
Functionalized Textile Based Therapy for the Treatment of Atopic Dermatitis



Abstract
:1. Introduction
2. Textiles-Based Complementary Therapy
2.1. Wet-Wrap Dressing
2.2. Healthcare Textiles
2.3. Medical Textiles
2.3.1. Antibacterial Agents for AD Treatment
Metal Nanoparticles
Organic Antibacterial Agents
2.3.2. Herbal Medicine Coated Textile Therapy for AD Treatment
3. Fixation Strategies of Antibacterial Agents on Fabrics
3.1. Inclusive Method
3.2. Textile Finishing Approaches
3.3. Encapsulation Techniques
3.3.1. Micro/Nano-Capsules
3.3.2. Cyclodextrin
3.3.3. Hydrogel Technology
Application of Hydrogel in Functional Textiles
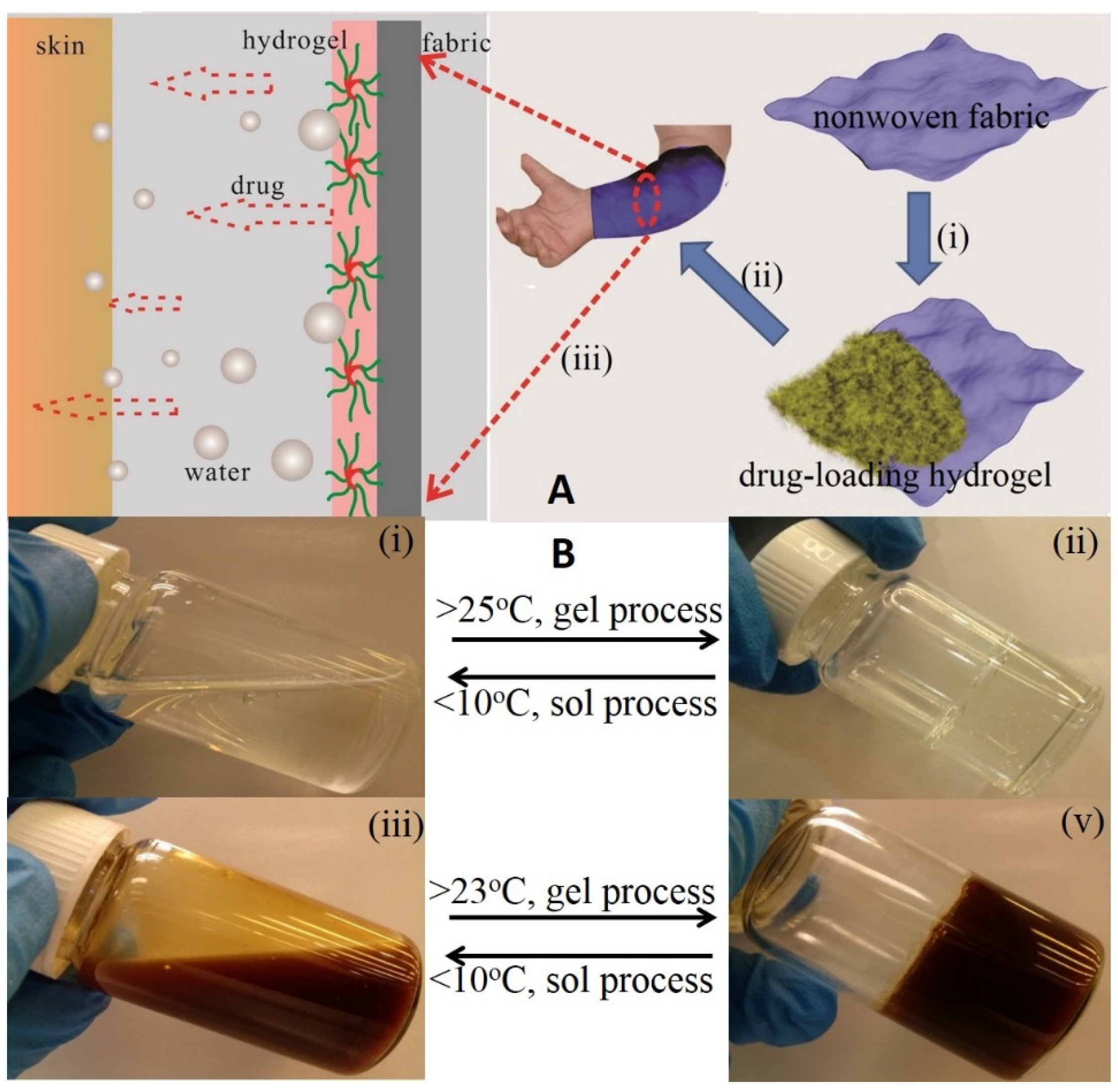
Hydrogel Based Transdermal Therapy
4. Conclusions and Future Outlook
Acknowledgments
Conflicts of Interest
References
- Wolter, S.; Price, H.N. Atopic dermatitis. Pediatr. Clin. N. Am. 2014, 61, 241–260. [Google Scholar] [CrossRef] [PubMed]
- Bieber, T. Mechanisms of disease: Atopic dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, S.F. Atopic dermatitis: Natural history, diagnosis, and treatment. ISRN Allergy 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Shekariah, T.; Kalavala, M.; Alfaham, M. Atopic dermatitis in children: A practical approach. Paediatr. Child Health 2011, 21, 112–118. [Google Scholar] [CrossRef]
- Tsianakas, A.; Ständer, S. Dupilumab: A milestone in the treatment of atopic dermatitis. Lancet 2016, 387, 4–5. [Google Scholar] [CrossRef]
- Lee, S.J.; Woo, S.I.; Ahn, S.H.; Lim, D.K.; Hong, J.Y.; Park, J.H.; Lim, J.; Kim, M.K.; Kwon, S.W. Functional interpretation of metabolomics data as a new method for predicting long-term side effects: Treatment of atopic dermatitis in infants. Sci. Rep. 2014, 4, 7408. [Google Scholar] [CrossRef] [PubMed]
- Akdis, C.A.; Akdis, M.; Bieber, T.; Bindslev-Jensen, C.; Boguniewicz, M.; Eigenmann, P.; Hamid, Q.; Kapp, A.; Leung, D.Y.; Platts-Mills, T.A.; et al. Diagnosis and treatment of atopic dermatitis in children and adults. Allergy 2006, 61, 969–987. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.K.; Burrows, N.P. Atopic dermatitis. Common Dermatoses 2009, 5, 242–245. [Google Scholar] [CrossRef]
- Watson, W.; Kapur, S. Atopic dermatitis. Allergy Asthma Clin. Immunol. 2011, 7. [Google Scholar] [CrossRef] [PubMed]
- Tokura, Y. Atopic Dermatitis: Common Extrinsic and Enigmatic Intrinsic Types. In Immunology of the Skin: Basic and Clinical Sciences in Skin Immune Responses; Kabashima, K., Ed.; Springer: Tokyo, Japan, 2016. [Google Scholar]
- Tang, T.S.; Bieber, T.; Williams, H.C. Does “autoreactivity” play a role in atopic dermatitis? J. Allergy Clin. Immun. 2012, 129, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, R.; Salio, M.; Lloyd-Lavery, A.; Subramaniam, S.; Bourgeois, E.; Archer, C.; Cheung, K.L.; Hardman, C.; Chandler, D.; Salimi, M.; et al. Filaggrin inhibits generation of CD1a neolipid antigens by house dust mite-derived phospholipase. Sci. Transl. Med. 2016, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kessel, J.; Goldenberg, G. Therapies to Improve the Cosmetic Symptoms of Atopic Dermatitis. Cutis 2016, 97, 183–186. [Google Scholar] [PubMed]
- Galli, E.; Neri, I.; Ricci, G.; Baldo, E.; Barone, M.; Fortina, A.B.; Bernardini, R.; Berti, I.; Caffarelli, C.; Calamelli, E. Consensus Conference on Clinical Management of pediatric Atopic Dermatitis. Ital. J. Pediatr. 2016, 42, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Farhi, D.; Taieb, A.; Tilles, G.; Wallach, D. The historical basis of a misconception leading to undertreating atopic dermatitis (eczema): Facts and controversies. Clin. Dermatol. 2010, 28, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Chan, B.C.; Leung, P.C. Chinese herbal medicine research in eczema treatment. Chin. Med. 2011, 6, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Dabade, T.S.; Davis, D.M.; Wetter, D.A.; Hand, J.L.; McEvoy, M.T.; Pittelkow, M.R.; Azhary, R.A.; Davis, M.D. Wet dressing therapy in conjunction with topical corticosteroids is effective for rapid control of severe pediatric atopic dermatitis: Experience with 218 patients over 30 years at Mayo Clinic. J. Am. Acad. Dermatol. 2012, 67, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Buschmann, H.J.; Dehabadi, V.A.; Wiegand, C. Medical, cosmetic and odour resistant finishes for textiles. In Functional Finishes for Textiles: Improving Comfort, Performance and Protection; Roshan, P., Ed.; Woodhead Publishing: Cambridge, UK, 2014; pp. 303–330. [Google Scholar]
- Oranje, A.P.; Devillers, A.C.; Kunz, B.; Jones, S.L.; DeRaeve, L.; Van Gysel, D.; de Waard-van der Spek, F.B.; Grimalt, R.; Torrelo, A.; Stevens, J.; et al. Treatment of patients with atopic dermatitis using wet-wrap dressings with diluted steroids and/or emollients. An expert panel's opinion and review of the literature. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Elliott, I.M.; Elliott, J.R. A Short History of Surgical Dressings; Pharmaceutical Press: London, UK, 1964; pp. 1–118. [Google Scholar]
- Nicol, N.H. Atopic dermatitis: The (wet) wrap-up. Am. J. Nurs. 1987, 87, 1560–1563. [Google Scholar] [CrossRef] [PubMed]
- Bingham, L.G.; Noble, J.W.; Davis, M.D. Wet dressings used with topical corticosteroids for pruritic dermatoses: A retrospective study. J. Am. Acad. Dermatol. 2009, 60, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Goodyear, H.M.; Harper, J.I. Wet-wrap dressings for the treatment of atopic eczema in children. Br. J. Dermatol. 1991, 125, 604. [Google Scholar] [CrossRef] [PubMed]
- Oranje, A.P.; Verbeek, R.; Verzaal, P.; Haspels, I.; Prens, E.; Nagelkerken, L. Wet-wrap treatment using dilutions of tacrolimus ointment and fluticasone propionate cream in human APOC1 (+/+) mice with atopic dermatitis. Br. J. Dermatol. 2009, 160, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Nicol, N.H.; Boguniewicz, M.; Strand, M.; Klinnert, M.D. Wet wrap therapy in children with moderate to severe atopic dermatitis in a multidisciplinary treatment program. J. Allergy Clin. Immunol. Pract. 2014, 2, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Janmohamed, S.R.; Oranje, A.P.; Devillers, A.C.; Rizopoulos, D.; van Praag, M.C.; Van Gysel, D.; Goeteyn, M. The proactive wet-wrap method with diluted corticosteroids versus emollients in children with atopic dermatitis: A prospective, randomized, double-blind, placebo-controlled trial. J. Am. Acad. Dermatol. 2014, 70, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, S.J.; Kim, D.; Bang, D. The effect of wet-wrap dressing on epidermal barrier in patients with atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Segre, J.A. Epidermal barrier formation and recovery in skin disorders. J. Clin. Investig. 2006, 116, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Hwang, S.H.; Hong, S.K.; Seo, J.K.; Sung, H.S.; Park, S.W.; Shin, J.H. The clinical efficacy, safety and functionality of anion textile in the treatment of atopic dermatitis. Ann. Dermatol. 2012, 24, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Kanehara, S.; Ohtani, T.; Uede, K.; Furukawa, F. Clinical effects of undershirts coated with borage oil on children with atopic dermatitis: A double-blind, placebo-controlled clinical trial. J. Dermatol. 2007, 34, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Wakamura, T.; Sato, M.; Sato, A.; Dohi, T.; Ozaki, K.; Asou, N.; Hagata, S.; Tokura, H. A preliminary study on influence of negative air ions generated from pajamas on core body temperature and salivary IgA during night sleep. Int. J. Occup. Med. Environ. 2004, 17, 295–298. [Google Scholar]
- Yang, M.X.; Pu, D.D. Research on Influencing Factors and Exploitation of Negative-ion Textiles. Prog. Text. Sci. Technol. 2009, 2, 10–11. [Google Scholar]
- Zheng, Q.S.; Hu, X.-Y. The Performance and Application of Yanniansu (Tourmaline) Fiber. Synth. Fiber China 2010, 1, 11–13. [Google Scholar]
- Lin, M.F.; Chen, H.J.; Chen, C.J.; Chen, Y.C.; Chen, C.M. Natural Tourmaline Anion Fiber and Filter and Producing Method. U.S. Patent 20,070,259,178, 8 November 2007. [Google Scholar]
- Dover, J.S.; Phillips, T.J.; Arndt, K.A. Cutaneous effects and therapeutic uses of heat with emphasis on infrared radiation. J. Am. Acad. Dermatol. 1989, 20, 278–286. [Google Scholar] [CrossRef]
- Sugihara, T.; Suzuki, M.; Komiya, M.M. Rayon fiber containing tourmaline particles and method for the preparation thereof. U.S. Patent 5,863,653 A, 26 January 1999. [Google Scholar]
- Lin, M.F.; Chen, H.J.; Chen, C.J.; Chen, Y.C.; Chen, C.M. Natural Tourmaline Anion Fiber and Filter and Production Method. U.S. Patent 8,231,968 B2, 31 July 2012. [Google Scholar]
- Tijing, L.D.; Ruelo, M.T.G.; Amarjargal, A.; Pant, H.R.; Park, C.-H.; Kim, D.W.; Kim, C.S. Antibacterial and superhydrophilic electrospun polyurethane nanocomposite fibers containing tourmaline nanoparticles. Chem. Eng. J. 2012, 197, 41–48. [Google Scholar] [CrossRef]
- Yeh, J.T.; Hsiung, H.H.; Wei, W.; Zhu, P.; Chen, K.N.; Jiang, T. Negative air ion releasing properties of tourmaline/bamboo charcoal compounds containing ethylene propylene diene terpolymer/polypropylene composites. J. Appl. Polym. Sci. 2009, 113, 1097–1110. [Google Scholar] [CrossRef]
- Melnik, B.; Plewig, G. Are disturbances of omega-6-fatty acid metabolism involved in the pathogenesis of atopic dermatitis? Acta Derm. 1992, 176, 77–85. [Google Scholar]
- Diezel, W.; Schulz, E.; Shanks, M.; Heise, H. Plant oils: Topical application and anti-inflammatory effects (Croton oil test). Dermatologische Monatsschrift 1993, 179, 173–176. [Google Scholar]
- Al-Khamees, W.A.; Schwartz, M.D.; Alrashdi, S.; Algren, A.D.; Morgan, B.W. Status epilepticus associated with borage oil ingestion. J. Med. Toxicol. 2011, 7, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Ernst, E. The usage of complementary therapies by dermatological patients: A systemic review. Br. J. Dermatol. 2000, 142, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Bamford, J.; Ray, S.; Musekiwa, A.; van Gool, C.; Humphreys, R.; Ernst, E. Oral evening primrose oil and borage oil for eczema. Cochrane Database Syst. Rev. 2013, 30, CD004416. [Google Scholar]
- Foster, R.H.; Hardy, G.; Alany, R.G. Borage oil in the treatment of atopic dermatitis. Nutrition 2010, 26, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, G.; Chakraborty, J.N. Antimicrobial performance of cotton finished with triclosan, silver and chitosan. Fash. Text. 2015, 2. [Google Scholar] [CrossRef]
- Dastjerdi, R.; Montazer, M. A review on the application of inorganic nano-structured materials in the modification of textiles: Focus on anti-microbial properties. Colloids Surf. B 2010, 79, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Cranston, R. Recent Advances in Antimicrobial Treatments of Textiles. Text. Res. J. 2008, 78, 60–72. [Google Scholar] [CrossRef]
- Windler, L.; Height, M.; Nowack, B. Comparative evaluation of antimicrobials for textile applications. Environ. Int. 2013, 53, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Simoncic, B.; Tomsic, B. Structures of Novel Antimicrobial Agents for Textiles—A Review. Text. Res. J. 2010, 80, 1721–1737. [Google Scholar] [CrossRef]
- Hebeish, A.; El-Naggar, M.E.; Fouda, M.M.G.; Ramadan, M.A.; Al-Deyab, S.S.; El-Rafie, M.H. Highly effective antibacterial textiles containing green synthesized silver nanoparticles. Carbohydr. Polym. 2011, 86, 936–940. [Google Scholar] [CrossRef]
- Xue, Y.; Xiao, H.; Zhang, Y. Antimicrobial polymeric materials with quaternary ammonium and phosphonium salts. Int. J. Mol. Sci. 2015, 16, 3626–3655. [Google Scholar] [CrossRef] [PubMed]
- Tayel, A.A.; Moussa, S.H.; El-Tras, W.F.; Elguindy, N.M.; Opwis, K. Antimicrobial textile treated with chitosan from Aspergillus niger mycelial waste. Int. J. Biol. Macromol. 2011, 49, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Ahmad, A.; Khan, M.I.; Yusuf, M.; Shahid, M.; Manzoor, N.; Mohammad, F. Antimicrobial activity of wool yarn dyed with Rheum emodi L. (Indian Rhubarb). Dyes Pigments 2012, 95, 206–214. [Google Scholar] [CrossRef]
- Majhi, B.; Satapathy, K.B.; Mishra, S.K.; Mohapatra, A. Studies on antimicrobial effect of natural dyes and pigments obtained from the leaf of Artocarpus heterophyllus Lam. and Tectona grandis L.F. Int. J. Phytomed. 2016, 7, 396–401. [Google Scholar]
- Haug, S.; Roll, A.; Schmid-Grendelmeier, P.; Johansen, P.; Wüthrich, B.; Kündig, T.; Senti, G. Coated textiles in the treatment of atopic dermatitis. In Biofunctional, Textiles and the Skin; Hipler, U.C., Elsner, P., Eds.; Karger Publishers: Karger, Basel, 2006; Volume 33, pp. 144–151. [Google Scholar]
- He, Z.P.; Fu, G.W.; Geng, Y.F. Test and evaluation of negative ions textiles. Text. Dyeing Finish. J. 2013, 35, 6–10. [Google Scholar]
- Leung, D.Y.; Boguniewicz, M.; Howell, M.D.; Nomura, I.; Hamid, Q.A. New insights into atopic dermatitis. J. Clin. Investig. 2004, 113, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Kale, R.; Meena, C.R. Synthesis of Titanium dioxide Nanoparticles and Application on Nylon fabric using Layer by Layer technique for Antimicrobial Property. Adv. Appl. Sci. Res. 2012, 3, 3073–3080. [Google Scholar]
- Dubas, S.T.; Kumlangdudsana, P.; Potiyaraj, P. Layer-by-layer deposition of antimicrobial silver nanoparticles on textile fibers. Colloid Surf. A 2006, 289, 105–109. [Google Scholar] [CrossRef]
- Ashayer-Soltani, R.; Hunt, C.; Thomas, O. Fabrication of highly conductive stretchable textile with silver nanoparticles. Text. Res. J. 2016, 86, 1041–1049. [Google Scholar] [CrossRef]
- Ditaranto, N.; Picca, R.; Sportelli, M.; Sabbatini, L.; Cioffi, N. Surface characterization of textiles modified by copper and zinc oxide nano-antimicrobials. Surf. Interface Anal. 2016, 48, 505–508. [Google Scholar] [CrossRef]
- Gedanken, A.; Nitzan, Y.; Perelshtein, I.; Perkas, N.; Applerot, G. Sonochemical Coating of Textiles with Metal Oxide Nanoparticles for Antimicrobial Fabrics. Google Patents EP2294260 A1, 16 March 2011. [Google Scholar]
- Sójka-Ledakowicz, J.; Chruściel, J.; Kudzin, M.H.; Łatwińska, M.; Kiwała, M. Antimicrobial functionalization of textile materials with copper silicate. Fibres Text. East. Eur. 2016, 5, 151–156. [Google Scholar] [CrossRef]
- Jaeger, T.; Rothmaier, M.; Zander, H.; Ring, J.; Gutermuth, J.; Anliker, M.D. Acid-coated Textiles (pH 5.5–6.5)—A New Therapeutic Strategy for Atopic Eczema? Acta Derm. Venereol. 2015, 95, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Eunjou, Y.; Yoo, E.S. A novel bioactive fabric dyed with unripe Citrus grandis Osbeck extract part 1: Dyeing properties and antimicrobial activity on cotton knit fabrics. Text. Res. J. 2010, 80, 2117–2123. [Google Scholar] [CrossRef]
- Eunjou, Y.; Hong, J.Y.; Yoo, E.S. A novel bioactive fabric dyed with unripe Citrus grandis Osbeck extract part 2: Effects of the Citrus extract and dyed fabric on skin irritancy and atopic dermatitis. Text. Res. J. 2010, 80, 2124–2131. [Google Scholar] [CrossRef]
- Radu, C.-D.; Parteni, O.; Ochiuz, L. Applications of cyclodextrins in medical textiles—Review. J. Control. Release 2016, 224, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Emam, H.E.; Manian, A.P.; Široká, B.; Duelli, H.; Redl, B.; Pipal, A.; Bechtold, T. Treatments to impart antimicrobial activity to clothing and household cellulosic-textiles—Why “Nano”-silver? J. Clean. Prod. 2013, 39, 17–23. [Google Scholar] [CrossRef]
- Budama, L.; Çakır, B.A.; Topel, Ö.; Hoda, N. A new strategy for producing antibacterial textile surfaces using silver nanoparticles. Chem. Eng. J. 2013, 228, 489–495. [Google Scholar] [CrossRef]
- Balakumaran, M.; Ramachandran, R.; Jagadeeswari, S.; Kalaichelvan, P. In vitro biological properties and characterization of nanosilver coated cotton fabrics—An application for antimicrobial textile finishing. Int. Biodeterior. Biodegrad. 2016, 107, 48–55. [Google Scholar] [CrossRef]
- Schmid, M.H.; Korting, H.C. The concept of the acid mantle of the skin: Its relevance for the choice of skin cleansers. Dermatology 1995, 191, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Bischof Vukušić, S.; Flinčec Grgac, S.; Budimir, A.; Kalenić, S. Cotton textiles modified with citric acid as efficient anti-bacterial agent for prevention of nosocomial infections. Croat. Med. J. 2011, 52, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.-S.; Lee, K.-K.; Kim, J.-W. Durable press and antimicrobial finishing of cotton fabrics with a citric acid and chitosan treatment. Text. Res. J. 1998, 68, 772–775. [Google Scholar] [CrossRef]
- Fluhr, J.W.; Breternitz, M.; Kowatzki, D.; Bauer, A.; Bossert, J.; Elsner, P.; Hipler, U.C. Silver-loaded seaweed-based cellulosic fiber improves epidermal skin physiology in atopic dermatitis: Safety assessment, mode of action and controlled, randomized single-blinded exploratory in vivo study. Exp. Dermatol. 2010, 19, e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.L.; Liu, B.Y.; Ma, K.W. Traditional Chinese medicine. Lancet 2008, 372, 1938–1940. [Google Scholar] [CrossRef]
- Xu, J.; Yang, Y. Traditional Chinese medicine in the Chinese health care system. Health Policy 2009, 90, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Leonard, T.; Bath-Hextall, F.; Chambers, C.; Lee, C.; Humphreys, R.; Williams, H. Chinese herbal medicine for atopic eczema. Cochrane Database Syst. Rev. 2013, 9, CD002291. [Google Scholar]
- Tan, H.Y.; Zhang, A.L.; Chen, D.; Xue, C.C.; Lenon, G.B. Chinese herbal medicine for atopic dermatitis: A systematic review. J. Am. Acad. Dermatol. 2013, 69, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.; Lee, S.; Kim, S.; Choi, I. Inpatient treatment for severe atopic dermatitis in a Traditional Korean Medicine hospital: Introduction and retrospective chart review. Complement. Ther. Med. 2013, 21, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Yang, A.; Xue, C.; Li, C.; Pang, C.; Zhang, W.; Williams, H. Chinese herbal medicine for atopic eczema. Cochrane Database Syst. Rev. 2013, 10, CD008642. [Google Scholar]
- Akamatsu, H.; Asada, Y.; Horio, T. Inhibitory effect of shofu-san, a Japanese kampo medicine, on neutrophil functions in vitro. Am. J. Chin. Med. 1998, 26, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.; Leung, T.; Wong, Y.; Lam, W.; Guan, D.; Ma, K.; Sung, Y.; Fok, T.; Leung, P. A pentaherbs capsule as a treatment option for atopic dermatitis in children: An open-labeled case series. Am. J. Chin. Med. 2004, 32, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Leung, T.F.; Ng, P.C.; Lam, M.C.; Kam, W.Y.; Wong, K.Y.; Lee, K.C.; Sung, Y.T.; Cheng, K.F.; Fok, T.F.; et al. Efficacy and tolerability of a Chinese herbal medicine concoction for treatment of atopic dermatitis: A randomized, double-blind, placebo-controlled study. Br. J. Dermatol. 2007, 157, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T. Efficacy of kampo medicine in treating atopic dermatitis: An overview. Evid. Based Complement. Altern. Med. 2013, 2013, 260235. [Google Scholar] [CrossRef] [PubMed]
- Yanagi, Y.; Yasuda, M.; Hashida, K.; Kadokura, Y.; Yamamoto, T.; Suzaki, H. Mechanism of salivary secretion enhancement by Byakkokaninjinto. Biol. Pharm. Bull. 2008, 31, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Saiki, I. A Kampo medicine “Juzen-taiho-to”—Prevention of malignant progression and metastasis of tumor cells and the mechanism of action. Biol. Pharm. Bull. 2000, 23, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, K.; Hikiami, H.; Goto, H.; Nakagawa, T.; Shibahara, N.; Shimada, Y. Keishibukuryogan (gui-zhi-fu-ling-wan), a Kampo formula, decreases disease activity and soluble vascular adhesion molecule-1 in patients with rheumatoid arthritis. Evid. Based Complement. Altern. Med. 2006, 3, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Kim, J.; Yu, Y.; Im, S. Modulation of experimental atopic dermatitis by topical application of Gami-Cheongyeul-Sodok-Eum. BMC Complement. Altern. Med. 2013, 13, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Hui, P.C.-L.; Wang, W.-Y.; Kan, C.-W.; Ng, F.S.-F.; Zhou, C.-E.; Wat, E.; Zhang, V.X.; Chan, C.-L.; Lau, C.B.-S.; Leung, P.-C. Preparation and characterization of chitosan/sodium alginate (CSA) microcapsule containing Cortex Moutan. Colloid Surf. A 2013, 434, 95–101. [Google Scholar] [CrossRef]
- Hui, P.C.; Wang, W.Y.; Kan, C.W.; Ng, F.S.; Wat, E.; Zhang, V.X.; Chan, C.L.; Lau, C.B.; Leung, P.C. Microencapsulation of Traditional Chinese Herbs-PentaHerbs extracts and potential application in healthcare textiles. Colloids Surf. B 2013, 111, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wat, E.; Hui, P.C.L.; Chan, B.; Ng, F.S.F.; Kan, C.W.; Wang, X.; Hu, H.; Wong, E.C.W.; Lau, C.B.S.; et al. Dual-functional transdermal drug delivery system with controllable drug loading based on thermosensitive poloxamer hydrogel for atopic dermatitis treatment. Sci. Rep. 2016, 6, 24112. [Google Scholar] [CrossRef] [PubMed]
- Klouda, L.; Mikos, A.G. Thermoresponsive hydrogels in biomedical applications. Eur. J. Pharm. Biopharm. 2008, 68, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Jeong, B.; Kim, S.W.; Bae, Y.H. Thermosensitive sol–gel reversible hydrogels. Adv. Drug Deliv. Rev. 2002, 54, 37–51. [Google Scholar] [CrossRef]
- Chen, C.C.; Fang, C.L.; Al-Suwayeh, S.A.; Leu, Y.L.; Fang, J.Y. Transdermal delivery of selegiline from alginate-Pluronic composite thermogels. Int. J. Pharm. 2011, 415, 119–128. [Google Scholar] [CrossRef] [PubMed]
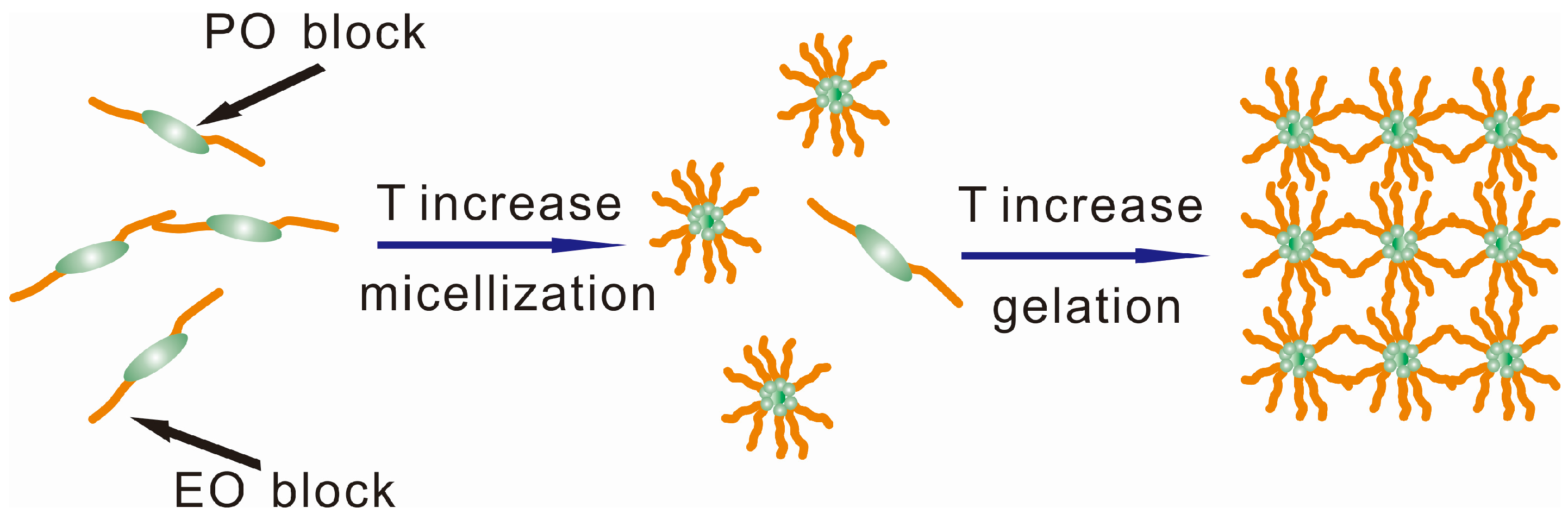
- Jia, L.; Guo, C.; Yang, L.; Xiang, J.; Tang, Y.; Liu, C.; Liu, H. Mechanism of PEO–PPO–PEO micellization in aqueous solutions studied by two-dimensional correlation FTIR spectroscopy. J. Colloid Interface Sci. 2010, 345, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Malal, R.; Li, C.; Lin, M.Y.; Colby, R.H.; Gersappe, D.; Rafailovich, M.H.; Sokolov, J.C.; Cohn, D. Rheology of thermoreversible hydrogels from multiblock associating copolymers. Macromolecules 2008, 41, 3646–3652. [Google Scholar] [CrossRef]
- Dumortier, G.; Grossiord, J.L.; Agnely, F.; Chaumeil, J.C. A review of poloxamer 407 pharmaceutical and pharmacological characteristics. Pharm. Res. 2006, 23, 2709–2728. [Google Scholar] [CrossRef] [PubMed]
- Alexandridis, P.; Hatton, T.A. Poly (ethylene oxide)/poly (propylene oxide)/poly (ethylene oxide) block copolymer surfactants in aqueous solutions and at interfaces: Thermodynamics, structure, dynamics, and modeling. Colloid Surface A 1995, 96, 1–46. [Google Scholar] [CrossRef]
- Alonso, C.; Marti, M.; Martinez, V.; Rubio, L.; Parra, J.L.; Coderch, L. Antioxidant cosmeto-textiles: Skin assessment. Eur. J. Pharm. Biopharm. 2013, 84, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.F.; Chen, H.J.; Chen, C.J.; Chen, Y.C.; Chen, C.M. Process of Making Natural Tourmaline Fiber and Filter. U.S. Patent 8491825B2, 23 July 2013. [Google Scholar]
- Hipler, U.C.; Elsner, P.; Fluhr, J.W. Antifungal and antibacterial properties of a silver-loaded cellulosic fiber. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 77, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Noé, P.; Chanzy, H. Swelling of Valonia cellulose microfibrils in amine oxide systems. Can. J. Chem. 2008, 86, 520–524. [Google Scholar] [CrossRef]
- Rosenau, T.; Potthast, A.; Sixta, H.; Kosma, P. The chemistry of side reactions and byproduct formation in the system NMMO/cellulose (Lyocell process). Prog. Polym. Sci. 2001, 26, 1763–1837. [Google Scholar] [CrossRef]
- Smartfiber AG. Available online: http://www.smartfiber.info/technology/innovation (accessed on 3 May 2016).
- Smartcel Sensitive. Available online: http://www.swicofil.com/smartfiber_smartcel_sensitive.html (accessed on 3 May 2016).
- Smartfiber AG. Available online: http://www.smartfiber.info/ (accessed on 3 May 2016).
- Leusch, A.; Holan, Z.R.; Volesky, B. Biosorption of heavy metals (Cd, Cu, Ni, Pb, Zn) by chemically-reinforced biomass of marine algae. J. Chem. Technol. Biotechnol. 1995, 62, 279–288. [Google Scholar] [CrossRef]
- AATCC Evalation Procedure 5-2011, Fabric Hand: Guidleine; American Association of Textile Chemists and Colorists: Research Triangle Park, NC, USA, 2012; pp. 388–390.
- Wiegand, C.; Hipler, U.C.; Boldt, S.; Strehle, J.; Wollina, U. Skin-protective effects of a zinc oxide-functionalized textile and its relevance for atopic dermatitis. Clin. Cosmet. Investig. Dermatol. 2013, 6, 115–121. [Google Scholar] [PubMed]
- Smartfiber AG. Available online: http://www.smartfiber.info/smartcel-sensitive/fiber (accessed on 3 May 2016).
- Yadav, A.; Prasad, V.; Kathe, A.A.; Raj, S.; Yadav, D.; Sundaramoorthy, C.; Vigneshwaran, N. Functional finishing in cotton fabrics using zinc oxide nanoparticles. Bull. Mater. Sci. 2006, 29, 641–645. [Google Scholar] [CrossRef]
- Chatterjee, S.; Salaun, F.; Campagne, C. Development of multilayer microcapsules by a phase coacervation method based on ionic interactions for textile applications. Pharmaceutics 2014, 6, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.K. Functional Coatings and Microencapsulation: A General Perspective. In Functional Coatings: By Polymer Microencapsulation; Ghosh, S.K., Ed.; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2006; pp. 1–28. [Google Scholar]
- Bansode, S.S.; Banarjee, S.K.; Gaikwad, D.D.; Jadhav, S.L.; Thorat, R.M. Microencapsulation: A review. Int. J. Pharm. Sci. Rev. Res. 2010, 1, 38–43. [Google Scholar]
- Nelson, G. Application of microencapsulation in textiles. Int. J. Pharm. 2002, 242, 55–62. [Google Scholar] [CrossRef]
- Parys, M.V. Smart Textiles Using Microencapsulation Technology. In Functional Coatings; Ghosh, S.K., Ed.; WILEY-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2006; pp. 221–258. [Google Scholar]
- Azizi, N.; Chevalier, Y.; Majdoub, M. Isosorbide-based microcapsules for cosmeto-textiles. Ind. Crops Prod. 2014, 52, 150–157. [Google Scholar] [CrossRef]
- Wang, J.M.; Xu, X.W.; Zhou, Y. The Anti-virus Properties of Nano-Chinese Medicine Microcapsule Treated Fabrics. JFBI 2008, 1, 193–200. [Google Scholar] [CrossRef]
- Liu, J.; Liu, C.; Liu, Y.; Chen, M.; Hu, Y.; Yang, Z. Study on the grafting of chitosan-gelatin microcapsules onto cotton fabrics and its antibacterial effect. Colloids Surf. B 2013, 109, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.M.; Sunderland, M. Antimicrobial and insect-resist wool fabrics by coating with microencapsulated antimicrobial and insect-resist agents. Prog. Org. Coat. 2015, 85, 221–229. [Google Scholar] [CrossRef]
- Hui, P.C.; Wang, W.Y.; Kan, C.W.; Zhou, C.E.; Ng, F.S.; Wat, E.; Zhang, V.X.; Chan, C.L.; Lau, C.B.; Leung, P.C. Preparation and characterisation of chitosan microcapsules loaded with Cortex Moutan. Int. J. Biol. Macromol. 2013, 55, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ritter, H. Cyclodextrin functionalized polymers as drug delivery systems. Polym. Chem. 2010, 1, 1552–1559. [Google Scholar] [CrossRef]
- Abdel-Halim, E.S.; Al-Deyab, S.S.; Alfaifi, A.Y. Cotton fabric finished with β-cyclodextrin: Inclusion ability toward antimicrobial agent. Carbohydr. Polym. 2014, 102, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, A.E. Cyclodextrins as a means to nanostructure and functionalize polymers. J. Incl. Phenom. Macrocycl. 2007, 60, 197–202. [Google Scholar] [CrossRef]
- Issazadeh-Baltorki, H.; Khoddami, A. Cyclodextrin-coated denim fabrics as novel carriers for ingredient deliveries to the skin. Carbohydr. Polym. 2014, 110, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, M.; Gupta, P.; Bajpai, S.K. Silver(I) ions loaded cyclodextrin-grafted-cotton fabric with excellent antimicrobial property. Fiber Polym. 2010, 11, 8–13. [Google Scholar] [CrossRef]
- Radu, C.D.; Salariu, M.; Avadanei, M.; Ghiciuc, C.; Foia, L.; Lupusoru, E.C.; Ferri, A.; Ulea, E.; Lipsa, F. Cotton-made cellulose support for anti-allergic pajamas. Carbohydr. Polym. 2013, 95, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Samchenko, Y.; Ulberg, Z.; Korotych, O. Multipurpose smart hydrogel systems. Adv. Colloid Interface Sci. 2011, 168, 247–262. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Mequanint, K. Hydrogel Biomaterials. In Biomedical Engineering-Frontiers and Challenges; Fazel, R., Ed.; Intechopen: Rijeka, Croatia, 2011; pp. 275–296. [Google Scholar]
- Hoffman, A.S. Hydrogels for biomedical applications. Adv. Drug Deliv. Rev. 2012, 64, 18–23. [Google Scholar] [CrossRef]
- Chen, Q.; Zhu, L.; Zhao, C.; Wang, Q.; Zheng, J. A robust, one-pot synthesis of highly mechanical and recoverable double network hydrogels using thermoreversible sol-gel polysaccharide. Adv. Mater. 2013, 25, 4171–4176. [Google Scholar] [CrossRef] [PubMed]
- Peppas, N.A.; Hilt, J.Z.; Khademhosseini, A.; Langer, R. Hydrogels in Biology and Medicine: From Molecular Principles to Bionanotechnology. Adv. Mater. 2006, 18, 1345–1360. [Google Scholar] [CrossRef]
- Yang, H.; Zhu, H.; Hendrix, M.M.; Lousberg, N.J.; de with, G.; Esteves, A.C.; Xin, J.H. Temperature-triggered collection and release of water from fogs by a sponge-like cotton fabric. Adv. Mater. 2013, 25, 1150–1154. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Meng, H.; Li, G.; Ibekwe, S.I. A review of stimuli-responsive polymers for smart textile applications. Smart Mater. Struct. 2012, 21, 053001. [Google Scholar] [CrossRef]
- Ter Schiphorst, J.; van den Broek, M.; de Koning, T.; Murphy, J.N.; Schenning, A.P.H.J.; Esteves, A.C.C. Dual light and temperature responsive cotton fabric functionalized with a surface-grafted spiropyran–NIPAAm-hydrogel. J. Mater. Chem. A 2016, 4, 8676–8681. [Google Scholar] [CrossRef]
- Hu, J.; Lu, J. Smart polymers for textile applications. In Smart Polymers and their Applications; Woodhead Publishing Limited: Cambridge, UK, 2014; p. 14. [Google Scholar]
- Sun, T.; Wang, G.; Feng, L.; Liu, B.; Ma, Y.; Jiang, L.; Zhu, D. Reversible switching between superhydrophilicity and superhydrophobicity. Angew. Chem. Int. Ed. Engl. 2004, 43, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Wang, Q.; Wang, T. Thermoresponsive PNIPAAm-modified cotton fabric surfaces that switch between superhydrophilicity and superhydrophobicity. Appl. Surf. Sci. 2012, 258, 4888–4892. [Google Scholar] [CrossRef]
- Bashari, A.; Hemmatinejad, N.; Pourjavadi, A. Surface modification of cotton fabric with dual-responsive PNIPAAm/chitosan nano hydrogel. Polym. Adv. Technol. 2013, 24, 797–806. [Google Scholar] [CrossRef]
- Gras, S.L.; Mahmud, T.; Rosengarten, G.; Mitchell, A.; Kalantar-Zadeh, K. Intelligent control of surface hydrophobicity. Chem. Phys. Chem. 2007, 8, 2036–2050. [Google Scholar] [CrossRef] [PubMed]
- Duval, A.; Lange, H.; Lawoko, M.; Crestini, C. Modification of Kraft Lignin to Expose Diazobenzene Groups: Toward pH- and Light-Responsive Biobased Polymers. Biomacromolecules 2015, 16, 2979–2989. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Hu, J.; Meng, Q. Nonwoven supported temperature-sensitive poly (N-isopropylacrylamide)/polyurethane copolymer hydrogel with antibacterial activity. J. Biomed. Mater. Res. B 2009, 89, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.P.; Espiga, A.; Silva, D.; Baptista, P.; Henriques, J.; Ferreira, C.; Silva, J.C.; Borges, J.P.; Pires, E.; Chaves, P. Development of a new chitosan hydrogel for wound dressing. Wound Repair Regen. 2009, 17, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Hu, H.; Yang, Z.; He, L.; Kong, Y.; Fei, B.; Xin, J.H. Smart hydrogel-functionalized textile system with moisture management property for skin application. Smart Mater. Struct. 2014, 23, 1–11. [Google Scholar] [CrossRef]
- Peppas, N.A.; Bures, P.; Leobandung, W.; Ichikawa, H. Hydrogels in pharmaceutical formulations. Eur. J. Pharm. Biopharm. 2000, 50, 27–46. [Google Scholar] [CrossRef]
- Cerchiara, T.; Bigucci, F.; Luppi, B. Hydrogel Vehicles for Hydrophilic Compounds. In Percutaneous Penetration Enhancers Chemical Methods in Penetration Enhancement: Drug Manipulation Strategies and Vehicle Effects; Dragicevic, N., Maibach, H.I., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 285–298. [Google Scholar]
- Kircik, L.; Del Rosso, J. A novel hydrogel vehicle formulated for the treatment of atopic dermatitis. J. Drugs Dermatol. 2007, 6, 718–722. [Google Scholar] [PubMed]
- Kircik, L.H. The effect of desonide hydrogel on pruritus associated with atopic dermatitis. J. Drugs Dermatol. 2014, 13, 725–728. [Google Scholar] [PubMed]
- Üstündağ Okur, N.; Çağlar, E.Ş.; Arpa, M.D.; Karasulu, H.Y. Preparation and evaluation of novel microemulsion-based hydrogels for dermal delivery of benzocaine. Pharm. Dev. Technol. 2016, 22, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.; Babla, H.; Han, T.; Das, D.B. Lidocaine carboxymethylcellulose with gelatine co-polymer hydrogel delivery by combined microneedle and ultrasound. Drug Deliv. 2016, 23, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Yapar, E.A.; Ýnal, Ö. Poly (ethylene oxide)–poly (propylene oxide)-based copolymers for transdermal drug delivery: An overview. Trop. J. Pharm. Res. 2013, 11, 855–866. [Google Scholar] [CrossRef]
- Arora, A.; Prausnitz, M.R.; Mitragotri, S. Micro-scale devices for transdermal drug delivery. Int. J. Pharm. 2008, 364, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; Singh, T.R.R.; Morrow, D.I.; Woolfson, A.D. Transdermal drug delivery-microneedle. In Microneedle-Mediated Transdermal and Intradermal Drug Delivery, 1st ed.; John Wiley & Sons: New York, NY, USA, 2012; pp. 1–19. [Google Scholar]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Cevc, G.; Vierl, U. Nanotechnology and the transdermal route: A state of the art review and critical appraisal. J. Control. Release 2010, 141, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.; Dwivedi, S.; Ajazuddin; Giri, T.K.; Saraf, S.; Saraf, S.; Tripathi, D.K. Approaches for breaking the barriers of drug permeation through transdermal drug delivery. J. Control. Release 2012, 164, 26–40. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, S.; Kuchler, S.; Wischke, C.; Lendlein, A.; Stein, C.; Schafer-Korting, M. A thermosensitive morphine-containing hydrogel for the treatment of large-scale skin wounds. Int. J. Pharm. 2013, 444, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Ishii, Y.; Nakae, T.; Sakamoto, F.; Matsuo, K.; Matsuo, K.; Quan, Y.S.; Kamiyama, F.; Fujita, T.; Yamamoto, A.; Nakagawa, S.; Okada, N. A transcutaneous vaccination system using a hydrogel patch for viral and bacterial infection. J. Control. Release 2008, 131, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Ajazuddin; Alexander, A.; Khichariya, A.; Gupta, S.; Patel, R.J.; Giri, T.K.; Tripathi, D.K. Recent expansions in an emergent novel drug delivery technology: Emulgel. J. Control. Release 2013, 171, 122–132. [Google Scholar]
- Jose, A.; Mandapalli, P.K.; Venuganti, V.V. Liposomal hydrogel formulation for transdermal delivery of pirfenidone. J. Liposome Res. 2016, 26, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Rajan, R.; Jose, S.; Mukund, V.P.B.; Vasudevan, D.T. Transferosomes—A vesicular transdermal delivery system for enhanced drug permeation. J. Adv. Pharm. Technol. Res. 2011, 2, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Jeong, B.; Kim, S.W.; Bae, Y.H. Thermosensitive sol–gel reversible hydrogels. Adv. Drug Deliv. Rev. 2012, 64, 154–162. [Google Scholar] [CrossRef]
- Li, Y.; Rodrigues, J.; Tomas, H. Injectable and biodegradable hydrogels: Gelation, biodegradation and biomedical applications. Chem. Soc. Rev. 2012, 41, 2193–2221. [Google Scholar] [CrossRef] [PubMed]
- Buwalda, S.J.; Boere, K.W.; Dijkstra, P.J.; Feijen, J.; Vermonden, T.; Hennink, W.E. Hydrogels in a historical perspective: From simple networks to smart materials. J. Control. Release 2014, 190, 254–273. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, E.M. Hydrogel: Preparation, characterization, and applications: A review. J. Adv. Res. 2015, 6, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Moreno, E.; Fernandez, C.; Navarro-Blasco, I.; Nguewa, P.A.; Palop, J.A.; Irache, J.M.; Sanmartin, C.; Espuelas, S. Topical treatment of L. major infected BALB/c mice with a novel diselenide chitosan hydrogel formulation. Eur. J. Pharm. Sci. 2014, 62, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.S.; Kong, B.J.; Park, S.N. Physicochemical properties of pH-sensitive hydrogels based on hydroxyethyl cellulose–hyaluronic acid and for applications as transdermal delivery systems for skin lesions. Eur. J. Pharm. Biopharm. 2015, 92, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Kabanov, A.V.; Vinogradov, S.V. Nanogels as pharmaceutical carriers: Finite networks of infinite capabilities. Angew. Chem. Int. Ed. Engl. 2009, 48, 5418–5429. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, C.; Pereira, P.; Gama, M. Self-assembled hydrogel nanoparticles for drug delivery applications. Materials 2010, 3, 1420–1460. [Google Scholar] [CrossRef]
- Mavuso, S.; Marimuthu, T.; Choonara, Y.E.; Kumar, P.; Toit, L.C.D.; Pillay, V. A review of polymeric colloidal nanogels in transdermal drug delivery. Curr. Pharm. Des. 2015, 21, 2801–2813. [Google Scholar] [CrossRef] [PubMed]
- Panyam, J.; Sahoo, S.K.; Prabha, S.; Bargar, T.; Labhasetwar, V. Fluorescence and electron microscopy probes for cellular and tissue uptake of poly(d,l-lactide-co-glycolide) nanoparticles. Int. J. Pharm. 2003, 262, 1–11. [Google Scholar] [CrossRef]
- Sultana, S.S.; Parveen, P.; Rekha, M.S.; Deepthi, K.; Sowjanya, C.; Devi, A.S. Emulgel-a novel surrogate approach for transdermal drug delivery system. Ind. Am. J. Pharm. Res. 2014, 4, 5250–5265. [Google Scholar]
- Naga Sravan Kumar Varma, V.; Maheshwari, P.V.; Navya, M.; Reddy, S.C.; Shivakumar, H.G.; Gowda, D.V. Calcipotriol delivery into the skin as emulgel for effective permeation. Saudi Pharm. J. 2014, 22, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Jeengar, M.K.; Rompicharla, S.V.; Shrivastava, S.; Chella, N.; Shastri, N.R.; Naidu, V.G.; Sistla, R. Emu oil based nano-emulgel for topical delivery of curcumin. Int. J. Pharm. 2016, 506, 222–236. [Google Scholar] [CrossRef] [PubMed]
- Khullar, R.; Kumar, D.; Seth, N.; Saini, S. Formulation and evaluation of mefenamic acid emulgel for topical delivery. Saudi Pharm. J. 2012, 20, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Carafa, M.; Marianecci, C.; di Marzio, L.; Rinaldi, F.; Meo, C.; Matricardi, P.; Alhaique, F.; Coviello, T. A new vesicle-loaded hydrogel system suitable for topical applications: Preparation and characterization. J. Pharm. Pharm. Sci. 2011, 14, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Escobar-Chávez, J.J. Nanocarriers for transdermal drug delivery. Skin 2012, 19, 3–17. [Google Scholar] [CrossRef]
- Hubbell, J.A.; Chilkoti, A. Nanomaterials for drug delivery. Science 2012, 337, 303–305. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types | Examples | References |
|---|---|---|
| Metal nanoparticles | titania nanoparticle | [59] |
| silver nanoparticle | [60,61] | |
| zinc oxide nanoparticle | [62,63] | |
| copper nanoparticles | [62,64] | |
| Organic antibacterials | citric acid | [65] |
| citrus grandis osbeck extract | [66,67] |
| Herbs Formula | Ingredients | References |
|---|---|---|
| Huangbai Zicao Diyu cream | Cortex phellodendri 50 g; Radix arnebiae 50 g; Radix sanguisorbae 100 g | [81] |
| Huanglian Qingdai ointment | Rhizoma coptidis 0.6 g; Indigo naturalis 0.3 g; Cortex phellodendri 0.3 g; Alum 0.3 g; Borneolum syntheticum; Urea cream 40 g | [81] |
| Xiao-Feng-San (XFS) | Radix saposhnikovia 2.5 mg; Herba schizonepetae 2.5 mg; Radix angelicae sinensis 2.5 mg; Radix rehmanniae 2.5 mg; Radix sophorae flavescentis 2.5 mg; Rhizoma atractylodis 2.5 mg; Periostracum cicdae 2.5 mg; Linum usitatissimum 2.5 mg; Rhizoma anemarrhenae 2.5 mg; Gypsum fibrosum 2.5 mg; Caulis clematidis armandii 1.25 mg; Radix glycyrrhizae 1.25 mg; Fructus arctii 2.5 mg | [81,82] |
| TCHM capsules | Flos lonicerae 2 g; Herba menthae 1 g; Cortex moutan 2 g; Rhizoma atractylodis 2 g; Cortex phellodendri 2 g | [83,84] |
| Byakkokaninjinto | Gypsum fibrosum; Anemarrhenae rhizome; Glycyrrhizae radix; Ginseng radix; Oryzae fructus | [85,86] |
| Juzen-Taiho-to | Astragali Radix; Cinnamomi Cortex, Rehmanniae Radix; Paeoniae Radix; Cnidii Rhizoma; Atractylodis Lanceae Rhizoma; Angelicae Radix; Ginseng Radix; Hoelen; Glycyrrhizae Radix | [85,87] |
| Keishibukuryogan | Cinnamomi cortex; Paeoniae Radix; Moutan cortex; Persicae semen; Hoelen | [85,88] |
| Gami-Cheongyeul-Sodok-Eum | Angelica gigas; Astragalus membranaceus; Atractylodes japonica; Coptis japonica; Forsythia virdissima; Glycyrrhiza uralensis; Lonicera japonica; Portulaca oleracea; Scutellaria baicalensis | [89] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Hui, P.C.L.; Kan, C.-W. Functionalized Textile Based Therapy for the Treatment of Atopic Dermatitis. Coatings 2017, 7, 82. https://doi.org/10.3390/coatings7060082
Wang W, Hui PCL, Kan C-W. Functionalized Textile Based Therapy for the Treatment of Atopic Dermatitis. Coatings. 2017; 7(6):82. https://doi.org/10.3390/coatings7060082
Chicago/Turabian StyleWang, Wenyi, Patrick C. L. Hui, and Chi-Wai Kan. 2017. "Functionalized Textile Based Therapy for the Treatment of Atopic Dermatitis" Coatings 7, no. 6: 82. https://doi.org/10.3390/coatings7060082
APA StyleWang, W., Hui, P. C. L., & Kan, C. -W. (2017). Functionalized Textile Based Therapy for the Treatment of Atopic Dermatitis. Coatings, 7(6), 82. https://doi.org/10.3390/coatings7060082