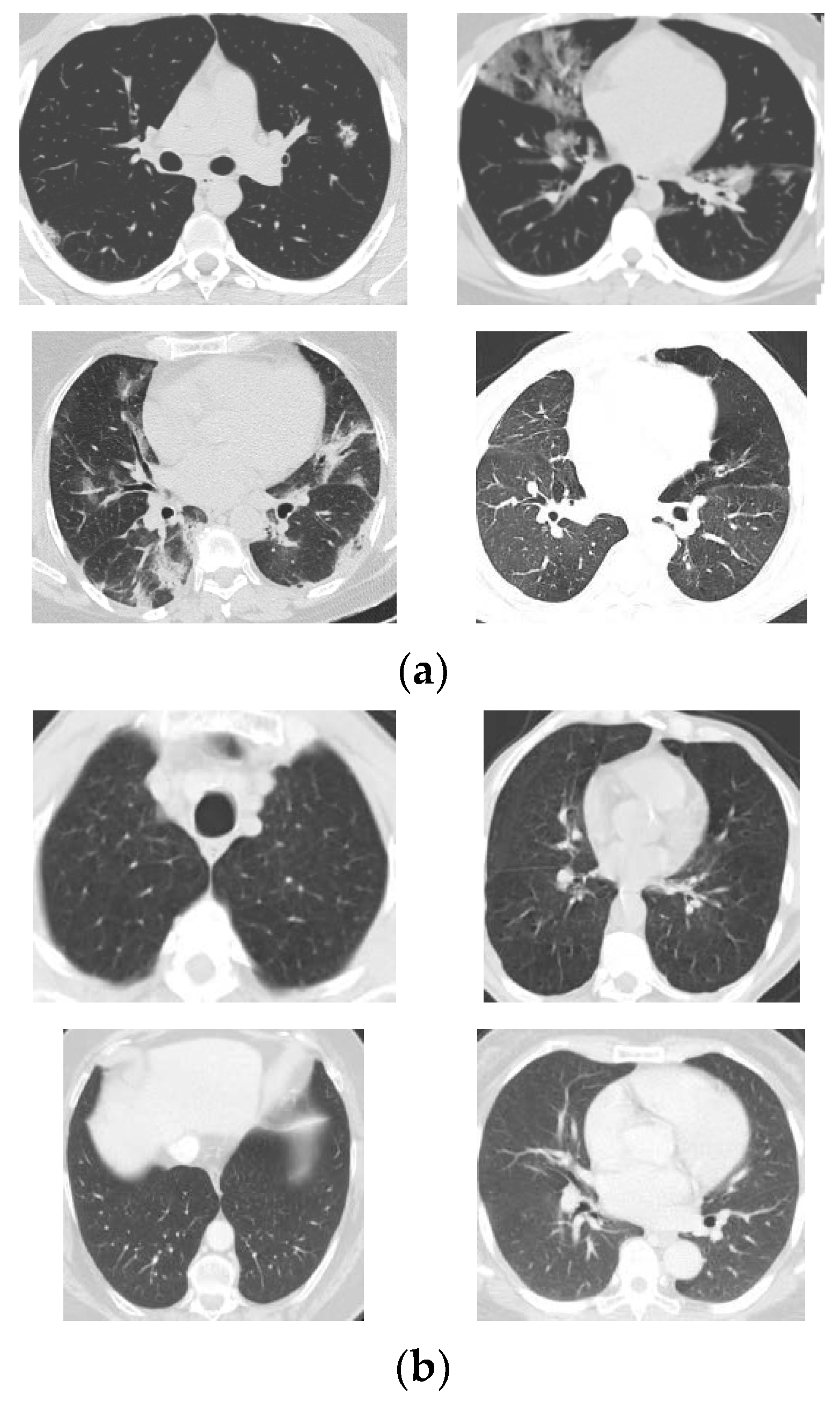
COVID-19, named by the World Health Organization, is a serious and contagious lung pneumonia caused by the coronavirus. The epidemic began in the winter of 2019 and spread worldwide shortly after. Most countries had to carry out lockdowns to control the epidemic, resulting in great economic loss. Isolating the confirmed COVID-19 cases is an effective way to control the pneumonia because the coronavirus can be transmitted among human beings by droplets. Therefore, accurate and early diagnosis is the primary step.
Sun, et al. [
2] proposed their CAD COVID-19 detection model called AFS-DF for chest CT images. Initially, local features were extracted based on CT images. Afterwards, they trained a forest to implement high-level representation learning as well as adaptive feature selection. Their method was evaluated on a dataset with multiple lung diseases, including COVID-19. The accuracy of the proposed algorithm was 91.79%. Roy, et al. [
3] suggested utilizing deep learning models to analyze automatically lung ultrasonography (LUS) images. They modified a spatial transformer network to predict the scores of the LUS frames and localize the potential lesions simultaneously. They also put forward an aggregation mechanism to generate video-level predictions. Their model achieved satisfactory results in the experiments. Oh, et al. [
4] proposed an automatic COVID-19 classification system based on chest X-ray images. A fully convolutional DenseNet was employed to generate contour patches from X-ray images. They then extracted small patches from these contour images and used these patches to train a group of pre-trained ResNets. Finally, the predictions of the original samples were generated based on the majority voting method. Ouyang, et al. [
5] discovered that COVID-19 CT datasets were usually class-imbalanced, so they proposed a dual-sampling algorithm to handle this problem. For classification, they presented an attention-based network. The 5-fold cross-validation (CV) was used to evaluate their method, and the accuracy was 87.5%. Wang, et al. [
6] presented a CAD method to implement classification and lesion localization simultaneously based on 3D CT images. Firstly, a UNet was employed for 3D image segmentation. Then, they constructed a 3D deep model named DeCoVNet, and trained it to predict the infectious probabilities. Finally, the potential lesions were localized based on the activation maps and a weakly supervised method. Wang, et al. [
7] developed their COVID-19 classification method using a COVID-Net. As the CT samples in different datasets were visually different, they tried to improve the generalization ability of COVID-Net using CT datasets from different sources. A feature normalization mechanism was implemented on the top of the COVID-Net, and the objective function was improved with a contrastive learning strategy. The performance of their model is promising. Yu, et al. [
8] tested a bunch of pre-trained deep CNN models with traditional machine learning classification algorithms. Four famous backbone models were employed to extract image features, and five classic classification algorithms were trained to identify COVID-19. Zhou, et al. [
9] developed a chest CT simulator to generate more samples from real cases to handle the data scarcity problem in training deep models for the diagnosis of COVID-19. A deep convolutional architecture was proposed for segmentation and classification which converted the tedious 3D CT segmentation into 2D segmentation. Angelov and Soares [
10] provided a large COVID-19 CT dataset and presented an explainable model for classification. Their method yielded an accuracy of 97.38%. Alam, et al. [
11] provided a CAD system using feature fusion for COVID-19 classification. They first extracted two different features sets using a gradient-based method and a convolutional neural network (CNN). Then, a VGG network was trained for classification. They also employed a watershed algorithm to segment the samples. Gupta, et al. [
12] integrated a bunch of on-the-shelf CNN models to construct their InstaCovNet-19 network which was trained to classify COVID-19 in X-ray images. Their system achieved state-of-the-art classification performance in the experiments. Jain, et al. [
13] trained an Xception network with their chest CT images to detect COVID-19. Experimental results suggested that their system produced an accuracy of 97.97%. Kc, et al. [
14] fine-tuned a pre-trained DenseNet-121 to detect COVID-19. It is reported that only 62% of the total parameters in the DenseNet-121 were re-trained in their simulation. Kumar, et al. [
15] put forward a federated learning method to detect COVID-19 using datasets from different sources with privacy protection. They invented a normalization approach to deal with the variance of the samples. Then, they trained a capsule network for every local dataset and generated their global model using federated learning. Rahimzadeh, et al. [
16] exploited ResNet-50V2 as the backbone model and proposed a feature pyramid approach to improve its classification performance for COVID-19 classification. Sadre, et al. [
17] presented a protocol to validate COVID-19 CAD systems and summarized some weaknesses in current methods. Shankar and Perumal [
18] employed a Gaussian filtering method for pre-processing of chest CT images. Afterward, they extracted deep learning features using an InceptionV3 and computed handcrafted features with the linear binary pattern algorithm. An entropy-based fusion method was employed to fuse the two types of features. Finally, a multi-layer perception was trained for classification. Zebin and Rezvy [
19] used a generative adversarial network for data augmentation in order to obtain more COVID-19 samples for training. An EfficientNet pre-trained on the ImageNet dataset was employed as the backbone. For fine-tuning, they had only to update the parameters in the fully connected layers. Zhou, et al. [
20] employed three deep CNNs for representation learning from CT images, and used softmax as the classification method. The final predictions were obtained using the relative majority voting. Wang, et al. [
21] used a deep graph neural network to classify COVID-19 samples from normal controls in chest CT images. Their model was evaluated on a private dataset and produced promising classification results. Ozturk, et al. [
22] proposed a DarkCovidNet with 17 convolutional layers to detect COVID-19 in X-ray images. For binary classification (COVID-19 versus No-findings), their model yielded a sensitivity of 95.13 based on 5-fold cross-validation.
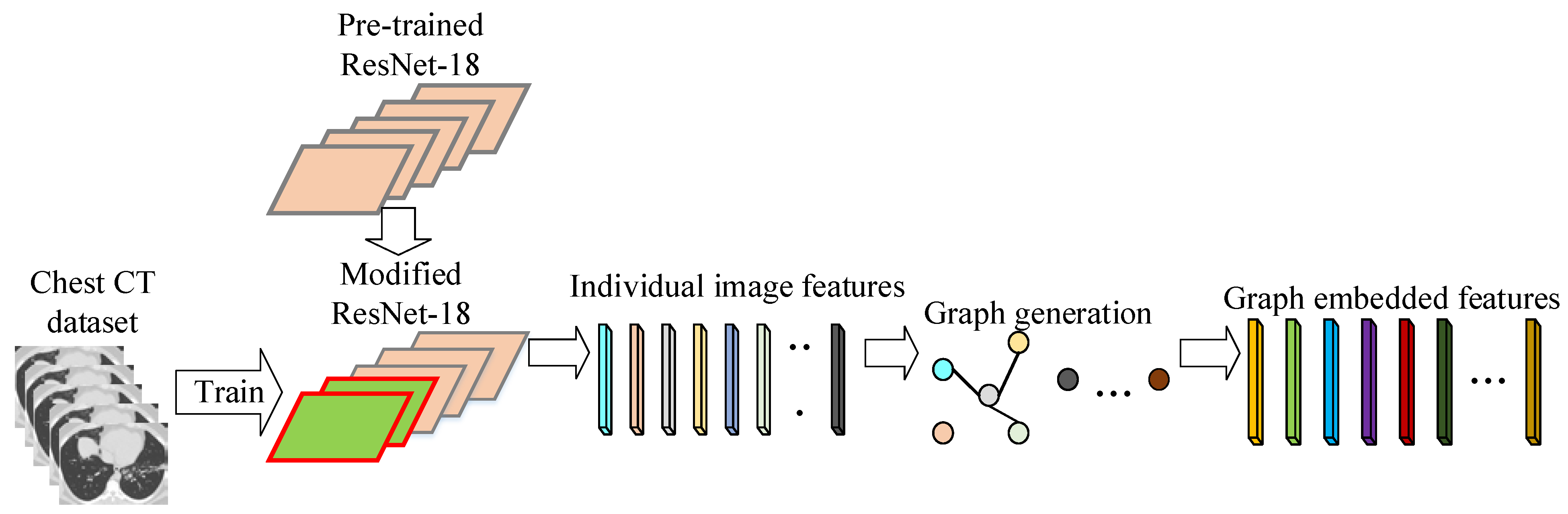
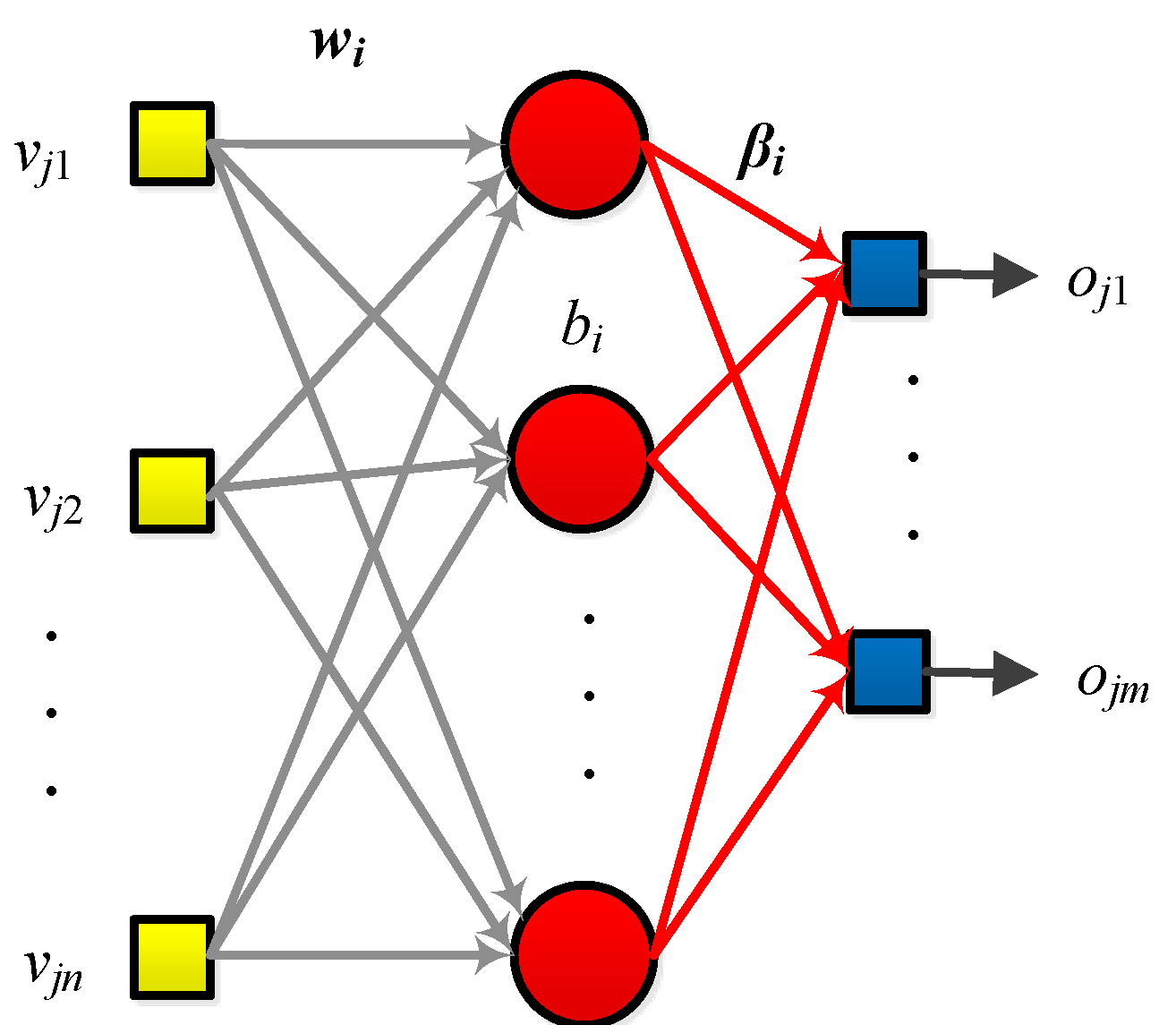
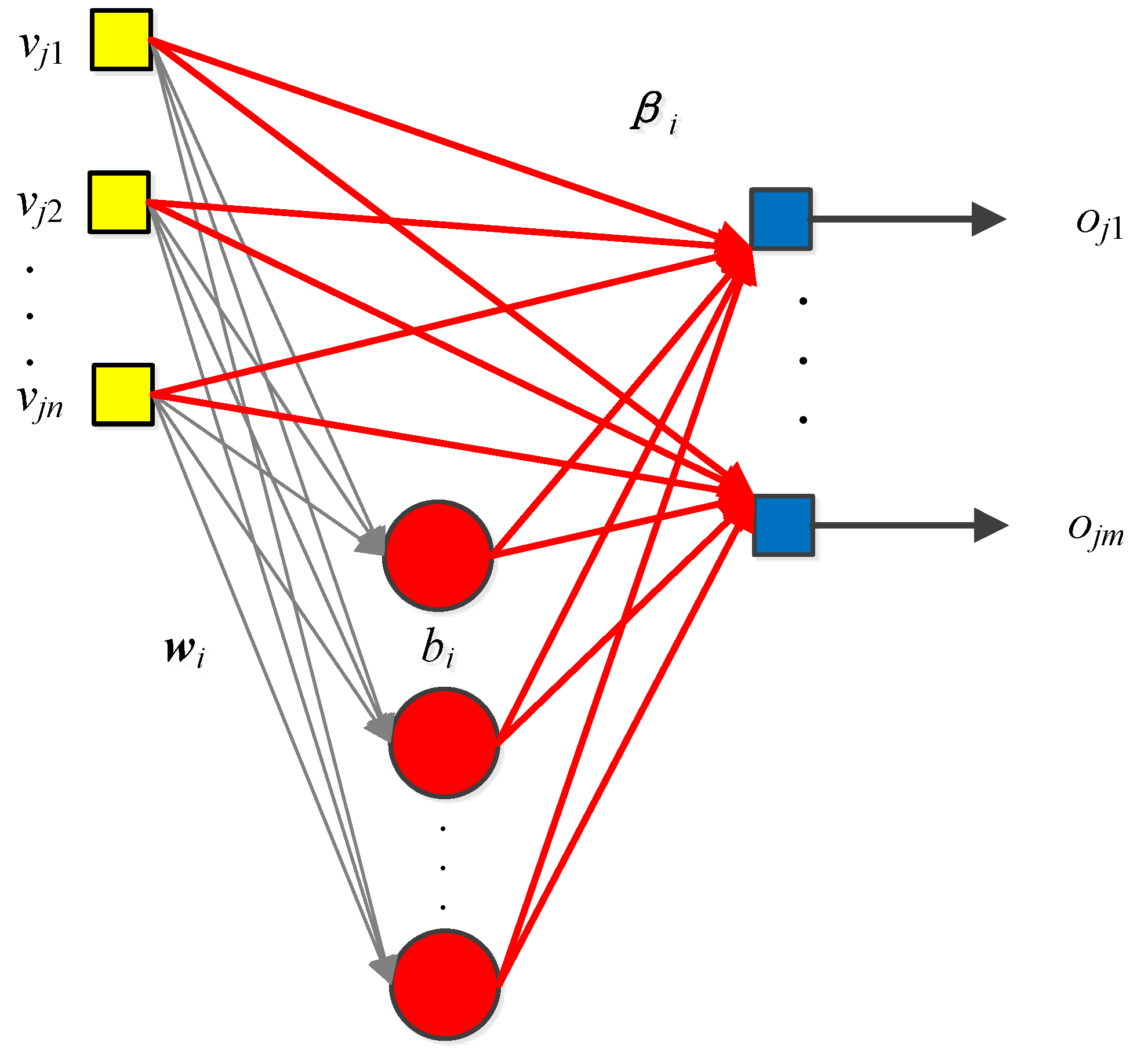
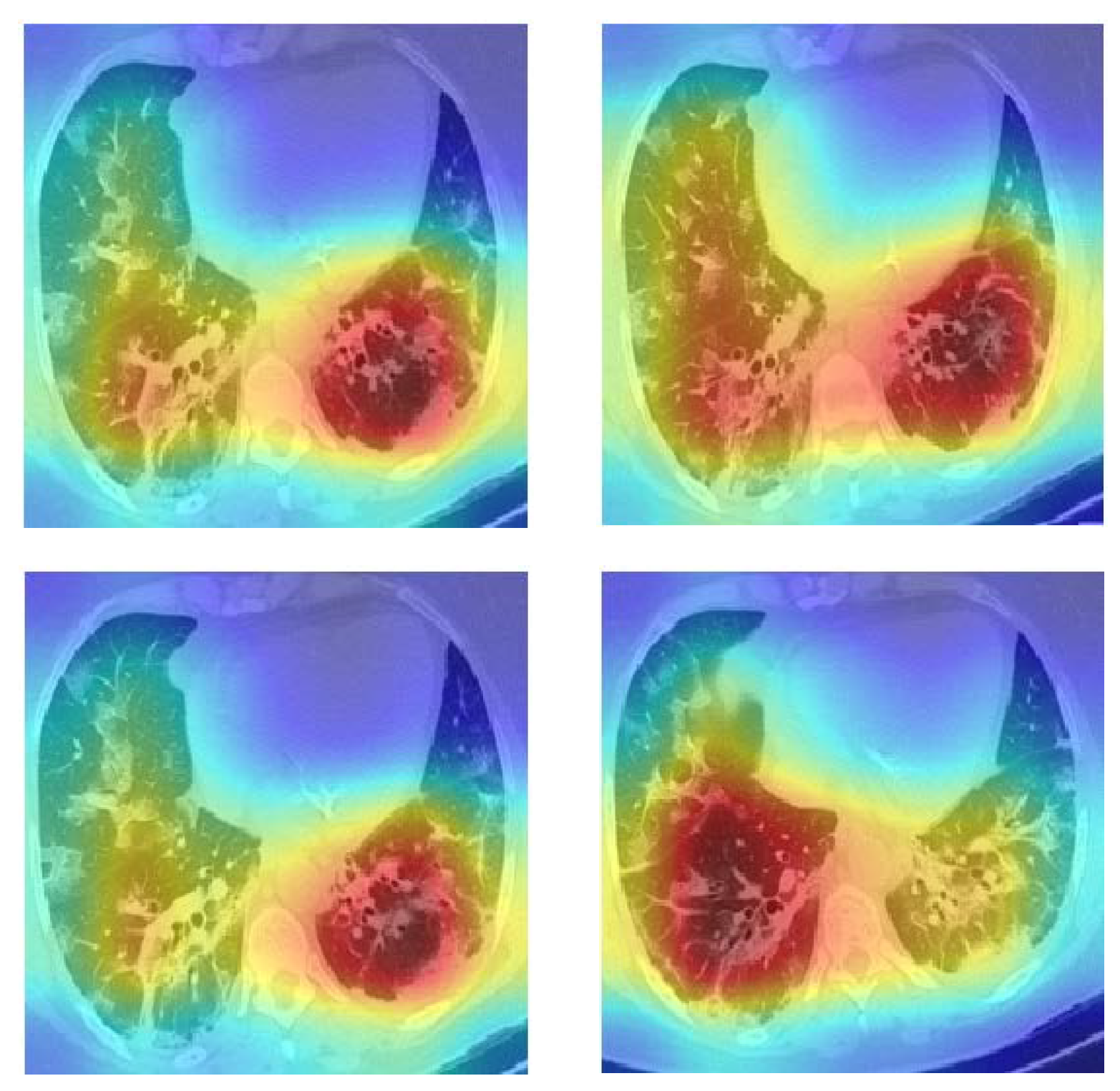
The above methods have produced promising results, but we hold the view that the classification performance can be further boosted. Many of these methods either employed deep models or traditional machine learning algorithms for classification. However, deep models usually require big datasets to train, and the training also demands a long time (usually several days) to converge. On the other side, traditional machine learning algorithms are dependent on the distribution of handcrafted features, which can be a challenge because the images contain massive information. Furthermore, the relationship among the samples can be used for classification, which is often neglected. To this end, we proposed a novel CGENet (COVID-19 Graph Extreme learning machine Network) based on the graph neural network and extreme learning machine (ELM) to detect COVID-19 in chest CT images. We put forward an optimal backbone selection algorithm to choose the best backbone model of the CGENet and leverage transfer learning to fine-tune it on the CT images. The relationship between the feature vectors in the latent space can be harnessed for the classification because the image features are closely related to their labels. It is believed that samples of the same labels should share similar features. We employed the k-NN algorithm for graph embedding in the CGENet based on the feature vectors extracted from the CT scans to leverage this relationship among the feature vectors. Finally, an ELM serves as the classifier in the CGENet to identify the samples as COVID-19 or non-COVID-19. The proposed CGENet is evaluated on a public dataset based on a 5-fold CV. The results of the experiments reveal that the CGENet yielded state-of-the-art classification performance. Meanwhile, the human readability of the deep networks is a significant topic in the development of CNN models, so the Grad-CAM is employed to offer a visual explanation of the CGENet. The regions of interest from the CGENet can be seen in the Grad-CAM maps based on the COVID-19 chest CT images. The contributions of this paper are summarized as follows:












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}