
Effects of Resistance Circuit-Based Training on Body Composition, Strength and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis

 ,
,  ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Sources and Search Profile
2.3. Selection Criteria
2.4. Study Selection and Data Extraction
2.5. Outcomes
2.6. Risk of Bias Assessment (Study Quality)
2.7. Data Synthesis and Statistical Analysis
2.8. Effects of Moderator Variables: Meta-Regression and Sub-Analysis
3. Results
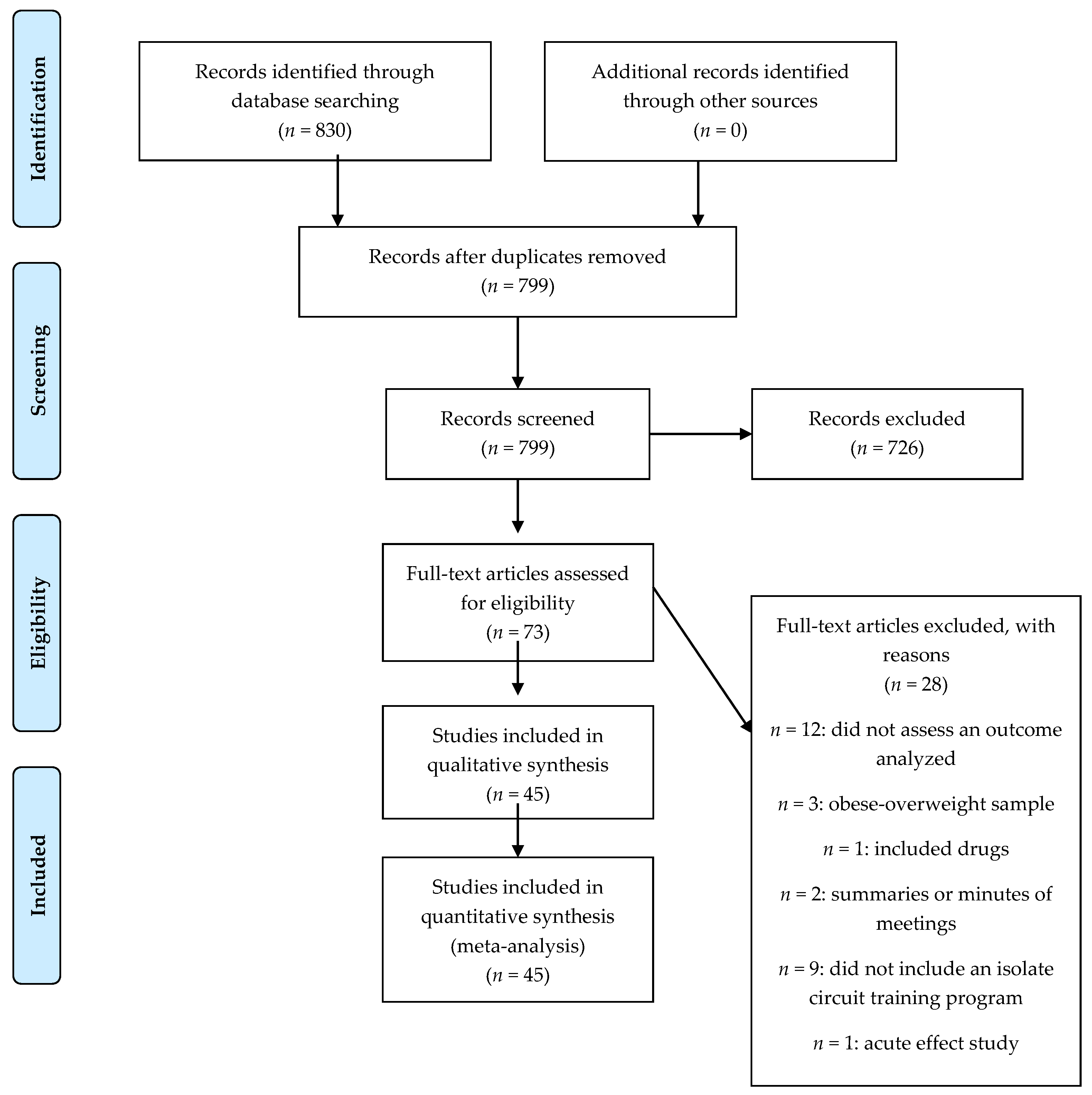
3.1. Search Results and Characteristics of Included Studies
3.2. Participants and CT Characteristics
3.3. Quality of Studies: Publication Bias
3.4. Meta-Analysis
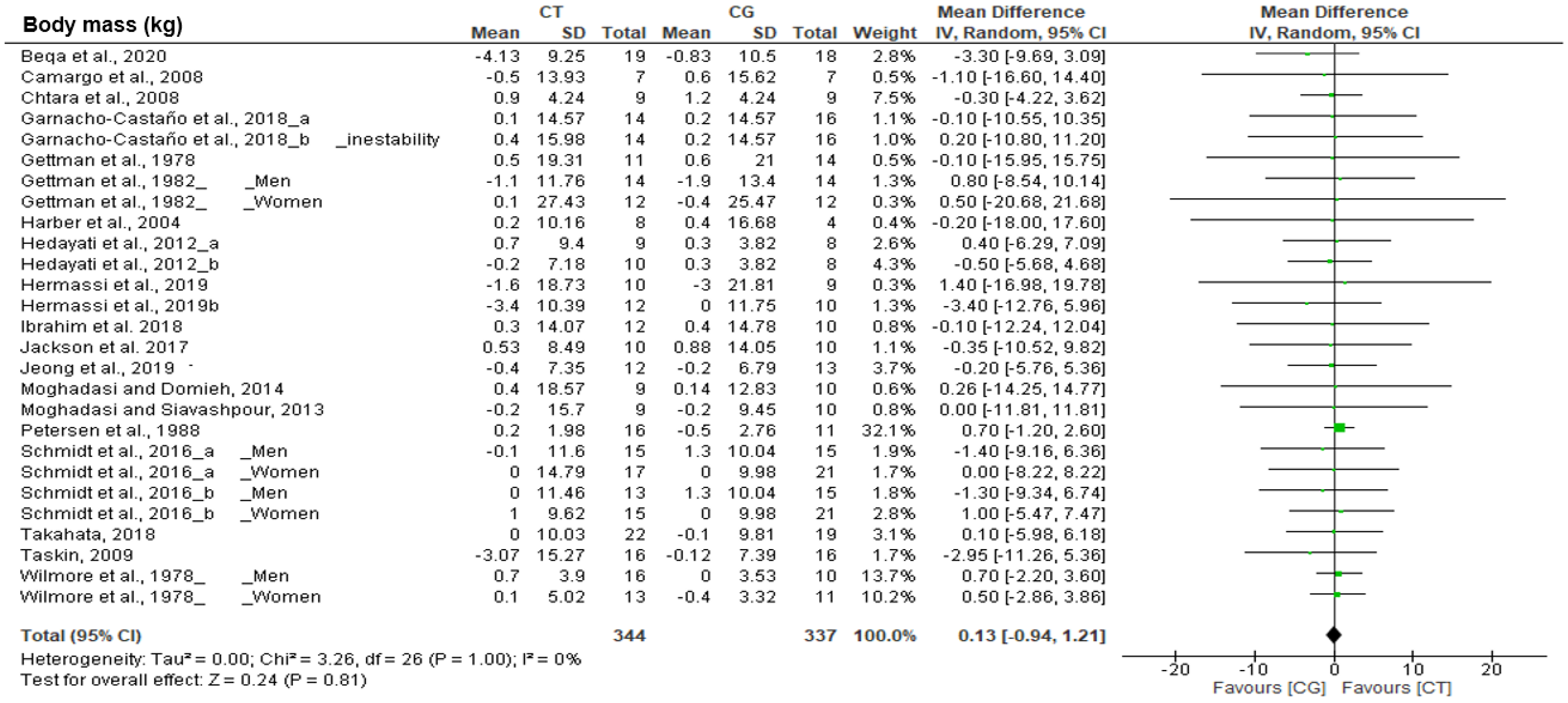
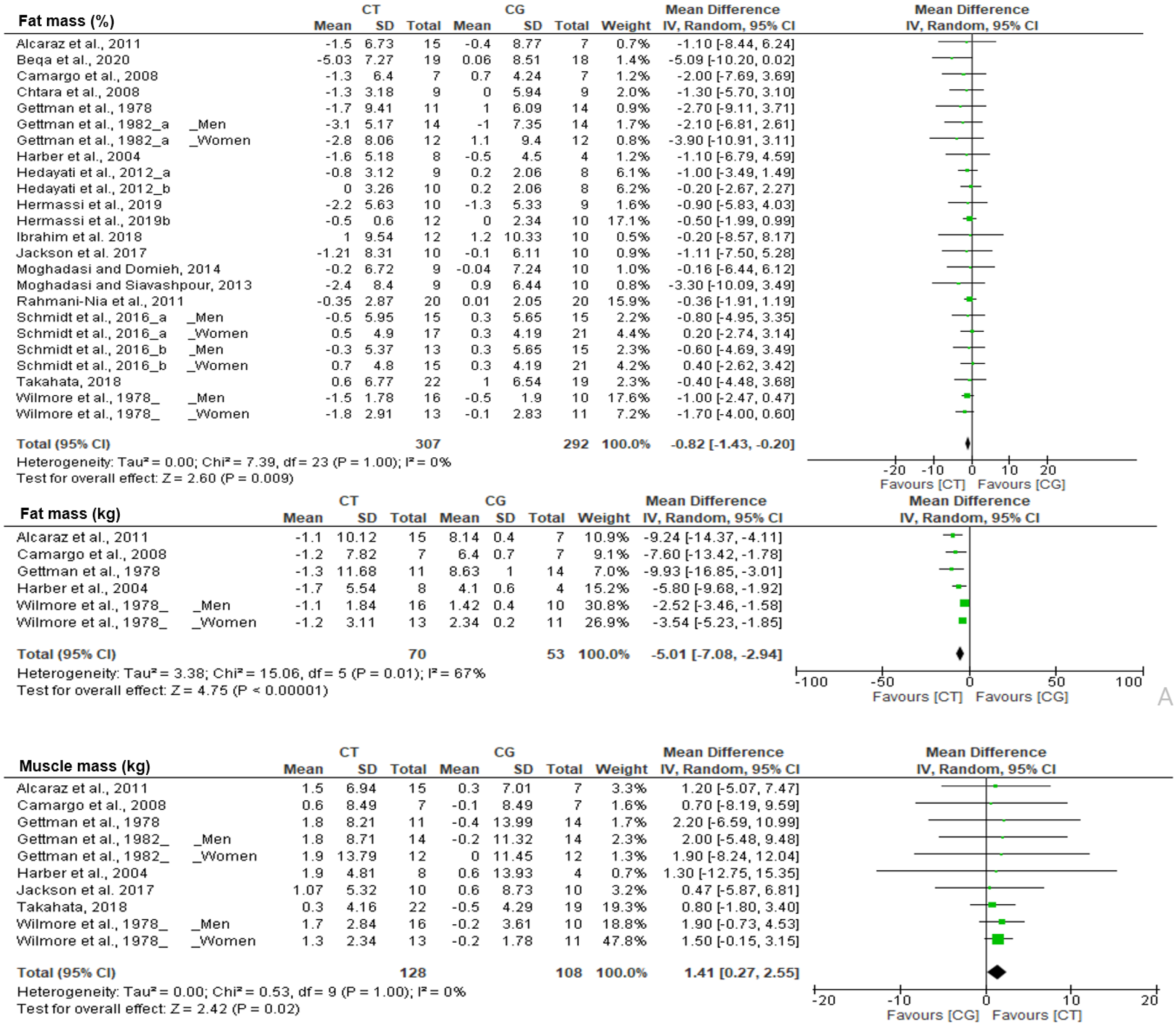
3.4.1. Effect of CT on Body Composition
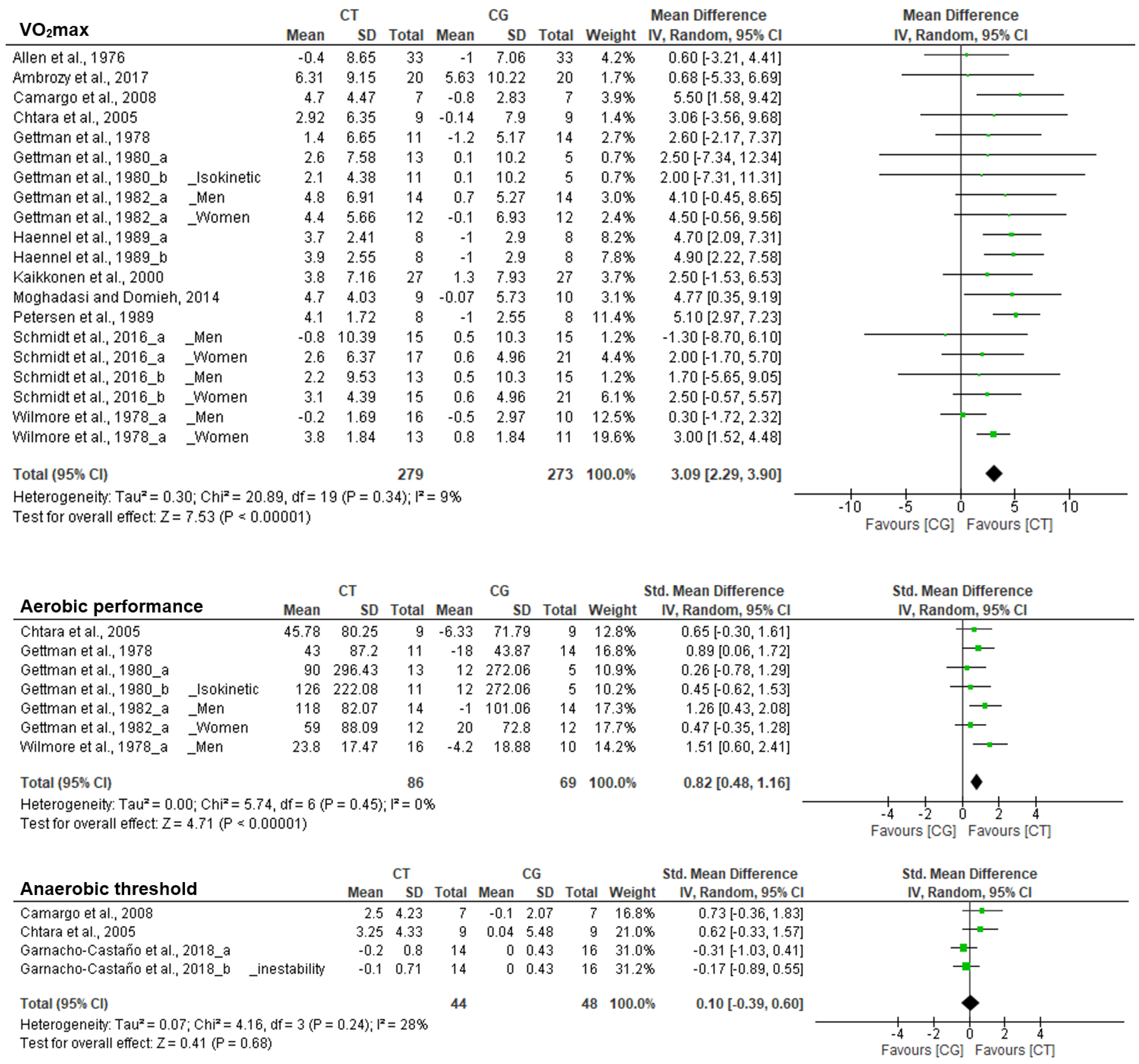
3.4.2. Effect of CT on Endurance Outcomes
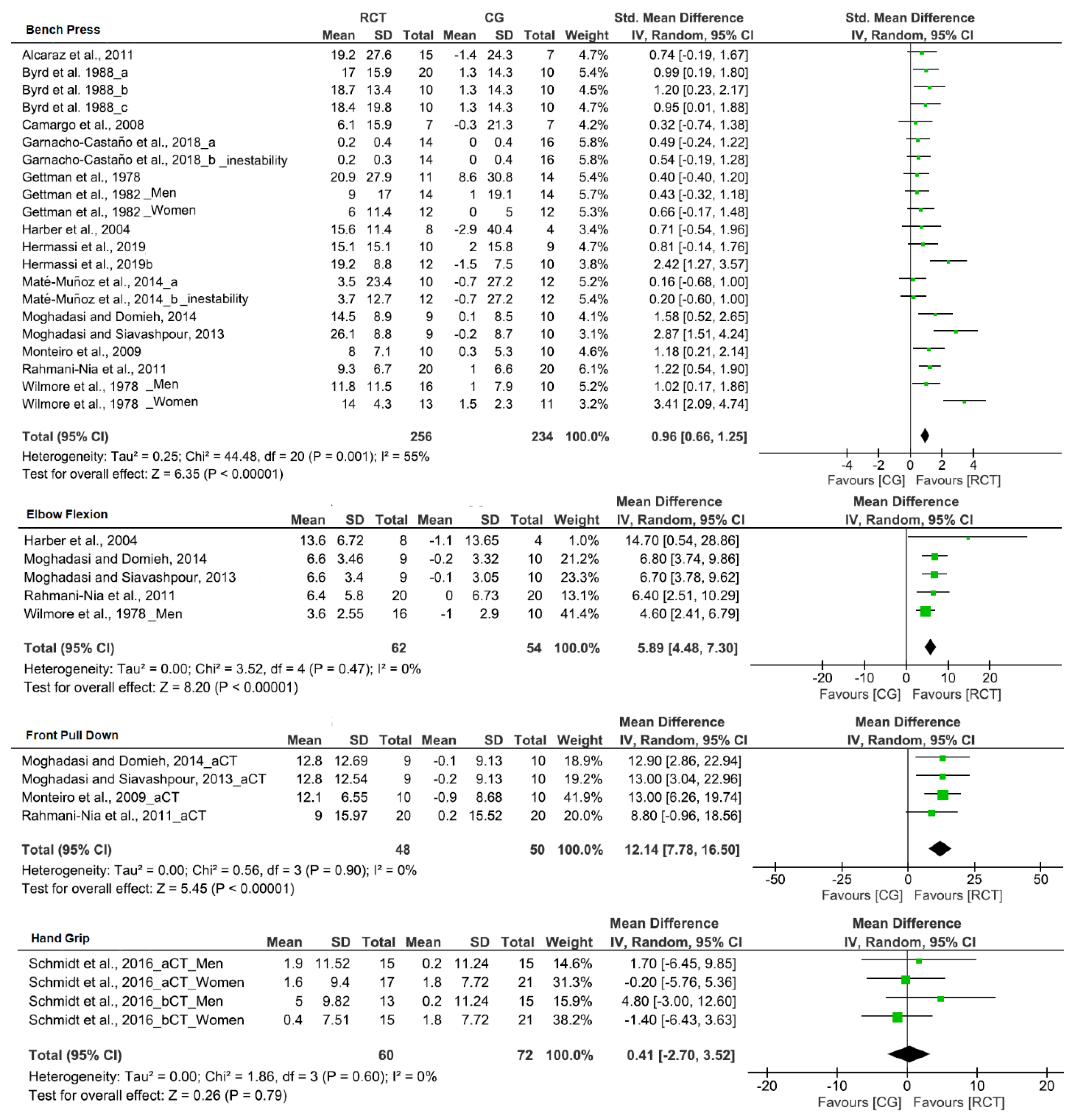
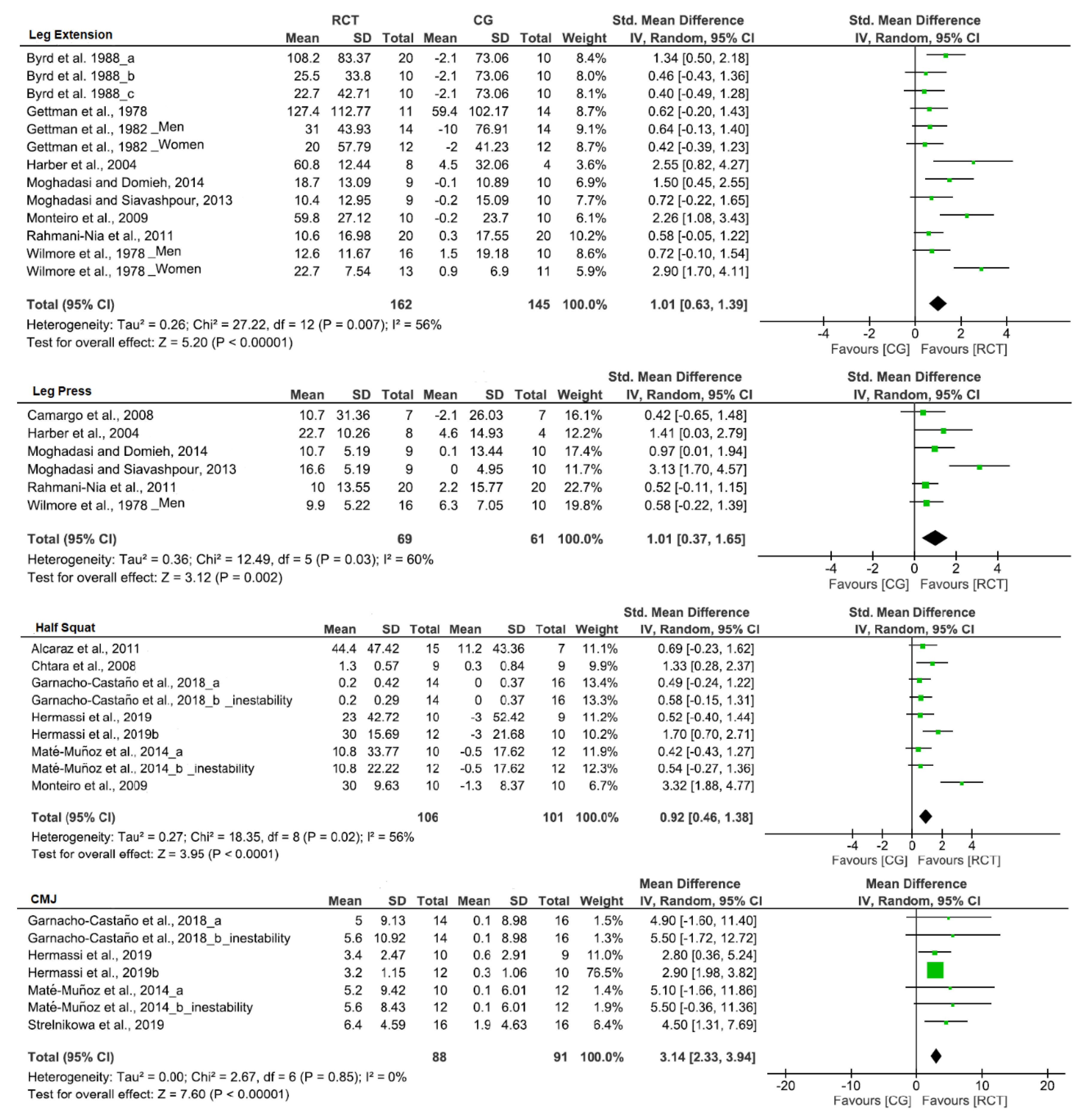
3.4.3. Effect of CT on Strength Outcomes
3.5. Subgroup Analysis
3.5.1. Subgroup Analysis on Body Composition Outcomes
3.5.2. Subgroup Analysis on Endurance Outcomes
3.5.3. Subgroup Analysis on Strength Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Liguori, G.; American College of Sports Medicine (ACSM). ACSM’s guidelines for exercise testing and prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2016. [Google Scholar]
- Tiedemann, A.; Sherrington, C.; Close, J.C.T.; Lord, S.R. Exercise and Sports Science Australia Position Statement on exercise and falls prevention in older people. J. Sci. Med. Sport 2011, 14, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, N.A.; Williams, A.D.; Levinger, I.; Selig, S.; Howden, E.; Coombes, J.S.; Fassett, R.G. Exercise & Sports Science Australia (ESSA) position statement on exercise and chronic kidney disease. J. Sci. Med. Sport 2013, 16, 406–411. [Google Scholar] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coffey, V.G.; Hawley, J.A. Concurrent exercise training: Do opposites distract? J. Physiol. 2017, 595, 2883–2896. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Martínez, F.A.; Rubio-Arias, J.; Ramos-Campo, D.J.; Alcaraz, P.E. Effectiveness of Resistance Circuit-Based Training for Maximum Oxygen Uptake and Upper-Body One-Repetition Maximum Improvements: A Systematic Review and Meta-Analysis. Sport. Med. 2017, 47, 2553–2568. [Google Scholar] [CrossRef]
- Gettman, L.R.; Pollock, M.L. Circuit Weight Training: A Critical Review of Its Physiological Benefits. Phys. Sportsmed. 1981, 9, 44–60. [Google Scholar] [CrossRef] [PubMed]
- Wilmore, J.H.; Parr, R.B.; Girandola, R.N.; Ward, P.; Vodak, P.A.; Barstow, T.J.; Pipes, T.V.; Romero, G.T.; Leslie, P. Physiological alterations consequent to circuit weight training. Med. Sci. Sports 1978, 10, 79–84. [Google Scholar] [PubMed]
- Alcaraz, P.E.; Perez-Gomez, J.; Chavarrias, M.; Blazevich, A.J. Similarity in adaptations to high-resistance circuit vs. traditional strength training in resistance-trained men. J. Strength Cond. Res. 2011, 25, 2519–2527. [Google Scholar] [CrossRef]
- Ramos-Campo, D.J.; Martínez-Guardado, I.; Olcina, G.; Marín-Pagán, C.; Martínez-Noguera, F.J.; Carlos-Vivas, J.; Alcaraz, P.E.; Rubio, J. Effect of high-intensity resistance circuit-based training in hypoxia on aerobic performance and repeat sprint ability. Scand. J. Med. Sci. Sports 2018, 28, 2135–2143. [Google Scholar] [CrossRef]
- Alcaraz, P.E.; Sánchez-Lorente, J.; Blazevich, A.J. Physical performance and cardiovascular responses to an acute bout of heavy resistance circuit training versus traditional strength training. J. Strength Cond. Res. 2008, 22, 667–671. [Google Scholar] [CrossRef] [Green Version]
- Marquez, G.; Romero-Arenas, S.; Marin-Pagan, C.; Vera-Ibanez, A.; Fernández Del Olmo, M.; Taube, W. Peripheral and central fatigue after high intensity resistance circuit training. Muscle Nerve 2017, 56, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Marín-Pagán, C.; Blazevich, A.J.; Chung, L.H.; Romero-Arenas, S.; Freitas, T.T.; Alcaraz, P.E. Acute Physiological Responses to High-Intensity Resistance Circuit Training vs. Traditional Strength Training in Soccer Players. Biology 2020, 9, 383. [Google Scholar] [CrossRef]
- Marín-Pagán, C.; Romero-Arenas, S.; Alcaraz, P.E. Post-exercise responses to an acute bout of high resistance circuit training vs. traditional strength training. J. Strength Cond. Res. 2014, 28, 75. [Google Scholar]
- Braun, W.A.; Hawthorne, W.E.; Markofski, M.M. Acute EPOC response in women to circuit training and treadmill exercise of matched oxygen consumption. Eur. J. Appl. Physiol. 2005, 94, 500–504. [Google Scholar] [CrossRef]
- Hurley, B.F.; Seals, D.R.; Ehsani, A.A.; Cartier, L.J.; Dalsky, G.P.; Hagberg, J.M.; Holloszy, J.O. Effects of high-intensity strength training on cardiovascular function. Med. Sci. Sports Exerc. 1984, 16, 483–488. [Google Scholar] [CrossRef]
- Camargo, M.D.; Stein, R.; Ribeiro, J.P.; Schvartzman, P.R.; Rizzatti, M.O.; Schaan, B.D. Circuit weight training and cardiac morphology: A trial with magnetic resonance imaging. Br. J. Sports Med. 2008, 42, 141–145. [Google Scholar] [CrossRef]
- Chtara, M.; Chamari, K.; Chaouachi, M.; Chaouachi, A.; Koubaa, D.; Feki, Y.; Millet, G.P.; Amri, M. Effects of intra-session concurrent endurance and strength training sequence on aerobic performance and capacity. Br. J. Sports Med. 2005, 39, 555–560. [Google Scholar] [CrossRef] [Green Version]
- Haennel, R.; Teo, K.K.; Quinney, A.; Kappagoda, T. Effects of hydraulic circuit training on cardiovascular function. Med. Sci. Sports Exerc. 1989, 21, 605–612. [Google Scholar] [CrossRef]
- Petersen, S.R.; Haennel, R.G.; Kappagoda, C.T.; Belcastro, A.N.; Reid, D.C.; Wenger, H.A.; Quinney, H.A. The influence of high-velocity circuit resistance training on VO2max and cardiac output. Can. J. Sport Sci. 1989, 14, 158–163. [Google Scholar] [PubMed]
- Taipale, R.S.; Mikkola, J.; Vesterinen, V.; Nummela, A.; Hakkinen, K. Neuromuscular adaptations during combined strength and endurance training in endurance runners: Maximal versus explosive strength training or a mix of both. Eur. J. Appl. Physiol. 2013, 113, 325–335. [Google Scholar] [CrossRef]
- Taipale, R.S.; Mikkola, J.; Salo, T.; Hokka, L.; Vesterinen, V.; Kraemer, W.J.; Nummela, A.; Hakkinen, K. Mixed maximal and explosive strength training in recreational endurance runners. J. strength Cond. Res. 2014, 28, 689–699. [Google Scholar] [CrossRef]
- Chtara, M.; Chaouachi, A.; Levin, G.T.; Chaouachi, M.; Chamari, K.; Amri, M.; Laursen, P.B. Effect of concurrent endurance and circuit resistance training sequence on muscular strength and power development. J. strength Cond. Res. 2008, 22, 1037–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperlich, B.; Hahn, L.-S.; Edel, A.; Behr, T.; Helmprobst, J.; Leppich, R.; Wallmann-Sperlich, B.; Holmberg, H.-C. A 4-Week Intervention Involving Mobile-Based Daily 6-Minute Micro-Sessions of Functional High-Intensity Circuit Training Improves Strength and Quality of Life, but Not Cardio-Respiratory Fitness of Young Untrained Adults. Front. Physiol. 2018, 9, 423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahata, Y. Usefulness of circuit training at home for improving bone mass and muscle mass while losing fat mass in undergraduate female students. Lipids Health Dis. 2018, 17, 104. [Google Scholar] [CrossRef] [Green Version]
- Allen, E.T.; Byrd, R.J.; Smith, D.P. Hemodynamic consequences of circuit weight training. Res. Q. Am. Alliance Heal. Phys. Educ. Recreat. 1976, 47, 299–306. [Google Scholar]
- Billat, L.V.; Koralsztein, J.P. Significance of the velocity at VO2max and time to exhaustion at this velocity. Sport. Med. 1996, 22, 90–108. [Google Scholar] [CrossRef]
- Noakes, T.D.; Myburgh, K.H.; Schall, R. Peak treadmill running velocity during the vo2 max test predicts running performance. J. Sports Sci. 1990, 8, 35–45. [Google Scholar] [CrossRef]
- Paoli, A.; Pacelli, Q.F.; Moro, T.; Marcolin, G.; Neri, M.; Battaglia, G.; Sergi, G.; Bolzetta, F.; Bianco, A. Effects of high-intensity circuit training, low-intensity circuit training and endurance training on blood pressure and lipoproteins in middle-aged overweight men. Lipids Health Dis. 2013, 12, 131. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Systematic Reviews and Meta-Analyses: The PRISMA Statement. Annu. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioural Science, 2nd ed.; Academic press: Cambridge, MA, USA, 1988; ISBN 0805802835. [Google Scholar]
- Higgins, J.; Green, S. Cochrane Handbook for conducting Systematic Reviews; John Wiley & Sons: Hoboken, NJ, USA, 2011; ISBN 9780470699515. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Esquivel, A.A.A.; Welsch, M.A. High and low volume resistance training and vascular function. Int. J. Sports Med. 2007, 28, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Ambrozy, T.; Kiszczak, L.; Omorczyk, J.; Ozimek, M.; Palka, T.; Mucha, D.; Stanula, A.; Mucha, D. Influence of experimental training with external resistance in a form of “kettlebell” on components of women’s physical fitness. Balt. J. Heal. Phys. Act. 2017, 9, 28–36. [Google Scholar] [CrossRef]
- Bachero-Mena, B.; Pareja-Blanco, F.; Gonzalez-Badillo, J.J. Effects of Resistance Training on Physical Performance in High-Level 800-Meter Athletes: A Comparison Between High-Speed Resistance Training and Circuit Training. J. Strength Cond. Res. 2019. Ahead of Print. [Google Scholar] [CrossRef]
- Beqa Ahmeti, G.; Idrizovic, K.; Elezi, A.; Zenic, N.; Ostojic, L. Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women. Int. J. Environ. Res. Public Health 2020, 17, 1222. [Google Scholar] [CrossRef] [Green Version]
- Byrd, R.; Centry, R.; Boatwright, D. Effect of inter-repetition rest intervals in circuit weight training on PWC170 during arm-kranking exercise. J. Sports Med. Phys. Fitness 1988, 28, 336–340. [Google Scholar]
- Dorgo, S.; King, G.A.; Rice, C.A. The effects of manual resistance training on improving muscular strength and endurance. J. Strength Cond. Res. 2009, 23, 293–303. [Google Scholar] [CrossRef]
- Garnacho-Castano, M.V.; Dominguez, R.; Munoz Gonzalez, A.; Feliu-Ruano, R.; Serra-Paya, N.; Mate-Munoz, J.L. Exercise Prescription Using the Borg Rating of Perceived Exertion to Improve Fitness. Int. J. Sports Med. 2018, 39, 115–123. [Google Scholar] [CrossRef]
- Gettman, L.R.; Ayres, J.J.; Pollock, M.L.; Jackson, A. The effect of circuit weight training on strength, cardiorespiratory function, and body composition of adult men. Med. Sci. Sports 1978, 10, 171–176. [Google Scholar] [PubMed]
- Gettman, L.R.; Ayres, J.J.; Pollock, M.L.; Durstine, J.L.; Grantham, W. Physiologic effects on adult men of circuit strength training and jogging. Arch. Phys. Med. Rehabil. 1979, 60, 115–120. [Google Scholar]
- Gettman, L.R.; Culter, L.A.; Strathman, T.A. Physiologic changes after 20 weeks of isotonic vs isokinetic circuit training. J. Sports Med. Phys. Fitness 1980, 20, 265–274. [Google Scholar]
- Gettman, L.R.; Ward, P.; Hagan, R.D. A comparison of combined running and weight training with circuit weight training. Med. Sci. Sports Exerc. 1982, 14, 229–234. [Google Scholar] [CrossRef]
- Getty, A.K.; Wisdo, T.R.; Chavis, L.N.; Derella, C.C.; McLaughlin, K.C.; Perez, A.N.; DiCiurcio, W.T., 3rd; Corbin, M.; Feairheller, D.L. Effects of circuit exercise training on vascular health and blood pressure. Prev. Med. Rep. 2018, 10, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Harber, M.P.; Fry, A.C.; Rubin, M.R.; Smith, J.C.; Weiss, L.W. Skeletal muscle and hormonal adaptations to circuit weight training in untrained men. Scand. J. Med. Sci. Sports 2004, 14, 176–185. [Google Scholar] [CrossRef]
- Hedayati, M.; Saghebjoo, M.; Ghanbari-Niaki, A. Effects of circuit resistance training intensity on the plasma ghrelin to obestatin ratios in healthy young women. Int. J. Endocrinol. Metab. 2012, 10, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Hermassi, S.; Wollny, R.; Schwesig, R.; Shephard, R.J.; Chelly, M.S. Effects of In-Season Circuit Training on Physical Abilities in Male Handball Players. J. Strength Cond. Res. 2019, 33, 944–957. [Google Scholar] [CrossRef]
- Hermassi, S.; Laudner, K.; Schwesig, R. The Effects of Circuit Strength Training on the Development of Physical Fitness and Performance-Related Variables in Handball Players. J. Hum. Kinet. 2020, 71, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Kaikkonen, H.; Yrjama, M.; Siljander, E.; Byman, P.; Laukkanen, R. The effect of heart rate controlled low resistance circuit weight training and endurance training on maximal aerobic power in sedentary adults. Scand. J. Med. Sci. Sports 2000, 10, 211–215. [Google Scholar] [CrossRef]
- Martinez-Guardado, I.; Ramos-Campo, D.J.; Olcina, G.J.; Rubio-Arias, J.A.; Chung, L.H.; Marin-Cascales, E.; Alcaraz, P.E.; Timon, R. Effects of high-intensity resistance circuit-based training in hypoxia on body composition and strength performance. Eur. J. Sport Sci. 2019, 19, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Mate-Munoz, J.L.; Monroy, A.J.A.; Jodra Jimenez, P.; Garnacho-Castano, M. V Effects of instability versus traditional resistance training on strength, power and velocity in untrained men. J. Sports Sci. Med. 2014, 13, 460–468. [Google Scholar] [PubMed]
- Messier, S.P.; Dill, M.E. Alterations in strength and maximal oxygen-uptake consequent to nautilus circuit weight training. Res. Q. Exerc. Sport 1985, 56, 345–351. [Google Scholar] [CrossRef]
- Moghadasi, M.; Mohammadi Domieh, A. Effects of Resistance versus Endurance Training on Plasma Lipocalin-2 in Young Men. Asian J. Sports Med. 2014, 5, 108–114. [Google Scholar] [PubMed]
- Moghadasi, M.; Siavashpour, S. The effect of 12 weeks of resistance training on hormones of bone formation in young sedentary women. Eur. J. Appl. Physiol. 2013, 113, 25–32. [Google Scholar] [CrossRef]
- Monteiro, A.G.; Alveno, D.A.; Prado, M.; Monteiro, G.A.; Ugrinowitsch, C.; Aoki, M.S.; Picarro, I.C. Acute physiological responses to different circuit training protocols. J. Sports Med. Phys. Fitness 2008, 48, 438–442. [Google Scholar]
- Ibrahim, N.S.; Muhamad, A.S.; Ooi, F.K.; Meor-Osman, J.; Chen, C.K. The effects of combined probiotic ingestion and circuit training on muscular strength and power and cytokine responses in young males. Appl. Physiol. Nutr. Metab. 2018, 43, 180–186. [Google Scholar] [CrossRef]
- Ibrahim, N.S.; Ooi, F.K.; Chen, C.K.; Muhamad, A.S. Effects of probiotics supplementation and circuit training on immune responses among sedentary young males. J. Sports Med. Phys. Fitness 2018, 58, 1102–1109. [Google Scholar]
- Jackson, M.; Fatahi, F.; Alabduljader, K.; Jelleyman, C.; Moore, J.P.; Kubis, H.-P. Exercise training and weight loss, not always a happy marriage: Single blind exercise trials in females with diverse BMI. Appl. Physiol. Nutr. Metab. 2017, 43, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, J.; Choi, D.-H.; Song, Y.; Shin, C.S. Muscle Strength Training Alters Muscle Activation of the Lower Extremity during Side-Step Cutting in Females. J. Mot. Behav. 2020, 52, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.R.; Miller, G.D.; Quinney, H.A.; Wenger, H.A. The influence of high-velocity resistance circuit training on aerobic power. J. Orthop. Sports Phys. Ther. 1988, 9, 339–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmani-Nia, F.; Arazi, H.; Rahimi, R.; Piri-Kurd, K.; Hossaini, K. Effects of an eight-week circuit strength training program on the body images and anxiety in untrained college students. Med. Dello Sport 2011, 64, 297–308. [Google Scholar]
- Schmidt, D.; Anderson, K.; Graff, M.; Strutz, V. The effect of high-intensity circuit training on physical fitness. J. Sports Med. Phys. Fitness 2016, 56, 534–540. [Google Scholar] [PubMed]
- Strelnikowa, I.V.; Polevoy, G.G. The influence of circuit training on the development of strength and speed-power abilities in basketball players of 18–19 years old. Phys. Educ. Students 2019, 23, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Taskin, H. Effect of circuit training on the sprint-agility and anaerobic endurance. J. Strength Cond. Res. 2009, 23, 1803–1810. [Google Scholar] [CrossRef]
- Paoli, A.; Pacelli, F.; Bargossi, A.M.; Marcolin, G.; Guzzinati, S.; Neri, M.; Bianco, A.; Palma, A. Effects of three distinct protocols of fitness training on body composition, strength and blood lactate. J. Sports Med. Phys. Fitness 2010, 50, 43–51. [Google Scholar]
- Achten, J.; Jeukendrup, A.E. Optimizing fat oxidation through exercise and diet. Nutrition 2004, 20, 716–727. [Google Scholar] [CrossRef]
- Gonzalez, A.M.; Hoffman, J.R.; Stout, J.R.; Fukuda, D.H.; Willoughby, D.S. Intramuscular Anabolic Signaling and Endocrine Response Following Resistance Exercise: Implications for Muscle Hypertrophy. Sport. Med. 2016, 46, 671–685. [Google Scholar] [CrossRef]
- Willis, L.H.; Slentz, C.A.; Bateman, L.A.; Shields, A.T.; Piner, L.W.; Bales, C.W.; Houmard, J.A.; Kraus, W.E. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J. Appl. Physiol. 2012, 113, 1831–1837. [Google Scholar] [CrossRef]
- Westerterp, K.R. Control of energy expenditure in humans. Eur. J. Clin. Nutr. 2017, 71, 340–344. [Google Scholar] [CrossRef]
- Bassett, D.R.; Howley, E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Egginton, S. Activity-induced angiogenesis. Eur. J. Physiol. 2009, 457, 963. [Google Scholar] [CrossRef] [PubMed]
- Baum, O.; Gübeli, J.; Frese, S.; Torchetti, E.; Malik, C.; Odriozola, A.; Graber, F.; Hoppeler, H.; Tschanz, S.A. Angiogenesis-related ultrastructural changes to capillaries in human skeletal muscle in response to endurance exercise. J. Appl. Physiol. 2015, 119, 1118–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holloway, T.M.; Snijders, T.; Van Kranenburg, J.; Van Loon, L.J.C.; Verdijk, L.B. Temporal Response of Angiogenesis and Hypertrophy to Resistance Training in Young Men. Med. Sci. Sports Exerc. 2018, 50, 36–45. [Google Scholar] [CrossRef]
- Folland, J.P.; Williams, A.G. The adaptations to strength training: Morphological and neurological contributions to increased strength. Sport. Med. 2007, 37, 145–168. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Rhea, M.R.; Alvar, B.A. Applications of the dose-response for muscular strength development: A review of meta-analytic efficacy and reliability for designing training prescription. J. Strength Cond. Res. 2005, 19, 950–958. [Google Scholar] [CrossRef]
- Ahtiainen, J.P.; Pakarinen, A.; Alen, M.; Kraemer, W.J.; Häkkinen, K. Muscle hypertrophy, hormonal adaptations and strength development during strength training in strength-trained and untrained men. Eur. J. Appl. Physiol. 2003, 89, 555–563. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Mayhew, J.L.; Grimstvedt, M.E.; Greenwood, M.; Rasmussen, C.J.; Kreider, R.B. Factors That Contribute to and Account for Strength and Work Capacity in a Large Cohort of Recreationally Trained Adult Healthy Men With High- and Low-Strength Levels. J. Strength Cond. Res. 2014, 28, 1246–1254. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Ogborn, D.; Krieger, J.W. Effects of Resistance Training Frequency on Measures of Muscle Hypertrophy: A Systematic Review and Meta-Analysis. Sport. Med. 2016, 46, 1689–1697. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Ogborn, D.; Krieger, J.W. Dose-response relationship between weekly resistance training volume and increases in muscle mass: A systematic review and meta-analysis. J. Sports Sci. 2017, 35, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Grgic, J.; Ogborn, D.; Krieger, J.W. Strength and hypertrophy adaptations between low- vs. High-load resistance training: A systematic review and meta-analysis. J. Strength Cond. Res. 2017, 31, 3508–3523. [Google Scholar] [CrossRef] [PubMed]
- Carroll, T.J.; Selvanayagam, V.S.; Riek, S.; Semmler, J.G. Neural adaptations to strength training: Moving beyond transcranial magnetic stimulation and reflex studies. Acta Physiol. 2011, 202, 119–140. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Marin, P.J.; Rhea, M.R.; Wilson, S.M.C.; Loenneke, J.P.; Anderson, J.C. Concurrent training: A meta-analysis examining interference of aerobic and resistance exercises. J. Strength Cond. Res. 2012, 26, 2293–2307. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Group | Duration (Weeks) | Frequency (Days x Week) | Intensity (% RM or Other) | Exercises (n) | Session Duration (min) | Total Session (n) | Bouts/Sets (n) | Repetitions (n) | Work Time Each Exercise (s) | Rest between Sets (s) | Rest between Exercise (s) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alcaraz et al., 2011 | CT | 8 | 3 | 85–90 | 6 | 55–78 | 24 | 3–6 | 6 | 25 | 300 | 35 |
| CG | 8 | |||||||||||
| Allen et al., 1976 | CT | 12 | 3 | 75 | 6 | 27 | 36 | 3 | 8 | 30 | - | 60 |
| CG | 12 | |||||||||||
| Ambrozy et al., 2017 | CT | 8 | 3 | - | 3–5 | 60 | 24 | 3 | 15–20 | - | 120 | - |
| CG | 8 | 3 | - | 2 | 60 | 24 | ||||||
| Arce-Esquivel and Welsch, 2007 | CT1 | 5 | 3 | 60 | 8 | 60 | 15 | 3 | 8–12 | - | - | - |
| CT2 | 5 | 3 | 60 | 8 | 60 | 15 | 1 | 8–12 | - | - | - | |
| Bachero-Mena et al., 2020 | CT | 25 | 1 | 0–40 | 7 | - | 25 | 3–5 | 10–30 | - | - | - |
| RT | 25 | 2 | 40–55 | 4 | - | 50 | 2–3 | 4–6 | - | - | - | |
| Beqa et al., 2020 | CT | 8 | 3 | - | 8–10 | 45–60 | 24 | 2–3 | - | 30 | 300 | 30 |
| CG | 8 | |||||||||||
| Byrd et al. 1988 | CT1 (no pause) | 10 | 3 | 75–85 | 6 | 30 | 3 | 6–10 | 60 | |||
| CT2 (1 sec rest between reps) | 10 | 3 | 75–85 | 6 | 30 | 3 | 6–10 | 60 | ||||
| CT3 (2 sec rest between reps) | 10 | 3 | 75–85 | 6 | 30 | 3 | 6–10 | 60 | ||||
| CG | 10 | |||||||||||
| Camargo et al., 2008 | CT | 12 | 3 | 60 | - | 35 | 36 | 3 | 15 | - | - | - |
| CG | 12 | |||||||||||
| Chtara et al., 2005 | CT | 12 | 2 | - | 6 | 30 | 24 | 4 | - | 30–40 | 120 | 20–30 |
| CG | 12 | - | - | - | - | - | - | - | - | - | - | |
| Chtara et al., 2008 | CT | 12 | 2 | - | 6 | 30 | 24 | 4 | - | 30–40 | 120 | 20–30 |
| CG | 12 | - | - | - | - | - | - | - | - | - | - | |
| Dorgo et al., 2009 | CT | 14 | 3 | 67–80 | 6–9 | 60 | 42 | 2–4 | 8–12 | - | - | 20–30 |
| Manual CT | 14 | 3 | 67–80 | 6–9 | 60 | 42 | 2–4 | 8–12 | - | - | 20–30 | |
| Garnacho-Castaño et al., 2018 | CT | 8 | 3 | 5–8 RPE | 8 | 45–60 | 24 | 3 | 15 | - | 60–120 | 0–30 |
| CT instability | 8 | 3 | 5–8 RPE | 8 | 45–60 | 24 | 3 | 15 | - | 60–120 | 0–30 | |
| CG | 8 | |||||||||||
| Gettman et al., 1978 | CT | 20 | 3 | 50 | 10 | 45 | 60 | 2 | 10–20 | - | - | 20–30 |
| CG | 20 | |||||||||||
| Gettman et al., 1979 | CT | 8 | 3 | 50–90 | 8 | 24 | 24 | 2 | 10–15 | - | - | 30 |
| Gettman et al., 1980 | CT | 20 | 3 | 50 | 9 | 25 | 60 | 2 | 12 | 30 | ||
| CT isokinetic | 20 | 3 | 60º/s | 10 | 29 | 60 | 2 | 12 | 30 | |||
| CG | 20 | |||||||||||
| Gettman et al., 1982 | CT | 12 | 3 | 40 | 10 | 22,5 | 36 | 3 | 12–20 | 30 | - | 15 |
| CG | 12 | |||||||||||
| Getty et al., 2018 | CT | 4 | 3 | - | 6 | - | - | 3 | - | - | - | - |
| Haennel et al., 1989 | CT 1 | 9 | 3 | 60 | 9 | 27 | 27 | 3 | - | 20 | 80 | 20 |
| CT 2 | 9 | 3 | 50 | 9 | 27 | 27 | 3 | - | 20 | 80 | 20 | |
| CG | 9 | |||||||||||
| Harber et al., 2004 | CT | 10 | 3 | 40–60 | 10 | - | 30 | 1–3 | 12–20 | 20–30 | - | 10–30 |
| CG | 10 | |||||||||||
| Hedayati et al., 2012 | CT1 | 4 | 4 | 40 | 9 | 50–55 | 16 | 3 | 8–11 | 30 | 120 | 30 |
| CT2 | 4 | 4 | 80 | 9 | 50–55 | 16 | 3 | 8–11 | 30 | 120 | 30 | |
| CG | 4 | |||||||||||
| Hermassi et al., 2019 | CT | 12 | 2 | 80–85 and body weight | 6 | 24 | 2 | 6–16 | 180 | 180 | ||
| CG | 12 | |||||||||||
| Hermassi et al., 2020 | CT | 10 | 2 | 60–80 | 8 | 20 | 2–3 | 8–12 | 180 | 180 | ||
| CG | 10 | |||||||||||
| Kaikkonen et al., 2000 | CT | 12 | 3 | 70–80% HR peak | 10 | 40 | 36 | 3 | - | 40 | - | 20 |
| CG | 12 | |||||||||||
| Martínez-Guardado et al., 2019 | CT | 7 | 2 | 85 | 6 | 60 | 14 | 3 | 6 | 25 | 300 | 35 |
| Maté-Muñoz et al., 2014 | CT | 7 | 3 | 10 RPE | 8 | 45–65 | 21 | 3 | 15 | - | 60–120 | 0–30 |
| CT instability | 7 | 3 | 10 RPE | 8 | 45–65 | 21 | 3 | 15 | - | 60–120 | 0–30 | |
| CG | 7 | |||||||||||
| Messier and Dill, 1985 | CT | 10 | 3 | 67–80/<65 | 12 | 20 | 30 | - | 8–12 | - | - | - |
| Moghadasi and Domieh, 2014 | CT | 8 | 3 | 65–80 | 8 | 50–60 | 24 | 2–4 | 8–12 | - | 120–180 | 60–90 |
| CG | 8 | |||||||||||
| Moghadasi and Siavashpour, 2013 | CT | 12 | 3 | 65–80 | 8 | 50–60 | 36 | 2–4 | 8–12 | - | 120–180 | 30 |
| CG | 12 | |||||||||||
| Monteiro et al., 2008 | CT | 10 | 3 | 65–80 | 7 | - | 30 | 3 | 8–12 | - | 120 | ratio 1:3 |
| CG | 10 | |||||||||||
| Ibrahim et al., 2018 | CT | 12 | 3 | - | 10 | - | 30 | 2–3 | - | 30 | 300 | 60 |
| CG | 12 | |||||||||||
| Ibrahim et al. 2018b | CT | 12 | 3 | Elastic bands | 10 | 36 | 3 | 10–20 | ratio 1:2 | 300 | ||
| CG | 12 | |||||||||||
| Jackson et al. 2017 | CT | 4 | 3 | 70–80% HRpeak | 6 | 60 | 12 | |||||
| CG | 4 | |||||||||||
| Jeong et al., 2019 | CT | 10 | 3 | 40–60 | 9 | 50 | 30 | 3 | 12–20 | - | - | 20–60 |
| CG | 10 | |||||||||||
| Petersen et al., 1988 | CT | 5 | 4 | 60% VO2max | 6 | 20 | 2–3 | 20–24 | 20 | 240 | 20–60 | |
| CG | 5 | 3 | ||||||||||
| Petersen et al., 1989 | CT | 6 | 3,5 | 10 | 21 | 2–3 | - | 20 | 240 | 20–60 | ||
| CG | 6 | 3 | - | 21 | - | - | - | - | - | |||
| Rahmani-Nia et al., 2011 | CT | 8 | 3 | 45–60 | 6–8 | 24 | 3 | 12–15 | - | 180 | 20 | |
| CG | 8 | |||||||||||
| Ramos-Campo et al., 2018 | CT | 7 | 2 | 85 | 6 | 60 | 14 | 3 | 6 | 25 | 300 | 35 |
| Schmidt et al., 2016 | CT 1 | 8 | 3 | - | 12 | 7 | 24 | 1 | - | 30 | - | 10 |
| CT 2 | 8 | 3 | - | 12 | 14 | 24 | 2 | - | 30 | - | 10 | |
| CG | 8 | |||||||||||
| Sperlich et al., 2018 | CT | 4 | 14 | 6 | 56 | |||||||
| CT | 4 | 28 | 6 | 112 | ||||||||
| Strelnikowa et al., 2019 | CT | 28 | 1–2 | 30–40% body weight or body weight | 13 | 1–5 | 5–30 | |||||
| CG | 28 | |||||||||||
| Taipale et al. 2013 | CT | 8 | 1–2 | 8 | ratio 1:3–1:5 | |||||||
| Taipale et al. 2014 | CT | 8 | 1–2 | 8 | 14 | ratio 1:3–1:5 | ||||||
| CT | 8 | 1–2 | 8 | 14 | ratio 1:3–1:5 | |||||||
| Takahata, 2018 | CT | 12 | 3 | - | 10 | 15 | 36 | 3 | - | 30 | 0 | 0 |
| CG | 12 | - | - | - | - | - | - | - | - | - | - | |
| Taskin, 2009 | CT | 10 | 3 | 75 | 8 | 30 | 3 | 15 | 10 | 40–60 | ||
| CG | 10 | 3 | 8 | - | - | - | - | - | ||||
| Wilmore et al., 1978 | CT | 10 | 3 | 40–55 | 10 | 22,5 | 30 | 3 | - | 30 | 15 | |
| CG | 10 |
| n Studies | n | Random IV, IC 95% | Test Overall Effects | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
| Participants | Effects | Z(p) | Tau2 | Chi2 | p | I2 | ||
| Weight (kg)-MD | ||||||||
| CG | 24 | 287 | −0.08 [−0.86, 0.70] | 0.20 (0.840) | 0.000 | 2.17 | 1.000 | 0% |
| CT | 34 | 456 | 0.06 [−0.59, 0.72] | 0.19 (0.850) | 0.000 | 7.46 | 1.000 | 0% |
| Fat Mass (%)-MD | ||||||||
| CG | 22 | 258 | 0.02 [−0.45, 0.48] | 0.07 (0.950) | 0.000 | 3.43 | 1.000 | 0% |
| CT | 29 | 395 | −0.70 [−0.98, −0.43] | 5.03 (<0.001) | 0.000 | 23.60 | 0.700 | 0% |
| Fat Mass (kg)-MD | ||||||||
| CG | 6 | 53 | − 0.30 [−1.00, 0.41] | 0.82 (0.410) | 0.000 | 0.58 | 0.990 | 0% |
| CT | 10 | 123 | −1.04 [−1.75, −0.33] | 2.87 (0.004) | 0.000 | 0.95 | 1.000 | 0% |
| Muscle Mass (kg)-SMD | ||||||||
| CG | 10 | 108 | −0.05 [−0.31, 0.22] | 0.34 (0.740) | 0.000 | 0.37 | 1.000 | 0% |
| CT | 14 | 181 | 0.28 [0.07, 0.49] | 2.63 (0.008) | 0.000 | 5.53 | 0.960 | 0% |
| n Studies | n | Random IV, IC 95% | Test Overall Effects | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
| Participants | Effects | Z(p) | Tau2 | Chi2 | p | I2 | ||
| VO2max (mL/kg/min)-MD | ||||||||
| CG | 16 | 234 | 0.03 [−0.55, 0.61] | 0.11 (0.91) | 0.000 | 13.88 | 0.530 | 0% |
| CT | 28 | 367 | 2.93 [1.97, 3.90] | 5.98 (<0.001) | 4.010 | 114.31 | <0.001 | 76% |
| MAS/MAP-MD | ||||||||
| CG | 1 | 9 | 0.04 [−0.67, 0.75] | 0.11 (0.91) | N/A | N/A | N/A | N/A |
| CT | 5 | 45 | 0.35 [0.02, 0.67] | 2.07 (0.04) | 0.000 | 3.73 | 0.440 | 0% |
| Aerobic Performance-SMD | ||||||||
| CG | 5 | 64 | −0.11 [−0.46, 0.24] | 0.63 (0.53) | 0.000 | 3.07 | 0.690 | 0% |
| CT | 10 | 128 | 0.65 [0.09, 1.20] | 2.27 (0.02) | 0.620 | 39.82 | <0.001 | 77% |
| VT2-SMD | ||||||||
| CG | 3 | 32 | −0.01 [−0.50, 0.48] | 0.05 (0.96) | 0.000 | 0.01 | 0.990 | 0% |
| CT | 5 | 57 | 0.20 [−0.29, 0.69] | 0.79 (0.43) | 0.120 | 6.63 | 0.160 | 40% |
| n Studies | n | Random IV, IC 95% | Test Overall Effects | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
| Participants | Effects | Z(p) | Tau2 | Chi2 | p | I2 | ||
| Upper Limbs | ||||||||
| Bench Press-SMD | ||||||||
| CG | 17 | 186 | 0.11 [−0.09, 0.31] | 1.05 (0.290) | 0.000 | 5.15 | 0.990 | 0% |
| CT | 27 | 404 | 1.16 [0.84, 1.47] | 7.21 (0.001) | 0.480 | 102.25 | <0.001 | 75% |
| Front Pull Down-MD | ||||||||
| CG | 4 | 50 | −0.30 [−3.21, 2.60] | 0.21 (0.840) | 0.000 | 0.07 | 0.990 | 0% |
| CT | 5 | 61 | 11.61 [8.83, 14.39] | 8.20 (0.001) | 0.000 | 0.78 | 0.940 | 0% |
| Elbow Flexion-MD | ||||||||
| CG | 5 | 54 | −0.41 [−1.44, 0.62] | 0.79 (0.430) | 0.000 | 0.64 | 0.960 | 0% |
| CT | 9 | 121 | 5.00 [3.09, 6.92] | 5.11 (0.001) | 6.970 | 63.86 | <0.001 | 87% |
| Hand Grip-MD | ||||||||
| CG | 2 | 36 | 1.40 [−1.46, 4.25] | 0.96 (0.340) | 0.000 | 0.23 | 0.630 | 0% |
| CT | 6 | 95 | 2.15 [0.01, 4.28] | 1.97 (0.050) | 0.000 | 2.48 | 0.780 | 0% |
| Lower Limbs | ||||||||
| Leg Press-SMD | ||||||||
| CG | 6 | 61 | 0.25 [−0.11, 0.61] | 1.34 (0.180) | 0.000 | 4.87 | 0.430 | 0% |
| CT | 9 | 177 | 1.83 [1.15, 2.52] | 5.25 (0.001) | 0.790 | 34.90 | <0.001 | 77% |
| Leg Extension-SMD | ||||||||
| CG | 11 | 125 | 0.08 [−0.17, 0.33] | 0.65 (0.510) | 0.000 | 4.21 | 0.940 | 0% |
| CT | 17 | 201 | 1.28 [0.83, 1.74] | 5.51 (<0.001) | 0.650 | 62.280 | <0.001 | 74% |
| Half-Squat-SMD | ||||||||
| CG | 7 | 73 | 0.02 [−0.31, 0.34] | 0.11 (0.910) | 0.000 | 1.80 | 0.940 | 0% |
| CT | 11 | 190 | 1.20 [0.72, 1.67] | 4.95 (0.001) | 0.430 | 38.70 | <0.001 | 74% |
| CMJ-MD | ||||||||
| CG | 5 | 63 | 0.43 [−0.16, 1.01] | 1.42 (0.150) | 0.000 | 1.85 | 0.760 | 0% |
| CT | 11 | 118 | 3.58 [2.69, 4.47] | 7.87 (0.001) | 0.430 | 12.80 | 0.240 | 22% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Campo, D.J.; Andreu Caravaca, L.; Martínez-Rodríguez, A.; Rubio-Arias, J.Á. Effects of Resistance Circuit-Based Training on Body Composition, Strength and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Biology 2021, 10, 377. https://doi.org/10.3390/biology10050377
Ramos-Campo DJ, Andreu Caravaca L, Martínez-Rodríguez A, Rubio-Arias JÁ. Effects of Resistance Circuit-Based Training on Body Composition, Strength and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Biology. 2021; 10(5):377. https://doi.org/10.3390/biology10050377
Chicago/Turabian StyleRamos-Campo, Domingo Jesús, Luis Andreu Caravaca, Alejandro Martínez-Rodríguez, and Jacobo Ángel Rubio-Arias. 2021. "Effects of Resistance Circuit-Based Training on Body Composition, Strength and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis" Biology 10, no. 5: 377. https://doi.org/10.3390/biology10050377
APA StyleRamos-Campo, D. J., Andreu Caravaca, L., Martínez-Rodríguez, A., & Rubio-Arias, J. Á. (2021). Effects of Resistance Circuit-Based Training on Body Composition, Strength and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Biology, 10(5), 377. https://doi.org/10.3390/biology10050377