Impact of Reappraisal of Fluoroquinolone Minimum Inhibitory Concentration Susceptibility Breakpoints in Gram-Negative Bloodstream Isolates

 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
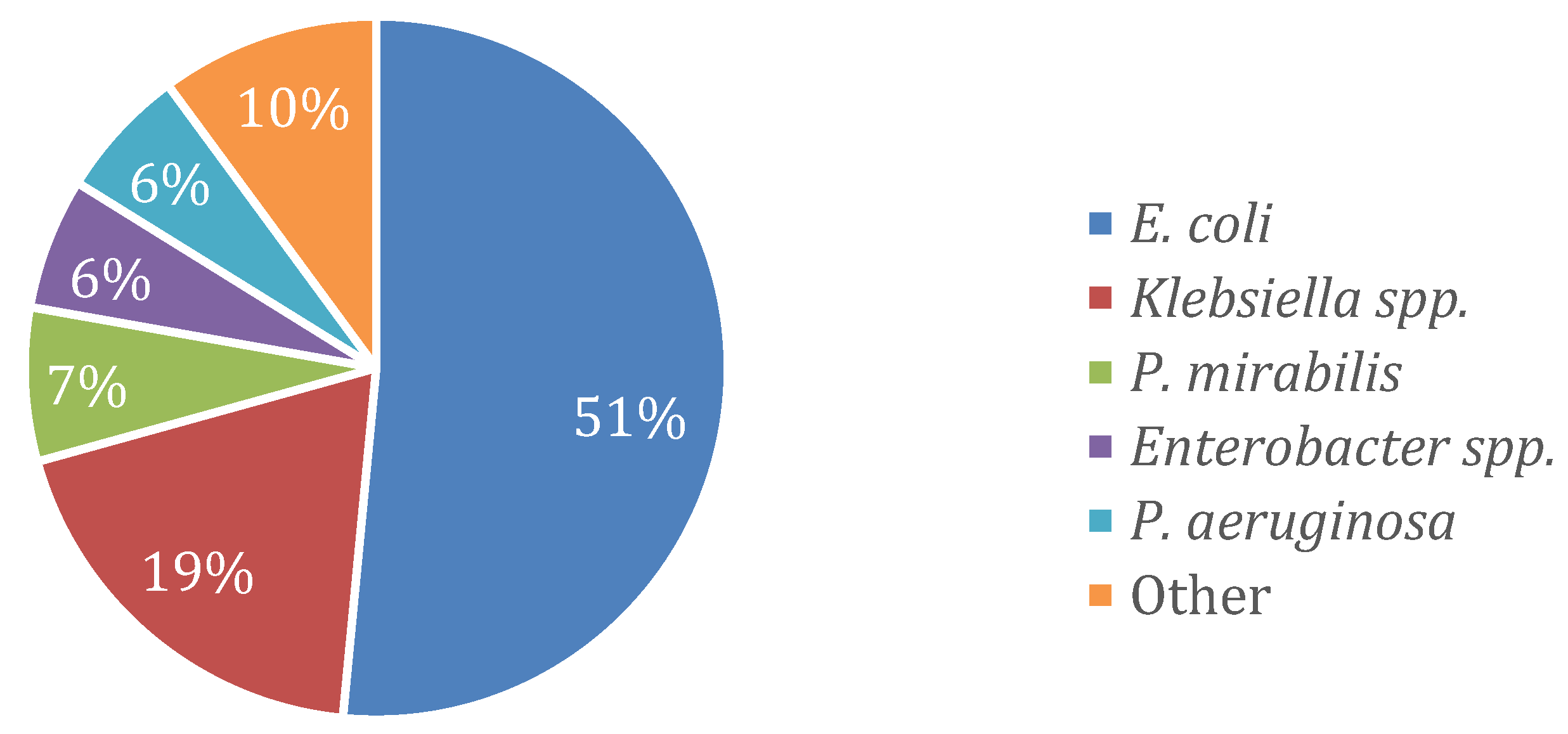
2.1. Microbiology
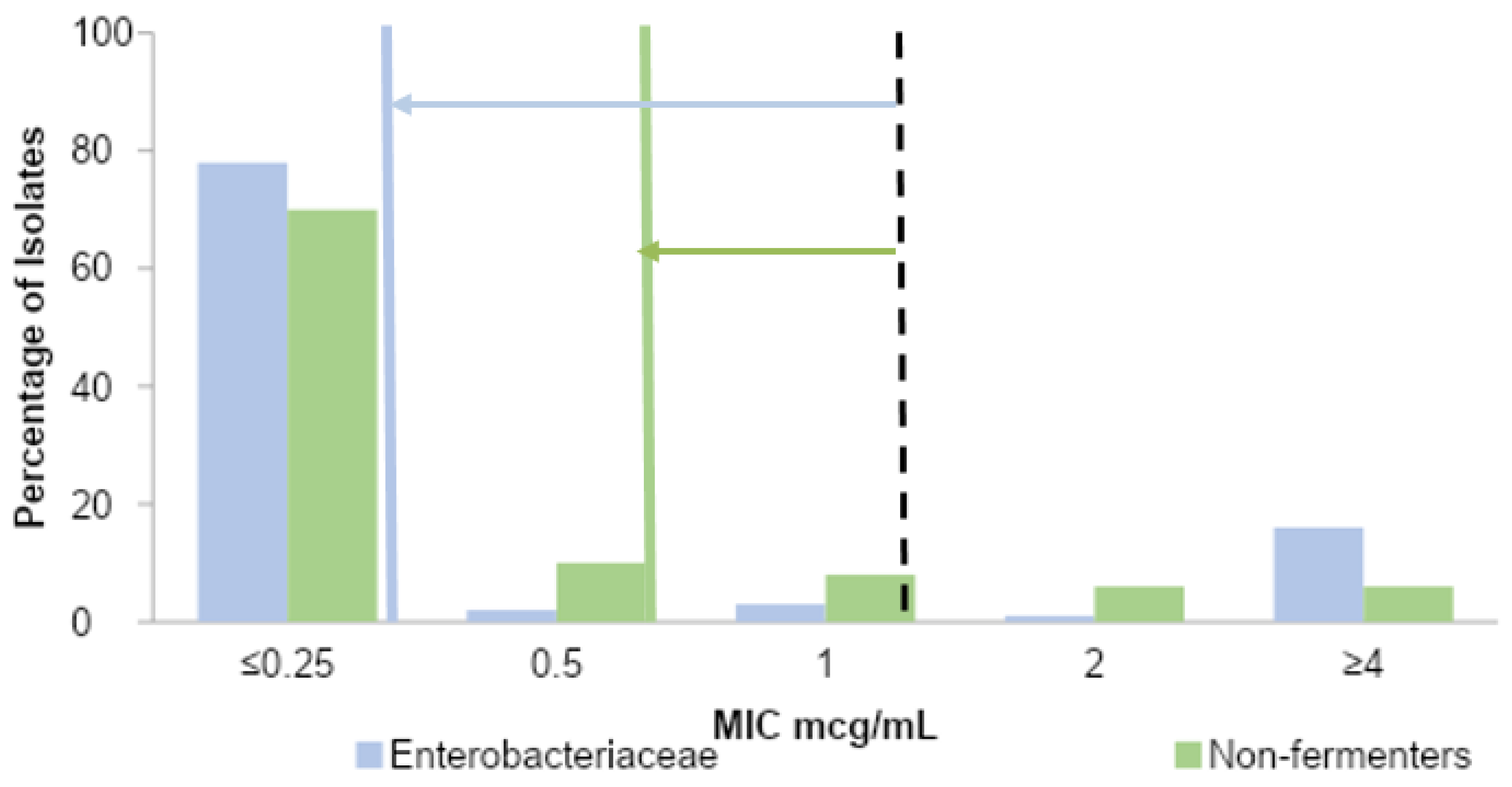
2.2. MIC Distribution by Organism
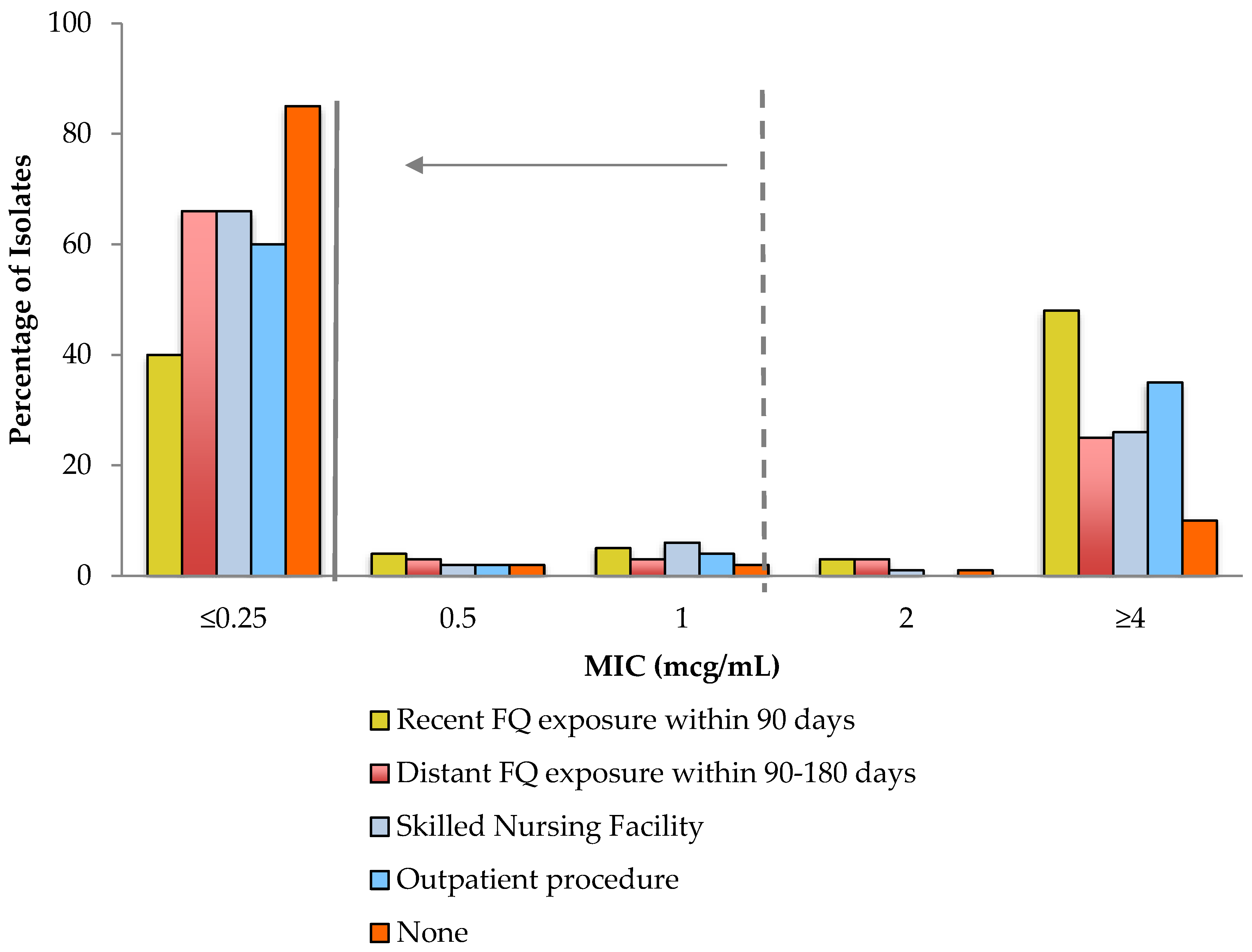
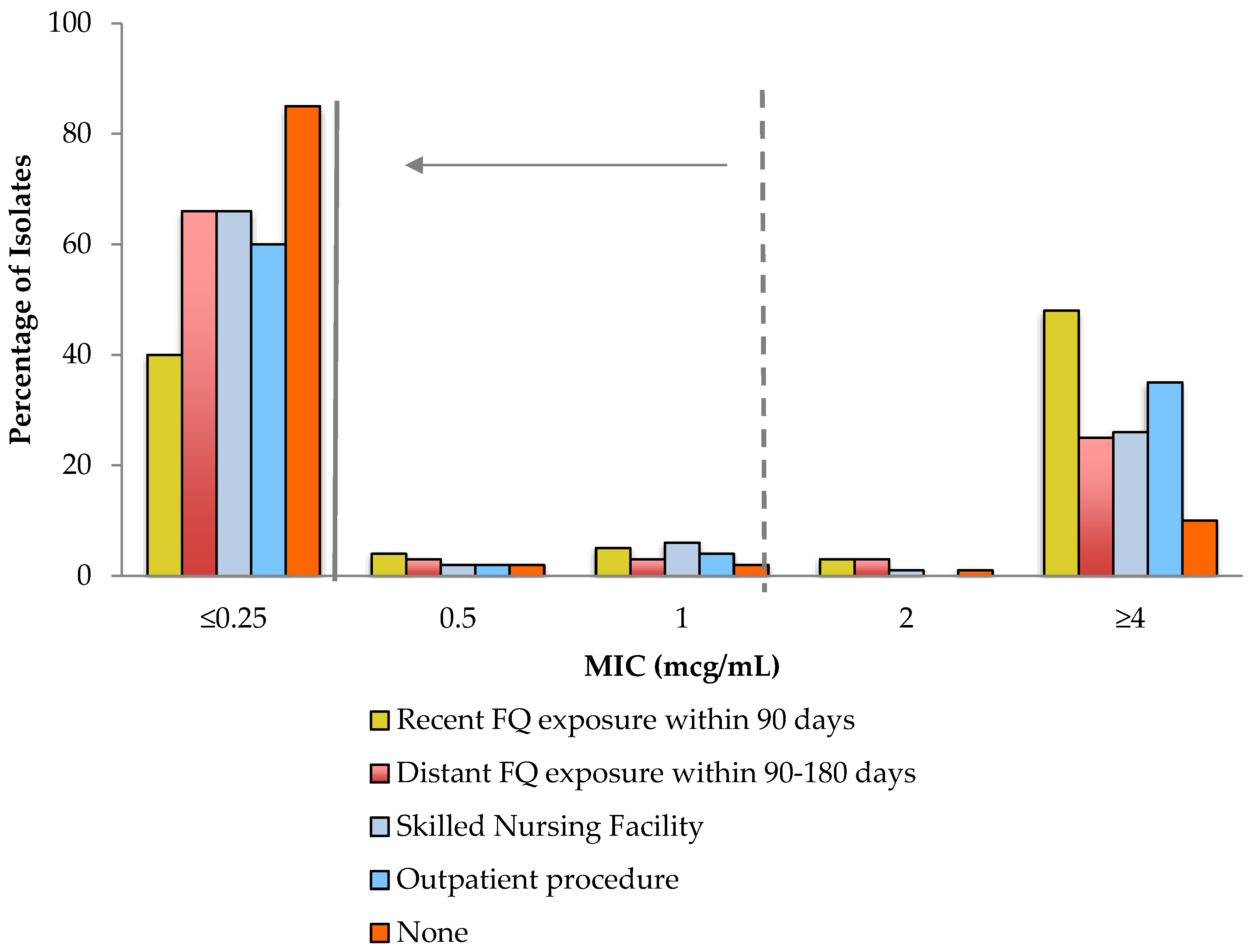
2.3. Impact of Reappraisal of MIC Values among Patients with Resistance Risk Factors
3. Discussion
3.1. Impact of Reappraisal of MIC Breakpoints
3.2. Systematic Adoption of Updated MIC Breakpoint Values
3.3. Impact on Fluoroquinlone Prescribing
3.4. Strengths and Limitations
4. Materials and Methods
4.1. Setting
4.2. Study Design and Definitions
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Center for Disease, Dynamics Economics & Policy. ResistanceMap: Antibiotic resistance. Available online: https://resistancemap.cddep.org/ (accessed on 26 December 2019).
- Kutob, L.F.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Effectiveness of oral antibiotics for definitive therapy of Gram-negative bloodstream infections. Int. J. Antimicrob. Agents. 2016, 48, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Thurber, K.M.; Arnold, J.R.; Narayanan, P.P.; Dierkhising, R.A.; Sampathkumar, P. Comparison of intravenous and oral definitive antibiotic regimens in hospitalised patients with Gram-negative bacteraemia from a urinary tract infection. J. Glob. Antimicrob. Resist. 2019, 18, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brigmon, M.M.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Impact of fluoroquinolone resistance in Gram-negative bloodstream infections on healthcare utilization. Clin. Microbiol. Infect. 2015, 21, 843–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camins, B.C.; Marschall, J.; DeVader, S.R.; Maker, D.E.; Hoffman, M.W.; Fraser, V.J. The clinical impact of fluoroquinolone resistance in patients with E. coli bacteremia. J. Hosp. Med. 2011, 6, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFife, R.; Scheetz, M.H.; Feinglass, J.M.; Postelnick, M.J.; Scarsi, K.K. Effect of differences in MIC values on clinical outcomes in patients with bloodstream infections caused by gram-negative organisms treated with levofloxacin. Antimicrob. Agents Chemother. 2009, 53, 1074–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattanaumpawan, P.; Nachamkin, I.; Bilker, W.B. High fluoroquinolone MIC is associated with fluoroquinolone treatment failure in urinary tract infections caused by fluoroquinolone susceptible Escherichia coli. Ann Clin. Microbiol. Antimicrob. 2017, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinolone In Vitro Susceptibility Test Interpretive Criteria Evaluations. Available online: http://www.uscast.org (accessed on 22 December 2019).
- Chantell, C.; Humphries, R.M.; Lewis, J.S. CLSI Rationale Document MR02. Available online: http://www.clsi.org (accessed on 22 December 2019).
- Hindler, J.A.; Schuetz, A.N. CLSI Subcommittee on Antimicrobial Susceptibility Testing News Update. Available online: http://www.clsi.org (accessed on 22 December 2019).
- Dan, S.; Shah, A.; Justo, J.A. Prediction of fluoroquinolone resistance in gram-negative bacteria causing bloodstream infections. Antimicrob. Agents Chemother. 2016, 60, 2265–2272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hasan, M.N.; Lahr, B.D.; Eckel-Passow, J.E.; Baddour, L.M. Antimicrobial resistance trends of Escherichia coli bloodstream isolates: A population-based study, 1998–2007. J. Antimicrob. Chemother. 2009, 64, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hasan, M.N.; Eckel-Passow, J.E.; Baddour, L.M. Impact of healthcare-associated acquisition on community-onset Gram-negative bloodstream infection: A population-based study. Eur. J. Clin. Microbiol. Infect Dis. Publ. Eur. Soc. Clin. Microbiol. 2012, 31, 1163–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hasan, M.N.; Gould, A.P.; Drennan, C. Empirical fluoroquinolones versus broad-spectrum beta-lactams for gram-negative bloodstream infections in the absence of antimicrobial resistance risk factors. J. Glob. Antimicrob. Resist. 2019. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Conley, A.T.; Cosgrove, S.E. Association of 30-day mortality with oral step-down vs. continued intravenous therapy in patients hospitalized with Enterobacteriaceae bacteremia. JAMA Intern. Med. 2019, 179, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Franceschini, E.; Koppel, F. Seven versus 14 days of antibiotic therapy for uncomplicated gram-negative bacteremia: A noninferiority randomized controlled trial. Clin. Infect. Dis. 2019, 69, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Peirano, G.; Pitout, J.D.D. Fluoroquinolone-resistant Escherichia coli sequence Type 131 isolates causing bloodstream infections in a Canadian region with a centralized laboratory system: Rapid emergence of the H30-Rx sublineage. Antimicrob. Agents Chemother. 2014, 58, 2699–2703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punjabi, C.; Tien, V.; Meng, L.; Deresinski, S.; Holubar, M. Oral fluoroquinolone or trimethoprim-sulfamethoxazole vs. β-lactams as step-down therapy for Enterobacteriaceae bacteremia: Systematic review and meta-analysis. Open Forum. Infect. Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Al-Hasan, M.N.; Rac, H. Transition from intravenous to oral antimicrobial therapy in patients with uncomplicated and complicated bloodstream infections. Clin. Microbiol. Infect. 2020, 26, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Yarrington, M.E. Impact of FDA black box warning on fluoroquinolone and alternative antibiotic use in southeastern US hospitals. Infect Control Hosp. Epidemiol. 2019, 40, 1297–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Organism | N | Previous Susceptibility | Updated Susceptibility | Mean Difference (95% CI) | p-Value |
|---|---|---|---|---|---|
| Enterobacteriaceae | 967 | 803 (83.0) | 753 (77.9) | −5.2 (−6.6, −3.8) | < 0.001 |
| E. coli | 543 | 416 (76.6) | 386 (71.1) | −5.5 (−7.5, −3.6) | < 0.001 |
| Klebsiella spp. | 205 | 187 (91.2) | 176 (85.9) | −5.4 (−8.5, −2.3) | < 0.001 |
| P. mirabilis | 72 | 63 (87.5) | 60 (83.3) | −4.2 (−8.9, 0.6) | 0.08 |
| Enterobacter spp. | 67 | 65 (97.0) | 63 (94.0) | −3.0 (−7.2, 1.2) | 0.16 |
| Non-fermenters | 88 | 78 (88.6) | 71 (80.7) | −8.0 (−13.7, −2.2) | 0.007 |
| P. aeruginosa | 64 | 57 (89.1) | 52 (81.3) | −7.8 (−14.6, −1.1) | 0.02 |
| Risk Factor | N * | Previous Susceptibility | Updated Susceptibility | Mean Difference (95% CI) | p-Value |
|---|---|---|---|---|---|
| Fluoroquinolone use within prior 90 d | 75 | 37 (49.3) | 30 (40.0) | −9.3 (−16.1, −2.6) | 0.007 |
| Fluoroquinolone use within prior 90–180 d | 32 | 23 (71.9) | 21 (65.6) | −6.3 (−15.1, 2.6) | 0.16 |
| Residence at skilled nursing facility | 152 | 112 (73.7) | 100 (65.8) | −7.9 (−12.2, −3.6) | < 0.001 |
| Outpatient GI/GU procedure within prior 30 d | 55 | 36 (65.5) | 33 (60.0) | −5.5 (−11.7, 0.7) | 0.08 |
| None | 682 | 607 (89.0) | 581 (85.2) | −3.8 (−5.3, −2.4) | < 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shealy, S.C.; Brigmon, M.M.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Al-Hasan, M.N. Impact of Reappraisal of Fluoroquinolone Minimum Inhibitory Concentration Susceptibility Breakpoints in Gram-Negative Bloodstream Isolates. Antibiotics 2020, 9, 189. https://doi.org/10.3390/antibiotics9040189
Shealy SC, Brigmon MM, Justo JA, Bookstaver PB, Kohn J, Al-Hasan MN. Impact of Reappraisal of Fluoroquinolone Minimum Inhibitory Concentration Susceptibility Breakpoints in Gram-Negative Bloodstream Isolates. Antibiotics. 2020; 9(4):189. https://doi.org/10.3390/antibiotics9040189
Chicago/Turabian StyleShealy, Stephanie C., Matthew M. Brigmon, Julie Ann Justo, P. Brandon Bookstaver, Joseph Kohn, and Majdi N. Al-Hasan. 2020. "Impact of Reappraisal of Fluoroquinolone Minimum Inhibitory Concentration Susceptibility Breakpoints in Gram-Negative Bloodstream Isolates" Antibiotics 9, no. 4: 189. https://doi.org/10.3390/antibiotics9040189
APA StyleShealy, S. C., Brigmon, M. M., Justo, J. A., Bookstaver, P. B., Kohn, J., & Al-Hasan, M. N. (2020). Impact of Reappraisal of Fluoroquinolone Minimum Inhibitory Concentration Susceptibility Breakpoints in Gram-Negative Bloodstream Isolates. Antibiotics, 9(4), 189. https://doi.org/10.3390/antibiotics9040189