Efficacy and Safety of First-Line Everolimus Therapy Alone or in Combination with Octreotide in Gastroenteropancreatic Neuroendocrine Tumors. A Hellenic Cooperative Oncology Group (HeCOG) Study

 , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Patients and Methods
2.1. Treatment Protocol
2.2. Laboratory and Imaging Studies
2.3. Pathology
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
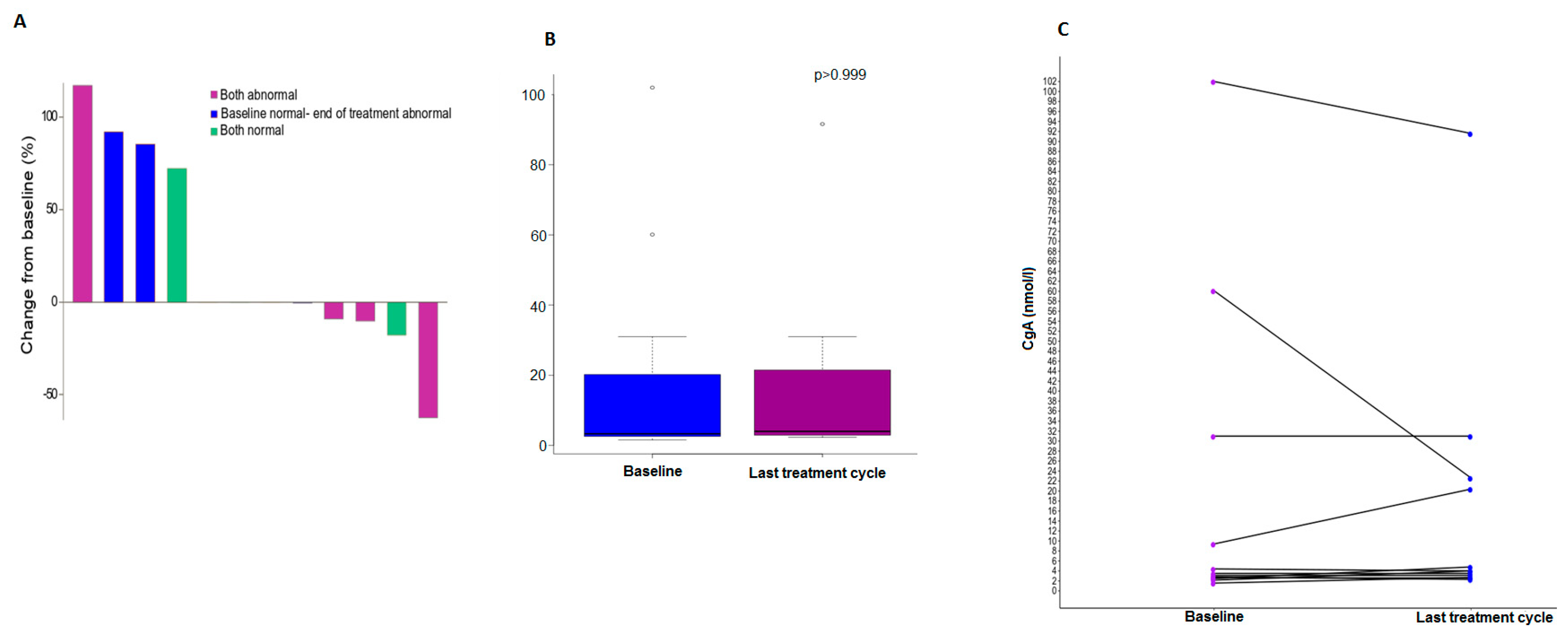
3.2. Chromogranin A Data
3.3. Treatment Cycles
3.4. Response Assessment
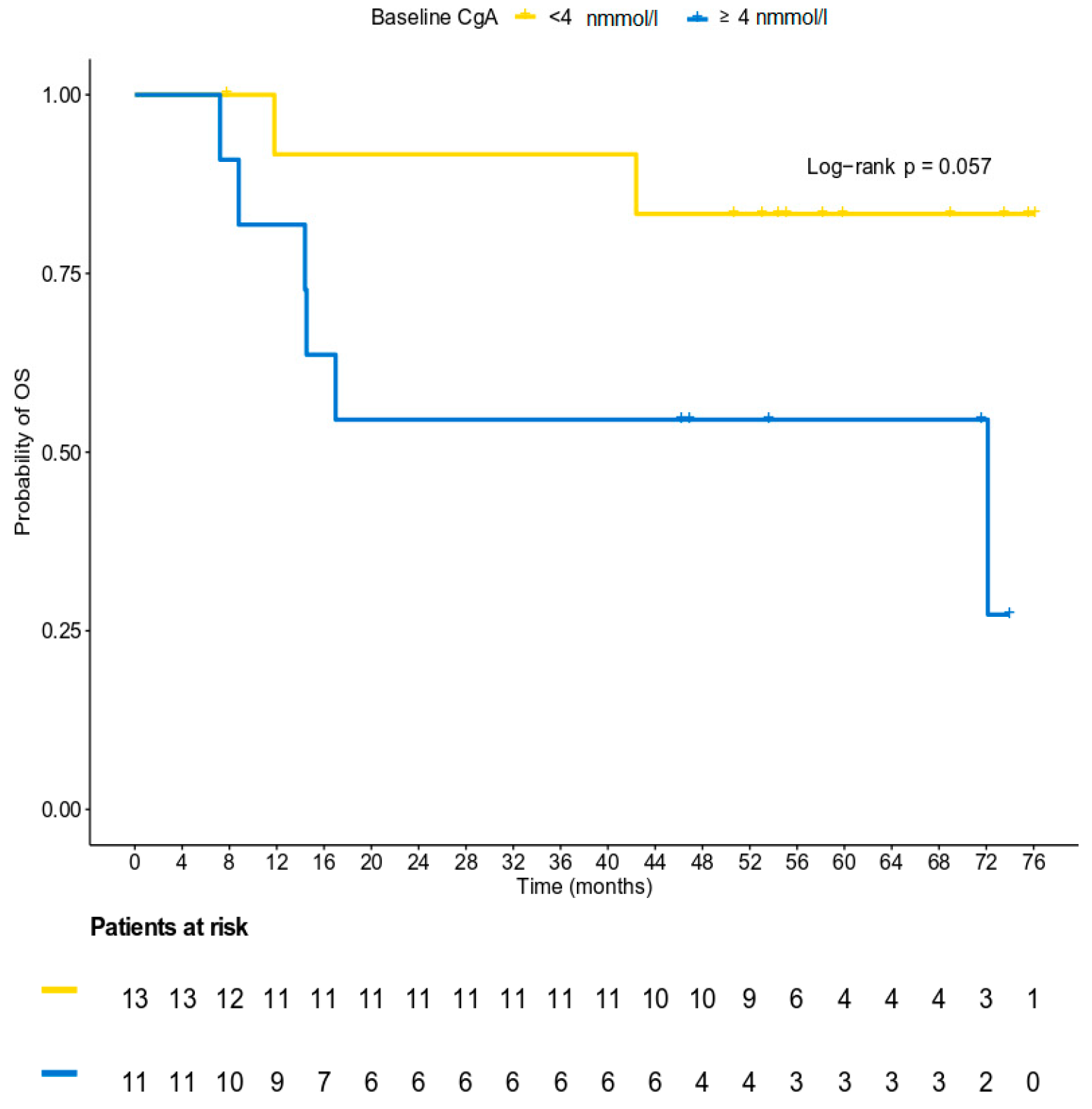
3.5. Survival Analysis
3.6. Safety Profile
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Modlin, I.M.; Oberg, K.; Chung, D.C.; Jensen, R.T.; de Herder, W.W.; Thakker, R.V.; Caplin, M.; Delle Fave, G.; Kaltsas, G.A.; Krenning, E.P.; et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008, 9, 61–72. [Google Scholar] [CrossRef]
- Chauhan, A.; Yu, Q.; Ray, N.; Farooqui, Z.; Huang, B.; Durbin, E.B.; Tucker, T.; Evers, M.; Arnold, S.; Anthony, L.B. Global burden of neuroendocrine tumors and changing incidence in Kentucky. Oncotarget 2018, 9, 19245–19254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Pavel, M.; Cwikla, J.B.; Phan, A.T.; Raderer, M.; Sedlackova, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.L.; Bang, Y.J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M.; et al. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): A randomised, placebo-controlled, phase 3 study. Lancet 2016, 387, 968–977. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.G.; et al. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Pyronnet, S.; Bousquet, C.; Najib, S.; Azar, R.; Laklai, H.; Susini, C. Antitumor effects of somatostatin. Mol. Cell Endocrinol. 2008, 286, 230–237. [Google Scholar] [CrossRef] [Green Version]
- Rinke, A.; Muller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Blaker, M.; et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Merola, E.; Panzuto, F.; Delle Fave, G. Antiproliferative effect of somatostatin analogs in advanced gastro-entero-pancreatic neuroendocrine tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 46624–46634. [Google Scholar] [CrossRef] [Green Version]
- DeBerardinis, R.J.; Lum, J.J.; Hatzivassiliou, G.; Thompson, C.B. The biology of cancer: Metabolic reprogramming fuels cell growth and proliferation. Cell Metab. 2008, 7, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavel, M.E.; Hainsworth, J.D.; Baudin, E.; Peeters, M.; Horsch, D.; Winkler, R.E.; Klimovsky, J.; Lebwohl, D.; Jehl, V.; Wolin, E.M.; et al. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): A randomised, placebo-controlled, phase 3 study. Lancet 2011, 378, 2005–2012. [Google Scholar] [CrossRef]
- Bousquet, C.; Lasfargues, C.; Chalabi, M.; Billah, S.M.; Susini, C.; Vezzosi, D.; Caron, P.; Pyronnet, S. Clinical review: Current scientific rationale for the use of somatostatin analogs and mTOR inhibitors in neuroendocrine tumor therapy. J. Clin. Endocrinol. Metab. 2012, 97, 727–737. [Google Scholar] [CrossRef]
- Yao, J.C.; Phan, A.T.; Chang, D.Z.; Wolff, R.A.; Hess, K.; Gupta, S.; Jacobs, C.; Mares, J.E.; Landgraf, A.N.; Rashid, A.; et al. Efficacy of RAD001 (everolimus) and octreotide LAR in advanced low- to intermediate-grade neuroendocrine tumors: Results of a phase II study. J. Clin. Oncol. 2008, 26, 4311–4318. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Lombard-Bohas, C.; Baudin, E.; Kvols, L.K.; Rougier, P.; Ruszniewski, P.; Hoosen, S.; St Peter, J.; Haas, T.; Lebwohl, D.; et al. Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: A phase II trial. J. Clin. Oncol. 2010, 28, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.H.; Litiere, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloppel, G.; La Rosa, S. Ki67 labeling index: Assessment and prognostic role in gastroenteropancreatic neuroendocrine neoplasms. Virchows Arch. 2018, 472, 341–349. [Google Scholar] [CrossRef]
- Fleming, T.R. One-sample multiple testing procedure for phase II clinical trials. Biometrics 1982, 38, 143–151. [Google Scholar] [CrossRef]
- Pavel, M.E.; Baudin, E.; Oberg, K.E.; Hainsworth, J.D.; Voi, M.; Rouyrre, N.; Peeters, M.; Gross, D.J.; Yao, J.C. Efficacy of everolimus plus octreotide LAR in patients with advanced neuroendocrine tumor and carcinoid syndrome: Final overall survival from the randomized, placebo-controlled phase 3 RADIANT-2 study. Ann. Oncol. 2017, 28, 1569–1575. [Google Scholar] [CrossRef]
- Anthony, L.B.; Pavel, M.E.; Hainsworth, J.D.; Kvols, L.K.; Segal, S.; Horsch, D.; Van Cutsem, E.; Oberg, K.; Yao, J.C. Impact of Previous Somatostatin Analogue Use on the Activity of Everolimus in Patients with Advanced Neuroendocrine Tumors: Analysis from the Phase III RADIANT-2 Trial. Neuroendocrinology 2015, 102, 18–25. [Google Scholar] [CrossRef]
- Capdevila, J.; Sevilla, I.; Alonso, V.; Anton Aparicio, L.; Jimenez Fonseca, P.; Grande, E.; Reina, J.J.; Manzano, J.L.; Alonso Lajara, J.D.; Barriuso, J.; et al. Evaluation of the efficacy and safety of lanreotide in combination with targeted therapies in patients with neuroendocrine tumours in clinical practice: A retrospective cross-sectional analysis. BMC Cancer 2015, 15, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajetta, E.; Catena, L.; Fazio, N.; Pusceddu, S.; Biondani, P.; Blanco, G.; Ricci, S.; Aieta, M.; Pucci, F.; Valente, M.; et al. Everolimus in combination with octreotide long-acting repeatable in a first-line setting for patients with neuroendocrine tumors: An ITMO group study. Cancer 2014, 120, 2457–2463. [Google Scholar] [CrossRef] [PubMed]
- Bajetta, E.; Catena, L.; Pusceddu, S.; Spada, F.; Iannacone, C.; Sarno, I.; Di Menna, G.; Dottorini, L.; Marte, A.M. Everolimus in Combination with Octreotide Long-Acting Repeatable in a First-Line Setting for Patients with Neuroendocrine Tumors: A 5-Year Update. Neuroendocrinology 2018, 106, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Kulke, M.H.; Ruszniewski, P.; Van Cutsem, E.; Lombard-Bohas, C.; Valle, J.W.; De Herder, W.W.; Pavel, M.; Degtyarev, E.; Brase, J.C.; Bubuteishvili-Pacaud, L.; et al. A randomized, open-label, phase 2 study of everolimus in combination with pasireotide LAR or everolimus alone in advanced, well-differentiated, progressive pancreatic neuroendocrine tumors: COOPERATE-2 trial. Ann. Oncol. 2017, 28, 1309–1315. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total |
|---|---|
| (N = 25) | |
| Median (min,max) | |
| Age (in years) ^ | 56.9 (37.6,79.9) |
| Tumor size (in mm) * | 35.0 (15.0,100.0) |
| Ki67 (% of positive nuclei per 2000 cells, central assessment) * | 0.0 (0.0–20.0) |
| N (%) | |
| Sex | |
| Man | 10 (40.0) |
| Woman | 15 (60.0) |
| PS | |
| 0 | 19 (76.0) |
| 1 | 6 (24.0) |
| Sporadic | |
| No | 4 (16.0) |
| Yes | 21 (84.0) |
| MEN testing | |
| No | 24 (96.0) |
| Yes | 1 (4.0) |
| Initial surgery | |
| No | 12 (48.0) |
| Yes | 13 (52.0) |
| Type of surgery | |
| Laparotomy | 1 (7.7) |
| Open surgery | 12 (92.3) |
| Type of open surgery | |
| Total resection | 4 (33.3) |
| Subtotal resection | 5 (41.7) |
| Other ** | 3 (25.0) |
| Tumor localization | |
| Jejunum | 2 (8.0) |
| Ileus | 4 (16.0) |
| Colon | 2 (8.0) |
| Pancreas | 10 (40.0) |
| Unknown primary | 2 (8.0) |
| Other *** | 5 (20.0) |
| Tumor grade | |
| G1 [Low grade] | 11 (44.0) |
| G2 [Intermediate grade] | 14 (56.0) |
| Ki67 (local assessment) | |
| <3% | 11(44.0) |
| 3–20% | 14 (56.0) |
| Ki67 (central assessment) * | |
| <3% | 10 (58.8) |
| 3–20% | 7 (41.2) |
| Locally advanced ^ | |
| No | 21 (84.0) |
| Yes | 4 (16.0) |
| Number of metastatic sites ^ | |
| 0 | 4 (16.0) |
| 1 | 17 (68.0) |
| 2 | 4 (16.0) |
| Site of metastases ^ | |
| Lung | 0 (0.0) |
| Liver | 19 (76.0) |
| Bones | 0 (0.0) |
| LNS | 5 (20.0) |
| Other **** | 1 (4.0) |
| CgA | Time point | ||
|---|---|---|---|
| Baseline | Last Cycle | p-Value | |
| N | 24 | 12 | >0.999 ^ |
| mean (std) | 21.22 (30.36) | 16.05 (25.73) | |
| median | 3.50 | 4 | |
| min-max | 1.57–102.0 | 2.30–91.60 | |
| p25–p75 | 2.55–27.60 | 2.90-21.50 | |
| Normal (N,%) | 13 (54.2) | 5 (41.7) | 0.16 ^^ |
| Abnormal (N,%) | 11 (45.8) | 7 (58.3) | |
| Adverse Event | Grade 1 | Grade 2 | ||||
|---|---|---|---|---|---|---|
| System Organ Class | N of evts | N of pts | % pts | N of evts | N of pts | % pts |
| Preferred Term | ||||||
| Anemia | 5 | 5 | 20.00 | 3 | 3 | 12.00 |
| Diarrhea | 2 | 2 | 8.00 | 6 | 6 | 24.00 |
| Edema limbs | 4 | 4 | 16.00 | 1 | 1 | 4.00 |
| Fatigue | 4 | 4 | 16.00 | 2 | 2 | 8.00 |
| Fever | 4 | 4 | 16.00 | 1 | 1 | 4.00 |
| Alanine aminotransferase increased | 6 | 6 | 24.00 | 4 | 4 | 16.00 |
| Alkaline phosphatase increased | 7 | 7 | 28.00 | 0 | 0 | 0.00 |
| Aspartate aminotransferase increased | 6 | 6 | 24.00 | 4 | 4 | 16.00 |
| Cholesterol high | 6 | 6 | 24.00 | 2 | 2 | 8.00 |
| Creatinine increased | 3 | 3 | 12.00 | 1 | 1 | 4.00 |
| GGT increased | 2 | 2 | 8.00 | 5 | 5 | 20.00 |
| White blood cell decreased | 4 | 4 | 16.00 | 1 | 1 | 4.00 |
| Hyperglycemia | 8 | 8 | 32.00 | 8 | 8 | 32.00 |
| Hypertriglyceridemia | 5 | 5 | 20.00 | 1 | 1 | 4.00 |
| Hypocalcemia | 4 | 4 | 16.00 | 1 | 1 | 4.00 |
| Hypokalemia | 3 | 3 | 12.00 | 1 | 1 | 4.00 |
| Hypophosphatemia | 2 | 2 | 8.00 | 3 | 3 | 12.00 |
| Rash maculo-papular | 4 | 4 | 16.00 | 2 | 2 | 8.00 |
| Adverse Event | Grade 3 | Grade 4 | ||||
|---|---|---|---|---|---|---|
| System Organ Class | N of evts | N of pts | % pts | N of evts | N of pts | % pts |
| Preferred Term | ||||||
| Total | 16 | 11 | 44.00 | 2 | 2 | 8.00 |
| Blood and lymphatic system disorders | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Anemia | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Gastrointestinal disorders | 5 | 5 | 20.00 | 0 | 0 | 0.00 |
| Diarrhea | 2 | 2 | 8.00 | 0 | 0 | 0.00 |
| Mucositis oral | 3 | 3 | 12.00 | 0 | 0 | 0.00 |
| Infections and infestations | 2 | 2 | 8.00 | 0 | 0 | 0.00 |
| Infections and infestations - Other, specify * | 2 | 2 | 8.00 | 0 | 0 | 0.00 |
| Investigations | 4 | 4 | 16.00 | 2 | 2 | 8.00 |
| Alanine aminotransferase increased | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| CPK increased | 1 | 1 | 4.00 | 1 | 1 | 4.00 |
| GGT increased | 1 | 1 | 4.00 | 1 | 1 | 4.00 |
| Neutrophil count decreased | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Metabolism and nutrition disorders | 3 | 3 | 12.00 | 0 | 0 | 0.00 |
| Anorexia | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Hyperglycemia | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Hypokalemia | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Vascular disorders | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
| Hypertension | 1 | 1 | 4.00 | 0 | 0 | 0.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koumarianou, A.; Pectasides, D.; Koliou, G.-A.; Dionysopoulos, D.; Kolomodi, D.; Poulios, C.; Skondra, M.; Sgouros, J.; Pentheroudakis, G.; Kaltsas, G.; et al. Efficacy and Safety of First-Line Everolimus Therapy Alone or in Combination with Octreotide in Gastroenteropancreatic Neuroendocrine Tumors. A Hellenic Cooperative Oncology Group (HeCOG) Study. Biology 2020, 9, 51. https://doi.org/10.3390/biology9030051
Koumarianou A, Pectasides D, Koliou G-A, Dionysopoulos D, Kolomodi D, Poulios C, Skondra M, Sgouros J, Pentheroudakis G, Kaltsas G, et al. Efficacy and Safety of First-Line Everolimus Therapy Alone or in Combination with Octreotide in Gastroenteropancreatic Neuroendocrine Tumors. A Hellenic Cooperative Oncology Group (HeCOG) Study. Biology. 2020; 9(3):51. https://doi.org/10.3390/biology9030051
Chicago/Turabian StyleKoumarianou, Anna, Dimitrios Pectasides, Georgia-Angeliki Koliou, Dimitrios Dionysopoulos, Dionysia Kolomodi, Christos Poulios, Maria Skondra, Joseph Sgouros, George Pentheroudakis, Gregory Kaltsas, and et al. 2020. "Efficacy and Safety of First-Line Everolimus Therapy Alone or in Combination with Octreotide in Gastroenteropancreatic Neuroendocrine Tumors. A Hellenic Cooperative Oncology Group (HeCOG) Study" Biology 9, no. 3: 51. https://doi.org/10.3390/biology9030051
APA StyleKoumarianou, A., Pectasides, D., Koliou, G.-A., Dionysopoulos, D., Kolomodi, D., Poulios, C., Skondra, M., Sgouros, J., Pentheroudakis, G., Kaltsas, G., & Fountzilas, G. (2020). Efficacy and Safety of First-Line Everolimus Therapy Alone or in Combination with Octreotide in Gastroenteropancreatic Neuroendocrine Tumors. A Hellenic Cooperative Oncology Group (HeCOG) Study. Biology, 9(3), 51. https://doi.org/10.3390/biology9030051