Impact of Antimicrobial Stewardship Interventions on Appropriateness of Surgical Antibiotic Prophylaxis: How to Improve

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
- -
- “Shifting the responsibility of SAP administration to the anaesthesiologist”.
- -
- “Audit and feedback”.
- -
- “Education/training”.
- -
- “Implementation of standardized order form”.
- -
- “Implementation of a multidisciplinary management team”.
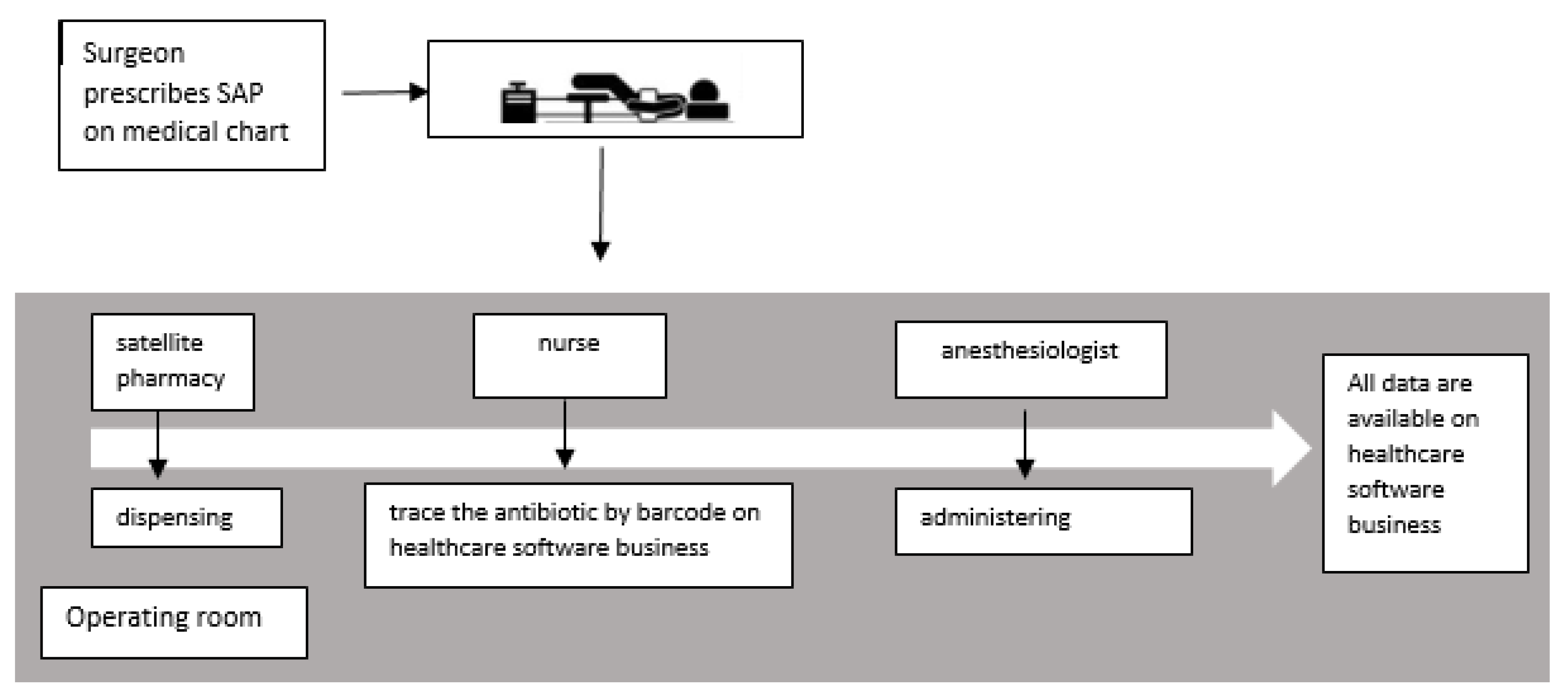
- The responsibility of SAP administration was shifted to the anaesthesiologists;
- Audits with feedback on appropriateness of prescription were performed every six months;
- Medical grand rounds were performed to promote the excellence and quality in Surgical Antibiotic Prophylaxis;
- The synergism with pharmacists permitted the organization of an operative block satellite pharmacy for antibiotic prophylaxis; and
- All the actions were performed by a multidisciplinary team.
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ban, K.A.; Minei, J.P.; Laronga, C.; Harbrecht, B.G.; Jensen, E.H.; Fry, D.E.; Itani, K.M.; Dellinger, E.P.; Ko, C.Y.; Duane, T.M. American College of Surgeons and Surgical Infection Society: Surgical Site Infection Guidelines, 2016 Update. J. Am. Coll. Surg. 2017, 224, 59–74. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Point Prevalence Survey of Health-caRe Associated Infections and Antimicrobial Use in European Acute Care Hospitals; ECDC: Stockholm, Sweden, 2013. [Google Scholar]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Burden of AMR Collaborative Group. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Badia, J.M.; Casey, A.L.; Petrosillo, N.; Crosby, C.; Hudson, P.; Mitchell, S. Impact of surgical site infection on healthcare costs and patient outcomes: A systematic review in six European countries. J. Hosp. Infect. 2017, 96, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, F.G. Efficacy of prophylactic antibiotic therapy in spinal surgery: A meta-analysis. Neurosurgery 2002, 51, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.; Lacerda, R.A.; Turrini, R.N.T.; Padoveze, M.C. Improving compliance with surgical antibiotic prophylaxis guidelines: A multicenter evaluation. Am. J. Infect. Control 2017, 45, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Askarian, M.; Moraweji, A.R.; Mirkhani, H.; Namazi, S.; Weed, H. Adherence to American Society of Health-System Pharmacists Surgical Antibiotic Prophylaxis Guidelines in Iran. Infect. Control Hosp. Epidemiol. 2006, 27, 876–878. [Google Scholar] [CrossRef]
- Van Disseldorp, J.; Slingenberg, E.J.M.H.; Matute, A.; Delgado, E.; Hak, E.; Hoepelman, I.M. Application of guidelines on preoperative antibiotic prophylaxis in León, Nicaragua. Neth. J. Med. 2006, 64, 411–416. [Google Scholar]
- Van Kasteren, M.E.E.; Mannien, J.; Kullberg, B.-J.; De Boer, A.S.; Nagelkerke, N.J.; Ridderhof, M.; Wille, J.C.; Gyssens, I.C. Quality improvement of surgical prophylaxis in Dutch hospitals: Evaluation of a multi-site intervention by time series analysis. J. Antimicrob. Chemother. 2005, 56, 1094–1102. [Google Scholar] [CrossRef]
- Abdel-Aziz, A.; El-Menyar, A.; Al-Thani, H.; Zarour, A.; Parchani, A.; Asim, M.; El-Enany, R.; Al-Tamimi, H.; Latifi, R. Adherence of Surgeons to Antimicrobial Prophylaxis Guidelines in a Tertiary General Hospital in a Rapidly Developing Country. Adv. Pharmacol. Sci. 2013, 2013, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ruscelli, P.; Renzi, C.; Polistena, A.; Sanguinetti, A.; Avenia, N.; Popivanov, G.; Cirocchi, R.; Lancia, M.; Gioia, S.; Tabola, R. Clinical signs of retroperitoneal abscess from colonic perforation. Medicine 2018, 97, e13176. [Google Scholar] [CrossRef]
- SNLG17. Antibioticoprofilassi perioperatoria nell’adulto LINEA GUIDA. In Data di Pubblicazione: Settembre 2008 Data di Aggiornamento: Settembre; Istituto Superiore di Sanità: Roma, Italy, 2011. [Google Scholar]
- Berríos-Torres, S.I.; Umscheid, C.A.; Bratzle, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017, 152, 784. [Google Scholar] [CrossRef] [PubMed]
- Scottish Intercollegiate Guidelines Network. Antibiotic Prophylaxis in Surgery; July 2008, updated April 2014; Healthcare Improvement Scotland: Edinburgh, Scotland, 2014. [Google Scholar]
- Plachouras, D.; Kärki, T.; Hansen, S.; Hopkins, S.; Lyytikäinen, O.; Moro, M.L.; Reilly, J.; Zarb, P.; Zingg, W.; Kinross, P.; et al. Antimicrobial use in European acute care hospitals: Results from the second point prevalence survey (PPS) of healthcare-associated infections and antimicrobial use, 2016 to 2017. Eurosurveillance 2018, 23, 1800393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dipartimento Scienze della Salute Pubblica e Pediatriche, Universit a di Torino. Secondo Studio di Prevalenza Italiano sulle Infezioni Correlate All’assistenza e sull’uso di Antibiotici negli Ospedali per Acuti—Protocollo ECDC [Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in Acute Care Hospitals]. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2791_allegato.pdf (accessed on 11 February 2019).
- Sartelli, M.; Labricciosa, F.M.; Barbadoro, P.; Pagani, L.; Ansaloni, L.; Brink, A.; Carlet, J.; Khanna, A.K.; Chichom-Mefire, A.; Coccolini, F.; et al. The Global Alliance for Infections in Surgery: Defining a model for antimicrobial stewardship-results from an international cross-sectional survey. World J. Emerg. Surg. 2017, 12, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goff, D.A.; Goldstein, E.J.C.; Gilchrist, M.; Nathwani, D.; Cheng, A.; Cairns, K.; Villegas, M.V.; Brink, A.; Mendelson, M.; Escandón-Vargas, K.; et al. A global call from five countries to collaborate in antibiotic stewardship: United we succeed, divided we might fail. Lancet Infect. Dis. 2017, 17, e56–e63. [Google Scholar] [CrossRef] [Green Version]
- Procedura Aziendale per la Prevenzione delle Infezioni del sito Chirurgico e Antibioticoprofilassi Perioperatoria nell’ Adulto. Available online: http://albo.aospterni.it/trasparenza_atti/portaldata/albo_files/2678_delibera_1287_2017.pdf (accessed on 29 December 2017).
- Rodríguez-Caravaca, G.; Gil-Yonte, P.; Risco-Risco, C.; Zamalloa, P.L.; Del Campo, M.C.V.; Cebrián, J.M.F.; Valverde-Núñez, I.; Lucendo, A.J. Antibiotic prophylaxis in elective cholecystectomy: Protocol adequacy and related outcomes in a retrospective single-centre analysis. Rev. Española de Enferm. Dig. 2016, 108, 15–19. [Google Scholar] [CrossRef] [Green Version]
- García, C.M.; Urbón, J.M.G.; Sanz, C.P.; Herranz, M.I.M. Auditing and Improving Surgical Antibiotic Prophylaxis. Surg. Infect. 2018, 19, 679–683. [Google Scholar] [CrossRef]
- World Health Organization. Global Guidelines for the Prevention of Surgical Site Infection; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Bratzle, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery. Surg. Infect. 2013, 14, 73–156. [Google Scholar] [CrossRef]
- De Jonge, S.W.; Gans, S.L.; Atema, J.J.; Solomkin, J.S.; Dellinger, P.E.; Boermeester, M. Timing of preoperative antibiotic prophylaxis in 54,552 patients and the risk of surgical site infection. Medicine 2017, 96, e6903. [Google Scholar] [CrossRef]
- Steinberg, J.P.; Braun, B.I.; Hellinger, W.C.; Kusek, L.; Bozikis, M.R.; Bush, A.J.; Dellinger, E.P.; Burke, J.P.; Simmons, B.; Kritchevsky, S. Timing of Antimicrobial Prophylaxis and the Risk of Surgical Site Infections. Ann. Surg. 2009, 250, 10–16. [Google Scholar] [CrossRef]
- Bertschi, D.; Weber, W.P.; Zeindler, J.; Stekhoven, D.; Mechera, R.; Salm, L.; Kralijevic, M.; Soysal, S.D.; Von Strauss, M.; Mujagic, E.; et al. Antimicrobial Prophylaxis Redosing Reduces Surgical Site Infection Risk in Prolonged Duration Surgery Irrespective of Its Timing. World J. Surg. 2019, 43, 2420–2425. [Google Scholar] [CrossRef]
- O’Sullivan, C.T.; Rogers, W.; Ackman, M.; Goto, M.; Hoff, B. Implementation of a multifaceted program to sustainably improve appropriate intraoperative antibiotic redosing. Am. J. Infect. Control. 2019, 47, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, B.; Van Assen, S.; Friedrich, A.W. Important issues for perioperative systemic antimicrobial prophylaxis in surgery. Curr. Opin. Anaesthesiol. 2014, 27, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Ansari, F.; Erntell, M.; Goossens, H.; Davey, P.; ESAC II Hospital Care Study Group. The European Surveillance of Antimicrobial Consumption (ESAC) Point-Prevalence Survey of Antibacterial Use in 20 European Hospitals in 2006. Clin. Infect. Dis. 2009, 49, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Robert, J.; Péan, Y.; Varon, E.; Bru, J.-P.; Bédos, J.P.; Bertrand, X.; Lepape, A.; Stahl, J.-P.; Gauzit, R. Point prevalence survey of antibiotic use in French hospitals in 2009. J. Antimicrob. Chemother. 2012, 67, 1020–1026. [Google Scholar] [CrossRef] [Green Version]
- Slimings, C.; Riley, T.V. Antibiotics and hospital-acquired Clostridium difficile infection: Update of systematic review and meta-analysis. J. Antimicrob. Chemother. 2013, 69, 881–891. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Drug | Dose (Adult) | Half-Life |
|---|---|---|
| Cefoxitin | >50 kg 2 g IV <50 kg 1 g IV | 1 h |
| Cefazolin | >50 kg 2 g IV <50 kg 1 g IV | 1.2–2.2 h |
| Cefuroxime | 2 g IV | 1 h |
| Clindamycin | 600 mg IV | 3 h |
| Gentamicin | 3 mg/kg IV | 1–2 h |
| Vancomycin | 15 mg/kg IV Max dose 1 G | 4–6 h |
| Doxycycline | 200 mg os before surgery (induced abortion) | 6–12 h |
| Metronidazole | 500 mg IV | 8 h |
| January–June 2018 | July–December 2018 | p-Value | |
|---|---|---|---|
| Elective surgical procedures | 2059 | 1781 | |
| Appropriate indication | 73.6% (1516/2059) | 77.8% (1386/1781) | 0.00128 |
| Appropriate antibiotic choice | 78.4% (1188/1516) | 78.4% (1087/1386) | 0.4863 |
| Appropriate dose | 69.7% (828/1188) | 83.8% (911/1087) | <2.2 × 10−16 |
| Overall compliance | 40.2% (828/2059) | 51.1% (911/1781) | <5.6 × 10−12 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiri, B.; Bruzzone, P.; Priante, G.; Sensi, E.; Costantini, M.; Vernelli, C.; Martella, L.A.; Francucci, M.; Andreani, P.; Mariottini, A.; et al. Impact of Antimicrobial Stewardship Interventions on Appropriateness of Surgical Antibiotic Prophylaxis: How to Improve. Antibiotics 2020, 9, 168. https://doi.org/10.3390/antibiotics9040168
Tiri B, Bruzzone P, Priante G, Sensi E, Costantini M, Vernelli C, Martella LA, Francucci M, Andreani P, Mariottini A, et al. Impact of Antimicrobial Stewardship Interventions on Appropriateness of Surgical Antibiotic Prophylaxis: How to Improve. Antibiotics. 2020; 9(4):168. https://doi.org/10.3390/antibiotics9040168
Chicago/Turabian StyleTiri, Beatrice, Paolo Bruzzone, Giulia Priante, Emanuela Sensi, Monya Costantini, Carlo Vernelli, Lucia Assunta Martella, Marsilio Francucci, Paolo Andreani, Alessandro Mariottini, and et al. 2020. "Impact of Antimicrobial Stewardship Interventions on Appropriateness of Surgical Antibiotic Prophylaxis: How to Improve" Antibiotics 9, no. 4: 168. https://doi.org/10.3390/antibiotics9040168
APA StyleTiri, B., Bruzzone, P., Priante, G., Sensi, E., Costantini, M., Vernelli, C., Martella, L. A., Francucci, M., Andreani, P., Mariottini, A., Capotorti, A., D’Andrea, V., Francisci, D., Cirocchi, R., & Cappanera, S. (2020). Impact of Antimicrobial Stewardship Interventions on Appropriateness of Surgical Antibiotic Prophylaxis: How to Improve. Antibiotics, 9(4), 168. https://doi.org/10.3390/antibiotics9040168