Relationship between Muscle Mass and Non-Alcoholic Fatty Liver Disease


Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. General Characteristics of the Study Population
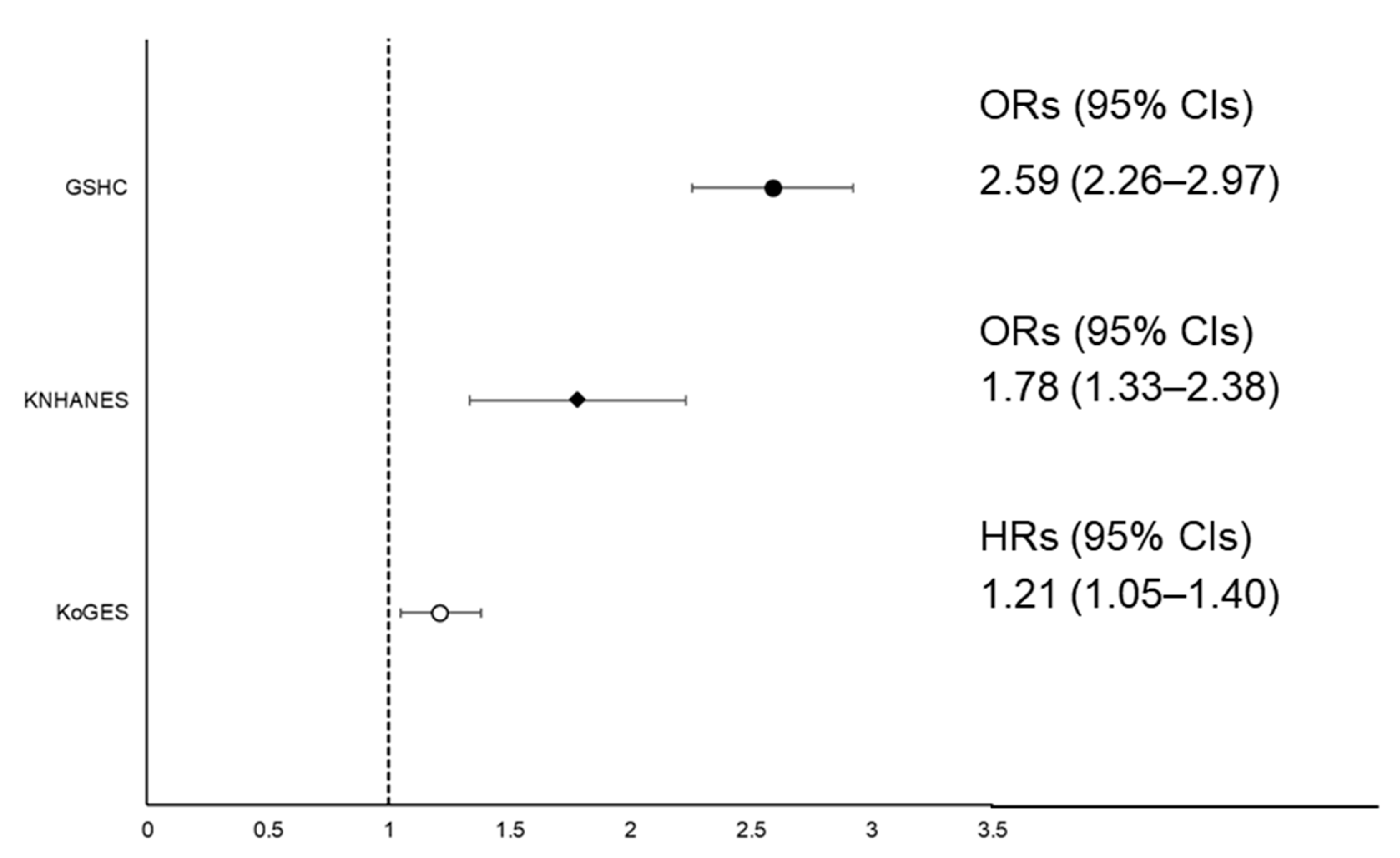
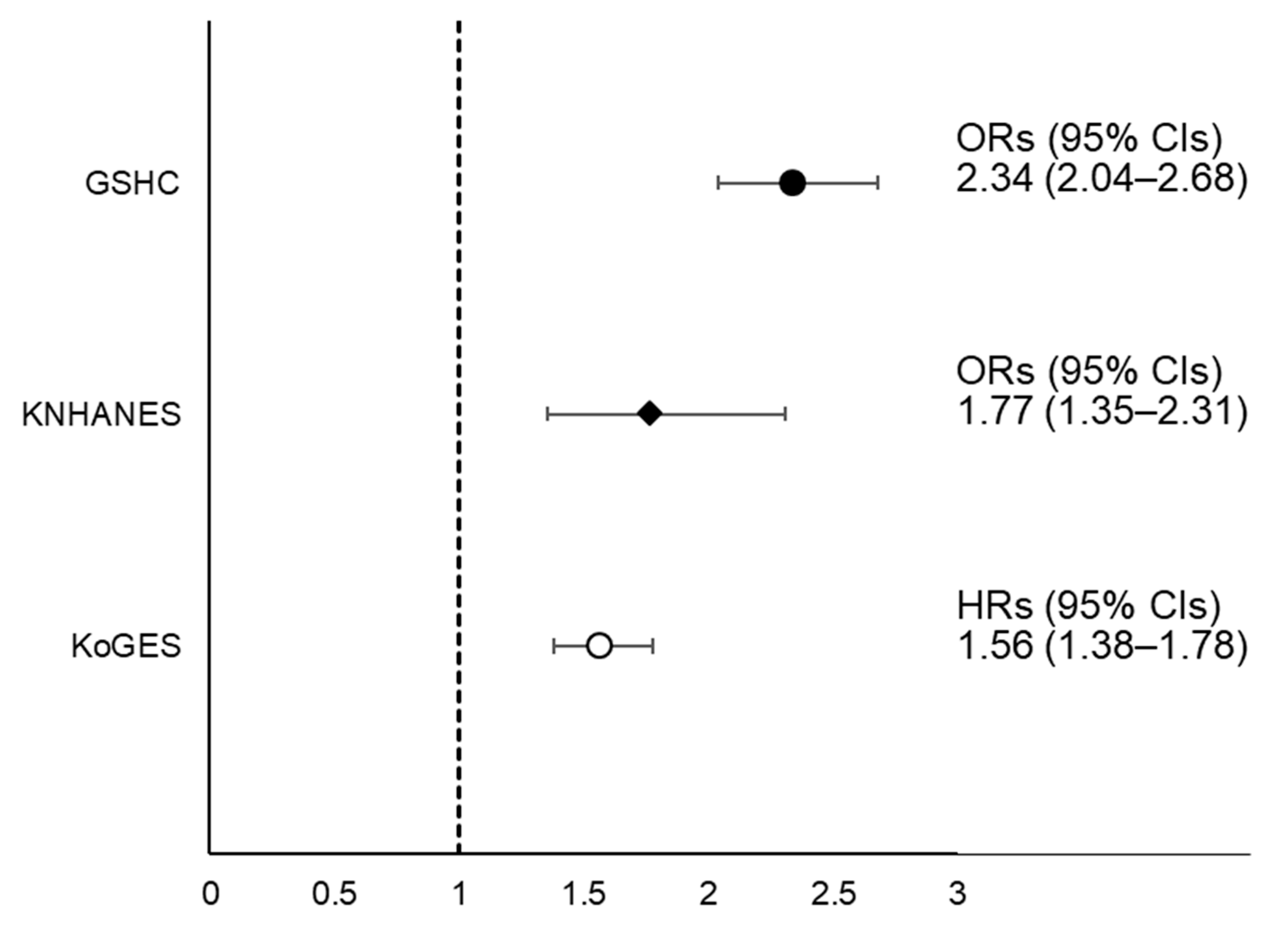
2.2. Relationship between SMI and NAFLD
2.3. Longitudinal Changes in SMI According to NAFLD
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Assessment of Body Composition
4.3. Assessment of NAFLD
4.4. Covariates
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NAFLD | Non-alcoholic fatty liver disease |
| WC | Waist circumference |
| BMI | Body mass index |
| MBP | Mean blood pressure |
| AST | Aspartate aminotransferase |
| ALT | Alanine aminotransferase |
| BEE | Basal energy expenditure |
| HDL | High-density lipoprotein |
| CVD | Cardiovascular disease |
| GSHC | Gangnam Severance Hospital Check-up |
| KNHANES | Korean National Health and Nutrition Examination Survey |
| KoGES | Korean Genome and Epidemiology Study |
| SMI | Skeletal muscle mass index |
| LSMI | Low skeletal muscle mass index |
| LDL | Low-density lipoprotein |
| HRs | Hazard ratios |
| CIs | Confidence intervals |
| SD | Standard deviations |
| ORs | Odds ratios |
| EI/BEE | Ratio of energy intake/basal energy expenditure |
| LECT2 | Leukocyte cell-derived chemotaxin 2 |
| HSP | Hepassocin |
| EGFR/JNK | Epidermal growth factor receptor/c-Jun N-terminal kinase |
| BIA | Bioelectrical impedance analysis |
| DXA | Dual energy X-ray absorptiometry |
| IRB | Institutional Review Boards |
| TSM | Total skeletal muscle mass |
| ASM | Appendicular skeletal muscle mass |
| FNIH | Foundation for the National Institutes of Health |
| SBP | Systolic blood pressure |
| DBP | Diastolic blood pressure |
| FFQ | Food frequency questionnaire |
| SE | Standard error |
References
- Haga, Y.; Kanda, T.; Sasaki, R.; Nakamura, M.; Nakamoto, S.; Yokosuka, O. Nonalcoholic fatty liver disease and hepatic cirrhosis: Comparison with viral hepatitis-associated steatosis. World J. Gastroenterol. 2015, 21, 12989–12995. [Google Scholar] [CrossRef]
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the american association for the study of liver diseases, american college of gastroenterology, and the american gastroenterological association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef]
- Park, S.H.; Jeon, W.K.; Kim, S.H.; Kim, H.J.; Park, D.I.; Cho, Y.K.; Sung, I.K.; Sohn, C.I.; Keum, D.K.; Kim, B.I. Prevalence and risk factors of non-alcoholic fatty liver disease among korean adults. J. Gastroenterol. Hepatol. 2006, 21, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Korean Association for the Study of the Liver. KASL clinical practice guidelines: Management of nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2013, 19, 325–348. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the american association for the study of liver diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of The Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. Easl-easd-easo clinical practice guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Palikaras, K.; Mari, M.; Petanidou, B.; Pasparaki, A.; Filippidis, G.; Tavernarakis, N. Ectopic fat deposition contributes to age-associated pathology in caenorhabditis elegans. J. Lipid Res. 2017, 58, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Byrne, C.D.; Targher, G. Ectopic fat, insulin resistance, and nonalcoholic fatty liver disease: Implications for cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1155–1161. [Google Scholar] [CrossRef] [Green Version]
- Wijarnpreecha, K.; Panjawatanan, P.; Aby, E.; Ahmed, A.; Kim, D. Nonalcoholic fatty liver disease in the over-60 s: Impact of sarcopenia and obesity. Maturitas 2019, 124, 48–54. [Google Scholar] [CrossRef]
- Lee, M.J.; Kim, E.H.; Bae, S.J.; Kim, G.A.; Park, S.W.; Choe, J.; Jung, C.H.; Lee, W.J.; Kim, H.K. Age-related decrease in skeletal muscle mass is an independent risk factor for incident nonalcoholic fatty liver disease: A 10-year retrospective cohort study. Gut Liver 2019, 13, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.B.; Ahn, C.W.; Lee, B.K.; Kang, S.; Nam, J.S.; You, J.H.; Kim, M.J.; Kim, M.K.; Park, J.S. Association between triglyceride glucose index and arterial stiffness in korean adults. Cardiovasc. Diabetol. 2018, 17, 41. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.H.; Jung, K.S.; Kim, S.U.; Yoon, H.J.; Yun, Y.J.; Lee, B.W.; Kang, E.S.; Han, K.H.; Lee, H.C.; Cha, B.S. Sarcopaenia is associated with nafld independently of obesity and insulin resistance: Nationwide surveys (knhanes 2008–2011). J. Hepatol. 2015, 63, 486–493. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Kim, D.; Raymond, P.; Scribani, M.; Ahmed, A. Associations between sarcopenia and nonalcoholic fatty liver disease and advanced fibrosis in the USA. Eur J. Gastroenterol. Hepatol. 2019, 31, 1121–1128. [Google Scholar] [CrossRef]
- Brown, J.C.; Harhay, M.O.; Harhay, M.N. Sarcopenia and mortality among a population-based sample of community-dwelling older adults. J. Cachexia Sarcopenia Muscle 2016, 7, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Sobestiansky, S.; Michaelsson, K.; Cederholm, T. Sarcopenia prevalence and associations with mortality and hospitalisation by various sarcopenia definitions in 85–89 year old community-dwelling men: A report from the ulsam study. BMC Geriatr. 2019, 19, 318. [Google Scholar] [CrossRef] [PubMed]
- De Bandt, J.P.; Jegatheesan, P.; Tennoune-El-Hafaia, N. Muscle loss in chronic liver diseases: The example of nonalcoholic liver disease. Nutrients 2018, 10, 1195. [Google Scholar] [CrossRef] [Green Version]
- Zhai, Y.; Xiao, Q.; Miao, J. The relationship between nafld and sarcopenia in elderly patients. Can. J. Gastroenterol. Hepatol. 2018, 2018, 5016091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, T.C.; Wu, L.W.; Chen, W.L.; Liaw, F.Y.; Chang, Y.W.; Kao, T.W. Nonalcoholic fatty liver disease and sarcopenia in a western population (nhanes iii): The importance of sarcopenia definition. Clin. Nutr. 2019, 38, 422–428. [Google Scholar] [CrossRef]
- Li, A.A.; Kim, D.; Ahmed, A. Association of sarcopenia and nafld: An overview. Clin. Liver Dis. 2020, 16, 73–76. [Google Scholar] [CrossRef]
- Lan, F.; Misu, H.; Chikamoto, K.; Takayama, H.; Kikuchi, A.; Mohri, K.; Takata, N.; Hayashi, H.; Matsuzawa-Nagata, N.; Takeshita, Y.; et al. Lect2 functions as a hepatokine that links obesity to skeletal muscle insulin resistance. Diabetes 2014, 63, 1649–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, T.W.; Chung, Y.H.; Kim, H.C.; Abd El-Aty, A.M.; Jeong, J.H. Hyperlipidemia-induced hepassocin in the liver contributes to insulin resistance in skeletal muscle. Mol. Cell. Endocrinol. 2018, 470, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Elsen, M.; Raschke, S.; Eckel, J. Browning of white fat: Does irisin play a role in humans? J. Endocrinol. 2014, 222, R25–R38. [Google Scholar] [CrossRef] [Green Version]
- Tang, H.; Yu, R.; Liu, S.; Huwatibieke, B.; Li, Z.; Zhang, W. Irisin inhibits hepatic cholesterol synthesis via ampk-srebp2 signaling. EBioMedicine 2016, 6, 139–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, K.S. Recent epidemiologic changes of acute and chronic hepatitis in Korea. J. Korean Med. Assoc. 2005, 48, 423–427. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Han, B.G.; KoGES Group. Cohort profile: The Korean genome and epidemiology study (koges) consortium. Int J. Epidemiol 2017, 46, e20. [Google Scholar] [CrossRef]
- Lee, S.Y.; Park, H.S.; Kim, D.J.; Han, J.H.; Kim, S.M.; Cho, G.J.; Kim, D.Y.; Kwon, H.S.; Kim, S.R.; Lee, C.B.; et al. Appropriate waist circumference cutoff points for central obesity in korean adults. Diabetes Res. Clin. Pract. 2007, 75, 72–80. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in asia: Consensus report of the asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Heymsfield, S.B. Bioelectrical impedance analysis in the assessment of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 366–374. [Google Scholar] [CrossRef]
- Meng, N.H.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Lin, C.H.; Chang, C.K.; Li, T.C.; Lin, C.C. Sarcopenia defined by combining height- and weight-adjusted skeletal muscle indices is closely associated with poor physical performance. J. Aging Phys. Act. 2015, 23, 597–606. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The fnih sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstrale, M.; Groop, L.; et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. Dietary Reference Intakes for Koreans 2015; Ministry of Health and Welfare: Sejong, Korea, 2015.
- Cho, Y.J.; Lim, Y.-H.; Yun, J.M.; Yoon, H.-J.; Park, M. Sex- and age-specific effects of energy intake and physical activity on sarcopenia. Sci. Rep. 2020, 10, 9822. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2016–2019 Gangnam Severance Hospital Check-Up | 2008–2010 KNHANES | KoGES: Ansan-Ansung Study | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Normal | NAFLD | p * | Normal | NAFLD | p† | Normal | NAFLD | p * |
| N | 5523 | 4168 | 6343 | 1977 | 3579 | 1008 | |||
| Male sex, % | 37.6 | 65.5 | <0.001 | 37.9 | 49.6 | <0.001 | 40.9 | 47.2 | <0.001 |
| Age, years | 47.4 ± 13.1 | 51.2 ± 11.5 | <0.001 | 47.3 ± 0.4 | 51.0 ± 0.6 | <0.001 | 50.0 ± 8.3 | 52.3 ± 8.4 | <0.001 |
| Abdominal obesity, % | 11.4 | 47.6 | <0.001 | 17.5 | 45.3 | <0.001 | 13.0 | 55.2 | <0.001 |
| Waist circumference, cm | 76.7 ± 9.3 | 88.2 ± 9.6 | <0.001 | 78.6 ± 0.2 | 87.0 ± 0.3 | <0.001 | 78.7 ± 7.7 | 87.7 ± 7.6 | <0.001 |
| BMI, kg/m2 | 22.5 ± 3.0 | 26.1 ± 3.5 | <0.001 | 22.9 ± 0.1 | 25.6 ± 0.1 | <0.001 | 23.5 ± 2.6 | 26.0 ± 2.7 | <0.001 |
| Mean blood pressure, mmHg | 86.6 ± 8.8 | 89.7 ± 9.2 | <0.001 | 89.6 ± 0.3 | 94.5 ± 0.4 | <0.001 | 89.8 ± 12.2 | 98.5 ± 11.7 | <0.001 |
| Basal energy expenditure, kcal/day | 1340.9 ± 209.1 | 1484.2 ± 227.3 | <0.001 | 1333.3 ± 3.5 | 1421.8 ± 7.6 | <0.001 | 1356.4 ± 179.1 | 1452.4 ± 207.9 | <0.001 |
| Fasting glucose, mg/dL | 94.5 ± 13.7 | 106.7 ± 25.9 | <0.001 | 93.8 ± 0.3 | 109.0 ± 1.0 | <0.001 | 82.5 ± 11.9 | 97.4 ± 32.3 | <0.001 |
| Fasting insulin, μIU/mL | - | - | - | 8.5 ± 0.1 | 14.1 ± 0.2 | <0.001 | 6.5 ± 2.7 | 10.7 ± 7.7 | <0.001 |
| Total cholesterol, mg/dL | 201.8 ± 36.3 | 208.3 ± 41.2 | <0.001 | 185.6 ± 0.6 | 193.4 ± 1.2 | <0.001 | 187.3 ± 33.6 | 201.0 ± 36.4 | <0.001 |
| Triglyceride, mg/dL | 88 (67, 120) | 141 (102, 197) | <0.001 | 115.1 ± 1.4 | 172.6 ± 4.0 | <0.001 | 115 (89, 151) | 191 (150, 258) | <0.001 |
| HDL cholesterol, mg/dL | 61.1 ± 13.3 | 51.6 ± 11.3 | <0.001 | 49.3 ± 0.2 | 44.2 ± 0.3 | <0.001 | 46.3 ± 9.9 | 39.6 ± 7.9 | <0.001 |
| LDL cholesterol, mg/dL | 126.0 ± 29.6 | 135.7 ± 32.6 | <0.001 | 113.4 ± 0.6 | 114.7 ± 1.1 | 0.306 | 115.1 ± 30.4 | 119.8 ± 33.0 | <0.001 |
| AST, IU/L | 24 (20, 30) | 27 (22, 35) | <0.001 | 19.8 ± 0.1 | 29.9 ± 0.8 | <0.001 | 25 (22, 29) | 29 (24, 36) | <0.001 |
| ALT, IU/L | 18 (13, 25) | 29 (20, 41) | <0.001 | 17.2 ± 0.1 | 36.2 ± 0.8 | <0.001 | 20 (16, 26) | 31 (24, 45) | <0.001 |
| Current smoker, % | 13.3 | 22.7 | <0.001 | 18.7 | 22.7 | 0.008 | 21.0 | 24.0 | 0.045 |
| Current drinker, % | 60.9 | 63.9 | 0.002 | 52.3 | 51.1 | 0.474 | 44.6 | 42.3 | 0.195 |
| Regular exercise, % | 23.8 | 25.6 | 0.043 | 23.6 | 20.4 | 0.028 | 52.1 | 49.8 | 0.193 |
| Daily caloric intake, kcal/day | - | - | - | 1855.5 ± 14.9 | 1889.4 ± 27.4 | 0.225 | 1842.8 (1539.9, 2194.0) | 1881.1 (1577.5, 2291.0) | 0.003 |
| Daily protein intake, g/day | - | - | - | 67.0 ± 0.8 | 68.8 ± 1.2 | 0.171 | 62.4 (48.4, 78.0) | 63.9 (50.3, 79.8) | 0.057 |
| Daily fat intake, g/day | - | - | - | 36.4 ± 0.6 | 37.5 ± 1.2 | 0.323 | 29.9 (20.1, 41.1) | 29.8 (19.7, 41.7) | 0.579 |
| Daily CHO intake, g/day | - | - | - | 308.2 ± 2.4 | 312.1 ± 4.2 | 0.380 | 322.7 (277.8, 375.1) | 331.0 (288.1, 397.2) | <0.001 |
| Skeletal muscle index | 1.866 ± 0.352 | 1.845 ± 0.356 | 0.005 | 0.751 ± 0.003 | 0.744 ± 0.006 | 0.308 | 1.828 ± 0.312 | 1.794 ± 0.305 | 0.002 |
| NAFLD liver fat score | - | - | - | −1.819 ± 0.127 | 0.368 ± 0.036 | <0.001 | −1.951 ± 0.638 | 0.479 ± 1.606 | <0.001 |
| LSMI, % | 11.8 | 30.9 | <0.001 | 8.4 | 15.7 | <0.001 | - | - | - |
| History of CVD, % | 4.4 | 5.7 | 0.002 | 3.0 | 5.2 | 0.001 | 2.1 | 3.3 | 0.046 |
| 2016–2019 Gangnam Severance Hospital Check-Up | 2008–2010 KNHANES | KoGES: Ansan-Ansung Study | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Normal | LSMI | p * | Normal | LSMI | p† | Normal | LSMI | p * |
| N | 7753 | 1938 | 7412 | 908 | 3405 | 831 | |||
| Male sex, % | 49.6 | 49.7 | 0.939 | 40.3 | 41.9 | 0.487 | 41.7 | 42.8 | 0.562 |
| Age, years | 47.5 ± 12.1 | 55.5 ± 12.3 | <0.001 | 45.6 ± 0.4 | 62.0 ± 0.8 | <0.001 | 49.9 ± 8.3 | 55.1 ± 8.8 | <0.001 |
| Abdominal obesity, % | 19.3 | 57.9 | <0.001 | 21.1 | 47.3 | <0.001 | 12.2 | 30.3 | <0.001 |
| Waist circumference, cm | 79.7 ± 10.2 | 89.4 ± 10.7 | <0.001 | 79.7 ± 0.2 | 86.8 ± 0.6 | <0.001 | 78.6 ± 7.6 | 83.8 ± 8.0 | <0.001 |
| BMI, kg/m2 | 23.2 ± 3.1 | 27.6 ± 3.9 | <0.001 | 23.3 ± 0.1 | 25.8 ± 0.2 | <0.001 | 23.4 ± 2.5 | 25.9 ± 3.0 | <0.001 |
| Mean blood pressure, mmHg | 87.5 ± 8.9 | 90.0 ± 9.4 | <0.001 | 90.1 ± 0.3 | 95.6 ± 0.6 | <0.001 | 89.8 ± 12.2 | 94.1 ± 12.6 | <0.001 |
| Basal energy expenditure, kcal/day | 1413.7 ± 229.8 | 1357.8 ± 217.3 | <0.001 | 1362.4 ± 3.7 | 1268.3 ± 7.4 | <0.001 | 1359.2 ± 179.8 | 1314.1 ± 167.0 | <0.001 |
| Fasting glucose, mg/dL | 97.9 ± 18.6 | 107.1 ± 26.7 | <0.001 | 96.3 ± 0.3 | 105.2 ± 1.3 | <0.001 | 82.4 ± 11.6 | 83.3 ± 12.7 | 0.057 |
| Fasting insulin, μIU/mL | - | - | - | 9.6 ± 0.1 | 11.1 ± 0.3 | <0.001 | 6.4 ± 2.7 | 6.5 ± 2.8 | 0.914 |
| Total cholesterol, mg/dL | 203.5 ± 37.8 | 208.9 ± 41.4 | <0.001 | 186.4 ± 0.6 | 196.0 ± 1.8 | <0.001 | 186.9 ± 33.7 | 195.9 ± 34.1 | <0.001 |
| Triglyceride, mg/dL | 102 (73, 146) | 130 (94, 181) | <0.001 | 123.9 ± 1.5 | 163.1 ± 4.9 | <0.001 | 115 (89, 150) | 133 (102, 179) | <0.001 |
| HDL-cholesterol, mg/dL | 57.9 ± 13.5 | 53.4 ± 11.9 | <0.001 | 48.4 ± 0.2 | 45.4 ± 0.5 | <0.001 | 46.3 ± 10.0 | 45.1 ± 9.8 | <0.001 |
| LDL-cholesterol, mg/dL | 128.9 ± 30.7 | 135.4 ± 33.2 | <0.001 | 113.2 ± 0.5 | 118.0 ± 1.7 | 0.007 | 114.7 ± 30.4 | 121.2 ± 31.8 | <0.001 |
| AST, IU/L | 24 (20, 31) | 28 (23, 36) | <0.001 | 21.8 ± 0.2 | 23.9 ± 0.5 | <0.001 | 25 (22, 29) | 26 (23, 30) | <0.001 |
| ALT, IU/L | 20 (14, 30) | 27 (19, 41) | <0.001 | 21.1 ± 0.3 | 23.7 ± 0.8 | 0.002 | 19 (16, 26) | 21 (18, 28) | <0.001 |
| Current smoker, % | 17.7 | 15.7 | 0.038 | 19.9 | 16.2 | 0.091 | 21.4 | 17.4 | 0.011 |
| Current drinker, % | 64.6 | 52.4 | <0.001 | 53.2 | 41.6 | <0.001 | 45.0 | 39.0 | 0.002 |
| Regular exercise, % | 23.7 | 28.0 | <0.001 | 23.3 | 19.0 | 0.049 | 52.2 | 48.7 | 0.071 |
| Daily caloric intake, kcal/day | - | - | - | 1888.6 ± 14.8 | 1646.1 ± 33.3 | <0.001 | 1851.7 (1546.3, 2200.9) | 1772.2 (1460.2, 2137.1) | 0.001 |
| Daily protein intake, g/day | - | - | - | 68.7 ± 0.7 | 57.1 ± 1.5 | <0.001 | 62.6 (48.7, 78.0) | 57.5 (44.7, 74.6) | <0.001 |
| Daily fat intake, g/day | - | - | - | 37.7 ± 0.6 | 27.3 ± 1.3 | <0.001 | 30.0 (14.2, 41.2) | 25.8 (17.0, 37.8) | <0.001 |
| Daily CHO intake, g/day | - | - | - | 311.7 ± 2.3 | 286.6 ± 5.6 | <0.001 | 323.8 (278.1, 376.3) | 315.9 (275.4, 375.6) | 0.252 |
| Skeletal muscle index | 1.938 ± 0.324 | 1.530 ± 0.271 | <0.001 | 0.768 ± 0.003 | 0.581 ± 0.007 | <0.001 | 1.842 ± 0.309 | 1.519 ± 0.254 | <0.001 |
| NAFLD liver fat score | - | - | - | −1.381 ± 0.021 | −0.9110 ± 0.064 | <0.001 | −1.958 ± 0.636 | −1.747 ± 0.648 | <0.001 |
| NAFLD, % | 37.1 | 66.5 | <0.001 | 20.8 | 34.7 | <0.001 | - | - | - |
| History of CVD, % | 4.2 | 7.8 | <0.001 | 2.7 | 10.5 | <0.001 | 2.1 | 3.1 | 0.081 |
| 2016–2019 Gangnam Severance Hospital Check-Up | Normal SMI without Abdominal Obesity | LSMI without Abdominal Obesity | Normal SMI with Abdominal Obesity | LSMI with Abdominal Obesity | |
|---|---|---|---|---|---|
| ORs (95% CIs) | p | ||||
| Unadjusted | 1 (reference) | 2.57 (2.22–2.99) | 7.16 (6.29–8.14) | 9.22 (7.90–10.75) | <0.001 |
| Model 1 * | 1 (reference) | 3.17 (2.70–3.73) | 3.57 (3.08–4.14) | 6.87 (5.85–8.07) | <0.001 |
| Model 2 | 1 (reference) | 2.76 (2.34–3.27) | 3.14 (2.70–3.66) | 5.67 (4.80–6.69) | <0.001 |
| 2008–2010 KNHANES | Normal SMI without abdominal obesity | LSMI without abdominal obesity | Normal SMI with abdominal obesity | LSMI with abdominal obesity | |
| ORs (95% CIs) | p | ||||
| Unadjusted | 1 (reference) | 1.78 (1.29–2.45) | 3.90 (3.30–4.62) | 4.89 (3.64–6.56) | <0.001 |
| Model 1 | 1 (reference) | 1.85 (1.24–2.75) | 1.60 (1.25–2.06) | 2.97 (2.12–4.18) | <0.001 |
| Model 2 | 1 (reference) | 1.67 (1.08–2.56) | 1.42 (1.10–1.83) | 2.63 (1.87–3.71) | <0.001 |
| KoGES: Ansan-Ansung study | Normal SMI without abdominal obesity | LSMI without abdominal obesity | Normal SMI with abdominal obesity | LSMI with abdominal obesity | |
| HRs (95% CIs) | p | ||||
| Unadjusted | 1 (reference) | 1.60 (1.39–1.84) | 2.15 (1.85–2.49) | 3.19 (2.70–3.77) | <0.001 |
| Model 1 | 1 (reference) | 1.72 (1.48–2.00) | 1.43 (1.21–1.70) | 2.21 (1.84–2.67) | <0.001 |
| Model 2 | 1 (reference) | 1.57 (1.35–1.83) | 1.39 (1.18–1.65) | 2.15 (1.79–2.60) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Lee, H.-S.; Lee, B.-K.; Kwon, Y.-J.; Lee, J.-W. Relationship between Muscle Mass and Non-Alcoholic Fatty Liver Disease. Biology 2021, 10, 122. https://doi.org/10.3390/biology10020122
Lee J-H, Lee H-S, Lee B-K, Kwon Y-J, Lee J-W. Relationship between Muscle Mass and Non-Alcoholic Fatty Liver Disease. Biology. 2021; 10(2):122. https://doi.org/10.3390/biology10020122
Chicago/Turabian StyleLee, Jun-Hyuk, Hye-Sun Lee, Byoung-Kwon Lee, Yu-Jin Kwon, and Ji-Won Lee. 2021. "Relationship between Muscle Mass and Non-Alcoholic Fatty Liver Disease" Biology 10, no. 2: 122. https://doi.org/10.3390/biology10020122