Al-Muwalid, A.S.; Al-Otabi, A.; Al-Subahi, E.; Bamomen, A.; Mohamed, M.M.; Elrggal, M.E. Community pharmacists’ knowledge, attitude, and practices towards dispensing antibiotics without prescription (DAwP): A cross-sectional survey in Makkah Province, Saudi Arabia. Int. J. Infect. Dis. 2016, 47, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Ye, D.; Lv, B.; Jiang, M.; Zhu, S.; Yan, K.; Tian, Y.; Fang, Y. Sale of antibiotics without a prescription at community pharmacies in urban China: A multicentre cross-sectional survey. J. Antimicrob. Chemother. 2017, 72, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Chuc, N.T.K.; Hoa, N.P.; Hoa, N.Q.; Nguyen, N.T.T.; Loan, H.T.; Toan, T.K.; Phuc, H.D.; Horby, P.; Van Yen, N.; Van Kinh, N.; et al. Antibiotic sales in rural and urban pharmacies in northern Vietnam: An observational study. BMC Pharmacol. Toxicol. 2014, 15, 6. [Google Scholar]
- Dameh, M.; Norris, P.; Green, J. New Zealand pharmacists’ experiences, practices and views regarding antibiotic use without prescription. J. Prim. Health Care 2012, 4, 131–140. [Google Scholar] [CrossRef]
- Guillemot, D.; Varon, E.; Bernède, C.; Weber, P.; Henriet, L.; Simon, S.; Laurent, C.; Lecoeur, H.; Carbon, C. Reduction of antibiotic use in the community reduces the rate of colonization with Penicillin G—Nonsusceptible Streptococcus pneumoniae. Clin. Infect. Dis. 2005, 41, 930–938. [Google Scholar] [CrossRef] [Green Version]
- Nasrin, D. Effect of β-lactam antibiotic use in children on pneumococcal resistance to penicillin: Morospective cohort study. BMJ 2002, 5, 324–328. [Google Scholar] [CrossRef] [Green Version]
- Jamshed, S.; Padzil, F.; Shamsudin, S.H.; Bux, S.H.; Jamaluddin, A.A.; Bhagavathula, A.S.; Azhar, S.; Hassali, M.A. Antibiotic stewardship in community pharmacies: A scoping review. Pharmacy 2018, 6, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Study Author Year | Country and Population | Methods and Mode | Response Rate | Questionnaire Developed by | Validation and no. of Questions | Outcome Domain | Reliability | Quality |
|---|---|---|---|---|---|---|---|---|
| Rizvi et al., 2018 | Australia Tasmanian CPs | Cross-sectional survey Online Email, fax and post | 61% (85/140) | Rizvi et al. | Validated 38 | K, Per, P, B, F | + | High |
| Khan et al., 2016 | Malaysia CPs from State of Selangor | Cross-sectional survey Paper-based | 83.5% (188/225) | Khan et al. | Validated 24 | Per, P | + | High |
| Erku et al., 2016 | Ethiopia CPs from eight cities of Ethiopia | Cross-sectional survey Paper-based | 86.6% (334/389) | Khan et al. | Validated 24 | Per, P | + | High |
| Pawluk et al., 2015 | Qatar CPs from Qatar | Cross-sectional survey Paper-based workshop | 51.6% (32/62) | Pawluk et al. | Developed by literature review 13 | Per, F | - | Low |
| Avent et al., 2018 | Australia CPs from Queensland | Cross-sectional survey Online e-newsletter | - 120 responses | Avent et al. | Not validated 21 | P, B | - | Low |
| Sarwar et al., 2018 | Pakistan CPs from Punjab province | Cross-sectional survey paper-based | 96.6% (400/441) | Sarwar et al. and Khan et al. | Validated 29 | A, P, B, F | + | High |
| Wilcock et al., 2017 | UK | Cross-sectional survey Paper-based | 91.9% (57/62) | Wilcock et al. | Not validated 10 | P, B | - | Low |
| Rehman et al., 2018 | Pakistan Urban settings | Cross-sectional survey Paper-based | 37% (20/67) | Khan et al. | Validated 26 | Per, P | + | Medium |
| Hancock et al., 2016 | UK CPs of Huddersfield town centre | cross sectional survey Paper-based | - 50 respondents | Hancock et al. | Not validated 28 | A, P, B, F | - | Medium |
| Lee et al., 2017 | Canada CPs from Saskatchewan | Cross sectional survey Paper-based | 12.4% (138/1109) | Lee et al. | Not validated 19 | K, A | - | Low |
| N | Criteria | Reviewer (R) | Rizvi et al., 2018 | Khan et al., 2016 | Erku et al., 2016 | Pawluk et al., 2015 | Avent et al., 2018 | Sarwar et al., 2018 | Wilcock et al., 2017 | Rehman et al., 2018 | Hancock et al., 2016 | Lee et al., 2017 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Was there a clearly defined research question? | R1 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| R2 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| 2 | Did the authors select samples that well represent the population to be studied? | R1 | ✓ | ✓ | ✓ | x | x | ✓ | x | x | ✓ | x |
| R2 | ✓ | ✓ | ✓ | x | ? | ✓ | x | x | ✓ | x | ||
| 3 | Did the authors use designs that balance costs with errors? | R1 | ? | x | ? | x | ? | ? | x | ? | ? | ? |
| R2 | ? | x | x | x | ? | ? | x | ? | ? | ? | ||
| 4 | Did the authors describe the research instrument? | R1 | ✓ | ✓ | ✓ | x | x | ✓ | x | ✓ | ✓ | ✓ |
| R2 | ✓ | ✓ | ✓ | ? | x | ✓ | x | ✓ | ✓ | ? | ||
| 5 | Was the instrument pretested? | R1 | ✓ | ✓ | ✓ | ✓ | x | ✓ | x | ✓ | ? | x |
| R2 | ✓ | ✓ | ✓ | ✓ | x | ✓ | ? | ✓ | ? | ? | ||
| 6 | Were quality control measures described? | R1 | ✓ | ? | ✓ | x | ? | ✓ | x | ✓ | ✓ | x |
| R2 | ✓ | ? | ✓ | x | x | ✓ | x | ? | ✓ | ? | ||
| 7 | Was the response rate sufficient to enable generalizing the results to the target population? | R1 | ✓ | ✓ | ✓ | x | ? | ✓ | x | x | x | x |
| R2 | ✓ | ✓ | ✓ | x | x | ✓ | x | x | x | x | ||
| 8 | Were the statistical, analytic, and reporting techniques appropriate to the data collected? | R1 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ? | x | ✓ | ✓ |
| R2 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | ? | ✓ | ||
| 9 | Was evidence of ethical treatment of human subjects provided? | R1 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| R2 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| 10 | Were the authors transparent to ensure evaluation and replication? | R1 | ✓ | ✓ | ✓ | x | x | ✓ | x | ✓ | x | x |
| R2 | ✓ | ✓ | ? | x | x | ✓ | x | ✓ | ? | x | ||
| Quality of survey studies | H | H | H | L | L | H | L | M | M | L | ||
| Items | Median (%) | IQR |
|---|---|---|
| AMS improve patient care (n = 6) | 86.0 | 83.3–93.5 |
| AMS reduce inappropriate use (n = 2) | 84.0 | 83–85 |
| CPs have important role in AMS (n = 4) | 93.0 | 90.8–94.7 |
| Willing to participate in future AMS initiatives (n = 6) | 87.8 | 83.6–90.3 |
| AMS should be practiced at community pharmacy level (n = 3) | 78.0 | 52.5–79.3 |
| AMS reduce infection associated costs (n = 1) | 78.0 | – |
| Health-care professionals other than prescribers need to understand AMS (n = 3) | 69.0 | 66.8–84.5 |
| Individual efforts at AMS have minimal impact on the antimicrobial resistance problem (n = 3) | 51.4 | 40.7–69.4 |
| AMS Practice Components | % CPs Often or Always Do This Practice | |
|---|---|---|
| Median | IQR | |
| Collaboration with prescribers | ||
| Collaborate with prescribers in case of uncertainty in appropriateness of antibiotic prescription (n = 5) | 77.0 | 55.2–77.8 |
| Collaborate with other health care professionals for infection control and AMS (n = 4) | 54.7 | 34.8–63.2 |
| Contacting prescriber when patient is allergic to prescribed antibiotic (n = 1) | 98.6 | – |
| Contacting prescriber when choice of antibiotic may not be optimal (n = 1) | 46.5 | – |
| Educating patients | ||
| Provide antibiotic information to patients (n = 1) | 56 | – |
| Educate patients on the use of antimicrobials and drug resistance issues (n = 5) | 53.0 | 43.2–67.4 |
| Provide clear message on expected side effect of using antibiotics (n = 1) | 86 | – |
| Provide advice to the patients when it would be appropriate to use repeat (n = 1) | 82.9 | – |
| Dispensing process | – | |
| Dispense antimicrobials without prescription (n = 5) | 34.1 | 19.4–47.0 |
| Screen antimicrobial prescription in accordance with guidelines before dispensing (n = 3) | 47.5 | 25.2–58.3 |
| Consider clinical safety parameters (drug interaction, allergy, ADRs) before dispensing (n = 5) | 68.7 | 53.6–70.7 |
| Evaluate prescription according to good dispensing practice guidelines (n = 1) | 33.4 | – |
| Refer patients to general practitioners when symptoms are suggestive of an infection (n = 1) | 99 | – |
| Recommending over the counter (OTC)/self-care treatment to patient with infections not needing antibiotics (n = 1) | 95.8 | – |
| Do not dispense delayed antibiotic prescription within 24 h of seeing doctor (n = 1) | 60 | – |
| Dispensed antibiotics for longer durations than prescribed by physicians (n = 2) | 18.4 | 13.6–23.2 |
| Participation in AMS campaign | ||
| Take part in AMS campaign/awareness movement (n = 1) | 40.9 | 20.4–41.5 |
| Barriers | Facilitators | Proposed Recommendation to Improve AMS in Community Pharmacy |
|---|---|---|
| Personal | Personal | Personal level |
| Education and training | Familiarity of AMS term Positive perception about AMS Willingness to participate future AMS training, workshop or conferences Skills of assessing drug interaction, adverse drug reactions (ADRs) and allergies to prescribed antibiotics | Provision of AMS training as a part of the CPD program |
| Interpersonal | Interpersonal | Interpersonal-level |
| Prescriber-CP interaction Non-receptive behaviours of GPs to pharmacist intervening the choice of antibiotics Fear of losing relationship with GPs while measuring guideline compliance of antimicrobial prescriptions | Positive intention to collaborate with prescribers | GP-CP network (policy guided) Local GP-pharmacy practice agreement |
| Community/policy | Community/policy | Community/policy level |
| provision of AMS campaign prolonged (e.g.,12 months) repeat dispensing of antibiotic policy Culture of GP-pharmacy team-based service CPs’ roles are not defined in AMS Limited patient awareness about CPs’ role in AMS | Professional organisation’s training modules and tool kits (e.g., NPS Medicine Wise, CDC, NHS) | Restriction on OTC sale of antibiotics Provision of providing audit and feedback data on both prescribing and dispensing Provision of patient education on antibiotic use, resistance and repeat use Use of patients leaflets (e.g., self-care advice for infections and antibiotic compliance advice) Public awareness campaign relevant with AMS Pharmacy professional organizations should define the role of CPs in AMS as a policy document |
| Health system structure | Health system structure | Health system structure-level |
| Accessibility of patient’s records and laboratory data No AMS compliant dispensing guidelines Technology that supports GP-CP communication Time poor settings No provision of point-of-care (POC) testing service to differentiate bacterial or viral infection | - | Decision support tools (antimicrobials review tools) IT technology Provision of guidelines to undertake AMS in pharmacy practices POC testing services and relevant training for CPs Provision of use of therapeutic guidelines by CPs to ensure appropriateness of antimicrobials |
| Financial | Financial | Financial-level |
| Reimbursement models Remuneration for AMS services | Remuneration for pharmacies involved in AMS programs Financing mechanism for GP-pharmacy collaboration |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saha, S.K.; Barton, C.; Promite, S.; Mazza, D. Knowledge, Perceptions and Practices of Community Pharmacists Towards Antimicrobial Stewardship: A Systematic Scoping Review. Antibiotics 2019, 8, 263. https://doi.org/10.3390/antibiotics8040263
Saha SK, Barton C, Promite S, Mazza D. Knowledge, Perceptions and Practices of Community Pharmacists Towards Antimicrobial Stewardship: A Systematic Scoping Review. Antibiotics. 2019; 8(4):263. https://doi.org/10.3390/antibiotics8040263
Chicago/Turabian StyleSaha, Sajal K., Chris Barton, Shukla Promite, and Danielle Mazza. 2019. "Knowledge, Perceptions and Practices of Community Pharmacists Towards Antimicrobial Stewardship: A Systematic Scoping Review" Antibiotics 8, no. 4: 263. https://doi.org/10.3390/antibiotics8040263
APA StyleSaha, S. K., Barton, C., Promite, S., & Mazza, D. (2019). Knowledge, Perceptions and Practices of Community Pharmacists Towards Antimicrobial Stewardship: A Systematic Scoping Review. Antibiotics, 8(4), 263. https://doi.org/10.3390/antibiotics8040263