



Significant Interrelations among Serum Annexin A1, Soluble Receptor for Advanced Glycation End Products (sRAGE) and rs2070600 in Chronic Obstructive Pulmonary Disease


Abstract
:Simple Summary
Abstract
1. Introduction
2. Subjects and Methods
2.1. Subjects and Anthropometric Parameters
2.2. Blood Sample Collection and General Biochemical Marker Assays
2.3. Determination of Serum sRAGE, Annexin A1, GSH and MDA Concentrations
2.4. DNA Extraction
2.5. Genotyping
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Analysis of RAGE rs2070600 Gene Polymorphism
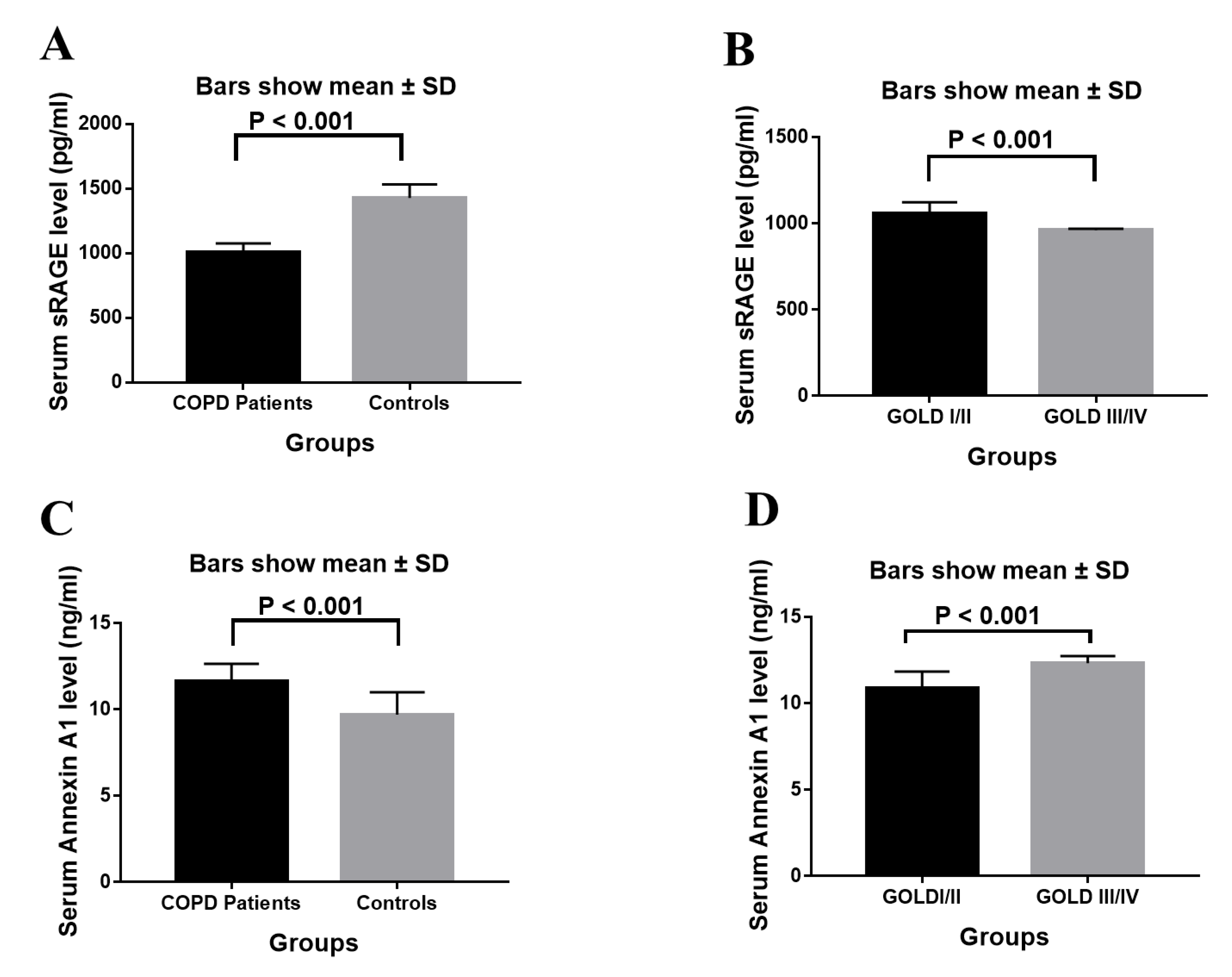
3.3. Analysis of Serum sRAGE, Annexin A1 Levels and Inflammatory Mediators
3.4. Association between sRAGE, Annexin A1 Levels and RAGE rs2070600 Polymorphism
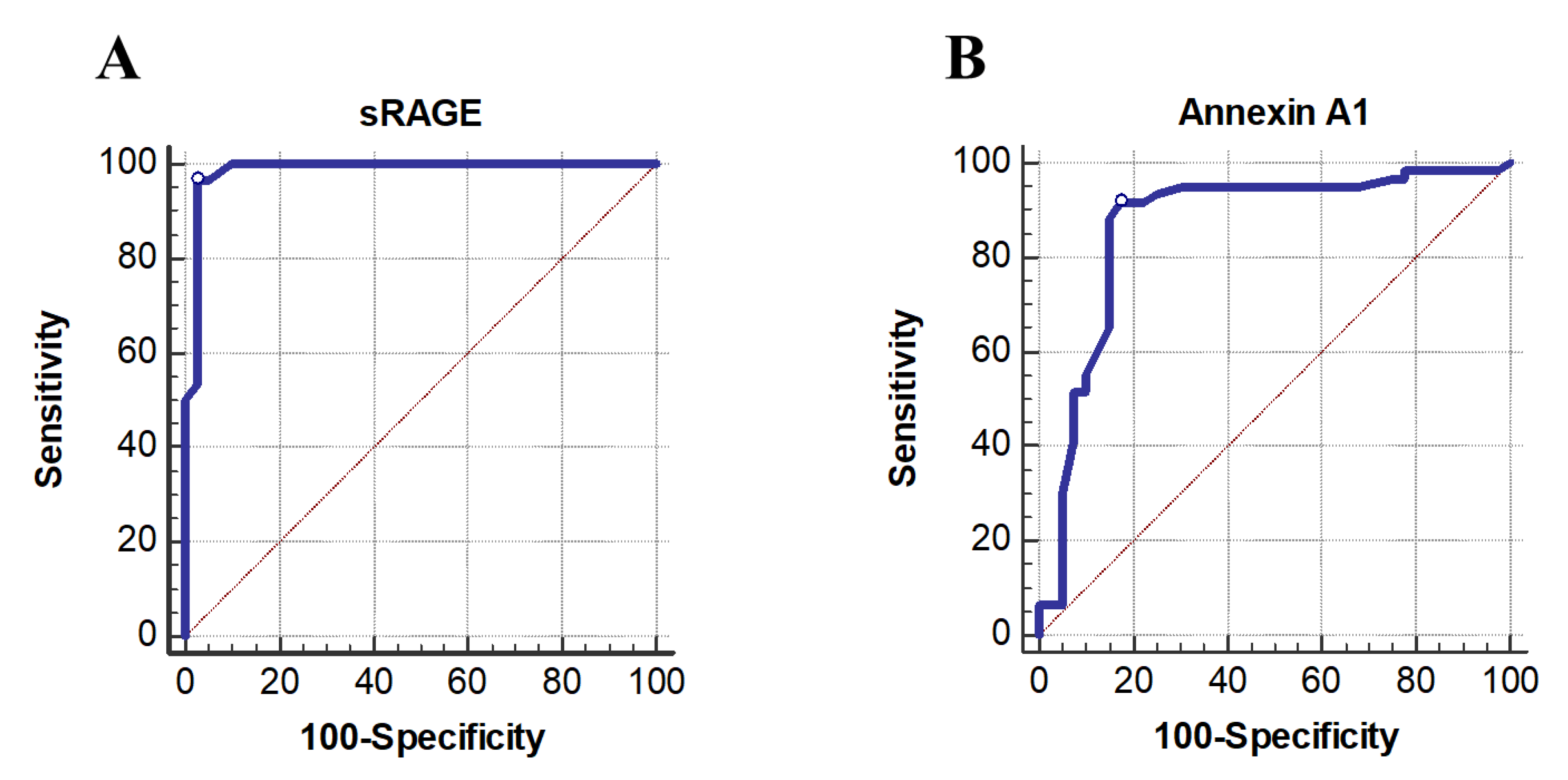
3.5. Diagnostic Performance of sRAGE and Annexin A1
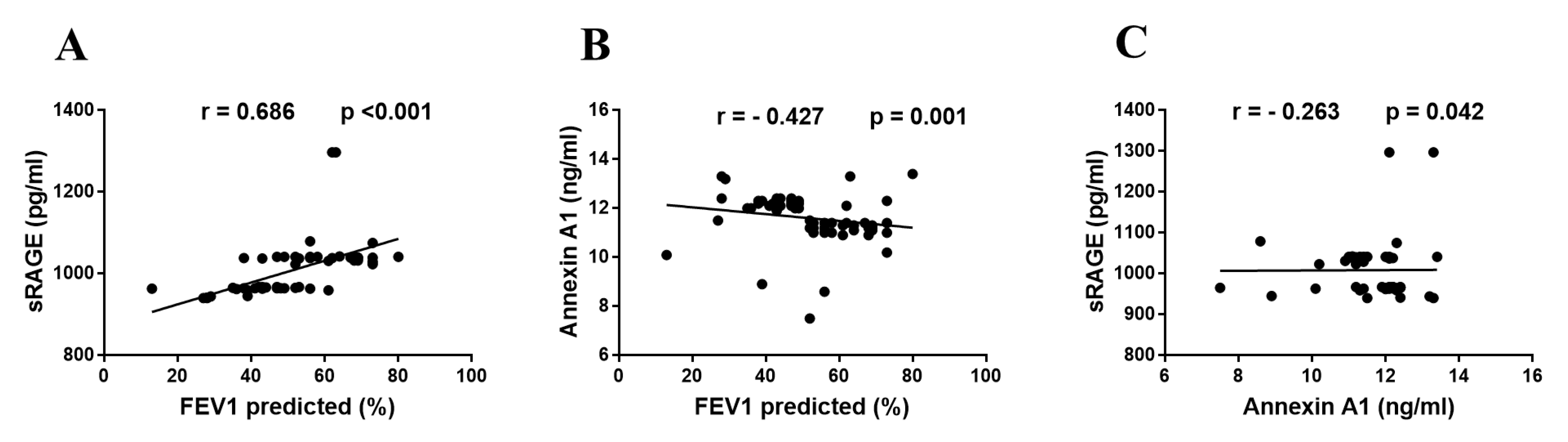
3.6. Correlations between sRAGE, Annexin A1 and FEV1 Predicted
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yonchuk, J.G.; Silverman, E.K.; Bowler, R.P.; Agustí, A.; Lomas, D.A.; Miller, B.E.; Tal-Singer, R.; Mayer, R.J. Circulating soluble receptor for advanced glycation end products (sRAGE) as a biomarker of emphysema and the RAGE axis in the lung. Am. J. Respir. Crit. Care Med. 2015, 192, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Christenson, S.A.; Smith, B.M.; Bafadhel, M.; Putcha, N. Chronic obstructive pulmonary disease. Lancet 2022, 399, 2227–2242. [Google Scholar] [CrossRef] [PubMed]
- Scaramuzzo, G.; Ottaviani, I.; Volta, C.A.; Spadaro, S. Mechanical ventilation and COPD: From pathophysiology to ventilatory management. Minerva Med. 2022, 113, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Kim, V.; Aaron, S.D. What is a COPD exacerbation? Current definitions, pitfalls, challenges and opportunities for improvement. Eur. Respir. J. 2018, 52, 1801261. [Google Scholar] [CrossRef] [PubMed]
- Gopal, P.; Rutten, E.P.; Dentener, M.A.; Wouters, E.F.; Reynaert, N.L. Decreased plasma sRAGE levels in COPD: Influence of oxygen therapy. Eur. J. Clin. Investig. 2012, 42, 807–814. [Google Scholar] [CrossRef]
- Gümüş, M.; Babacan, Ş.N.; Demir, Y.; Sert, Y.; Koca, İ.; Gülçin, İ. Discovery of sulfadrug-pyrrole conjugates as carbonic anhydrase and acetylcholinesterase inhibitors. Arch. Der Pharm. 2022, 355, e2100242. [Google Scholar] [CrossRef]
- Sharma, A.; Kaur, S.; Sarkar, M.; Sarin, B.C.; Changotra, H. The AGE-RAGE Axis and RAGE Genetics in Chronic Obstructive Pulmonary Disease. Clin. Rev. Allergy Immunol. 2021, 60, 244–258. [Google Scholar] [CrossRef]
- Perkins, T.N.; Donnell, M.L.; Oury, T.D. The axis of the receptor for advanced glycation endproducts in asthma and allergic airway disease. Allergy 2021, 76, 1350–1366. [Google Scholar] [CrossRef]
- Dong, H.; Zhang, Y.; Huang, Y.; Deng, H. Pathophysiology of RAGE in inflammatory diseases. Front. Immunol. 2022, 13, 931473. [Google Scholar] [CrossRef]
- Li, Y.; Yang, C.; Ma, G.; Gu, X.; Chen, M.; Chen, Y.; Zhao, B.; Cui, L.; Li, K. Association of polymorphisms of the receptor for advanced glycation end products gene with COPD in the Chinese population. DNA Cell Biol. 2014, 33, 251–258. [Google Scholar] [CrossRef]
- Yue, Q.; Song, Y.; Liu, Z.; Zhang, L.; Yang, L.; Li, J. Receptor for Advanced Glycation End Products (RAGE): A Pivotal Hub in Immune Diseases. Molecules 2022, 27, 4922. [Google Scholar] [CrossRef] [PubMed]
- Miłkowska-Dymanowska, J.; Białas, A.J.; Szewczyk, K.; Kurmanowska, Z.; Górski, P.; Piotrowski, W.J. The usefulness of soluble receptor for advanced glycation end-products in the identification of COPD frequent exacerbator phenotype. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 3879–3884. [Google Scholar] [CrossRef] [PubMed]
- Scavello, F.; Zeni, F.; Tedesco, C.C.; Mensà, E.; Veglia, F.; Procopio, A.D.; Bonfigli, A.R.; Olivieri, F.; Raucci, A. Modulation of soluble receptor for advanced glycation end-products (RAGE) isoforms and their ligands in healthy aging. Aging 2019, 11, 1648–1663. [Google Scholar] [CrossRef]
- Go, H.; Ohto, H.; Nollet, K.E.; Sato, K.; Miyazaki, K.; Maeda, H.; Ichikawa, H.; Chishiki, M.; Kashiwabara, N.; Kume, Y.; et al. Biomarker Potential of the Soluble Receptor for Advanced Glycation End Products to Predict Bronchopulmonary Dysplasia in Premature Newborns. Front. Pediatr. 2021, 9, 649526. [Google Scholar] [CrossRef]
- Faiz, A.; Rathnayake, S.N.H.; ten Hacken, N.H.T.; Guryev, V.; van den Berge, M.; Pouwels, S.D. Single-nucleotide polymorphism rs2070600 regulates AGER splicing and the sputum levels of the COPD biomarker soluble receptor for advanced glycation end-products. ERJ Open Res. 2021, 7, 00947-2020. [Google Scholar] [CrossRef]
- Wiersma, V.R.; Pouwels, S.D. An Integrative Genomic Strategy Identifies Soluble Receptor for Advanced Glycation End-Products as a Causal and Protective Biomarker of Lung Function. Chest 2022, 161, 3–5. [Google Scholar] [CrossRef]
- Kinjo, T.; Kitaguchi, Y.; Droma, Y.; Yasuo, M.; Wada, Y.; Ueno, F.; Ota, M.; Hanaoka, M. The Gly82Ser mutation in AGER contributes to pathogenesis of pulmonary fibrosis in combined pulmonary fibrosis and emphysema (CPFE) in Japanese patients. Sci. Rep. 2020, 10, 12811. [Google Scholar] [CrossRef]
- Li, L.; Xu, L.; Chen, W.; Li, X.; Xia, Q.; Zheng, L.; Duan, Q.; Zhang, H.; Zhao, Y. Reduced Annexin A1 Secretion by ABCA1 Causes Retinal Inflammation and Ganglion Cell Apoptosis in a Murine Glaucoma Model. Front. Cell. Neurosci. 2018, 12, 347. [Google Scholar] [CrossRef]
- Kelly, L.; McGrath, S.; Rodgers, L.; McCall, K.; Virlan, A.T.; Dempsey, F.; Crichton, S.; Goodyear, C.S. Annexin-A1: The culprit or the solution? Immunology 2022, 166, 2–16. [Google Scholar] [CrossRef]
- Takaoka, R.T.C.; Sertório, N.D.; Magalini, L.P.J.; Dos Santos, L.M.; Souza, H.R.; Iyomasa-Pilon, M.M.; Possebon, L.; Costa, S.S.; Girol, A.P. Expression profiles of Annexin A1, formylated peptide receptors and cyclooxigenase-2 in gastroesophageal inflammations and neoplasias. Pathol. Res. Pract. 2018, 214, 181–186. [Google Scholar] [CrossRef]
- Rabe, K.F.; Hurd, S.; Anzueto, A.; Barnes, P.J.; Buist, S.A.; Calverley, P.; Fukuchi, Y.; Jenkins, C.; Rodriguez-Roisin, R.; van Weel, C.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2007, 176, 532–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erusalimsky, J.D. The use of the soluble receptor for advanced glycation-end products (sRAGE) as a potential biomarker of disease risk and adverse outcomes. Redox Biol. 2021, 42, 101958. [Google Scholar] [CrossRef] [PubMed]
- Pratte, K.A.; Curtis, J.L.; Kechris, K.; Couper, D.; Cho, M.H.; Silverman, E.K.; DeMeo, D.L.; Sciurba, F.C.; Zhang, Y.; Ortega, V.E.; et al. Soluble receptor for advanced glycation end products (sRAGE) as a biomarker of COPD. Respir. Res. 2021, 22, 127. [Google Scholar] [CrossRef] [PubMed]
- Cockayne, D.A.; Cheng, D.T.; Waschki, B.; Sridhar, S.; Ravindran, P.; Hilton, H.; Kourteva, G.; Bitter, H.; Pillai, S.G.; Visvanathan, S.; et al. Systemic biomarkers of neutrophilic inflammation, tissue injury and repair in COPD patients with differing levels of disease severity. PLoS ONE 2012, 7, e38629. [Google Scholar] [CrossRef]
- Iwamoto, H.; Gao, J.; Pulkkinen, V.; Toljamo, T.; Nieminen, P.; Mazur, W. Soluble receptor for advanced glycation end-products and progression of airway disease. BMC Pulm. Med. 2014, 14, 68. [Google Scholar] [CrossRef] [Green Version]
- Sanches, J.M.; Branco, L.M.; Duarte, G.H.B.; Oliani, S.M.; Bortoluci, K.R.; Moreira, V.; Gil, C.D. Annexin A1 Regulates NLRP3 Inflammasome Activation and Modifies Lipid Release Profile in Isolated Peritoneal Macrophages. Cells 2020, 9, 926. [Google Scholar] [CrossRef] [Green Version]
- Lai, T.; Li, Y.; Mai, Z.; Wen, X.; Lv, Y.; Xie, Z.; Lv, Q.; Chen, M.; Wu, D.; Wu, B. Annexin A1 is elevated in patients with COPD and affects lung fibroblast function. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 473–486. [Google Scholar] [CrossRef] [Green Version]
- Rastrick, J.M.; Stevenson, C.S.; Eltom, S.; Grace, M.; Davies, M.; Kilty, I.; Evans, S.M.; Pasparakis, M.; Catley, M.C.; Lawrence, T.; et al. Cigarette smoke induced airway inflammation is independent of NF-κB signalling. PLoS ONE 2013, 8, e54128. [Google Scholar] [CrossRef]
- Gallucci, G.; Tartarone, A.; Lerose, R.; Lalinga, A.V.; Capobianco, A.M. Cardiovascular risk of smoking and benefits of smoking cessation. J. Thorac. Dis. 2020, 12, 3866–3876. [Google Scholar] [CrossRef]
- He, Y.; Zhang, Y.; Wu, H.; Luo, J.; Cheng, C.; Zhang, H. The role of annexin A1 peptide in regulating PI3K/Akt signaling pathway to reduce lung injury after cardiopulmonary bypass in rats. Perfusion 2021, 2676591211052162. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| COPD Patients (n = 60) | Controls (n = 40) | p-Value | |
|---|---|---|---|
| Age (Year) | |||
| Mean ± SD | 62.65 ± 6.49 | 61.45 ± 5.72 | 0.345 |
| Sex | |||
| Male n (%) | 50 (83.3%) | 32 (80%) | 0.671 |
| Female n (%) | 10 (16.7%) | 8 (20%) | |
| BMI (kg/m2) | |||
| Mean ± SD | 26.42 ± 6.72 | 28.362 ± 6.29 | 0.067 |
| Smoking Status n (%) | |||
| Current | 15 (25) | 8 (20) | <0.001 |
| Ex | 39 (65) | 7 (17.5) | |
| None | 6 (10) | 25 (62.5) | |
| Comorbidity n (%) | NA | ||
| DM | 9 (15) | ||
| HTN | 14 (23.3) | ||
| Cardiovascular | 4 (6.7) | ||
| None | 33 (55) | ||
| Exacerbations n (%) | NA | ||
| None or One | 19 (31.7) | ||
| Two or More | 41 (68.3) | ||
| History n (%) | NA | ||
| Cough | 8 (13.3) | ||
| Dyspnea | 9 (15) | ||
| Cough, Dyspnea | 31 (51.7) | ||
| Cough, Dyspnea, Wheezes | 12 (20) | ||
| FEV1/FVC (%) post-bronchodilator | |||
| Mean ± SD | 53.28 ± 8.1721 | 77.05 ± 4.37 | <0.001 |
| FEV1 (%) Predicted | |||
| Mean ± SD | 51.48 ± 13.76 | 85.0 ± 2.85 | <0.001 |
| GOLD staging n (%) | NA | ||
| Mild | 4 (6.7) | ||
| Moderate | 26 (43.3) | ||
| Severe | 25 (41.7) | ||
| Very severe | 5 (8.3) |
| COPD Patients (n = 60) | Controls (n = 40) | p-Value | |
|---|---|---|---|
| WBC (10 × 3/µL) | |||
| Mean ± SD | 7.41 ± 1.9 | 7.78 ± 1.65 | 0.26 |
| Hb (g/dL) | |||
| Mean ± SD | 13.11 ± 1.49 | 12.6 ± 1.54 | 0.167 |
| HCT (%) | |||
| Mean ± SD | 42.75 ± 4.36 | 41.21 ± 4.52 | 0.135 |
| PLT (10 × 3/µL) | |||
| Mean ± SD | 209.05 ± 55.49 | 206.27 ± 54.71 | 0.74 |
| Urea (mmol/L) | |||
| Mean ± SD | 6.8 ± 2.32 | 6.55 ± 1.98 | 0.708 |
| Creatinine (µmol/L) | |||
| Mean ± SD | 79.7± 24.88 | 77.57 ± 23.59 | 0.554 |
| Bilirubin (mg/dL) | |||
| Mean ± SD | 0.66 ± 0.26 | 0.65 ± 0.23 | 0.792 |
| Total serum Protein (g/dL) | |||
| Mean ± SD | 6.3 ± 0.57 | 6.52 ± 0.64 | 0.149 |
| Albumin (g/dL) | |||
| Mean ± SD | 3.41 ± 0.24 | 3.46 ± 0.21 | 0.331 |
| ALT (U/L) | |||
| Mean ± SD | 23.1 ± 8.04 | 22.3 ± 7.28 | 0.565 |
| AST (U/L) | |||
| Mean ± SD | 32.11 ± 7.1 | 31.32 ± 6.47 | 0.367 |
| ESR (mm/h) | |||
| Mean ± SD | 17.7 ± 12.54 | 15.95 ± 10.61 | 0.37 |
| pH | |||
| Mean ± SD | 7.415 ± 0.023 | 7.409 ± 0.022 | 0.17 |
| PaCO2 (mmHg) | |||
| Mean ± SD | 55.383 ± 6.86 | 41.0 ± 3.70 | <0.001 |
| PaO2 (mmHg) | |||
| Mean ± SD | 75.9 ± 7.04 | 80.07 ± 4.72 | 0.003 |
| SaO2 (%) | |||
| Mean ± SD | 94.8 ± 1.18 | 95.62 ± 1.19 | 0.001 |
| HCO3 (mEq/L) | |||
| Mean ± SD | 37.53 ± 4.81 | 25.85 ± 2.39 | <0.001 |
| COPD Patients (n = 60) | Controls (n = 40) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Genotype | ||||
| GG | 17 (28.3%) | 25 (62.5%) | 0.237 (0.101–0.556) | 0.001 |
| GA | 33 (55%) | 10 (25%) | 3.667 (1.524–8.822) | 0.003 |
| AA | 10 (16.7%) | 5 (12.5%) | 1.4 (0.44–4.453) | 0.568 |
| Allele | ||||
| G | 67 (55.8%) | 60 (75%) | 0.421 (0.226–0.784) | 0.006 |
| A | 53 (44.2%) | 20 (25%) |
| Smokers (Current and Ex) (n = 69) | Non-Smokers (n = 31) | |||||||
|---|---|---|---|---|---|---|---|---|
| Genotype | COPD Patients (n = 54) | Controls (n = 15) | OR (95% CI) | p-Value | COPD Patients (n = 6) | Controls (n = 25) | OR (95% CI) | p-Value |
| GG | 14 (25.9%) | 7 (46.7%) | 0.40 (0.123–1.306) | 0.122 | 3 (50%) | 18 (72%) | 0.389 (0.063–2.407) | 0.301 |
| GA | 31 (57.4%) | 4 (26.7%) | 3.707 (1.046–13.134) | 0.035 | 2 (33.3%) | 6 (24%) | 1.583 (0.230–10.904) | 0.639 |
| AA | 9 (16.7%) | 4 (26.7%) | 0.550 (0.143–2.121) | 0.381 | 1 (16.7%) | 1 (4%) | 4.800 (0.255–90.298) | 0.257 |
| Allele | ||||||||
| G | 59 (54.6%) | 18 (60%) | 0.803 (0.353–1.828) | 0.600 | 8 (66.7%) | 42 (84%) | 0.381 (0.092–1.574) | 0.172 |
| A | 49 (45.4%) | 12 (40%) | 4 (33.3%) | 8 (16%) | ||||
| COPD Patients (n = 60) | Controls (n = 40) | p-Value | COPD Patients GOLD I, II (n = 30) | COPD Patients GOLD III, IV (n = 30) | p-Value | |
|---|---|---|---|---|---|---|
| sRAGE pg/mL Mean ± SD | 1008.78 ± 67.50 | 1428.32 ± 103.49 | <0.001 | 1057.0 ± 66.21 | 960.57± 8.74 | <0.001 |
| Annexin A1 (ng/mL) Mean ± SD | 11.608 ± 1.03 | 9.697 ± 1.3 | <0.001 | 11.41 ± 0.87 | 11.81 ± 1.15 | 0.002 |
| MDA (nmol/mL) Mean ± SD | 6.88 ± 1.72 | 3.39 ± 0.71 | <0.001 | 5.36 ± 0.78 | 8.4± 0.8 | <0.001 |
| GSH (mmol/L) Mean ± SD | 16.33 ± 2.76 | 41.91 ± 3.79 | <0.001 | 18.68 ± 1.02 | 13.98 ± 1.75 | <0.001 |
| COPD Patients | |||||||
|---|---|---|---|---|---|---|---|
| GG (n = 17) | GA (n = 33) | AA (n = 10) | P1 | P2 | P3 | P4 | |
| sRAGE pg/mL | |||||||
| Mean ± SD | 1059.88 ± 95.59 | 994.3 ± 39.539 | 969.7 ± 25.83 | <0.001 | 0.001 | 0.257 | <0.001 |
| Annexin A1 (ng/mL) | |||||||
| Mean ± SD | 11.56 ± 1.04 | 11.79 ± 0.75 | 11.1 ± 1.61 | 0.177 | 0.453 | 0.066 | 0.262 |
| Controls | |||||||
| GG | GA | AA | P1 | P2 | P3 | P4 | |
| (n = 25) | (n = 10) | (n = 5) | |||||
| sRAGE pg/mL | |||||||
| Mean ± SD | 1473.68 ± 40.86 | 1407.1 ± 32.49 | 1202.8 ± 131.83 | <0.001 | 0.003 | <0.001 | <0.001 |
| Annexin A1 (ng/mL) | |||||||
| Mean ± SD | 9.8 ± 1.4 | 9.46 ± 1.33 | 9.64 ± 0.63 | 0.782 | 0.491 | 0.805 | 0.801 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamel, A.A.; Hashem, M.K.; AbdulKareem, E.S.; Ali, A.H.; Mahmoud, E.A.-R.; Abd-Elkader, A.S.; Abdellatif, H.; Abdelbadea, A.; Abdel-Rady, N.M.; Al Anany, M.G.E.; et al. Significant Interrelations among Serum Annexin A1, Soluble Receptor for Advanced Glycation End Products (sRAGE) and rs2070600 in Chronic Obstructive Pulmonary Disease. Biology 2022, 11, 1707. https://doi.org/10.3390/biology11121707
Kamel AA, Hashem MK, AbdulKareem ES, Ali AH, Mahmoud EA-R, Abd-Elkader AS, Abdellatif H, Abdelbadea A, Abdel-Rady NM, Al Anany MGE, et al. Significant Interrelations among Serum Annexin A1, Soluble Receptor for Advanced Glycation End Products (sRAGE) and rs2070600 in Chronic Obstructive Pulmonary Disease. Biology. 2022; 11(12):1707. https://doi.org/10.3390/biology11121707
Chicago/Turabian StyleKamel, Amira A., Maiada K. Hashem, Ebtsam S. AbdulKareem, Amal H. Ali, Ekram Abdel-Rahman Mahmoud, Alaa S. Abd-Elkader, Hebatallah Abdellatif, Alzahra Abdelbadea, Nessren M. Abdel-Rady, Mona Gamal E. Al Anany, and et al. 2022. "Significant Interrelations among Serum Annexin A1, Soluble Receptor for Advanced Glycation End Products (sRAGE) and rs2070600 in Chronic Obstructive Pulmonary Disease" Biology 11, no. 12: 1707. https://doi.org/10.3390/biology11121707