
Second-Generation Neuroendocrine Immunohistochemical Markers: Reflections from Clinical Implementation


Abstract
:Simple Summary
Abstract
1. Introduction
1.1. First-Generation Neuroendocrine Markers
1.2. Second-Generation Neuroendocrine Markers
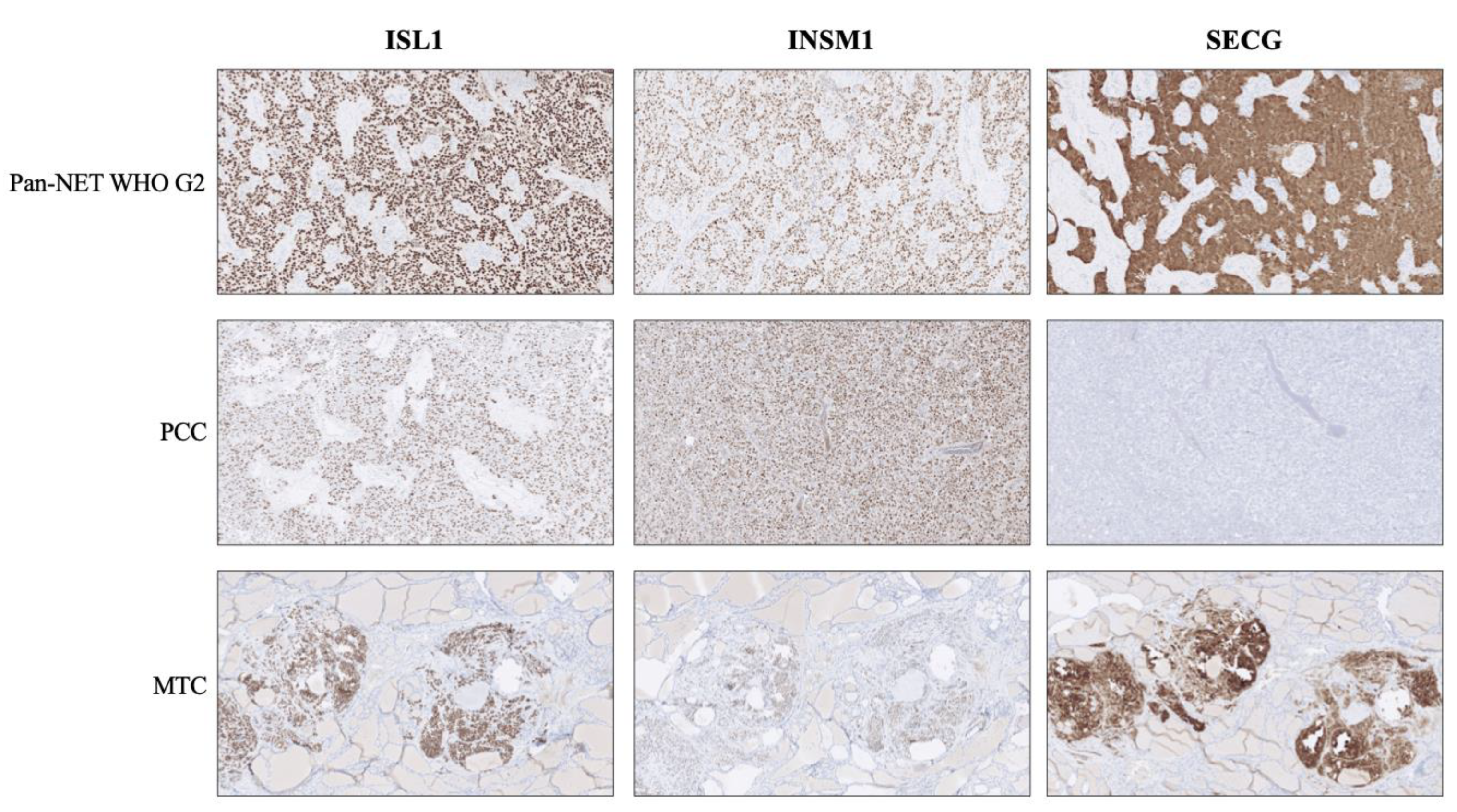
1.3. Experiences and Reflections from Clinical Implementation
2. Discussion
3. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marotta, V.; Zatelli, M.C.; Sciammarella, C.; Ambrosio, M.R.; Bondanelli, M.; Colao, A.; Faggiano, A. Chromogranin A as Circulating Marker for Diagnosis and Management of Neuroendocrine Neoplasms: More Flaws than Fame. Endocr. Relat. Cancer 2018, 25, R11–R29. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.T.; Burton, D.; Deftos, L.J. Immunoreactive Human Chromogranin A in Diverse Polypeptide Hormone Producing Human Tumors and Normal Endocrine Tissues. J. Clin. Endocrinol. Metab. 1983, 57, 1084–1086. [Google Scholar] [CrossRef]
- Lloyd, R.V.; Wilson, B.S. Specific Endocrine Tissue Marker Defined by a Monoclonal Antibody. Science 1983, 222, 628–630. [Google Scholar] [CrossRef] [PubMed]
- Wiedenmann, B.; Franke, W.W. Identification and Localization of Synaptophysin, an Integral Membrane Glycoprotein of Mr 38,000 Characteristic of Presynaptic Vesicles. Cell 1985, 41, 1017–1028. [Google Scholar] [CrossRef]
- Wiedenmann, B.; Franke, W.W.; Kuhn, C.; Moll, R.; Gould, V.E. Synaptophysin: A Marker Protein for Neuroendocrine Cells and Neoplasms. Proc. Natl. Acad. Sci. USA 1986, 83, 3500–3504. [Google Scholar] [CrossRef] [Green Version]
- Zeromski, J.; Lawniczak, M.; Galbas, K.; Jenek, R.; Golusiński, P. Expression of CD56/N-CAM Antigen and Some Other Adhesion Molecules in Various Human Endocrine Glands. Folia Histochem. Cytobiol. 1998, 36, 119–125. [Google Scholar]
- Ronkainen, H.; Soini, Y.; Vaarala, M.H.; Kauppila, S.; Hirvikoski, P. Evaluation of Neuroendocrine Markers in Renal Cell Carcinoma. Diagn Pathol. 2010, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Karpathiou, G.; Chauleur, C.; Papoudou-Bai, A.; Dagher, S.; Peoc’h, M. CD56 Is Expressed in Uterine Smooth Muscle Tumors. Int. J. Gynecol. Pathol. 2021, 40, 315–323. [Google Scholar] [CrossRef]
- Madahian, S.; Judelson, R.; Zhu, X.; Meng, X.; Dresser, K.; Hutchinson, L.; Bledsoe, J.R. CD56 Expression in Basaloid Anal Squamous Cell Carcinoma–A Potential Diagnostic Pitfall. Ann. Diagn Pathol. 2021, 53, 151758. [Google Scholar] [CrossRef] [PubMed]
- Mjønes, P.; Sagatun, L.; Nordrum, I.S.; Waldum, H.L. Neuron-Specific Enolase as an Immunohistochemical Marker Is Better Than Its Reputation. J. Histochem. Cytochem. 2017, 65, 687–703. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours of Endocrine Organs, 4th ed.; Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J.; International Agency for Research on Cancer (Eds.) World Health Organization classification of tumours; International Agency for Research on Cancer: Lyon, France, 2017; ISBN 978-92-832-4493-6. [Google Scholar]
- Karlsson, O.; Thor, S.; Norberg, T.; Ohlsson, H.; Edlund, T. Insulin Gene Enhancer Binding Protein Isl-1 Is a Member of a Novel Class of Proteins Containing Both a Homeo- and a Cys-His Domain. Nature 1990, 344, 879–882. [Google Scholar] [CrossRef]
- Ahlgren, U.; Pfaff, S.L.; Jessell, T.M.; Edlund, T.; Edlund, H. Independent Requirement for ISL1 in Formation of Pancreatic Mesenchyme and Islet Cells. Nature 1997, 385, 257–260. [Google Scholar] [CrossRef]
- Agaimy, A.; Erlenbach-Wünsch, K.; Konukiewitz, B.; Schmitt, A.M.; Rieker, R.J.; Vieth, M.; Kiesewetter, F.; Hartmann, A.; Zamboni, G.; Perren, A.; et al. ISL1 Expression Is Not Restricted to Pancreatic Well-Differentiated Neuroendocrine Neoplasms, but Is Also Commonly Found in Well and Poorly Differentiated Neuroendocrine Neoplasms of Extrapancreatic Origin. Mod. Pathol. 2013, 26, 995–1003. [Google Scholar] [CrossRef] [Green Version]
- Graham, R.P.; Shrestha, B.; Caron, B.L.; Smyrk, T.C.; Grogg, K.L.; Lloyd, R.V.; Zhang, L. Islet-1 Is a Sensitive but Not Entirely Specific Marker for Pancreatic Neuroendocrine Neoplasms and Their Metastases. Am. J. Surg. Pathol. 2013, 37, 399–405. [Google Scholar] [CrossRef]
- Schmitt, A.M.; Riniker, F.; Anlauf, M.; Schmid, S.; Soltermann, A.; Moch, H.; Heitz, P.U.; Klöppel, G.; Komminoth, P.; Perren, A. Islet 1 (Isl1) Expression Is a Reliable Marker for Pancreatic Endocrine Tumors and Their Metastases. Am. J. Surg. Pathol. 2008, 32, 420–425. [Google Scholar] [CrossRef]
- Juhlin, C.C.; Zedenius, J.; Höög, A. Clinical Routine Application of the Second-Generation Neuroendocrine Markers ISL1, INSM1, and Secretagogin in Neuroendocrine Neoplasia: Staining Outcomes and Potential Clues for Determining Tumor Origin. Endocr. Pathol. 2020, 31, 401–410. [Google Scholar] [CrossRef]
- Lan, M.S.; Li, Q.; Lu, J.; Modi, W.S.; Notkins, A.L. Genomic Organization, 5’-Upstream Sequence, and Chromosomal Localization of an Insulinoma-Associated Intronless Gene, IA-1. J. Biol. Chem. 1994, 269, 14170–14174. [Google Scholar] [CrossRef]
- Mellitzer, G.; Bonné, S.; Luco, R.F.; Van De Casteele, M.; Lenne-Samuel, N.; Collombat, P.; Mansouri, A.; Lee, J.; Lan, M.; Pipeleers, D.; et al. IA1 Is NGN3-Dependent and Essential for Differentiation of the Endocrine Pancreas. EMBO J. 2006, 25, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Kuji, S.; Watanabe, R.; Sato, Y.; Iwata, T.; Hirashima, Y.; Takekuma, M.; Ito, I.; Abe, M.; Nagashio, R.; Omae, K.; et al. A New Marker, Insulinoma-Associated Protein 1 (INSM1), for High-Grade Neuroendocrine Carcinoma of the Uterine Cervix: Analysis of 37 Cases. Gynecol. Oncol. 2017, 144, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Lilo, M.T.; Chen, Y.; LeBlanc, R.E. INSM1 Is More Sensitive and Interpretable than Conventional Immunohistochemical Stains Used to Diagnose Merkel Cell Carcinoma. Am. J. Surg. Pathol. 2018, 42, 1541–1548. [Google Scholar] [CrossRef]
- Rooper, L.M.; Sharma, R.; Li, Q.K.; Illei, P.B.; Westra, W.H. INSM1 Demonstrates Superior Performance to the Individual and Combined Use of Synaptophysin, Chromogranin and CD56 for Diagnosing Neuroendocrine Tumors of the Thoracic Cavity. Am. J. Surg. Pathol. 2017, 41, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, R.; Kobayashi, M.; Takahashi, N.; Inamura, K.; Ninomiya, H.; Wakejima, R.; Kitazono, S.; Yanagitani, N.; Horiike, A.; Ichinose, J.; et al. Insulinoma-Associated Protein 1 (INSM1) Is a Better Marker for the Diagnosis and Prognosis Estimation of Small Cell Lung Carcinoma Than Neuroendocrine Phenotype Markers Such as Chromogranin A, Synaptophysin, and CD56. Am. J. Surg. Pathol. 2020. [Google Scholar] [CrossRef]
- Staaf, J.; Tran, L.; Söderlund, L.; Nodin, B.; Jirström, K.; Vidarsdottir, H.; Planck, M.; Mattsson, J.S.M.; Botling, J.; Micke, P.; et al. Diagnostic Value of Insulinoma-Associated Protein 1 (INSM1) and Comparison With Established Neuroendocrine Markers in Pulmonary Cancers: A Comprehensive Study and Review of the Literature. Arch. Pathol. Lab. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Birkenkamp-Demtröder, K.; Wagner, L.; Brandt Sørensen, F.; Bording Astrup, L.; Gartner, W.; Scherübl, H.; Heine, B.; Christiansen, P.; Ørntoft, T.F. Secretagogin Is a Novel Marker for Neuroendocrine Differentiation. Neuroendocrinology 2005, 82, 121–138. [Google Scholar] [CrossRef]
- Wagner, L.; Oliyarnyk, O.; Gartner, W.; Nowotny, P.; Groeger, M.; Kaserer, K.; Waldhäusl, W.; Pasternack, M.S. Cloning and Expression of Secretagogin, a Novel Neuroendocrine- and Pancreatic Islet of Langerhans-Specific Ca2+-Binding Protein. J. Biol. Chem. 2000, 275, 24740–24751. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Li, Y.; Liu, R.; Li, Y.; Zhang, H.; Liu, H.; Chen, J. Secretagogin, a Marker for Neuroendocrine Cells, Is More Sensitive and Specific in Large Cell Neuroendocrine Carcinoma Compared with the Markers CD56, CgA, Syn and Napsin A. Oncol. Lett. 2020, 19, 2223–2230. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Suye, S.; Huang, R.; Liang, Q.; Fu, C. Expression and Clinical Significance of a New Neuroendocrine Marker Secretagogin in Cervical Neuroendocrine Carcinoma. J. Clin. Pathol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Juhlin, C.C.; Bertherat, J.; Giordano, T.J.; Hammer, G.D.; Sasano, H.; Mete, O. What Did We Learn from the Molecular Biology of Adrenal Cortical Neoplasia? From Histopathology to Translational Genomics. Endocr. Pathol. 2021, 32, 102–133. [Google Scholar] [CrossRef] [PubMed]
- Juhlin, C.C. Challenges in Paragangliomas and Pheochromocytomas: From Histology to Molecular Immunohistochemistry. Endocr. Pathol. 2021, 32, 228–244. [Google Scholar] [CrossRef] [PubMed]
- Baloch, Z.; Mete, O.; Asa, S.L. Immunohistochemical Biomarkers in Thyroid Pathology. Endocr. Pathol. 2018, 29, 91–112. [Google Scholar] [CrossRef]
- Erickson, L.A.; Mete, O. Immunohistochemistry in Diagnostic Parathyroid Pathology. Endocr. Pathol. 2018, 29, 113–129. [Google Scholar] [CrossRef]
- Juhlin, C.C.; Zedenius, J.; Haglund, F. Metastatic Malignant Melanoma with Neuroendocrine Differentiation: A Case Report and Review of the Literature. J. Med. Case Rep. 2020, 14, 44. [Google Scholar] [CrossRef]
- Mankuzhy, N.P.; Almahariq, M.F.; Ye, H.; Amin, M.; Stone, B.; Krauss, D.J. Investigation of the Prognostic Significance of Neuroendocrine Differentiation in Gleason Score 7 to 10 Prostate Adenocarcinoma in Patients With Distant Metastasis After Definitive Radiotherapy. Am. J. Clin. Pathol. 2021, 155, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Kriegsmann, K.; Zgorzelski, C.; Muley, T.; Christopoulos, P.; Thomas, M.; Winter, H.; Eichhorn, M.; Eichhorn, F.; von Winterfeld, M.; Herpel, E.; et al. Role of Synaptophysin, Chromogranin and CD56 in Adenocarcinoma and Squamous Cell Carcinoma of the Lung Lacking Morphological Features of Neuroendocrine Differentiation: A Retrospective Large-Scale Study on 1170 Tissue Samples. BMC Cancer 2021, 21, 486. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Bai, Q.; Wu, B.; Chang, B.; Bi, R.; Yang, W.; Wang, J.; Tu, X. Clinicopathologic and Molecular Cytogenetic Analysis of 8 Cases With Uterine Cervical Ewing Sarcoma: Case Series With Literature Review. Am. J. Surg. Pathol. 2021, 45, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S.; Dermawan, J.K.; Lanigan, C.P.; Farver, C.F. Insulinoma-Associated Protein 1 (INSM1) Is a Sensitive and Highly Specific Marker of Neuroendocrine Differentiation in Primary Lung Neoplasms: An Immunohistochemical Study of 345 Cases, Including 292 Whole-Tissue Sections. Mod. Pathol. 2019, 32, 100–109. [Google Scholar] [CrossRef]
- Yu, S.; Hornick, J.L.; Gonzalez, R.S. An Algorithmic Approach Utilizing CK7, TTF1, Beta-Catenin, CDX2, and SSTR2A Can Help Differentiate between Gastrointestinal and Pulmonary Neuroendocrine Carcinomas. Virchows Arch. 2021. [Google Scholar] [CrossRef]
- Selberherr, A.; Koperek, O.; Riss, P.; Scheuba, C.; Kaderli, R.; Perren, A.; Niederle, B. Neuroendocrine Liver Metastasis-a Specific Set of Markers to Detect Primary Tumor Sites. Endocr. Pathol. 2019, 30, 31–34. [Google Scholar] [CrossRef] [Green Version]
- Fahrenkamp, A.G.; Wibbeke, C.; Winde, G.; Ofner, D.; Böcker, W.; Fischer-Colbrie, R.; Schmid, K.W. Immunohistochemical Distribution of Chromogranins A and B and Secretogranin II in Neuroendocrine Tumours of the Gastrointestinal Tract. Virchows Arch. 1995, 426, 361–367. [Google Scholar] [CrossRef]
- La Rosa, S.; Sessa, F.; Uccella, S. Mixed Neuroendocrine-Nonneuroendocrine Neoplasms (MiNENs): Unifying the Concept of a Heterogeneous Group of Neoplasms. Endocr. Pathol. 2016, 27, 284–311. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CGA | SYP | ISL1 | INSM1 | SECG | |
|---|---|---|---|---|---|
| Lung | + | + | + | + | + |
| Pancreas | + | + | + | + | + |
| Small intestine | + | + | - | + | + |
| PPGL | + | + | + | + | - |
| Colorectum | - | + | + | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juhlin, C.C. Second-Generation Neuroendocrine Immunohistochemical Markers: Reflections from Clinical Implementation. Biology 2021, 10, 874. https://doi.org/10.3390/biology10090874
Juhlin CC. Second-Generation Neuroendocrine Immunohistochemical Markers: Reflections from Clinical Implementation. Biology. 2021; 10(9):874. https://doi.org/10.3390/biology10090874
Chicago/Turabian StyleJuhlin, Carl Christofer. 2021. "Second-Generation Neuroendocrine Immunohistochemical Markers: Reflections from Clinical Implementation" Biology 10, no. 9: 874. https://doi.org/10.3390/biology10090874
APA StyleJuhlin, C. C. (2021). Second-Generation Neuroendocrine Immunohistochemical Markers: Reflections from Clinical Implementation. Biology, 10(9), 874. https://doi.org/10.3390/biology10090874