High Intensity Training Improves Health and Physical Function in Middle Aged Adults


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants

{kind=link}
{kind=link}
{kind=link}
| Parameter | CON | HIT | ||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| Sex | 1 male, 5 female | 2 male, 6 female | ||
| Age (y) | 42 ± 8 | 42 ± 8 | 43 ± 8 | 43 ± 8 |
| Height (cm) | 162 ± 7 | 162 ± 7 | 165 ± 7 | 165 ± 7 |
| Weight (kg) | 64 ± 9 | 64 ± 10 | 80 ± 8 | 79 ± 9 |
| BMI (kg·m−2) | 24.3 ± 1.9 | 24.3 ± 1.6 | 29.5 ± 4.1 | 29.1 ± 4.6 † |
| Energy Intake (Kcal·d−1) | 4651 ± 1767 | 4361 ± 1544 | 5217 ± 1918 | 5567 ± 1262 |
| Systolic Blood Pressure (mmHg) | 128 ± 20 | 127 ± 11 | 137 ± 11 | 133 ± 9 |
| Diastolic Blood Pressure (mmHg) | 77 ± 11 | 78 ± 7 | 81 ± 9 | 79 ± 5 |
| Fasting glucose (mmol·L−1) | 4.3 ± 0.5 | 4.2 ± 0.5 | 4.6 ± 0.3 | 4.3 ± 0.2 *† |
| 2h glucose (mmol·L−1) | 4.7 ± 0.9 | 4.5 ± 1.1 | 5.4 ± 1.3 | 4.8 ± 1.2 *† |
2.2. Experimental Protocol
2.2.1. Session 1: Oral Glucose Tolerance Test (OGTT)
2.2.2. Session 2: Physical Function
2.2.2.1. Get Up and Go
2.2.2.2. Sit to Stand
2.2.2.3. 50 Metre Loaded Walk
2.2.3. Time to Exhaustion
2.2.4. High Intensity Training
2.2.5. Post-Training Assessment
2.2.6. Calculations and Statistical Analysis
3. Results and Discussion
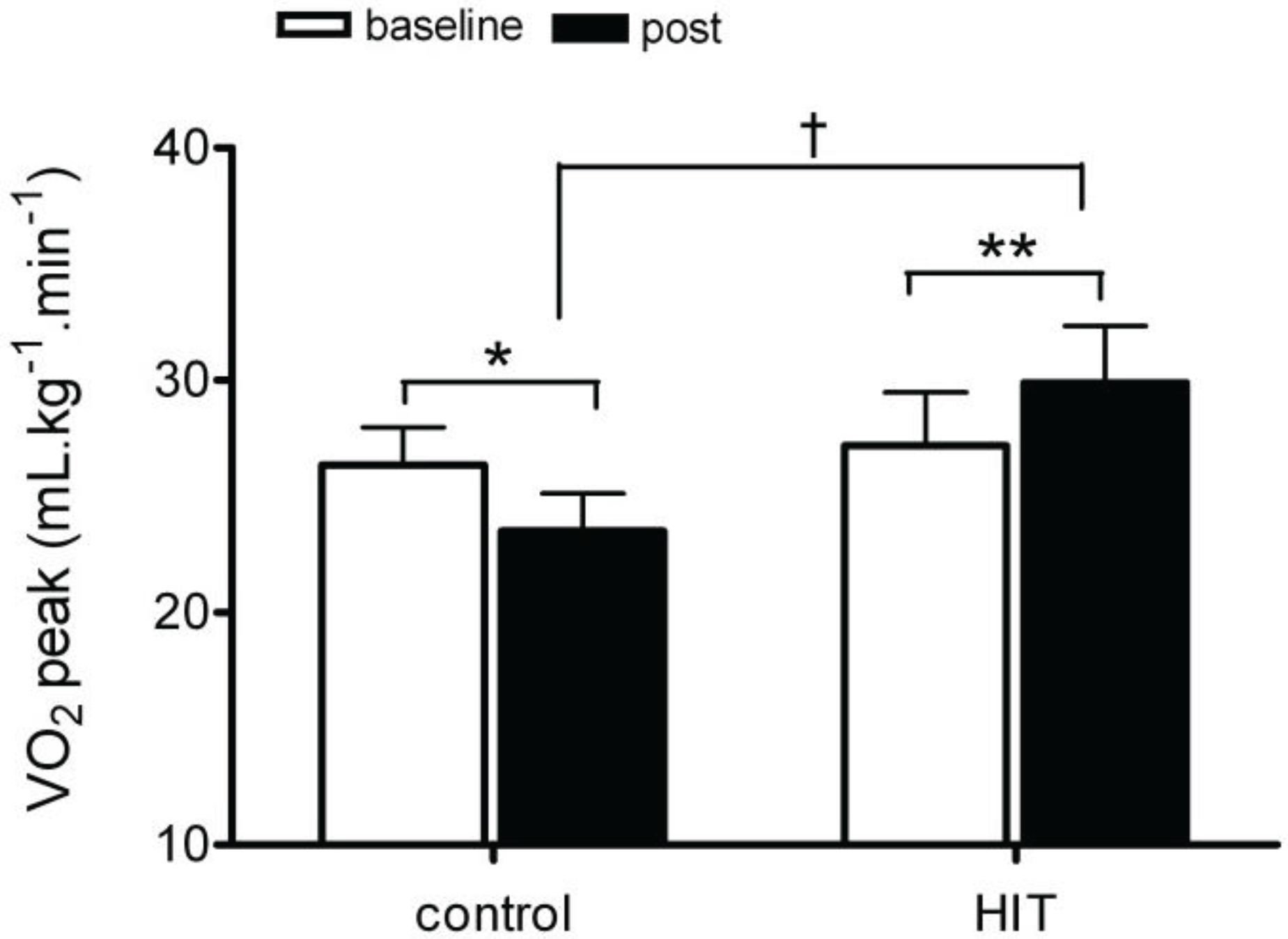
3.1. VO2 Peak

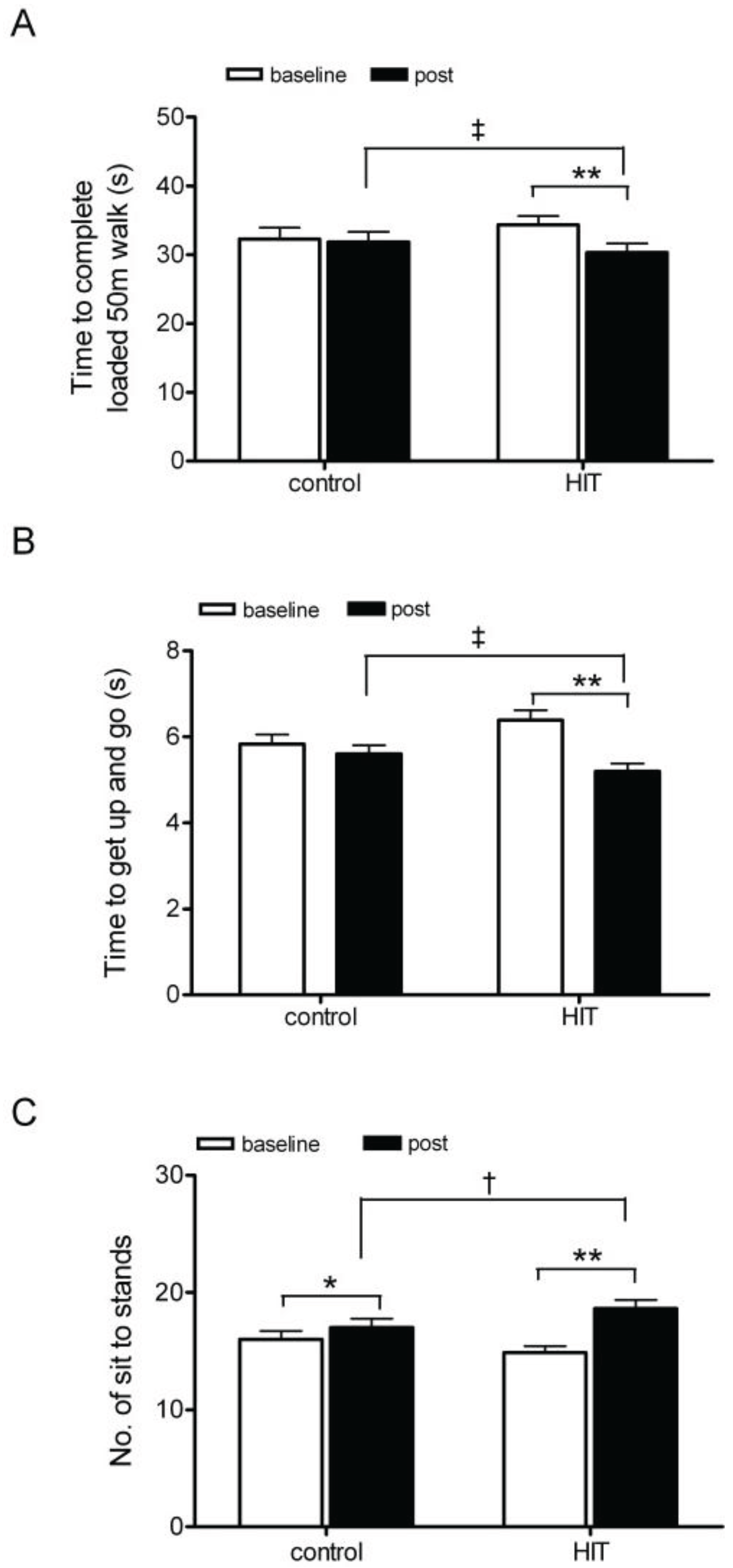
3.2. Functional Capacity

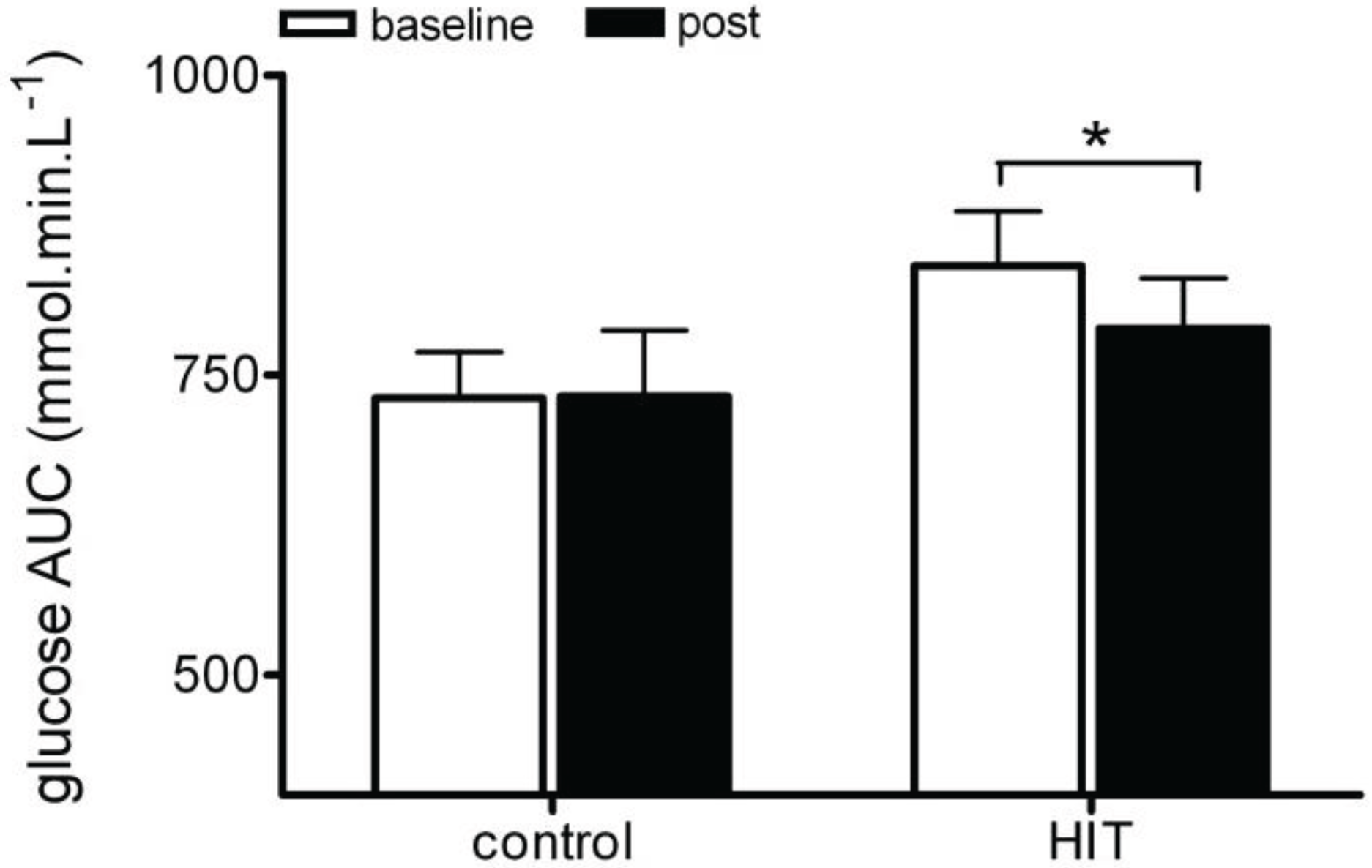
3.3. Plasma Glucose AUC

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Short, K.R.; Vittone, J.L.; Bigelow, M.L.; Proctor, D.N.; Rizza, R.A.; Coenen-Schmike, J.M. Impact of aerobic exercise training on age related changes in insulin sensitivity and muscle oxidative capacity. Diabetes 2003, 52, 1888–1896. [Google Scholar] [CrossRef]
- Samson, M.M.; Meeuwsen, I.B.A.E.; Crowe, A.; Dessens, J.A.G.; Duursma, S.A.; Verhaar, H.J.J. Relationships between physical performance measures, age, height and body weight in healthy adults. Age Ageing 2000, 29, 235–242. [Google Scholar] [CrossRef]
- Rooyackers, O.E.; Adey, D.B.; Ades, P.A.; Nair, K.S. Effect of age on in vivo rates of mitochondrial protein synthesis in human skeletal muscle. Proc. Natl. Acad. Sci. USA 1996, 93, 15364–15369. [Google Scholar] [CrossRef]
- Pederson, B.; Saltin, B. Evidence for prescribing exercise as therapy in chronic disease. Scand. J. Med. Sci. Sports 2006, 16, 3–63. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler S, E.; Hamman R, F.; Lachin, J.M.; Walker, E.A. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar]
- Laaksonen, D.E.; Lindström, J.; Lakka, T.A.; Eriksson, J.G.; Niskanen, L.; Wikström, K.; Aunola, S.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Valle, TT.; et al. Physical activity in the prevention of type 2 diabetes—The Finnish Diabetes Prevention Study. Diabetes 2005, 54, 158–165. [Google Scholar] [CrossRef]
- Houmard, J.A.; Shinebarger, M.H.; Dolan, P.L.; Leggett-Frazier, N.; Bruner, R.K.; McCammon, M.R.; Israel, R.G.; Dohm, G.L. Exercise training increases GLUT-4 protein concentration in previously sedentary middle aged men. Am. J. Physiol. 1993, 264, 896–901. [Google Scholar]
- Hougham, K.A.; Ross, R. Evidence that the association between exercise intensity and insulin sensitivity is sex dependent. Appl. Physiol. Nutr. Metab. 2011, 36, 730–735. [Google Scholar] [CrossRef]
- O’Donovan, G.; Owen, A.; Bird, S.R.; Kearney, E.M.; Nevill, A.M.; Jones, D.W.; Woolf-May, K. Changes in cardiorespiratory fitness and coronary heart disease risk factors following 24 wk of moderate or high intensity exercise of equal energy cost. J. Appl. Physiol. 2005, 98, 1619–1625. [Google Scholar] [CrossRef]
- Davies, D.S.; Burns, H.; Jewell, T.; McBride, M. Start active, stay active: A report on physical activity from the four home countries’ Chief Medical Officers. 16306; Department of Health: London, UK, 2011; pp. 1–62. [Google Scholar]
- Korkiakangas, E.; Alahuhta, M.; Laitinen, J. Barriers to regular exercise among adults at high risk or diagnosed with type 2 diabetes: A systematic review. Health Promot. Int. 2009, 24, 416–427. [Google Scholar] [CrossRef]
- Kowal, J.; Fortier, M.S. Physical activity behaviour change in middle aged and older women: The role of barriers and of environmental characteristics. J. Behav. Med. 2007, 30, 233–242. [Google Scholar] [CrossRef]
- Burgomaster, K.A.; Hughes, S.C.; Heigenhauser, G.J.; Bradwell, S.N.; Gibala, M.J. Six sessions of sprint interval training increases muscle oxidative potential and cycle endurance capacity in humans. J. Appl. Physiol. 2005, 98, 1985–1990. [Google Scholar] [CrossRef]
- Burgomaster, K.A.; Cermak, N.M.; Phillips, S.M.; Benton, C.R.; Bonen, A.; Gibala, M.J. Divergent response of metabolite transport proteins in human skeletal muscle after sprint interval training and detraining. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, 1970–1976. [Google Scholar] [CrossRef]
- Babraj, J.A.; Vollard, N.B.; Keast, C.; Guppy, F.M.; Cottrell, G.; Timmons, J.A. Extremely short duration high intensity training substantially improves insulin action in young healthy males. BMC Endocr. Disord. 2009, 9, 1–8. [Google Scholar] [CrossRef]
- Metcalfe, R.S.; Babraj, J.A.; Fawkner, S.G.; Vollaard, N.B.J. Towards the minimal amount of exercise for improving metabolic health: Beneficial effects of reduced exertion high intensity interval training. Eur. J. Appl. Physiol. 2012, 112, 2767–2775. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.C.; Johnson, T.K.; Kuzma, J.N.; Lonac, M.C.; Schweder, M.M.; Voyles, W.F.; Bell, C. Short term sprint interval training increases insulin sensitivity in healthy adults but does not affect the thermogenic response to beta-adrenergic stimulation. J. Physiol. 2010, 588, 2961–2972. [Google Scholar] [CrossRef]
- McRae, G.; Payne, A.; Zelt, J.G.E.; Scribbans, T.D.; Jung, M.E.; Little, J.P.; Gurd, B.J. Extremely low volume, whole body aerobic resistance training improves aerobic fitness and muscular endurance in females. Appl. Physiol. Nutr. Metab. 2012, 37, 1124–1131. [Google Scholar] [CrossRef]
- Freese, E.C.; Levine, A.S.; Chapman, D.P.; Hausman, D.B.; Cureton, K.J. Effects of acute sprint interval cycling and energy replacement on postprandial lipemia. J. Appl. Physiol. 2011, 111, 1584–1589. [Google Scholar] [CrossRef]
- Jakeman, J.; Adamson, S.; Babraj, J.A. Extremely short duration high-intensity training substantially improves endurance performance in triathletes. Appl. Physiol. Nutr. Metab. 2012, 37, 976–981. [Google Scholar] [CrossRef]
- LeBrasseur, N.K.; Bhasin, S.; Miciek, R.; Storer, T.W. Tests of muscle strength and physical function: reliability and discrimination of performance in younger and older men with mobility limitations. J. Am. Geriatr. Soc. 2008, 56, 2118–2128. [Google Scholar] [CrossRef]
- Elliot, D.; Denehy, L.; Berney, S.; Alison, J.A. Assessing physical function and activity for survivors of critical illness: A review of instruments. Aust. Crit. Care 2011, 24, 155–156. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed ‘up & go’: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Bohannon, R.W.; Smith, J.; Hull, D.; Palmeri, D.; Barnhard, R. Deficits in lower extremity muscle and gait performance among renal transplant candidates. Arch. Phys. Med. Rehabil. 1995, 76, 547–551. [Google Scholar] [CrossRef]
- Takeshima, N.; Rogers, M.E.; Islam, M.M.; Yamauchi, T.; Watanable, E.; Okada, A. Effect of concurrent aerobic and resistance circuit exercise training on fitness in older adults. Eur. J. Appl. Physiol. 2004, 93, 173–182. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef]
- Hopkins, W.G. Spreadsheets for analysis of controlled trials with adjustment for a subject characteristic. Sportscience 2006, 10, 46–50. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Whyte, L.; Gill, J.M.R.; Cathcart, A.J. Effect of 2 weeks of sprint interval training on health related outcomes in sedentary overweight/obese men. Metabolism 2009, 59, 1421–1428. [Google Scholar] [CrossRef]
- MacDougall, J.D.; Hicks, A.L.; MacDonald, J.R.; McKelvie, R.S.; Green, H.J.; Smith, K.M. Muscle performance and enzymatic adaptations to sprint interval training. J. Appl. Physiol. 1998, 84, 2138–2142. [Google Scholar] [CrossRef]
- Keteyian, S.J.; Brawer, C.A.; Savage, P.D.; Ehrman, J.K.; Schairer, J.; Divine, G.; Aldred, H.; Ophaug, K.; Ades, P.A. Peak aerobic capacity predicts prognosis in patients with coronary artery disease. Am. Heart J. 2008, 156, 292–300. [Google Scholar] [CrossRef]
- Buscemi, S.; Canino, B.; Batsis, J.A.; Buscemi, C.; Calandrino, V.; Mattina, A.; Arnone, M.; Caimi, G.; Cerasola, G.; Verga, S. Relationships between maximal oxygen uptake and endothelial function in healthy male adults: A preliminary study. Acta Diabetol. 2013, 50, 135–141. [Google Scholar] [CrossRef]
- Boyd, J.C.; Simpson, C.A.; Jung, M.E.; Gurd, B.J. Reducing the intensity and volume of interval training diminishes cardiovascular adaptation but not mitochondrial biogenesis in overweight/obese men. PLoS One 2013, 8, e68091. [Google Scholar]
- Matsuo, T.; Saotome, K.; Seino, S.; Shimojo, N.; Matsushita, A.; Iemitsu, M.; Ohshima, H.; Tanaka, K.; Mukai, C. Effect of a low volume aerobic type interval exercise on VO2 max and cardiac mass. Med. Sci. Sport. Exerc. 2014, 46, 42–50. [Google Scholar] [CrossRef]
- Rakobowchuk, M.; Tanguay, S.; Burgomaster, K.A.; Howarth, K.R.; Gibala, M.J.; MacDonald, M.J. Sprint interval and traditional endurance training induce similar improvements in peripheral arterial stiffness and flow mediated dilation in healthy humans. Am. J. Physiol. 2008, 295, 236–242. [Google Scholar]
- Gibala, M.J.; McGee, S.L.; Garnham, A.P.; Howlett, K.F.; Snow, R.J.; Hargreaves, M. Brief intense interval exercise activates AMPK and p38 MAPK signaling and increases expression of PGC-1∝ in human skeletal muscle. J. Appl. Physiol. 2009, 106, 929–934. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; van Essen, M.; Wilkin, G.P.; Burgomaster, K.A.; Safdar, A.; Raha, S.; Tarnopolsky, M.A. Short term sprint interval versus traditional endurance training: Similar initial adaptations in human skeletal muscle and exercise performance. J. Physiol. 2006, 575, 901–911. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Kelley, D.E.; Thaete, F.L.; He, J.; Ross, R. Skeletal muscle attenuation determined by computed tomography is associated with skeletal muscle lipid content. J. Appl. Physiol. 2000, 89, 104–110. [Google Scholar]
- Guillet, G.; Biorie, Y. Insulin resistance: A contributing factor to age-related muscle mass loss? Diabetes Metabol. 2005, 31, 5S20–5S26. [Google Scholar]
- Sevits, K.J.; Melanson, E.L.; Swibas, T.; Binns, S.E.; Klochak, A.L.; Lonac, M.C.; Peltonen, G.L.; Scalzo, R.L.; Schweder, M.M.; Smith, A.M.; et al. Total daily energy expenditure is increased following a single bout of sprint interval training. Physiol. Rep. 2013, 1, e00131. [Google Scholar]
- Baron, A.D.; Brechtel, G.; Wallace, P.; Edelman, S.V. Rates and tissue sites of non-insulin and insulin mediated glucose uptake in humans. Am. J. Physiol. 1998, 255, 769–774. [Google Scholar]
- Greiwe, J.; Hickner, R.O.; Hansen, P.A.; Racette, S.B.; Chen, M.M.; Holloszy, J.O. Effects of endurance exercise training on muscle glycogen accumulation in humans. J. Appl. Physiol. 1999, 87, 222–226. [Google Scholar]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19–39. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Adamson, S.; Lorimer, R.; Cobley, J.N.; Lloyd, R.; Babraj, J. High Intensity Training Improves Health and Physical Function in Middle Aged Adults. Biology 2014, 3, 333-344. https://doi.org/10.3390/biology3020333
Adamson S, Lorimer R, Cobley JN, Lloyd R, Babraj J. High Intensity Training Improves Health and Physical Function in Middle Aged Adults. Biology. 2014; 3(2):333-344. https://doi.org/10.3390/biology3020333
Chicago/Turabian StyleAdamson, Simon, Ross Lorimer, James N. Cobley, Ray Lloyd, and John Babraj. 2014. "High Intensity Training Improves Health and Physical Function in Middle Aged Adults" Biology 3, no. 2: 333-344. https://doi.org/10.3390/biology3020333
APA StyleAdamson, S., Lorimer, R., Cobley, J. N., Lloyd, R., & Babraj, J. (2014). High Intensity Training Improves Health and Physical Function in Middle Aged Adults. Biology, 3(2), 333-344. https://doi.org/10.3390/biology3020333