Validation of the American English Acute Cystitis Symptom Score


Abstract
:1. Introduction
2. Results
2.1. Linguistic Validation
2.2. Study Population of Clinical Validation
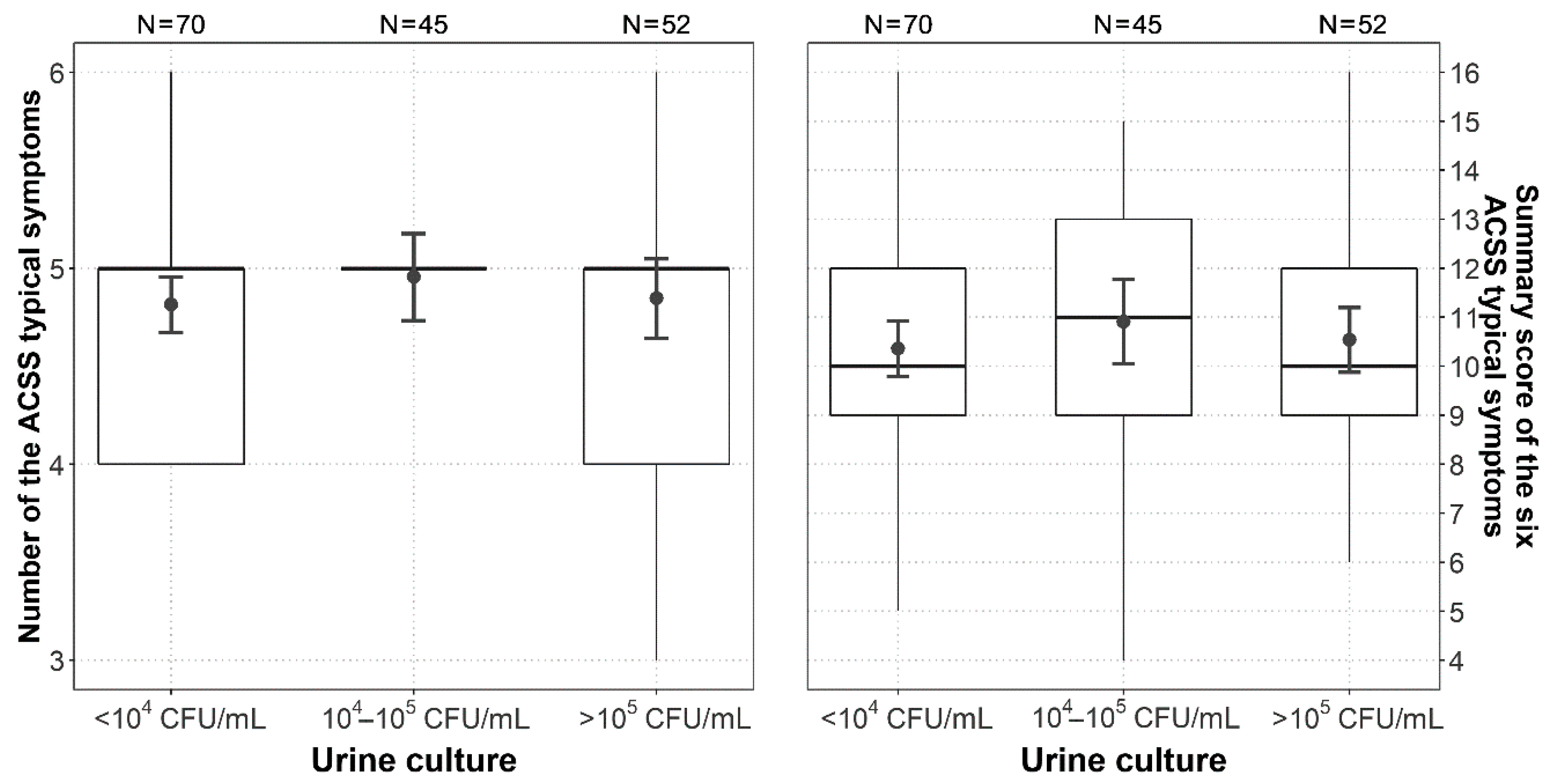
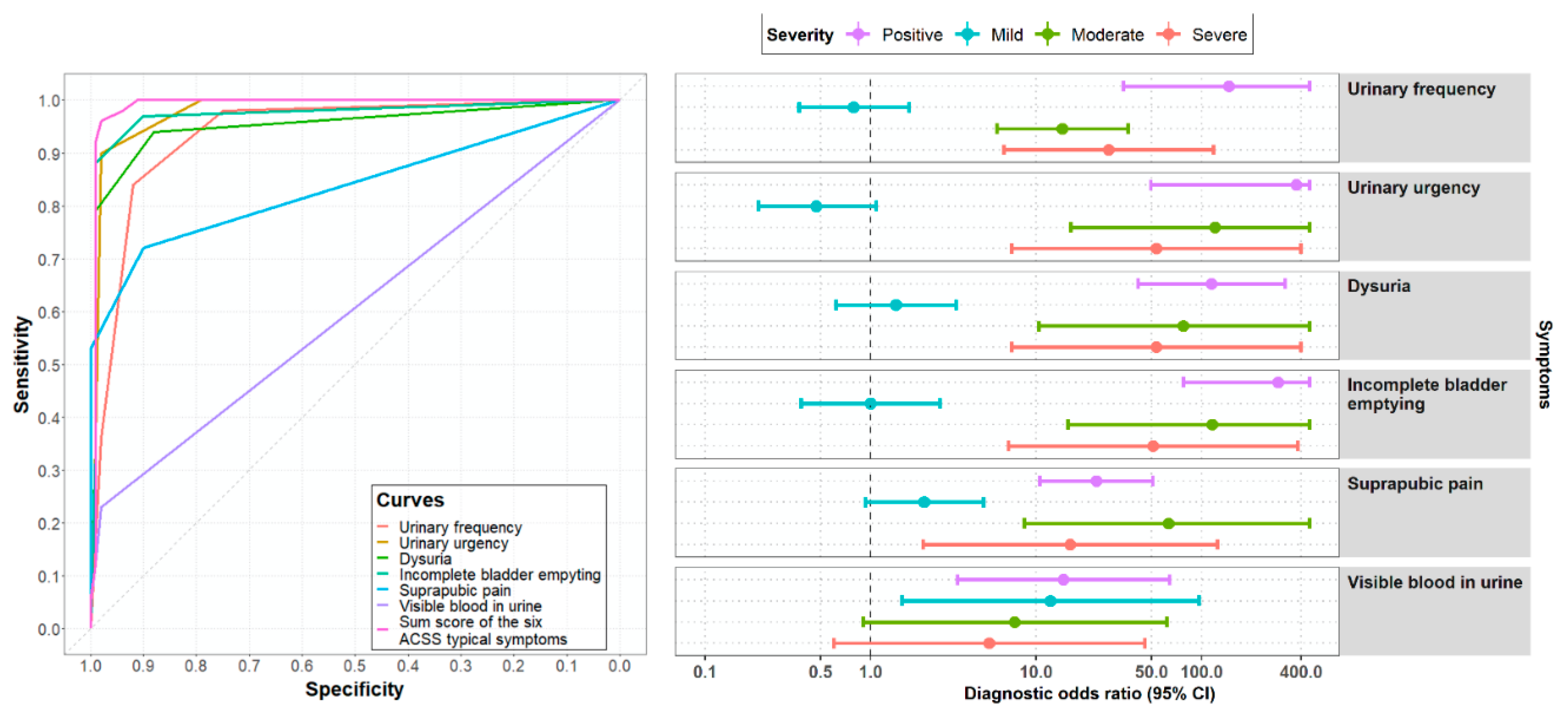
2.3. The ACSS in US Cohort at Day 1 (Diagnostics)
2.4. Comparison of the ACSS between the US and International Cohort at Day 1 (Diagnostics)
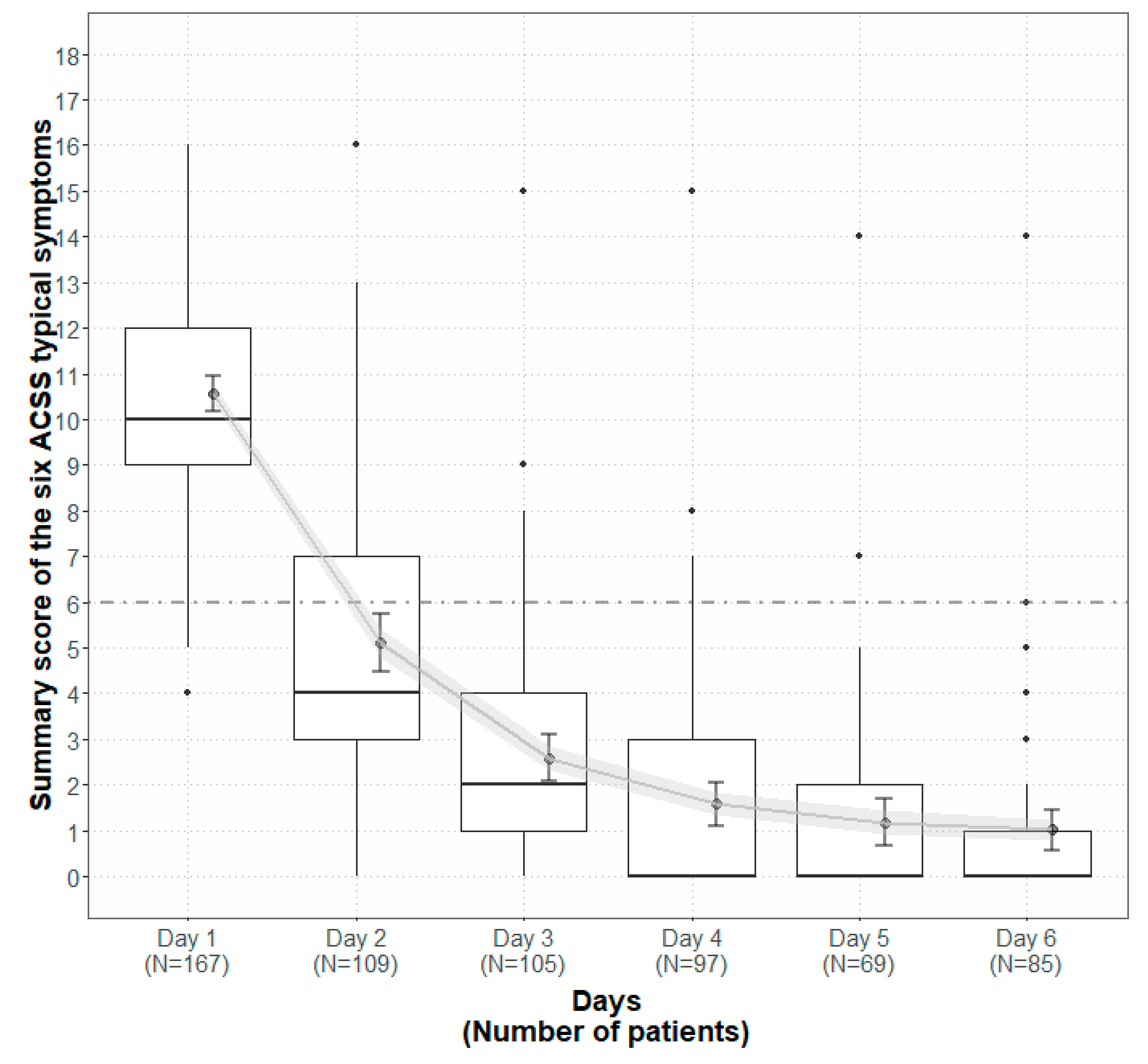
2.5. Patient-Reported Outcome Before, During and After Therapy
2.6. Comparison of Patient-Reported Outcome Between the US and the International Cohort
2.7. Validation of the American English ACSS Using Pre- and Posttreatment Results
3. Discussion
4. Material and Methods
4.1. Study Design
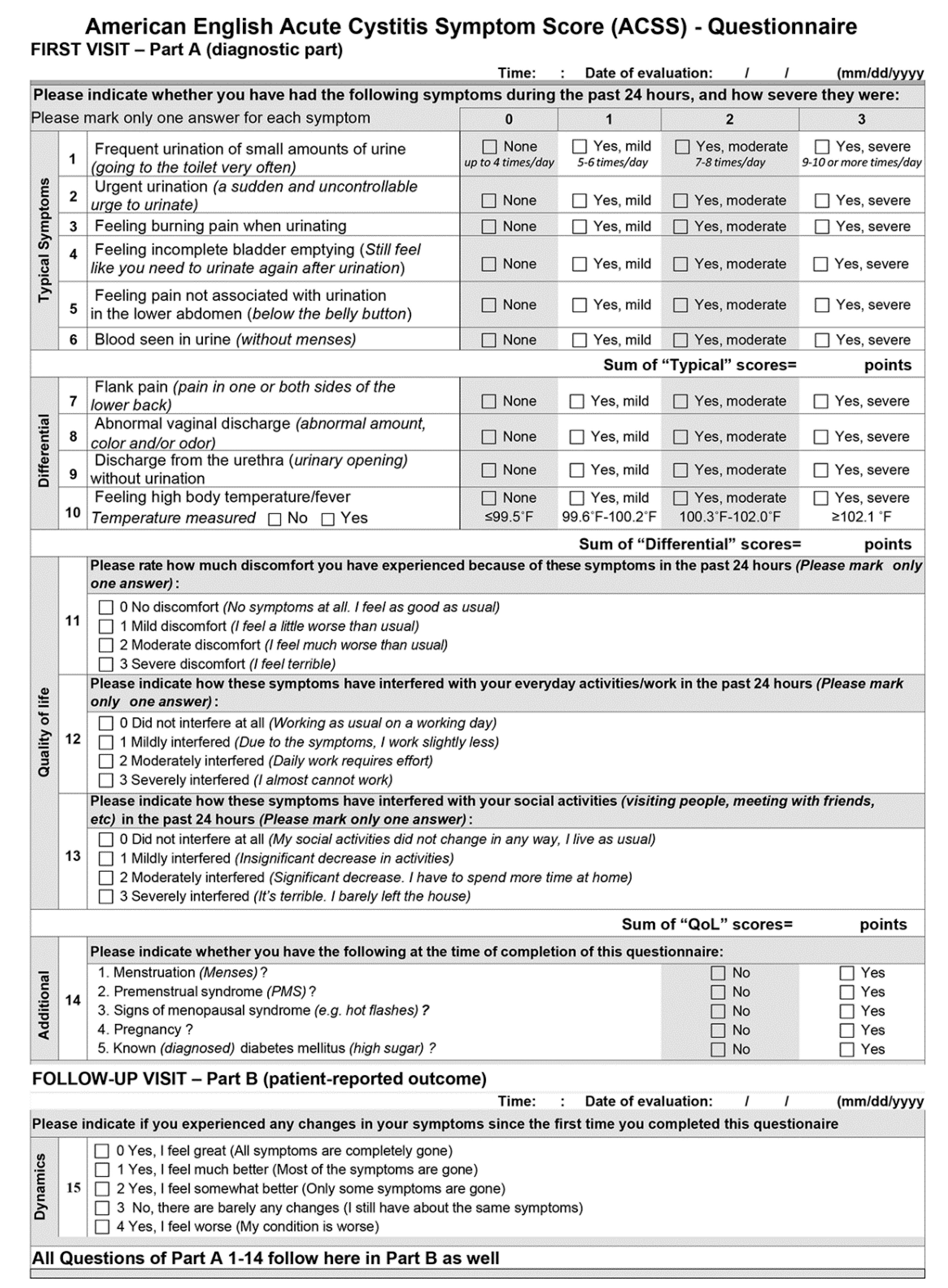
4.2. The ACSS as a Study Tool
- (i).
- Six questions about typical symptoms of UC (“Typical“ domain): urinary frequency, urinary urgency, dysuria, incomplete bladder emptying, suprapubic pain, visible blood in the urine.
- (ii).
- Four questions regarding differential diagnosis (“Differential“ domain): flank pain, abnormal vaginal discharge, urethral discharge, elevated body temperature/fever.
- (iii).
- Three questions on the quality of life (“QoL“ domain): general discomfort, interference with everyday activity/work, interference with social life.
- (iv).
- All questions of the domains i–iii are to be answered according to severity (scoring 0–3): no (0), mild (1), moderate (2), severe (3).
- (v).
- 5 questions on additional conditions, which may affect therapy (“Additional“ domain): menstruation, premenstrual syndrome, menopause, pregnancy, diabetes mellitus. The answers are yes or no.
- (vi).
- 5 questions on the patient’s assessment of overall symptomatic changes after the baseline visit (“Dynamics“ domain). The answers are rated (scored): Feeling normal (0), much better (1), somewhat better (2), barely any change (3), worse (4).
- (vii).
- Part A includes the domains i-iii, v (Typical, Differential, QoL, Additional) and Part B includes the domains vi (Dynamics) and i-iii, v as in Part A.
4.3. Linguistic Validation of the American English Version of the ACSS
4.4. Clinical Validation
4.5. Data Acquisition and Processing
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Copyright of the ACSS
Acknowledgments
Conflicts of Interest
Abbreviations
| ACSS | acute cystitis symptom score |
| AUC | area under the curve; |
| CFU | colony-forming units |
| CI | confidence interval |
| DOR | diagnostic odds ratio |
| EMA | European Medical Agency |
| EoT | end of treatment |
| FDA | Food and Drug Administration |
| IQR | interquartile range |
| +LR | positive likelihood ratio |
| -LR | negative likelihood ratio |
| N | number |
| NPV | negative predictive value; |
| PMS | premenstrual syndrome |
| PO | positive outcome (diagnosis is correct) |
| PPV | positive predictive value, |
| PRO | patient-reported outcome |
| p-value | probability value |
| Q | question of the ACSS |
| QID | four times a day |
| QoL | quality of life |
| ROC | Receiver operating characteristic |
| SC | scientific committee |
| SD | standard deviation |
| UC | uncomplicated cystitis |
| US | United States of America |
| UTI | urinary tract infection |
| VBU | visible blood in urine |
References
- Colgan, R.; Williams, M. Diagnosis and treatment of acute uncomplicated cystitis. Am. Fam. Physician 2011, 84, 771–776. [Google Scholar] [PubMed]
- Desforges, J.F.; Stamm, W.E.; Hooton, T.M. Management of urinary tract infections in adults. N. Engl. J. Med. 1993, 329, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Barry, H.C.; Ebell, M.H.; Hickner, J. Evaluation of suspected urinary tract infection in ambulatory women: A cost-utility analysis of office-based strategies. J. Fam. Pr. 1997, 44, 49–60. [Google Scholar] [CrossRef]
- Colgan, R.; Keating, K.; Dougouih, M. Survey of symptom burden in women with uncomplicated urinary tract infections. Clin. Drug Investig. 2004, 24, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Clayson, D.; Wild, D.; Doll, H.; Keating, K.; Gondek, K. Validation of a patient-administered questionnaire to measure the severity and bothersomeness of lower urinary tract symptoms in uncomplicated urinary tract infection (UTI): The UTI Symptom Assessment questionnaire. BJU Int. 2005, 96, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Clayson, D.J.; Keating, K.N.; Gondek, K. Validation of a patient-administered questionnaire to measure the activity impairment experienced by women with uncomplicated urinary tract infection: The Activity Impairment Assessment (AIA). Health Qual. Life Outcomes 2005, 3, 42. [Google Scholar] [CrossRef] [Green Version]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M. Reliability of Symptom-Based Diagnosis of Uncomplicated Cystitis. Urol. Int. 2018, 102, 83–95. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Abdufattaev, U.A.; Makhsudov, S.A.; Pilatz, A.; Akilov, F.A.; Naber, K.G.; Wagenlehner, F.M. New self-reporting questionnaire to assess urinary tract infections and differential diagnosis: Acute cystitis symptom score. Urol Int. 2014, 92, 230–236. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Radzhabov, A.; Zamuddinov, M.; Magyar, A.; Tenke, P.; Wagenlehner, F.M. Evaluation of the draft guidelines proposed by EMA and FDA for the clinical diagnosis of acute uncomplicated cystitis in women. World J. Urol. 2020, 38, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Radzhabov, A.; Zamuddinov, M.; Magyar, A.; Tenke, P.; Wagenlehner, F.M. Additional assessment of Acute Cystitis Symptom Score questionnaire for patient-reported outcome measure in female patients with acute uncomplicated cystitis: Part II. World J. Urol. 2020, 38, 1977–1988. [Google Scholar] [CrossRef] [Green Version]
- Food Drug Administration Center for Drugs Evaluation Research. Uncomplicated Urinary Tract Infections: Developing Drugs for Treatment: Guidance for Industry; U.S. Food and Drug Administration; Silver Spring: Maryland, MD, USA, 2019; p. 20. [Google Scholar]
- European Medicines Agency Committee for Human Medicinal Products. Evaluation of medicinal products indicated for treatment of bacterial infections. In Draft Guideline; European Medicines Agency Committee for Human Medicinal Products: Amsterdam, The Netherlands, 2018; p. 20. [Google Scholar]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Hurley, M.; Mohoney, C.M.; Barnes, B.D.; Werchan, P.; Wagenlehner, F. The American English Acute Cystitis Symptom Score—Linguistic Validation. In Proceedings of the 33rd Annual Congress of the European Association of Urology, Copenhagen, Denmark, 16–20 March 2018; European Association of Urology: Copenhagen, Denmark, 2018. [Google Scholar]
- Alidjanov, J.F.; Abdufattaev, U.A.; Makhmudov, D.; Mirkhamidov, D.; Khadzhikhanov, F.A.; Azgamov, A.V.; Pilatz, A.; Naber, K.; Wagenlehner, F.M.; Akilov, F.A. Development and clinical testing of the Russian version of the Acute Cystitis Symptom Score—ACSS. Urologiia 2014, 6, 14–22. [Google Scholar]
- Alidjanov, J.F.; Pilatz, A.; Abdufattaev, U.A.; Wiltink, J.; Weidner, W.; Naber, K.G.; Wagenlehner, F. German validation of the Acute Cystitis Symptom Score. Urologe A 2015, 54, 1269–1276. [Google Scholar] [CrossRef] [PubMed]
- Alidjanov, J.F. Preliminary Clinical Validation of the UK English Version of the Acute Cystitis Symptom Score in UK English-speaking female population of Newcastle, Great Britain. JOJ Urol. Nephrol. 2017, 1, 555561. [Google Scholar]
- Di Vico, T.; Morganti, R.; Cai, T.; Naber, K.G.; Wagenlehner, F.M.; Pilatz, A.; Alidjanov, J.F.; Morelli, G.; Bartoletti, R. Acute Cystitis Symptom Score (ACSS): Clinical Validation of the Italian Version. Antibiotics 2020, 9, 104. [Google Scholar] [CrossRef] [Green Version]
- Magyar, A.; Alidjanov, J.F.; Pilatz, A.; Nagy, K.; Arthanareeswaran, V.K.A.; Póth, S.; Bécsi, A.; Wagenlehner, F.M.; Naber, K.G.; Tenke, P.; et al. The role of the Acute Cystitis Symptom Score questionnaire for research and antimicrobial stewardship. Validation of the Hungarian version. Central Eur. J. Urol. 2017, 71, 134–141. [Google Scholar]
- Heytens, S.; De Sutter, A.; Coorevits, L.; Cools, P.; Boelens, J.; Van Simaey, L.; Christiaens, T.; Vaneechoutte, M.; Claeys, G. Women with symptoms of a urinary tract infection but a negative urine culture: PCR-based quantification of Escherichia coli suggests infection in most cases. Clin. Microbiol. Infect. 2017, 23, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Hooton, T.M.; Roberts, P.L.; Cox, M.E.; Stapleton, A.E. Voided midstream urine culture and acute cystitis in premenopausal women. N. Engl. J. Med. 2013, 369, 1883–1891. [Google Scholar] [CrossRef] [Green Version]
- Stamm, W.E.; Counts, G.W.; Running, K.R.; Fihn, S.; Turck, M.; Holmes, K.K. Diagnosis of coliform infection in acutely dysuric women. N. Engl. J. Med. 1982, 307, 463–468. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M. Reevaluation of the Acute Cystitis Symptom Score, a Self-Reporting Questionnaire. Part II. Patient-Reported Outcome Assessment. Antibioics 2018, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M.E. Reevaluation of the Acute Cystitis Symptom Score, a Self-Reporting Questionnaire. Part I Development, Diagnosis and Differential Diagnosis. Antibiotics 2018, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Acquadro, C. Linguistic Validation Manual for Patient-Reported Outcomes (PRO) Instruments; Mapi Research Institute: Lyon, France, 2004. [Google Scholar]
- Acquadro, C.; Conway, K.; Giroudet, C.; Mear, I. Linguistic Validation Manual for Health Outcome Assessments; Mapi Institute: Lyon, France, 2012. [Google Scholar]
- Acquadro, C.; Jambon, B.D.E.; Marquis, P. Language and translation issues. In Quality of Life and Pharmacoeconomics in Clinical Trials; Spilker, B., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1996; pp. 575–586. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2017. [Google Scholar]
- Robin, X.A.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Nunes, T.; Heuer, C.; Marshall, J.; Sanchez, J.; Thornton, R.; Reiczigel, J.; Robison-Cox, J.; Sebastiani, P.; Solymos, P.; et al. epiR: Tools for the Analysis of Epidemiological Data. 2017. Available online: https://cran.r-project.org/web/packages/epiR/index.html (accessed on 18 December 2020).
- Wickham, H. Tidyverse: Easily Install and Load the ‘Tidyverse’. 2017. Available online: https://cran.r-project.org/web/packages/tidyverse/index.html (accessed on 18 December 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| US Study Group | International Study Group | ||
|---|---|---|---|
| Patients | N (%) | N (%) | p1-value |
| Total | 167 (100%) | 237 (100%) | |
| Range age (years) | 17–87 | 17–87 | 0.072 |
| Mean age (SD) | 36.8 (15.3) | 34.6 (15.1) | |
| Median age (IQR) | 32 (25;46) | 30 (23;40) | |
| 18–32 years | 86 (51.5%) | 138 (58.2%) | 0.233 |
| 33–47 years | 43 (25.8%) | 50 (21.1%) | |
| 48–62 years | 21 (12.6%) | 28 (11.8%) | |
| >62 years | 17 (10.2%) | 19 (8.0%) | |
| NA | - | 2 (0.8%) | |
| p2-value | |||
| Menstruation | 19 (11.4%) | 25 (10.6%) | 0.943 |
| PMS | 8 (4.8%) | 20 (8.4% | 0.201 |
| Menopause | 11 (6.6%) | 19 (8.0%) | 0.676 |
| Pregnancy | 0 (0%) | 27 (11.4%) | <0.001 |
| Diabetes mellitus | 2 (1.2%) | 2 (0.8%) | 1.000 |
| ACSS | Total Patients (N = 167; 100%) | Symptom Severity (N, %) | |||||
|---|---|---|---|---|---|---|---|
| Do- main | Q | Symptoms | 0 None (N, %) | 1 Mild (N, %) | 2 Moderate (N, %) | 3 Severe (N, %) | 2 + 3 Mod + Sev (N, %) |
| Typical Symptoms | 1 | Urinary frequency | 3 (1.80%) | 18 (10.78%) | 82 (49.10%) | 64 (38.32%) | 146 (87.42%) |
| 2 | Urinary urgency | 1 (0.60%) | 16 (9.58%) | 90 (53.89%) | 60 (35.93%) | 150 (89.82%) | |
| 3 | Dysuria (burning pain when urinating) | 12 (7.19%) | 22 (13.17%) | 76 (45.51%) | 57 (34.13%) | 133 (79.64%) | |
| 4 | Incomplete bladder emptying | 3 (1.80%) | 17 (10.18%) | 96 (57.49%) | 51 (30.54%) | 147 (88.03%) | |
| 5 | Pain in lower abdomen (suprapubic pain) | 46 (27.54%) | 30 (17.96%) | 72 (43.11%) | 19 (11.38%) | 91 (54.49%) | |
| 6 | Visible blood in urine | 125 (74.85%) | 20 (11.98%) | 10 (5.99%) | 12 (7.19%) | 22 (13.18%) | |
| Differential Symptoms | 7 | Flank pain | 86 (51.50%) | 30 (17.96%) | 38 (22.75%) | 13 (7.78%) | 51 (30.53%) |
| 8 | Abnormal vaginal discharge | 106 (63.47%) | 38 (22.75%) | 18 (10.78%) | 5 (2.99%) | 23 (13.77%) | |
| 9 | Discharge from the urethra | 125 (74.85%) | 30 (17.96%) | 12 (7.19%) | 0 (0.00%) | 12 (7.19%) | |
| 10 | High body temperature/fever | 157 (94.01%) | 9 (5.39%) | 1 (0.60%) | 0 (0.00%) | 1 (0.60%) | |
| Quality of Life | 11 | Discomfort because of symptoms | 9 (5.39%) | 27 (16.17%) | 83 (49.70%) | 48 (28.74%) | 131 (78.44%) |
| 12 | Interference with everyday activities/work | 14 (8.38%) | 47 (28.14%) | 72 (43.11%) | 34 (20.36%) | 106 (63.47%) | |
| 13 | Interference with social activities | 26 (15.57%) | 43 (25.75%) | 70 (41.92%) | 28 (16.77%) | 98 (58.69%) | |
| US Group | International Group | ||||
|---|---|---|---|---|---|
| ACSS | Patients | Sum Score | Patients | Sum Score | |
| Domain | N (Total) | Mean (SD) | N (Total) | Mean (SD) | p-Value * |
| Typical | 167 | 10.60 (2.51) | 237 | 10.12 (3.76) | 0.155 |
| Differential | 167 | 1.79 (1.81) | 237 | 2.39 (2.05) | 0.003 |
| QoL | 167 | 5.37 (2.34) | 237 | 5.58 (1.92) | 0.443 |
| ACSS total | 167 | 17.72 (5.0) | 237 | 18.08 (5.99) | 0.314 |
| Day 1 (Diagnostics) | Day 5/6 (End of Therapy) | |||||||
|---|---|---|---|---|---|---|---|---|
| ACSS | Patients | Sum Score | Patients | Sum Score | ||||
| Domain | N (total) | Mean (SD) | Median (IQR) | N (total) | Mean (SD) | Median (IQR) | p-value | |
| Typical | Total | 100 | 10.49 (2.60) | 10 (9;12) | 100 | 0.98 (1.94) | 0 (0;1) | <0.001 |
| <104 CFU/mL | 43 | 10.53 (2.59) | 11 (9;12.5) | 43 | 1.49 (2.60) | 0 (0;2) | <0.001 | |
| 104 CFU/mL | 29 | 10.66 (2.93) | 11 (9;13) | 29 | 0.48 (1.12) | 0 (0:0) | <0.001 | |
| >105 CFU/mL | 28 | 10.25 (2.29) | 10 (9;12) | 28 | 0.71 (1.12) | 0 (0;1.3) | <0.001 | |
| Differential | 100 | 1.57 (1.74) | 1 (0;3) | 100 | 0.34 (0.62) | 0 (0;1) | <0.001 | |
| QoL | 100 | 5.48 (2.46) | 6 (4;7) | 100 | 0.46 (0.93) | 0 (0;0) | <0.001 | |
| ACSS total | 100 | 17.54 (5.30) | 17 (14;22) | 100 | 1.78 (2.82) | 0 (0;2) | <0.001 | |
| Day 1 (Diagnostics) | Day 5/6 (End of Therapy) | 0 + 1 vs. 2 + 3 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACSS | Total | Symptom Severity | Total | Symptom Severity | |||||||||||
| Do- main | Q | N (100%) | 0 None (N,%) | 1 Mild (N,%) | 2 Moderate (N,%) | 3 Severe (N,%) | 2 + 3 Mod/Sev (N,%) | N (100%) | 0 None (N,%) | 1 Mild (N,%) | 2 Moderate (N,%) | 3 Severe (N,%) | 2 + 3 Mod/Sev (N,%) | p1-value | p2-value |
| Typical Symptoms | 1 | 100 | 2 | 14 | 48 | 36 | 84 | 100 | 75 | 17 | 6 | 2 | 8 | <0.001 | <0.001 |
| 2 | 100 | 0 | 10 | 55 | 35 | 90 | 100 | 79 | 19 | 1 | 1 | 2 | <0.001 | <0.001 | |
| 3 | 100 | 6 | 15 | 44 | 35 | 79 | 100 | 88 | 11 | 0 | 1 | 1 | <0.001 | <0.001 | |
| 4 | 100 | 3 | 9 | 54 | 34 | 88 | 100 | 90 | 9 | 0 | 1 | 1 | <0.001 | <0.001 | |
| 5 | 100 | 28 | 19 | 39 | 14 | 53 | 100 | 90 | 10 | 0 | 0 | 0 | <0.001 | <0.001 | |
| 6 | 100 | 77 | 11 | 7 | 5 | 12 | 100 | 98 | 1 | 1 | 0 | 1 | <0.001 | 0.002 | |
| Differential Symptoms | 7 | 100 | 54 | 21 | 18 | 7 | 25 | 200 | 85 | 13 | 2 | 0 | 2 | <0.001 | <0.001 |
| 8 | 100 | 71 | 16 | 10 | 3 | 13 | 100 | 90 | 9 | 1 | 0 | 1 | <0.001 | 0.001 | |
| 9 | 100 | 78 | 16 | 6 | 0 | 6 | 100 | 95 | 5 | 0 | 0 | 0 | <0.001 | 0.014 | |
| 10 | 100 | 88 | 12 | 0 | 0 | 0 | 100 | 96 | 4 | 0 | 0 | 0 | 0.024 | NA | |
| Quality of Life | 11 | 100 | 7 | 11 | 48 | 34 | 82 | 100 | 76 | 23 | 1 | 0 | 1 | <0.001 | <0.001 |
| 12 | 100 | 10 | 26 | 41 | 23 | 64 | 100 | 89 | 11 | 0 | 0 | 0 | <0.001 | <0.001 | |
| 13 | 100 | 15 | 24 | 45 | 16 | 61 | 100 | 90 | 10 | 0 | 0 | 0 | <0.001 | <0.001 | |
| Dyna- mics | Grading of “Dynamics“ | ||||||||||||||
| 0 | 1 | 2 | 3 | 4 | |||||||||||
| 100 | 64 | 27 | 7 | 2 | 0 | ||||||||||
| Type | Thresholds for Clinical Success | American English | International |
|---|---|---|---|
| A | Sum score of typical domain ≤5 scores, no item >1 | 91 (91%) | 66 (80.49%) |
| B | Sum score of typical domain ≤5 scores, no item >1 and no item of QoL >1 | 91 (91%) | 60 (73.17%) |
| C | Dynamics, no item >1 | 91 (91%) | 64 (78.05%) |
| D | Sum score of the 4 FDA symptoms ≤4, no item >1 | 91 (91%) | 66 (80.49%) |
| E | Sum score of the 3 EMA symptoms ≤3, no item>1 | 91 (91%) | 67 (81.71%) |
| Criteria | N (%) Positive | N (%) Negative | Sensitivity | Specificity | PPV | NPV | +LR | −LR | AUC | Correlation with PO |
|---|---|---|---|---|---|---|---|---|---|---|
| ACSS: typical domain, sumscore ≥6 | 96 (96%) | 2 (2%) | 0.96 (0.90–0.99) | 0.98 (0.93–1.00) | 0.98 (0.92–1.00) | 0.96 (0.90–0.99) | 48.00 (12.17–189.38) | 0.04 (0.02–0.11) | 0.97 (0.95–0.99) | 0.94 (0.92–0.95) |
| ACSS: main symptoms, sumscore ≥6 | 77 (77%) | 1 (1%) | 0.77 (0.68–0.85) | 0.99 (0.95–1.00) | 0.99 (0.93–1.00) | 0.81 (0.73–0.88) | 77.00 (10.92–542.88) | 0.23 (0.16–0.33) | 0.88 (0.84–0.92) | 0.78 (0.72–0.83) |
| FDA: at least 2 positive symptom of 4 | 100 (100%) | 33 (33%) | 1.00 (0.96–1.00) | 0.67 (0.57–0.76) | 0.75 (0.67–0.82) | 1.00 (0.95–1.00) | 3.03 (2.29–4.01) | 0.00 (0.00-NA) | 0.84 (0.79–0.88) | 0.71 (0.63–0.77) |
| EMA: at least 1 positive symptom of 3 | 100 (100%) | 22 (22%) | 1.00 (0.96–1.00) | 0.78 (0.69–0.86) | 0.82 (0.74–0.88) | 1.00 (0.95–1.00) | 4.55 (3.14–6.57) | 0.00 (0.00-NA) | 0.89 (0.85–0.93) | 0.80 (0.74–0.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Wagenlehner, F.M. Validation of the American English Acute Cystitis Symptom Score. Antibiotics 2020, 9, 929. https://doi.org/10.3390/antibiotics9120929
Alidjanov JF, Naber KG, Pilatz A, Wagenlehner FM. Validation of the American English Acute Cystitis Symptom Score. Antibiotics. 2020; 9(12):929. https://doi.org/10.3390/antibiotics9120929
Chicago/Turabian StyleAlidjanov, Jakhongir F., Kurt G. Naber, Adrian Pilatz, and Florian M. Wagenlehner. 2020. "Validation of the American English Acute Cystitis Symptom Score" Antibiotics 9, no. 12: 929. https://doi.org/10.3390/antibiotics9120929