In Vitro Activity of Pentamidine Alone and in Combination with Antibiotics against Multidrug-Resistant Clinical Pseudomonas aeruginosa Strains

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Results
2.1. MIC/MBC and Heteroresistance
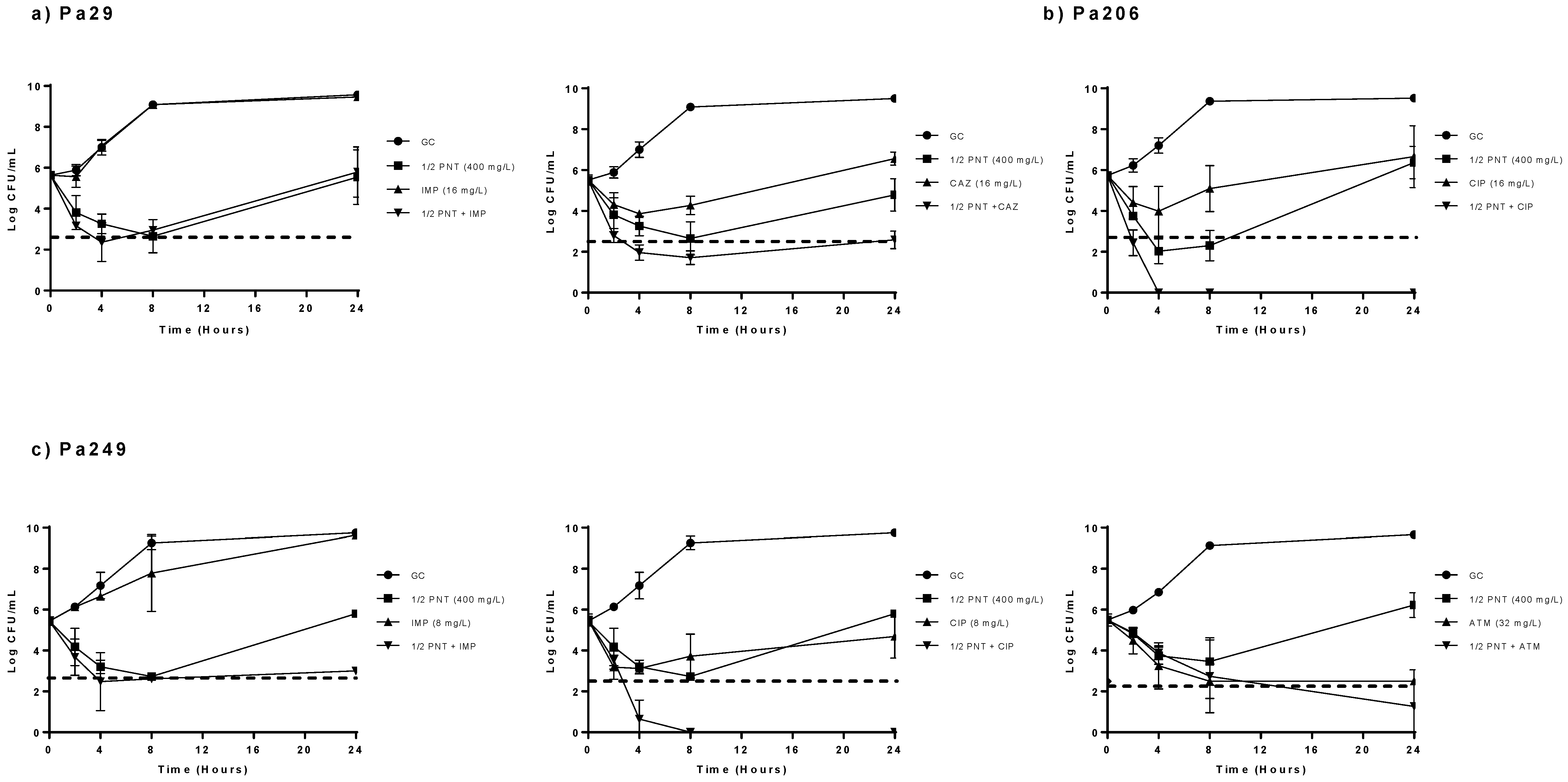
2.2. Time–Kill Curves
3. Discussion
4. Materials and Methods
4.1. Bacterial Isolates
4.2. Drugs
4.3. Antimicrobial Susceptibility Testing
4.4. Bactericidal Activity and Synergy Studies
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Botelho, J.; Grosso, F.; Peixe, L. Antibiotic resistance in Pseudomonas aeruginosa—Mechanisms, epidemiology and evolution. Drug Resist. Updates Rev. Comment. Antimicrob. Anticancer Chemother. 2019, 44, 100640. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Pham, D.T.N.; Oloketuyi, S.F.; Kim, Y.M. Regulation and controlling the motility properties of Pseudomonas aeruginosa. Appl. Microbiol. Biotechnol. 2020, 104, 33–49. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Yoshimura, K.; Yano, I.; Yamamoto, T.; Kawanishi, M.; Isomoto, Y.; Yonezawa, A.; Kondo, T.; Takaori-Kondo, A.; Matsubara, K. Population pharmacokinetics and pharmacodynamics of mycophenolic acid using the prospective data in patients undergoing hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Surveillance Report. Surveillance of Antimicrobial Resistance in Europe. 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/surveillance-antimicrobial-resistance-Europe-2018.pdf (accessed on 9 October 2020).
- Khodare, A.; Kale, P.; Pindi, G.; Joy, L.; Khillan, V. Incidence, Microbiological Profile, and Impact of Preventive Measures on Central Line-associated Bloodstream Infection in Liver Care Intensive Care Unit. Indian J. Crit. Care Med. Peer-Rev. Off. Publ. Indian Soc. Crit. Care Med. 2020, 24, 17–22. [Google Scholar] [CrossRef]
- Tabak, Y.P.; Merchant, S.; Ye, G.; Vankeepuram, L.; Gupta, V.; Kurtz, S.G.; Puzniak, L.A. Incremental clinical and economic burden of suspected respiratory infections due to multi-drug-resistant Pseudomonas aeruginosa in the United States. J. Hosp. Infect. 2019, 103, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.; Cerceo, E. Trends, Epidemiology, and Management of Multi-Drug Resistant Gram-Negative Bacterial Infections in the Hospitalized Setting. Antibiotics 2020, 9, 196. [Google Scholar] [CrossRef] [PubMed]
- Pang, Z.; Raudonis, R.; Glick, B.R.; Lin, T.J.; Cheng, Z. Antibiotic resistance in Pseudomonas aeruginosa: Mechanisms and alternative therapeutic strategies. Biotechnol. Adv. 2019, 37, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Miro-Canturri, A.; Ayerbe-Algaba, R.; Smani, Y. Drug Repurposing for the Treatment of Bacterial and Fungal Infections. Front. Microbiol. 2019, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- Brown, D. Antibiotic resistance breakers: Can repurposed drugs fill the antibiotic discovery void? Nat. Rev. Drug Discov. 2015, 14, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Rampioni, G.; Visca, P.; Leoni, L.; Imperi, F. Drug repurposing for antivirulence therapy against opportunistic bacterial pathogens. Emerg. Top. Life Sci. 2017, 1, 13–22. [Google Scholar] [CrossRef]
- Ayerbe-Algaba, R.; Gil-Marques, M.L.; Miro-Canturri, A.; Parra-Millan, R.; Pachon-Ibanez, M.E.; Jimenez-Mejias, M.E.; Pachon, J.; Smani, Y. The anthelmintic oxyclozanide restores the activity of colistin against colistin-resistant Gram-negative bacilli. Int. J. Antimicrob. Agents 2019, 54, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Cebrero-Cangueiro, T.; Alvarez-Marin, R.; Labrador-Herrera, G.; Smani, Y.; Cordero-Matia, E.; Pachon, J.; Pachon-Ibanez, M.E. In vitro Activity of Pentamidine Alone and in Combination With Aminoglycosides, Tigecycline, Rifampicin, and Doripenem Against Clinical Strains of Carbapenemase-Producing and/or Colistin-Resistant Enterobacteriaceae. Front. Cell. Infect. Microbiol. 2018, 8, 363. [Google Scholar] [CrossRef]
- Stokes, J.M.; MacNair, C.R.; Ilyas, B.; French, S.; Cote, J.P.; Bouwman, C.; Farha, M.A.; Sieron, A.O.; Whitfield, C.; Coombes, B.K.; et al. Pentamidine sensitizes Gram-negative pathogens to antibiotics and overcomes acquired colistin resistance. Nat. Microbiol. 2017, 2, 17028. [Google Scholar] [CrossRef] [PubMed]
- Adams, F.G.; Stroeher, U.H.; Hassan, K.A.; Marri, S.; Brown, M.H. Resistance to pentamidine is mediated by AdeAB, regulated by AdeRS, and influenced by growth conditions in Acinetobacter baumannii ATCC 17978. PLoS ONE 2018, 13, e0197412. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- 2019 First Generic Drug Approvals. Available online: https://www.fda.gov/drugs/first-generic-drug-approvals/2019-first-generic-drug-approvals (accessed on 9 October 2019).
- Maciejewska, D.; Żabiński, J.; Kaźmierczak, P.; Wójciuk, K.; Kruszewski, M.; Kruszewska, H. In vitro screening of pentamidine analogs against bacterial and fungal strains. Bioorg. Med. Chem. Lett. 2014, 24, 2918–2923. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Xia, L.; Huang, W.; Xu, Y.; Gu, Y.; Liu, C.; Ji, L.; Li, W.; Wu, Y.; Zhou, K.; et al. Pentamidine sensitizes FDA-approved non-antibiotics for the inhibition of multidrug-resistant Gram-negative pathogens. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1771–1779. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 29th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- EUCAST Breakpoint Tables for Interpretation of MICs and Zone Diameters Version 9.0. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_9.0_Breakpoint_Tables.pdf (accessed on 9 December 2020).
- Pachón-Ibáñez, M.E.; Labrador-Herrera, G.; Cebrero-Cangueiro, T.; Díaz, C.; Smani, Y.; Del Palacio, J.P.; Rodríguez-Baño, J.; Pascual, A.; Pachón, J.; Conejo, M.C. Efficacy of Colistin and Its Combination With Rifampin. Front. Microbiol. 2018, 9, 912. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinical Strains | MIC/MBC (mg/L) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PNT | AMK | GEN | TOB | IMP | MEM | ATM | CAZ | CIP | LFX | COL | |
| Pa29 | 800 | 1/2 | 1/1 | 0.25/0.25 | 16/16 | 32/32 | 16/64 | 16/32 | 0.50/4 | 1/1 | 0.13/1 |
| Pa194 | 400 | 16/16 | 16/>32 | 32/>32 | 64/64 | 32/>64 | 2/8 | 512/512 | 1/1 | 32/64 | 0.50/1 |
| Pa206 | 800 | 1/2 | 0.13/0.13 | 0.50/1 | 8/8 | 16/16 | 16/16 | 2/4 | 16/32 | 64/>64 | 0.13/0.13 |
| Pa215 | 1600 | 32/32 | 8/16 | 2/2 | 8/8 | 32/32 | 16/32 | 32/64 | 4/8 | 16/64 | 4/8 |
| Pa223 | 400 | 32/32 | 1/1 | 1/1 | 32/32 | 16/16 | 16/64 | 32/128 | 1/2 | 2/16 | <0.06/<0.06 |
| Pa249 | 800 | 2/2 | 0.13/0.13 | 0.13/0.25 | 8/8 | 16/32 | 32/32 | 8/8 | 8/16 | 32/64 | 0.25/0.5 |
| Pa302 | 400 | 2/4 | 1/2 | 0.25/0.5 | 8/8 | 2/4 | 8/32 | 1/4 | 0.5/1 | 2/8 | 2/8 |
| Clinical Strain | PNT | AMK | GEN | TOB | IMP | MEM | ATM | CAZ | CIP | LFX | COL |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pa29 | B (2–8) | - | - | - | NA | NA | - | NA | - | - | - |
| Pa194 | B (2–8) | NA | NA | B (2–8) | NA | B (8) | - | NA | NA | B (2–24) | - |
| Pa206 | B (2–24) | - | - | - | NA | NA | - | - | NA | B (8–24) | - |
| Pa215 | B (2–4) | B (8) | NA | - | NA | NA | - | NA | NA | NA | B (2–8) |
| Pa223 | NA | NA | - | - | NA | NA | - | NA | NA | NA | - |
| Pa249 | B (8) | - | - | - | NA | NA | B (8–24) | - | NA | B (2–24) | - |
| Pa302 | B (8–24) | - | - | - | NA | - | - | - | - | NA | - |
| Clinical Strain | PNT + AMK | PNT + GEN | PNT + TOB | PNT + IMP | PNT + MEM | PNT + ATM | PNT + CAZ | PNT + CIP | PNT + LFX | PNT + COL |
|---|---|---|---|---|---|---|---|---|---|---|
| Pa29 | - | - | - | B (2–24) S (24) | B (2–24) S (24) | - | B (4–24) | - | - | - |
| Pa194 | B (4–24) S (8–24) | B (2–8) S (8–24) | B (2–24) S (24) | B (2–24) S (24) | B (2–24) S (24) | - | B (2–24) S (24) | B (4–24) S (8–24) | B (2–24) | - |
| Pa206 | - | - | - | B (2–24) | B (8–24) S (24) | - | - | B (2–24) | B (2–24) | - |
| Pa215 | B (2–24) S (8–24) | B (2–24) S (8–24) | - | B (2–8) S (8) | B (2–24) | - | B (2–8) | B (2–24) S (2–24) | B (2–24) S (8–24) | B (2–8) |
| Pa223 | B (24) S (24) | - | - | B (2–24) S (8–24) | B (2–24) S (24) | B (4–24) S (24) | B (4–24) S (24) | B (4–24) S (24) | B (2–24) | - |
| Pa249 | - | - | - | B (2–24) S (2–24) | B (2–24) S (24) | B (8–24) | - | B (2–24) S (2–24) | B (2–24) S (2–24) | - |
| Pa302 | - | - | - | B (4–24) S (8) | - | - | - | - | B (8–24) S (24) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Espejo, S.; Cebrero-Cangueiro, T.; Labrador-Herrera, G.; Pachón, J.; Pachón-Ibáñez, M.E.; Álvarez-Marín, R. In Vitro Activity of Pentamidine Alone and in Combination with Antibiotics against Multidrug-Resistant Clinical Pseudomonas aeruginosa Strains. Antibiotics 2020, 9, 885. https://doi.org/10.3390/antibiotics9120885
Herrera-Espejo S, Cebrero-Cangueiro T, Labrador-Herrera G, Pachón J, Pachón-Ibáñez ME, Álvarez-Marín R. In Vitro Activity of Pentamidine Alone and in Combination with Antibiotics against Multidrug-Resistant Clinical Pseudomonas aeruginosa Strains. Antibiotics. 2020; 9(12):885. https://doi.org/10.3390/antibiotics9120885
Chicago/Turabian StyleHerrera-Espejo, Soraya, Tania Cebrero-Cangueiro, Gema Labrador-Herrera, Jerónimo Pachón, María Eugenia Pachón-Ibáñez, and Rocío Álvarez-Marín. 2020. "In Vitro Activity of Pentamidine Alone and in Combination with Antibiotics against Multidrug-Resistant Clinical Pseudomonas aeruginosa Strains" Antibiotics 9, no. 12: 885. https://doi.org/10.3390/antibiotics9120885
APA StyleHerrera-Espejo, S., Cebrero-Cangueiro, T., Labrador-Herrera, G., Pachón, J., Pachón-Ibáñez, M. E., & Álvarez-Marín, R. (2020). In Vitro Activity of Pentamidine Alone and in Combination with Antibiotics against Multidrug-Resistant Clinical Pseudomonas aeruginosa Strains. Antibiotics, 9(12), 885. https://doi.org/10.3390/antibiotics9120885