
Breast Cancer Mortality in the Americas and Australasia over the Period 1980–2017 with Predictions for 2025



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Hensing, W.; Santa-Maria, C.A.; Peterson, L.L.; Sheng, J.Y. Landmark trials in the medical oncology management of early stage breast cancer. Semin. Oncol. 2020, 47, 278–292. [Google Scholar] [CrossRef]
- Carioli, G.; Malvezzi, M.; Rodriguez, T.; Bertuccio, P.; Negri, E.; La Vecchia, C. Trends and predictions to 2020 in breast cancer mortality: Americas and Australasia. Breast 2018, 37, 16–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, K.; Ding, P.; Wu, Y.; Tian, W.; Pan, T.; Zhang, S. Global patterns and trends in the breast cancer incidence and mortality according to sociodemographic indices: An observational study based on the global burden of diseases. BMJ Open 2019, 9, e028461. [Google Scholar] [CrossRef]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, regional, and National cancer incidence, mortality, years of life lost, years lived with disability, and Disability-Adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar]
- Ginsburg, O.; Bray, F.; Coleman, M.P.; Vanderpuye, V.; Eniu, A.; Kotha, S.R.; Sarker, M.; Huong, T.T.; Allemani, C.; Dvaladze, A.; et al. The global burden of women’s cancers: A grand challenge in global health. Lancet 2017, 389, 847–860. [Google Scholar] [CrossRef]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Wojtyla, C.; Bertuccio, P.; Wojtyla, A.; La Vecchia, C. European trends in breast cancer mortality, 1980-2017 and predictions to 2025. Eur. J. Cancer 2021, 152, 4–17. [Google Scholar] [CrossRef]
- World Health Organization Statistical Information System. WHO Mortality Database. Available online: http://www.who.int/healthinfo/statistics/mortality_rawdata/en/index.html (accessed on 20 February 2020).
- World Health Organization. International Classification of Disease and Related Health Problems; 10th Revision; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- United Nations DoEaSA, Population Division. World Population Prospects: The 2017 Revision; DVD Edition; United Nations: New York, NY USA, 2017. [Google Scholar]
- Pan American Health Organization (PAHO). Regional Core Health Data Initiative. Table Generator System. Available online: http://www.paho.org/English/SHA/coredata/tabulator/newTabulator.htm (accessed on 20 April 2020).
- Doll, R.; Smith, P.G.; Waterhouse, J.A.H.; Muir, C.S.; Shanmugaratnam, K.; Powell, J.; Peacham, D.; Whelan, S. Comparison between registries: Age-standardized rates. In Cancer Incidence in Five Continents; IARC SciPubl No. 42; World Health Organization: Lyon, France, 1982; vol. IV, p. 671.e5. [Google Scholar]
- National Cancer Institute. Joinpoint Regression Program; version 4.6.0.0. Available online: http://srab.cancer.gov/joinpoint/ (accessed on 20 April 2020).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates (Erratum in: Stat Med 2001; 20:655). Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Clegg, L.X.; Hankey, B.F.; Tiwari, R.; Feuer, E.J.; Edwards, B.K. Estimating average annual per cent change in trend analysis. Stat. Med. 2009, 28, 3670–3682. [Google Scholar] [CrossRef] [Green Version]
- Bonadonna, G.; Valagussa, P.; Moliterni, A.; Zambetti, M.; Brambilla, C. Adjuvant cyclophosphamide, methotrexate, and fluorouracil in node-positive breast cancer: The results of 20 years of follow-up. N. Engl. J. Med. 1995, 332, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Comparisons be- tween different polychemotherapy regimens for early breast cancer: Meta–analyses of long-term outcome among 100000 women in 123 randomized trials. Lancet 2012, 379, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Davies, C.; Godwin, J.; Gray, R.; Clarke, M.; Cutter, D.; Darby, S.; McGale, P.; Pan, H.C.; Taylor, C.; et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level metaanalysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar] [CrossRef] [Green Version]
- Goldhirsch, A.; Gelber, R.D.; Piccart-Gebhart, M.J.; de Azambuja, E.; Procter, M.; Suter, T.M.; Jackisch, C.; Cameron, D.; Weber, H.A.; Herceptin Adjuvant (HERA) Trial Study Team. 2 years versus 1 year of adjuvant trastuzumab for HER2-positive breast cancer (HERA): An open-label, randomised controlled trial. Lancet 2013, 382, 1021–1028. [Google Scholar] [CrossRef]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Breast Cancer International Research Group. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.H.; Davidson, N.E.; Geyer, C.E., Jr.; Martino, S.; Mamounas, E.P.; Kaufman, P.; Wolmark, N. Four-year follow-up of trastuzumab plus adjuvant chemotherapy for operable human epidermal growth factor receptor 2-positive breast cancer: Joint analysis of data from NCCTG N9831 and NSABP B-31. J. Clin. Oncol. 2011, 29, 3366–3373. [Google Scholar] [CrossRef] [Green Version]
- Dignam, J.J. Disparities in Breast Cancer: Narrowing the Gap. J. Natl. Cancer Inst. 2021, 113, 349–350. [Google Scholar] [CrossRef]
- Albain, K.S.; Gray, R.J.; Makower, D.F.; Faghih, A.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Goetz, M.P.; Olson, J.A.; Lively, T. Race, Ethnicity, and Clinical Outcomes in Hormone Receptor-Positive, HER2-Negative, Node-Negative Breast Cancer in the Randomized TAILORx Trial. J. Natl. Cancer Inst. 2021, 113, 390–399. [Google Scholar] [CrossRef]
- EBCTCG (Early Breast Cancer Trialists’ Collaborative Group); McGale, P.; Taylor, C.; Correa, C.; Cutter, D.; Duane, F.; Ewertz, M.; Gray, R.; Mannu, G.; Peto, R.; et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: Meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 2014, 383, 2127–2135. [Google Scholar] [CrossRef]
- Pinheiro, P.S.; Callahan, K.E.; Siegel, R.L.; Jin, H.; Morris, C.R.; Trapido, E.J.; Gomez, S.L. Cancer Mortality in Hispanic Ethnic Groups. Cancer Epidemiol. Biomark. Prev. 2017, 26, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and breastfeeding: Collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet 2002, 360, 187–195. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Boyle, P. Reproductive factors and breast cancer: An overview. Soz Praventivmed. 1989, 34, 101–107. [Google Scholar] [CrossRef]
- Brinton, L.A.; Gaudet, M.M.; Gierach, G.L. Breast cancer. In Cancer Epidemiology and Prevention, 4th ed.; Thun, M., Linet, M.S., Cerhan, J.R., Haiman, C.A., Eds.; Oxford University Press: Oxford, UK, 2018; pp. 861–888. [Google Scholar]
- van den Broek, J.J.; Schechter, C.B.; van Ravesteyn, N.T.; Janssens, A.C.J.W.; Wolfson, M.C.; Trentham-Dietz, A.; Simard, J.; Easton, D.F.; Mandelblatt, J.S.; Kraft, P.; et al. Personalizing Breast Cancer Screening Based on Polygenic Risk and Family History. J. Natl. Cancer Inst. 2021, 113, 434–442. [Google Scholar] [CrossRef]
- Welch, H.G.; Prorok, P.C.; O’Malley, A.J.; Kramer, B.S. Breast-Cancer Tumor Size, Overdiagnosis, and Mammography Screening Effectiveness. N. Engl. J. Med. 2016, 375, 1438–1447. [Google Scholar] [CrossRef]
- Bulliard, J.L.; Beau, A.B.; Njorv, S.; Wu, W.Y.; Procopio, P.; Nickson, C.; Lynge, E. Breast cancer screening and overdiagnosis. Int. J. Cancer 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [Green Version]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.; Howard, B.V.; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results From the Women’s Health Initiative randomized controlled trial. JAMA 2002, 288, 321–333. [Google Scholar] [CrossRef] [Green Version]
- Breen, N.; Gentleman, J.F.; Schiller, J.S. Update on mammography trends: Comparisons of rates in 2000, 2005, and 2008. Cancer 2011, 117, 2209–2218. [Google Scholar] [CrossRef]
- Reeves, G.K.; Pirie, K.; Beral, V.; Green, J.; Spencer, E.; Bull, D.; Million Women Study Collaboration. Cancer incidence and mortality in relation to body mass index in the Million Women Study: Cohort study. BMJ 2007, 335, 1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiol. Rev. 2014, 36, 114–136. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Orsini, N.; Saji, S.; Key, T.J.; Wolk, A. Body weight and incidence of breast cancer defined by estrogen and progesterone receptor status--a meta-analysis. Int. J. Cancer 2009, 124, 698–712. [Google Scholar] [CrossRef] [PubMed]
- Gilliland, F.D.; Joste, N.; Stauber, P.M.; Hunt, W.C.; Rosenberg, R.; Redlich, G.; Key, C.R. Biologic characteristics of interval and screen-detected breast cancers. J. Natl. Cancer Inst. 2000, 92, 743–749. [Google Scholar] [CrossRef] [Green Version]
- Porter, P.L.; El-Bastawissi, A.Y.; Mandelson, M.T.; Lin, M.G.; Khalid, N.; Watney, E.A.; Cousens, L.; White, D.; Taplin, S.; White, E. Breast tumor characteristics as predictors of mammographic detection: Comparison of interval and screen-detected cancers. J. Natl. Cancer Inst. 1999, 91, 2020–2028. [Google Scholar] [CrossRef]
- Maroni, R.; Massat, N.J.; Parmar, D.; Dibden, A.; Cuzick, J.; Sasieni, P.D.; Duffy, S.W. A case-control study to evaluate the impact of the breast screening programme on mortality in England. Br. J. Cancer 2021, 124, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Nyante, S.J.; Benefield, T.S.; Kuzmiak, C.M.; Earnhardt, K.; Pritchard, M.; Henderson, L.M. Population-level impact of coronavirus disease 2019 on breast cancer screening and diagnostic procedures. Cancer 2021. Epub ahead of print. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
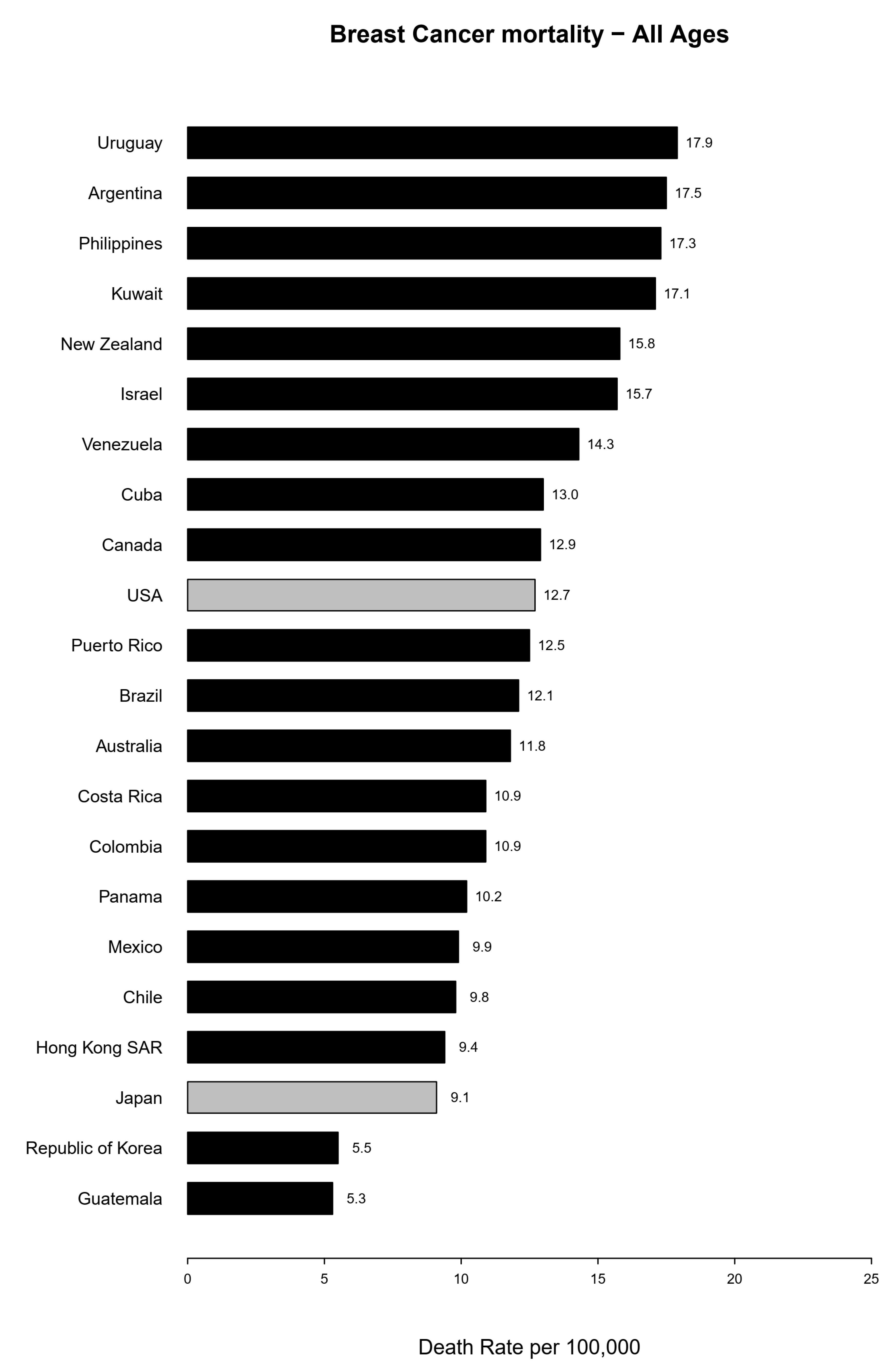
| All Ages | ||||
|---|---|---|---|---|
| Year | Around 2012 | 2017 | Deaths in 2017 | % Change |
| North America | ||||
| Canada | 13.7 | 12.9 | 5318 | −5.8 |
| USA | 13.7 | 12.7 | 42,000 | −7.3 |
| Latin America | ||||
| Argentina | 17.5 | 17.5 | 6049 | 0.0 |
| Brazil | 11.6 | 12.1 | 16,724 | 4.3 |
| Chile | 10.2 | 9.8 | 1504 | −3.9 |
| Colombia | 9.8 | 10.9 | 3300 | 11.2 |
| Costa Rica | 10.7 | 10.9 | 366 | 1.9 |
| Cuba | 14.6 | 13.0 | 1519 | −11.0 |
| Guatemala | 4.8 | 5.3 | 353 | 10.4 |
| Mexico | 9.3 | 9.9 | 6756 | 6.5 |
| Panama | 10.1 | 10.2 | 241 | 1.0 |
| Puerto Rico | 13.0 | 12.5 | 445 | −3.8 |
| Uruguay | 18.4 | 17.9 | 611 | −2.7 |
| Venezuela | 13.8 | |||
| Asia and Oceania | ||||
| Hong Kong SAR | 8.5 | 9.4 | 721 | 10.6 |
| Israel | 16.9 | 15.7 | 1078 | −7.1 |
| Japan | 9.0 | 9.1 | 14,285 | 1.1 |
| Kuwait | 15.2 | 17.1 | 102 | 12.5 |
| Philippines | 16.7 | |||
| Republic of Korea | 5.3 | 5.5 | 2497 | 3.8 |
| Australia | 13.3 | 11.8 | 2898 | −11.3 |
| New Zealand | 15.9 | 15.8 | 669 | −0.6 |
| Age | Age Group 20–49 | Age Group 50–69 | Age Group 70–79 | Age Group 80+ | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2012 | 2017 | Deaths | % Change | 2012 | 2017 | Deaths | % Change | 2012 | 2017 | Deaths | % Change | 2012 | 2017 | Deaths | % Change |
| North America | ||||||||||||||||
| Canada | 6.1 | 6.2 | 488 | 1.6 | 42.7 | 38.5 | 1944 | −9.8 | 86.9 | 84.2 | 1199 | −3.1 | 89.6 | 88.4 | 1687 | −1.3 |
| USA | 6.4 | 6.1 | 4139 | −4.7 | 44.4 | 40.3 | 17,170 | −9.2 | 84.8 | 78.7 | 9293 | −7.2 | 75.8 | 74.9 | 11,398 | −1.2 |
| Latin America | ||||||||||||||||
| Argentina | 8.3 | 9.0 | 838 | 8.4 | 58.5 | 55.4 | 2298 | −5.3 | 101.1 | 111.1 | 1408 | 9.9 | 90.1 | 86.9 | 1480 | −3.6 |
| Brazil | 7.1 | 7.5 | 3761 | 5.6 | 36.9 | 38.0 | 7715 | 3.0 | 57.5 | 62.2 | 2772 | 8.2 | 54.7 | 56.5 | 2475 | 3.3 |
| Chile | 5.5 | 4.6 | 197 | −16.4 | 32.0 | 31.9 | 645 | −0.3 | 58.4 | 60.7 | 323 | 3.9 | 57.7 | 49.4 | 339 | −14.4 |
| Colombia | 5.5 | 6.0 | 687 | 9.1 | 31.5 | 35.0 | 1611 | 11.1 | 54.9 | 59.3 | 536 | 8.0 | 46.7 | 54.8 | 464 | 17.3 |
| Costa Rica | 5.2 | 5.8 | 63 | 11.5 | 34.0 | 32.7 | 155 | −3.8 | 62.3 | 69.9 | 77 | 12.2 | 66.1 | 62.4 | 71 | −5.6 |
| Cuba | 6.5 | 5.5 | 163 | −15.4 | 47.8 | 40.4 | 595 | −15.5 | 87.3 | 90.5 | 355 | 3.7 | 84.2 | 80.4 | 406 | −4.5 |
| Guatemala | 3.0 | 4.2 | 121 | 40.0 | 16.4 | 15.5 | 140 | −5.5 | 19.8 | 29.7 | 60 | 50.0 | 17.9 | 15.4 | 31 | −14.0 |
| Mexico | 5.9 | 6.2 | 1795 | 5.1 | 31.7 | 33.8 | 3280 | 6.6 | 42.8 | 48.9 | 977 | 14.3 | 28.5 | 29.0 | 702 | 1.8 |
| Panama | 5.4 | 6.8 | 60 | 25.9 | 33.5 | 31.3 | 102 | −6.6 | 50.9 | 50.2 | 39 | −1.4 | 49.3 | 47.3 | 40 | −4.1 |
| Puerto Rico | 6.4 | 7.0 | 59 | 9.4 | 44.5 | 37.5 | 169 | −15.7 | 76.1 | 88.2 | 120 | 15.9 | 54.4 | 53.0 | 97 | −2.6 |
| Uruguay | 9.0 | 10.2 | 75 | 13.3 | 59.3 | 55.7 | 210 | −6.1 | 113.9 | 106.1 | 138 | −6.8 | 96.7 | 87.8 | 188 | −9.2 |
| Venezuela | 7.8 | 46.9 | 67.2 | 57.8 | ||||||||||||
| Asia and Oceania | ||||||||||||||||
| Hong Kong SAR | 4.9 | 5.6 | 125 | 14.3 | 31.1 | 35.0 | 398 | 12.5 | 31.4 | 35.3 | 83 | 12.4 | 62.6 | 52.3 | 114 | −16.5 |
| Israel | 8.1 | 8.2 | 142 | 1.2 | 52.2 | 45.4 | 372 | −13.0 | 102.2 | 99.8 | 227 | −2.3 | 227.4 | 220.3 | 337 | −3.1 |
| Japan | 5.3 | 5.2 | 1508 | −1.9 | 33.4 | 33.5 | 5856 | 0.3 | 34.3 | 38.5 | 3019 | 12.2 | 49.1 | 55.5 | 3901 | 13.0 |
| Kuwait | 3.8 | 2.3 | 25 | −39.5 | 50.9 | 33.4 | 48 | −34.4 | 87.3 | 129.0 | 20 | 47.8 | 284.3 | 697.6 | 7 | 145.4 |
| Philippines | 11.5 | 56.7 | 63.9 | 105.3 | ||||||||||||
| Korea | 4.5 | 4.7 | 648 | 4.4 | 17.2 | 17.4 | 1210 | 1.2 | 16.1 | 19.7 | 367 | 22.4 | 20.7 | 26.3 | 272 | 27.1 |
| Australia | 6.0 | 5.1 | 281 | −15.0 | 42.8 | 37.1 | 1074 | −13.3 | 80.3 | 73.7 | 635 | −8.2 | 159.4 | 157.7 | 908 | −1.1 |
| New Zealand | 9.2 | 9.1 | 95 | −1.1 | 50.6 | 48.5 | 272 | −4.2 | 84.0 | 88.1 | 134 | 4.9 | 160.2 | 173.8 | 168 | 8.5 |
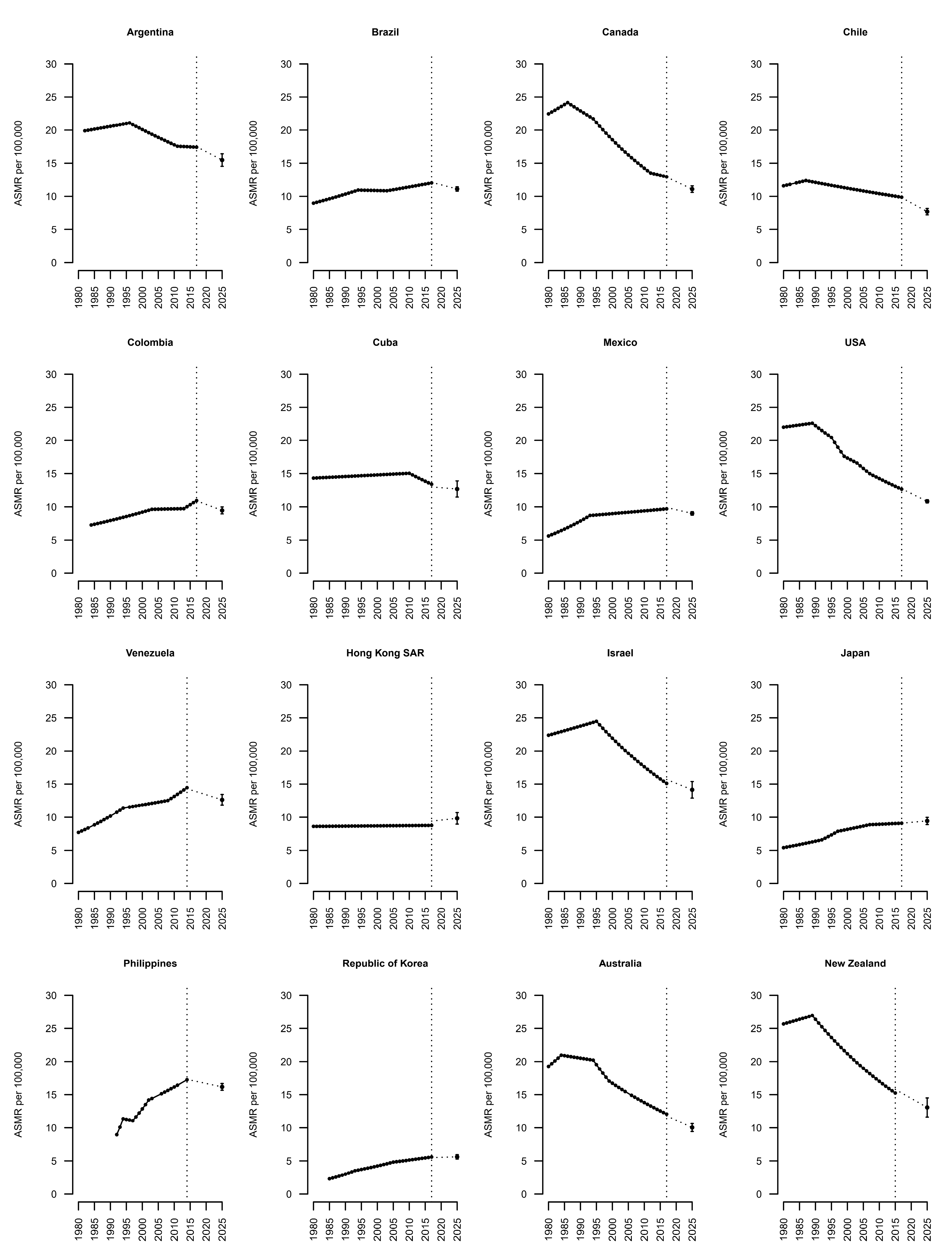
| Country | Trend 1 | APC | Trend 2 | APC | Trend 3 | APC | Trend 4 | APC | Trend 5 | APC | Trend 6 | APC | AAPC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| North America | |||||||||||||
| Canada | 1980–1986 | 1.2 b | 1986–1994 | −1.3 b | 1994–2012 | −2.6 b | 2012–2017 | −0.9 | −1.5 b | ||||
| USA | 1980–1989 | 0.3 b | 1989–1995 | −1.7 b | 1995–1999 | −3.7 b | 1999–2003 | −1.5 b | 2003–2007 | −2.5 b | 2007–2017 | −1.7 b | −1.5 b |
| Latin America | |||||||||||||
| Argentina | 1982–1996 | 0.4 b | 1996–2011 | −1.2 b | 2011–2017 | −0.1 | |||||||
| Brazil | 1980–1994 | 1.4 b | 1994–2003 | −0.1 | 2003–2017 | 0.7 b | 0.8 b | ||||||
| Chile | 1980–1987 | 1 | 1987–2017 | −0.8 b | −0.4 b | ||||||||
| Colombia | 1984–2003 | 1.5 b | 2003–2013 | 0.1 | 2013–2017 | 3 b | 1.2 b | ||||||
| Cuba | 1980–2010 | 0.2 b | 2010–2017 | −1.6 b | −0.2 | ||||||||
| Mexico | 1980–1993 | 3.4 b | 1993–2017 | 0.5 b | 1.5 b | ||||||||
| Venezuela | 1980–1994 | 2.8 b | 1994–2008 | 0.7 b | 2008–2014 | 2.4 b | 1.9 b | ||||||
| Asia and Oceania | |||||||||||||
| Hong Kong SAR | 1980–2017 | 0 | 0 | ||||||||||
| Israel | 1980–1995 | 0.6 b | 1995–2017 | −2.2 b | −1.1 b | ||||||||
| Japan | 1980–1992 | 1.7 b | 1992–1997 | 3.6 b | 1997–2007 | 1.2 b | 2007–2017 | 0.2 | 1.4 b | ||||
| Philippines | 1992–1994 | 12.6 b | 1994–1997 | −0.8 | 1997–2002 | 5.1 b | 2002–2014 | 1.6 b | 3 b | ||||
| Korea | 1985–1993 | 5.5 b | 1993–2005 | 2.7 b | 2005–2017 | 1.2 b | 2.8 b | ||||||
| Australia | 1980–1984 | 2.1 | 1984–1994 | −0.4 | 1994–1999 | −3.4 b | 1999–2017 | −1.9 b | −1.3 b | ||||
| New Zealand | 1980–1989 | 0.5 | 1989–2015 | −2.2 b | −1.5 b |
| Country | Observed Number of Deaths 2017 | Predicted Number of Deaths 2025 (95% PI) | Observed ASR 2017 | Predicted ASR 2025 (95% PI) | % Difference 2025 vs. 2017 |
|---|---|---|---|---|---|
| North America | |||||
| Canada | 5318 | 5800 (5618–6028) | 12.04 | 11.08 (10.59–11.57) | −8 |
| USA | 42,000 | 42,800 (42,047–43,454) | 12 | 10.82 (10.59–11.06) | −9.8 |
| Latin America | |||||
| Argentina | 6024 | 6700 (6269–7069) | 16.67 | 15.48 (14.54–16.43) | −7.1 |
| Brazil | 16,723 | 20,100 (19,605–20,605) | 11.5 | 11.1 (10.77–11.43) | −3.4 |
| Chile | 1504 | 1600 (1508–1674) | 9.26 | 7.69 (7.21–8.17) | −16.9 |
| Colombia | 3300 | 3700 (3446–3870) | 10.33 | 9.46 (8.95–9.98) | −8.4 |
| Cuba | 1519 | 1700 (1621–1870) | 12.17 | 12.68 (11.47–13.89) | 4.2 |
| Mexico | 6755 | 8100 (7845–8308) | 9.64 | 9.02 (8.76–9.29) | −6.4 |
| Venezuela | 2204 | 2700 (2579–2917) | 13.69 | 12.64 (11.84–13.43) | −7.7 |
| Asia and Oceania | |||||
| Hong Kong SAR | 720 | 800 (771–919) | 9.44 | 9.83 (8.96–10.69) | 4.1 |
| Israel | 1078 | 1100 (1011–1191) | 15.75 | 14.15 (12.9–15.39) | −10.2 |
| Japan | 14,284 | 16,200 (15,697–16,752) | 9.15 | 9.43 (8.9–9.97) | 3.1 |
| Philippines | 7145 | 9600 (9270–9848) | 17.25 | 16.17 (15.67–16.67) | −6.3 |
| Korea | 2497 | 2800 (2635–2913) | 5.53 | 5.62 (5.28–5.95) | 1.6 |
| Australia | 2898 | 2900 (2797–3092) | 11.76 | 10.04 (9.44–10.64) | −14.7 |
| New Zealand | 669 | 600 (578–703) | 15.78 | 13.07 (11.62–14.51) | −17.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wojtyla, C.; Bertuccio, P.; Ciebiera, M.; La Vecchia, C. Breast Cancer Mortality in the Americas and Australasia over the Period 1980–2017 with Predictions for 2025. Biology 2021, 10, 814. https://doi.org/10.3390/biology10080814
Wojtyla C, Bertuccio P, Ciebiera M, La Vecchia C. Breast Cancer Mortality in the Americas and Australasia over the Period 1980–2017 with Predictions for 2025. Biology. 2021; 10(8):814. https://doi.org/10.3390/biology10080814
Chicago/Turabian StyleWojtyla, Cezary, Paola Bertuccio, Michal Ciebiera, and Carlo La Vecchia. 2021. "Breast Cancer Mortality in the Americas and Australasia over the Period 1980–2017 with Predictions for 2025" Biology 10, no. 8: 814. https://doi.org/10.3390/biology10080814
APA StyleWojtyla, C., Bertuccio, P., Ciebiera, M., & La Vecchia, C. (2021). Breast Cancer Mortality in the Americas and Australasia over the Period 1980–2017 with Predictions for 2025. Biology, 10(8), 814. https://doi.org/10.3390/biology10080814