Abstract
Background: Helicobacter pylori eradication containing the potassium-competitive acid blocker, vonoprazan, achieves a higher eradication rate than therapy with proton pump inhibitors (PPIs). Because vonoprazan is mainly metabolized by CYP3A4/5, CYP genotype may affect the eradication rate. We investigated the influence of antibiotic susceptibility and CYP3A4/5 and CYP2C19 genotypes on the eradication rates. Methods: A total of 307 Japanese who were genotyped for CYP3A4 *1/*22, CYP3A5 *1/*3 and CYP2C19 *1/*2/*3/*17, and investigated for susceptibility to antimicrobial agents, received vonoprazan-containing regimens: (1) With amoxicillin and clarithromycin as the first-line treatment; (2) with amoxicillin and metronidazole as the second-line treatment; or (3) with amoxicillin and sitafloxacin as the third-line treatment. Results: The eradication rate was 84.5% (95% confidence interval [CI]: 78.9–89.1%) using first-line, 92.6% (95% CI: 82.1–97.9%) using second-line and 87.5% (95% CI: 73.1–95.8%) using third-line treatment. Infection with clarithromycin-resistant strains was a predictive factor for failed eradication (odds ratio: 5.788, 95% CI: 1.916–17.485, p = 0.002) in multivariate analysis. No significant differences were observed in the eradication rate of regimens among CYP3A4, CYP3A5 and CYP2C19 genotypes. Conclusions: Genotyping for CYP3A4 *1/*22, CYP3A5 *1/*3 and CYP2C19 *1/*2/*3/*17 before vonoprazan-containing eradication treatment may not be useful for predicting clinical outcomes.
1. Introduction
In 2013, the Japanese health insurance system began covering eradication treatment for all Helicobacter pylori-positive patients [1]. However, eradication rates of first-line therapy, twice-daily dosing (bid) with a proton pump inhibitor (PPI), amoxicillin (750 mg), and clarithromycin (200 mg or 400 mg) for 7 days, have decreased to approximately 65% due to a > 35% prevalence of clarithromycin-resistant H. pylori strains in Japan [1,2]. The cure rate of PPI-containing triple therapy is affected by several factors, including antibiotic susceptibility (e.g., clarithromycin, amoxicillin, and metronidazole) [1,2,3], insufficient acid inhibition during eradication treatment (e.g., CYP2C19 genotype, dose of drug, treatment schedule and type of acid-inhibitory drug) [3,4,5], the environment (e.g., smoking), poor adherence to medication and infection of H. pylori strain with low virulence activity (e.g., cagA-negative, vacA s2 genotype and dupA-negative strains) [4,6]. Previously, we showed that an intragastric pH > 4 must be maintained for 24 h and that the 24-h pH should be higher than 6.0 for successful eradication in the first-line triple therapy [5]. However, because it is not possible to maintain pH > 4.0 for 24 h in all patients using triple therapy with a standard dose of PPI bid, [7,8] treatment failure is often observed in such an insufficient patients [5,9,10]. A recent study reported that vonoprazan 20 mg inhibits H+/K+-ATPase activity at a 400-fold lower dose than lansoprazole 30 mg at pH 6.6 [11]. Therefore, vonoprazan-containing eradication therapy appears to have a higher eradication rate than PPI-containing regimen [12,13,14,15,16].
Because PPIs, such as omeprazole, lansoprazole and rabeprazole, undergo extensive hepatic metabolism by CYP2C19 [17], differing plasma PPI levels and intragastric pH values after administration of PPIs among CYP2C19 genotypes can be a clinical problem [7,18,19,20]. In general, the effect of CYP2C19 genotype on outcome of PPI-containing eradication treatment cannot be ignored, especially in CYP2C19 extensive metabolizers (EMs). In contrast, vonoprazan is metabolized to its inactive form mainly by CYP3A4/5 and partially by CYP2C19, making the effects of vonoprazan less affected by CYP2C19 genotype than PPIs [21]. However, although it is expected to associate with the outcome of vonoprazan-containing eradication therapy and CYP3A4/5 genotype, it is unclear whether CYP3A4/5 and CYP2C19 genotype influence the outcome of vonoprazan-containing therapy [22].
It is important to identify any factors that may influence the clinical outcome of vonoprazan-containing eradication therapy and to determine optimal alternative vonoprazan-containing regimens. Here, we assessed antibiotic susceptibility and the influence of CYP3A4/5 and CYP2C19 genotype on the clinical outcome of first-line, second-line and third-line vonoprazan-containing triple eradication therapies in Japanese.
2. Materials and Methods
We retrospectively investigated a total of H. pylori-positive patients treated with eradication therapy after upper gastroduodenal endoscopy at the Shiga University of Medical Science Hospital from April 2015 to December 2019 (Table 1). We excluded patients who had no informed consent, no result of eradication outcome, no detailed clinical information including CYP2C19 genotype and had more than three time of eradication history (Figure 1).

Table 1.
Characteristics of patients positive for Helicobacter pylori.
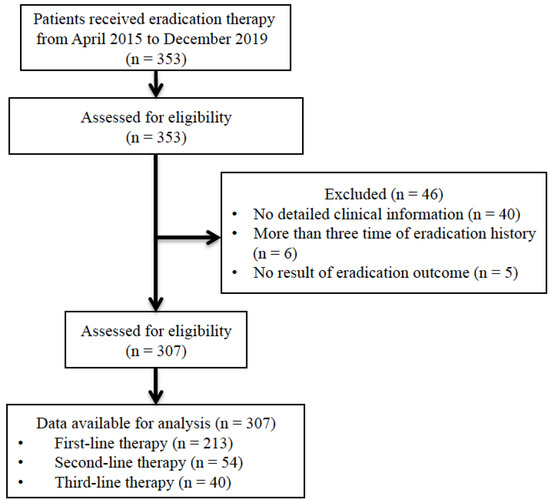
Figure 1.
Flow for the selection of patients.
The study was conducted in accordance with the guidelines of the Declaration of Helsinki. Approval for the study protocol was obtained in advance from the Institutional Review Board of the Shiga University of Medicine Science. Written informed consent was obtained from each patient who underwent endoscopy. The information about this study was available online of Shiga University of Medical Science Hospital, and the participants gave their informed consent.
2.1. Treatment Regimen
Patients were treated with vonoprazan 20 mg bid and a combination of two antimicrobial agents, amoxicillin (750 mg, bid) and clarithromycin (200 mg, bid) as first-line treatment (n = 213); amoxicillin (750 mg, bid) and metronidazole (250 mg, bid) as second-line treatment (n = 54); or amoxicillin (500 mg, qid) and sitafloxacin (100 mg, bid) as third-line treatment (n = 40) for 7 days.
2.1.1. CYP2C19, CYP3A4 and CYP3A5 Genotyping
Genomic DNA was extracted from the blood (DNA Extract All Reagents, Applied Biosystems, Foster City, CA, USA). Genotyping was performed using a single-nucleotide polymorphism genotyping assay (StepOnePlusTM, Applied Biosystems) in a real-time polymerase chain reaction system. We evaluated polymorphisms in CYP3A4*22 (rs35599367, C>T) and CYP3A5*3 (rs776746, G>A). To classify each subject, genotyping was performed to identify the CYP2C19 wild-type gene and three mutant alleles, CYP2C19 *2 (rs4244285, A/G), *3 (rs-4986893, G/A) and *17 (rs12248560, A/C/T).
2.1.2. Esophagogastroduodenoscopy
The six grades of the Kimura-Takemoto gastric atrophy classification were used: Closed (C)-I, C-II, C-III, and Open (O)-I, O-II, and O-III [23]. Patients were also scored based on the severity of atrophy, intestinal metaplasia, hypertrophy of gastric folds, and diffuse redness according to the Kyoto classification of gastritis [24].
2.1.3. Infection Status and Measurement of Antibiotic Resistance
Infection status was evaluated based on findings from three tests: An anti-H pylori IgG serological test, a rapid urease test, and a culture test. Patients were diagnosed as being positive for H. pylori infection when positive results were obtained in at least one of the three tests. Eradication success was evaluated using a 13C-urea breath test with a cut-off value of 2.5 ‰ at 6–8 weeks after treatment.
For bacterial culture and antimicrobial sensitivity testing, agar plates were inoculated with biopsy specimens and incubated at 37 °C under microaerophilic conditions. H. pylori colonies were subcultured using the agar dilution method to determine the minimum inhibitory concentration (MIC) for amoxicillin, metronidazole, clarithromycin and sitafloxacin. Cut-off MICs used to define resistance were > 1.0 µg/mL for clarithromycin and sitafloxacin and > 8 µg/mL for metronidazole [25]. The cut-off MICs used to define resistance and the absence of sensitivity were > 0.5 µg/mL and > 0.06 µg/mL for amoxicillin, respectively.
2.2. Data Analysis
The patients enrolled in this study who were recruited from 2015 to 2017 were overlapped with those in our previous report performed as a preliminary study (n =126) [22]. Age is shown as mean ± standard deviation (SD). Eradication rate was evaluated using intention-to-treat (ITT) and per-protocol (PP) analyses and calculated with 95% confidence intervals (CIs). Statistical differences in eradication rates among the regimens and CYP2C19, CYP3A4, and CYP3A5 genotypes were assessed using Fisher’s exact test. All p-values were two-sided, and p < 0.05 was considered statistically significant. Calculations were conducted using commercial software (SPSS version 20, IBM Inc.; Armonk, NY, USA).
3. Results
Of a total of 353 H. pylori-positive patients treated eradication therapy at Shiga University of Medical Science Hospital from April 2015 to December 2019, we excluded 46 patients who had no result of eradication outcome (n = 5), no detailed clinical information including CYP2C19 genotype (n = 40) and had more than three time of eradication history (n = 6) (Figure 1). Of the remaining 307 patients, 213 had no prior eradication history, 54 had undergone one course of eradication treatment (PPI or vonoprazan with clarithromycin and amoxicillin), and 40 had undergone two courses (PPI or vonoprazan with clarithromycin and amoxicillin as first-line treatment and PPI or vonoprazan with metronidazole and amoxicillin as second-line treatment). There were no significant differences in age, sex, body weight, height, or history of smoking and drinking among the first-, second-, and third-line treatment groups (Table 1).
In patients receiving first-line therapy, the prevalence of the CYP2C19 genotype was 3.3% (7/213) in ultra rapid metabolizers (UR), 25.8% (55/213) in EM, 52.1% (111/213) in intermediate metabolizers (IM) and 18.8% (40/213) in poor metabolizers (PM) (Table 1). The prevalence of CYP3A5 polymorphisms was 8.3% for CYP3A5 *1/*1, 39.3% for *1/*3, and 52.4% for *3/*3 (Table 1). There was no significant difference in the prevalence of CYP2C19 or CYP3A5 genotype among patients receiving first-, second- and third-line therapies. In this study, no patients had the *22 mutant allele in CYP3A4.
In the association with eradication time and endoscopic finding, the score for diffuse redness in patients receiving third-line therapy was significantly lower than that in patients receiving first- (p = 0.006) and second-line therapies (p = 0.022) (Table 1).
3.1. Susceptibility to Antimicrobial Agents
Among patients receiving first-line therapy, 40.6% (56/138) had clarithromycin-resistant strains (Table 1). The proportion of patients showing no sensitivity to amoxicillin and metronidazole resistance was 14.5% (20/138) and 8.0% (11/138), respectively. Among patients receiving second-line therapy, the proportion showing clarithromycin and metronidazole resistance and no sensitivity to amoxicillin was 77.4%, 9.7%, and 32.3%, respectively.
3.2. Eradication Rates in Vonoprazan-Containing Eradication Therapy
The eradication rate was 84.5% (95% CI: 78.9–89.1%) using first-line treatment, 92.6% (95% CI: 82.1–97.9%) using second-line treatment and 87.5% (95% CI: 73.1–95.8%) using third-line treatment (p = 0.295) (Table 2). Although the eradication rate in CYP2C19 UM treated with first-line treatment was lower (57.1%) than that in other genotypes (81.1–90.9%), there was no significant difference among CYP2C19 genotypes irrespective of whether they received first-, second-, or third-line therapy. Among those who received first-line treatment, the eradication rate in CYP3A5 *1 allele carriers was 82.1% (95% CI: 69.6–91.1%, 46/56), which is similar to that in the *3/*3 type (84.7%, 95% CI: 73.0–92.8%, 50/59, p = 0.344) (Table 2).
Table 2.
Eradication rates in the first-line, second-line and third-line regimens.
Among those who received first-line treatment, the eradication rate in patients infected with H. pylori strains sensitive and resistant to clarithromycin was 91.5% (95% CI: 83.1–96.5%) and 71.4% (95% CI: 57.8–82.7%), respectively (Table 2). The eradication rate in patients infected with strains that were not sensitive to amoxicillin was lower than that in patients infected with amoxicillin-sensitive strains, albeit not significantly so. Likewise, no significant difference in eradication rate was observed between metronidazole-sensitive and -resistant strains.
In the univariate analysis, infection with clarithromycin-resistant strains (OR: 4.286, 95% CI: 1.628–11.279, p = 0.003), endoscopic diffuse redness (OR: 2.868, 95% CI: 1.092–7.530, p = 0.032) and total endoscopic score based on the Kyoto classification of gastritis (OR: 1.470, 95% CI: 1.057–2.043, p = 0.022) were identified as predictive factors for failed eradication (Table 3). In the multivariate analysis, which examined factors showing a p-value < 0.2 in the univariate analysis (sex, endoscopic intestinal metaplasia, endoscopic diffuse redness, clarithromycin resistance, and no sensitivity to amoxicillin), infection with clarithromycin-resistant strains was identified as a predictive factor for failed eradication (OR: 5.788, 95% CI: 1.916–17.485, p = 0.002) (Table 3).
Table 3.
Univariate and multivariate analyses of factors for eradication failure in first-line therapy.
3.3. Complications
Among 260 patients, 63 experienced adverse events, including diarrhea (n = 19), loose stools (n = 18), abdominal pain (n = 9) and allergic reaction (n = 10) (Table 4). There was no significant difference in the incidence of adverse events among the treatment regimens.
Table 4.
Adverse events related to eradication treatment.
4. Discussion
Successful eradication therapy for H. pylori infection using acid-sensitive anti-microbial agents, such as clarithromycin and amoxicillin, requires the maintenance of an intragastric pH > 4.0 for 24 h a day [5,9,10]. In this study, we demonstrated that vonoprazan-containing eradication therapy was well tolerated and achieved an eradication rate of approximately 85%, irrespective of prior eradication history (84.5% for first-line, 92.6% for second-line, and 87.5% for third-line therapy). In addition, we examined the influence of genetic variations in drug-metabolizing liver enzymes (i.e., CYP2C19, CYP3A4, and CYP3A5) on the outcomes of vonoprazan-containing regimens and found that there was no significant difference among genotypes. Despite the preliminary nature of this study, owing to its limited sample size, we showed that infection with clarithromycin-resistant strains may be a risk factor for failed eradication using first-line vonoprazan-containing therapy. We therefore recommend the use of alternative first-line therapies in patients infected with clarithromycin-resistant strains.
4.1. Eradication Rate of Vonoprazan-Containing First-Line Eradication Therapy
Vonoprazan induces sustained acid inhibition throughout a 24-h period, with the pH ≥ 4 and ≥ 5 holding time ratios for vonoprazan 20 mg bid being 100% and 99%, respectively, even in H. pylori-negative subjects [26]. Consistent acid inhibition increases the stability and bioavailability of acid-sensitive antibiotics, preventing their degradation and increasing their concentration in the gastric mucosa [9,27,28]. In 2016, a phase III randomized, double-blind study reported an eradication rate of 92.6% (95% CI: 89.2–95.2%) using a first-line vonoprazan-containing regimen and 75.9% (70.9–80.5%) using a lansoprazole-containing regimen [12]. Other studies have reported that the efficacy of first-line vonoprazan-containing regimens ranges from 82.9% to 94.6% [13,14,15,16,29,30,31]. Based on 21 studies that investigated a total of 12,010 patients receiving PPI-containing first-line therapy, no studies reported an eradication rate higher than 85% [32]. Therefore, as observed in this study, potent acid inhibition using vonoprazan is a key requirement for successful eradication in Japanese.
4.2. Eradication Rate of Vonoprazan-Based First-Line Therapy for Clarithromycin-Resistant H. pylori Strains
Clarithromycin resistance is a rising clinical problem for H. pylori eradication in many countries where the antibiotic has been widely used to treat patients with bacterial infection, making bacterial culture and antimicrobial sensitivity testing effective clinical options. In fact, a randomized controlled trial has shown that vonoprazan-containing first-line therapy is significantly superior to PPI-containing therapy in patients with clarithromycin-resistant strains (eradication rate: 82.0% [vonoprazan] and 40.0% [PPI], OR: 6.83, 95% CI: 3.63–12.86, p < 0.0001) [33]. In this study, 40.6% (56/138) of patients receiving first-line treatment were infected with clarithromycin-resistant strains and the eradication rate was 71.4% (95% CI: 57.8–82.7%) and 91.5% (95% CI: 83.1–96.5%) in patients infected with strains resistant and sensitive to clarithromycin, respectively. Infection with clarithromycin-resistant strains was identified as a predictive factor for failed eradication in multivariate analysis (OR: 5.788, 95% CI: 1.916–17.485, p = 0.002). Given that an eradication rate of 80% is not satisfactory, alternative treatment options, such as replacing clarithromycin with metronidazole, are needed to obtain a higher eradication rate in patients infected with clarithromycin-resistant strains. Then, future trials should investigate the efficacy of vonoprazan-containing concomitant therapy, sequential therapy, and bismuth-containing quadruple therapy.
4.3. Second-Line and Third-Line Vonoprazan-Containing Eradication Therapy
While the prevalence of metronidazole-resistant strains is 5–12% in Japan and metronidazole is not an acid-sensitive antimicrobial agent, the eradication rate of PPI/metronidazole-containing second-line regimen has remained constant at approximately 80%. A meta-analysis showed that the eradication rate of vonoprazan-containing regimens (83.4%) is similar to that for PPI-containing regimens (81.2%, OR: 1.04, 95% CI: 0.77–1.42, p = 0.79) [34]. Therefore, PPI/amoxicillin/metronidazole regimen may be recommended as a second-line treatment over vonoprazan-containing regimens due to cost-effectiveness and comparable efficacy and safety in Japan.
Eradication therapy using PPI/amoxicillin/sitafloxacin or PPI/metronidazole/sitafloxacin is the main third-line regimen in Japan [35,36,37,38]. However, reports investigating the efficacy of vonoprazan-containing third-line treatment are limited [39]. Sitafloxacin is a new quinolone antibacterial agent that is expected to show efficacy due to its low MIC for H. pylori, and the low rate of sitafloxacin-resistant strains (less than 10%) is a strong motivator for its use as an eradication therapy [37,38]. Sitafloxacin is also an acid-sensitive antimicrobial agent, whose stability and bioavailability are increased by potent acid inhibition. Evidence from the present and a previous study suggest that the vonoprazan/amoxicillin/sitafloxacin regimen is more effective than PPI-containing regimens as a third-line therapy in patients [39].
4.4. Vonoprazan-Containing Eradication Therapy and CYP3A4/5 and CYP2C19 Genotype
Because vonoprazan is metabolized mainly by CYP3A4/5 and partially by CYP2B6, CYP2C19, and CYP2D6 [21], its pharmacokinetics and pharmacodynamics may be influenced by genetic variations in the respective genes. Many drugs are metabolized by CYP3A4, and the CYP3A4*22 decrease-of-function allele has been associated with attenuated metabolism of CYP3A4-dependent drugs, such as statins and tacrolimus [40]. CYP3A4 enzyme activity in the CYP3A4 *1 /*1 wild-type genotype is 2.5-fold higher than that in CYP3A4 *22 carriers [40]. However, no patients in this study had the CYP3A4 *22 allele. Therefore, the influence of this and other CYP3A4 polymorphisms associated with CYP3A4 protein expression levels in Japanese warrants further investigation.
The inter-individual variability in the pharmacokinetics of CYP3A5-metabolized drugs is explained by a single nucleotide polymorphism in intron 3 of CYP3A5, 6986A > G. Blood tacrolimus levels are higher in patients with the CYP3A5 *3/*3 genotype than *1 genotype [41,42]. We previously reported that the incidence of adverse events in ulcerative colitis patients treated with tacrolimus was significantly higher in CYP3A5 expressers than non-expressers [43]. The elimination rate of vonoprazan was significantly correlated with CYP3A4/5 activity, suggesting that CYP3A4/5 activity influences the pharmacokinetics of vonoprazan [21]. However, although our previous preliminary report showed a significant association between CYP3A5 genotype and vonoprazan-containing treatment outcome in the first-line triple therapy [22], when we entered the larger number of patients in this study, we failed to show a significant association. Although significant differences were not observed in the eradication rate of vonoprazan-containing regimens among CYP3A4 genotypes, the findings about the importance of clarithromycin-resistance rather than such genotype for eradication is thought to be a significance on clinical pharmacology. Previously, because there was no data to investigate pharmacokinetics (PK)/pharmacodynamics (PD) of vonoprazan among different CYP3A5 genotypes, future trials should investigate the direct association between CYP3A5 genotype and the PK/PD of vonoprazan to clarify this concern.
Acid inhibition by administration of vonoprazan 20 mg qd and bid is similar among CYP2C19 genotypes [26]. Murakami et al [12] reported an eradication rate of 92.9% in CYP2C19 EMs/IMs, which was similar to that in PMs (90.9%). We found no significant difference in eradication rates among CYP2C19 genotypes. These observations suggest that CYP2C19 genotype-based tailored treatment using vonoprazan may not be necessary for acid-related diseases.
5. Conclusions
We assessed the effect of CYP3A4/5 and CYP2C19 genotype and antibiotic susceptibility on clinical outcome following treatment with first-line, second-line and third-line vonoprazan-containing therapy in Japanese. Vonoprazan-related genetic variations in CYP3A4/5 and CYP2C19 were not associated with clinical outcome of H pylori eradication therapy. Although vonoprazan-containing triple therapy shows high efficacy in terms of H. pylori eradication compared to PPI-containing therapy, especially in patients infected with clarithromycin-resistant strains, an eradication rate of 80% is not satisfactory. We think there is potential for the development of a culture test-based tailored treatment that can achieve an eradication rate exceeding 95%.
Author Contributions
Conceptualization: M.S.; Methodology: M.S.; Software: M.S.; Formal Analysis: M.S. and M.M.; Investigation: M.S., M.M. and D.H.; Data Curation: M.S.; Writing—Original Draft Preparation: M.S.; Writing—Review and Editing: M.S., D.H., M.M., T.K. and T.T.; Visualization: M.M.; Supervision: M.S.; Project Administration: M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a Grant-in-aid for Scientific Research from the Ministry of Education, Culture, Sports, Science & Technology of Japan (18K07938).
Acknowledgments
We thank Heidi Tran, PhD, from DMC Corp. (http://www.dmed.co.jp/) for editing drafts of this manuscript.
Conflicts of Interest
None of the authors have any conflict of interest related to this study.
References
- Asaka, M.; Sugiyama, T.; Kato, M.; Satoh, K.; Kuwayama, H.; Fukuda, Y.; Fujioka, T.; Takemoto, T.; Kimura, K.; Shimoyama, T.; et al. A multicenter, double-blind study on triple therapy with lansoprazole, amoxicillin and clarithromycin for eradication of Helicobacter pylori in Japanese peptic ulcer patients. Helicobacter 2001, 6, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sato, R.; Okimoto, T.; Nasu, M.; Fujioka, T.; Kodama, M.; Kagawa, J.; Sato, S.; Abe, H.; Arita, T. Eradication rates of clarithromycin-resistant Helicobacter pylori using either rabeprazole or lansoprazole plus amoxicillin and clarithromycin. Aliment. Pharmacol. Ther. 2002, 16, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Shirai, N.; Takashima, M.; Xiao, F.; Hanai, H.; Sugimura, H.; Ohashi, K.; Ishizaki, T.; Kaneko, E. Effect of genotypic differences in CYP2C19 on cure rates for Helicobacter pylori infection by triple therapy with a proton pump inhibitor, amoxicillin, and clarithromycin. Clin. Pharmacol. Ther. 2001, 69, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Yamaoka, Y. Virulence factor genotypes of Helicobacter pylori affect cure rates of eradication therapy. Arch. Immunol. Ther. Exp. (Warsz.) 2009, 57, 45–56. [Google Scholar] [CrossRef]
- Sugimoto, M.; Furuta, T.; Shirai, N.; Kodaira, C.; Nishino, M.; Ikuma, M.; Ishizaki, T.; Hishida, A. Evidence that the degree and duration of acid suppression are related to Helicobacter pylori eradication by triple therapy. Helicobacter 2007, 12, 317–323. [Google Scholar] [CrossRef]
- Shiota, S.; Nguyen, L.T.; Murakami, K.; Kuroda, A.; Mizukami, K.; Okimoto, T.; Kodama, M.; Fujioka, T.; Yamaoka, Y. Association of helicobacter pylori dupA with the failure of primary eradication. J. Clin. Gastroenterol. 2012, 46, 297–301. [Google Scholar] [CrossRef]
- Sugimoto, M.; Furuta, T.; Shirai, N.; Kajimura, M.; Hishida, A.; Sakurai, M.; Ohashi, K.; Ishizaki, T. Different dosage regimens of rabeprazole for nocturnal gastric acid inhibition in relation to cytochrome P450 2C19 genotype status. Clin. Pharmacol. Ther. 2004, 76, 290–301. [Google Scholar] [CrossRef]
- Sahara, S.; Sugimoto, M.; Uotani, T.; Ichikawa, H.; Yamade, M.; Iwaizumi, M.; Yamada, T.; Osawa, S.; Sugimoto, K.; Umemura, K.; et al. Twice-daily dosing of esomeprazole effectively inhibits acid secretion in CYP2C19 rapid metabolisers compared with twice-daily omeprazole, rabeprazole or lansoprazole. Aliment. Pharmacol. Ther. 2013, 38, 1129–1137. [Google Scholar] [CrossRef]
- Grayson, M.L.; Eliopoulos, G.M.; Ferraro, M.J.; Moellering, R.C., Jr. Effect of varying pH on the susceptibility of Campylobacter pylori to antimicrobial agents. Eur. J. Clin. Microbiol. Infect. Dis. 1989, 8, 888–889. [Google Scholar] [CrossRef]
- Hunt, R.H. pH and Hp--gastric acid secretion and Helicobacter pylori: Implications for ulcer healing and eradication of the organism. Am. J. Gastroenterol. 1993, 88, 481–483. [Google Scholar]
- Hori, Y.; Imanishi, A.; Matsukawa, J.; Tsukimi, Y.; Nishida, H.; Arikawa, Y.; Hirase, K.; Kajino, M.; Inatomi, N. 1-[5-(2-Fluorophenyl)-1-(pyridin-3-ylsulfonyl)-1H-pyrrol-3-yl]-N-methylmethanamin e monofumarate (TAK-438), a novel and potent potassium-competitive acid blocker for the treatment of acid-related diseases. J. Pharmacol. Exp. Ther. 2010, 335, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016. [Google Scholar] [CrossRef] [PubMed]
- Shichijo, S.; Hirata, Y.; Niikura, R.; Hayakawa, Y.; Yamada, A.; Mochizuki, S.; Matsuo, K.; Isomura, Y.; Seto, M.; Suzuki, N.; et al. Vonoprazan versus conventional proton pump inhibitor-based triple therapy as first-line treatment against Helicobacter pylori: A multicenter retrospective study in clinical practice. J. Dig. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, D.; Akazawa, Y.; Takeshima, F.; Nakao, K.; Fukuda, Y. Safety and efficacy of Vonoprazan-based triple therapy against Helicobacter pylori infection: A single-center experience with 1118 patients. Therap. Adv. Gastroenterol. 2016, 9, 747–748. [Google Scholar] [CrossRef] [PubMed]
- Katayama, Y.; Toyoda, K.; Kusano, Y.; Suda, T.; Adachi, S.; Terauchi, I.; Oka, S.; Takahashi, M.; Tamano, M. Efficacy of vonoprazan-based second-line Helicobacter pylori eradication therapy in patients for whom vonoprazan-based fi rst-line treatment failed. Gut 2016. [Google Scholar] [CrossRef]
- Kawashima, K.; Ishihara, S.; Kinoshita, Y. Successful eradication of Helicobacter pylori infection with vonoprazan-based triple therapy after failure of PPI-based triple therapy. Dig. Liver Dis. 2016, 48, 688–689. [Google Scholar] [CrossRef]
- Ishizaki, T.; Horai, Y. Review article: Cytochrome P450 and the metabolism of proton pump inhibitors--emphasis on rabeprazole. Aliment. Pharmacol. Ther. 1999, 13 (Suppl. 3), 27–36. [Google Scholar] [CrossRef]
- Horai, Y.; Kimura, M.; Furuie, H.; Matsuguma, K.; Irie, S.; Koga, Y.; Nagahama, T.; Murakami, M.; Matsui, T.; Yao, T.; et al. Pharmacodynamic effects and kinetic disposition of rabeprazole in relation to CYP2C19 genotypes. Aliment. Pharmacol. Ther. 2001, 15, 793–803. [Google Scholar] [CrossRef]
- Shirai, N.; Furuta, T.; Moriyama, Y.; Okochi, H.; Kobayashi, K.; Takashima, M.; Xiao, F.; Kosuge, K.; Nakagawa, K.; Hanai, H.; et al. Effects of CYP2C19 genotypic differences in the metabolism of omeprazole and rabeprazole on intragastric pH. Aliment. Pharmacol. Ther. 2001, 15, 1929–1937. [Google Scholar] [CrossRef]
- Shirai, N.; Furuta, T.; Xiao, F.; Kajimura, M.; Hanai, H.; Ohashi, K.; Ishizaki, T. Comparison of lansoprazole and famotidine for gastric acid inhibition during the daytime and night-time in different CYP2C19 genotype groups. Aliment. Pharmacol. Ther. 2002, 16, 837–846. [Google Scholar] [CrossRef]
- Yamasaki, H.; Kawaguchi, N.; Nonaka, M.; Takahashi, J.; Morohashi, A.; Hirabayashi, H.; Moriwaki, T.; Asahi, S. In vitro metabolism of TAK-438, vonoprazan fumarate, a novel potassium-competitive acid blocker. Xenobiotica 2016, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Ban, H.; Hira, D.; Kamiya, T.; Otsuka, T.; Inatomi, O.; Bamba, S.; Terada, T.; Andoh, A. Letter: CYP3A4/5 genotype status and outcome of vonoprazan-containing Helicobacter pylori eradication therapy in Japan. Aliment. Pharmacol. Ther. 2017, 45, 1009–1010. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Takemoto, T. An Endoscopic Recognition of the Atrophic Border and its Significance in Chronic Gastritis. Endoscopy 1969, 1, 87–97. [Google Scholar] [CrossRef]
- Sugimoto, M.; Ban, H.; Ichikawa, H.; Sahara, S.; Otsuka, T.; Inatomi, O.; Bamba, S.; Furuta, T.; Andoh, A. Efficacy of the Kyoto Classification of Gastritis in Identifying Patients at High Risk for Gastric Cancer. Intern. Med. 2017, 56, 579–586. [Google Scholar] [CrossRef]
- Adamek, R.J.; Szymanski, C.; Pfaffenbach, B. Pantoprazole versus omeprazole in one-week low-dose triple therapy for curve of H. pylori infection. Am. J. Gastroenterol. 1997, 92, 1949–1950. [Google Scholar]
- Kagami, T.; Sahara, S.; Ichikawa, H.; Uotani, T.; Yamade, M.; Sugimoto, M.; Hamaya, Y.; Iwaizumi, M.; Osawa, S.; Sugimoto, K.; et al. Potent acid inhibition by vonoprazan in comparison with esomeprazole, with reference to CYP2C19 genotype. Aliment. Pharmacol. Ther. 2016, 43, 1048–1059. [Google Scholar] [CrossRef]
- Goddard, A.F.; Jessa, M.J.; Barrett, D.A.; Shaw, P.N.; Idstrom, J.P.; Cederberg, C.; Spiller, R.C. Effect of omeprazole on the distribution of metronidazole, amoxicillin, and clarithromycin in human gastric juice. Gastroenterology 1996, 111, 358–367. [Google Scholar] [CrossRef]
- Scott, D.; Weeks, D.; Melchers, K.; Sachs, G. The life and death of Helicobacter pylori. Gut 1998, 43 (Suppl. 1), S56–S60. [Google Scholar] [CrossRef]
- Kajihara, Y.; Shimoyama, T.; Mizuki, I. Analysis of the cost-effectiveness of using vonoprazan-amoxicillin-clarithromycin triple therapy for first-line Helicobacter pylori eradication. Scand. J. Gastroenterol. 2016, 1–4. [Google Scholar] [CrossRef]
- Yamada, S.; Kawakami, T.; Nakatsugawa, Y.; Suzuki, T.; Fujii, H.; Tomatsuri, N.; Nakamura, H.; Sato, H.; Okuyama, Y.; Kimura, H.; et al. Usefulness of vonoprazan, a potassium ion-competitive acid blocker, for primary eradication of Helicobacter pylori. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 550–555. [Google Scholar] [CrossRef]
- Shinozaki, S.; Nomoto, H.; Kondo, Y.; Sakamoto, H.; Hayashi, Y.; Yamamoto, H.; Lefor, A.K.; Osawa, H. Comparison of vonoprazan and proton pump inhibitors for eradication of Helicobacter pylori. Kaohsiung J. Med. Sci. 2016, 32, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Yamaoka, Y. Role of Vonoprazan in Helicobacter pylori Eradication Therapy in Japan. Front. Pharmacol. 2018, 9, 1560. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Oshima, T.; Horikawa, T.; Tozawa, K.; Tomita, T.; Fukui, H.; Watari, J.; Miwa, H. Systematic review with meta-analysis: Vonoprazan, a potent acid blocker, is superior to proton-pump inhibitors for eradication of clarithromycin-resistant strains of Helicobacter pylori. Helicobacter 2018, e12495. [Google Scholar] [CrossRef]
- Dong, S.Q.; Singh, T.P.; Wei, X.; Yao, H.; Wang, H.L. Review: A Japanese population-based meta-analysis of vonoprazan versus PPI for Helicobacter pylori eradication therapy: Is superiority an illusion? Helicobacter 2017, 22. [Google Scholar] [CrossRef]
- Furuta, T.; Sugimoto, M.; Kodaira, C.; Nishino, M.; Yamade, M.; Uotani, T.; Sahara, S.; Ichikawa, H.; Yamada, T.; Osawa, S.; et al. Sitafloxacin-based third-line rescue regimens for Helicobacter pylori infection in Japan. J. Gastroenterol. Hepatol. 2014, 29, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Furuta, T.; Ando, T.; Nakajima, T.; Inui, Y.; Oshima, T.; Tomita, T.; Mabe, K.; Sasaki, M.; Suganuma, T.; et al. Multi-center randomized controlled study to establish the standard third-line regimen for Helicobacter pylori eradication in Japan. J. Gastroenterol. 2013, 48, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Suzuki, H.; Matsuzaki, J.; Tsugawa, H.; Fukuhara, S.; Miyoshi, S.; Hirata, K.; Seino, T.; Matsushita, M.; Masaoka, T.; et al. Efficacy of 10-day Sitafloxacin-Containing Third-Line Rescue Therapies for Helicobacter pylori Strains Containing the gyrA Mutation. Helicobacter 2016, 21, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Sahara, S.; Ichikawa, H.; Kagami, T.; Uotani, T.; Furuta, T. High Helicobacter pylori cure rate with sitafloxacin-based triple therapy. Aliment. Pharmacol. Ther. 2015, 42, 477–483. [Google Scholar] [CrossRef]
- Sue, S.; Shibata, W.; Sasaki, T.; Kaneko, H.; Irie, K.; Kondo, M.; Maeda, S. Randomized Trial of Vonoprazan- Versus PPI-Based Third-Line Triple Therapy With Sitafloxacin for Helicobacter pylori. J. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef]
- Wang, D.; Guo, Y.; Wrighton, S.A.; Cooke, G.E.; Sadee, W. Intronic polymorphism in CYP3A4 affects hepatic expression and response to statin drugs. Pharmacogenomics J. 2011, 11, 274–286. [Google Scholar] [CrossRef]
- Hesselink, D.A.; Bouamar, R.; Elens, L.; van Schaik, R.H.; van Gelder, T. The role of pharmacogenetics in the disposition of and response to tacrolimus in solid organ transplantation. Clin. Pharmacokinet. 2014, 53, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Staatz, C.E.; Goodman, L.K.; Tett, S.E. Effect of CYP3A and ABCB1 single nucleotide polymorphisms on the pharmacokinetics and pharmacodynamics of calcineurin inhibitors: Part I. Clin. Pharmacokinet. 2010, 49, 141–175. [Google Scholar] [CrossRef] [PubMed]
- Asada, A.; Bamba, S.; Morita, Y.; Takahashi, K.; Imaeda, H.; Nishida, A.; Inatomi, O.; Sugimoto, M.; Sasaki, M.; Andoh, A. The effect of CYP3A5 genetic polymorphisms on adverse events in patients with ulcerative colitis treated with tacrolimus. Dig. Liver Dis. 2016. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).