

Development and Validation of an Instrument to Appraise the Tolerability, Safety of Use, and Pleasantness of a Cosmetic Product

 , , ,
, , ,
Abstract
1. Introduction
2. Methods and Materials
2.1. Study Design
2.2. Recruitment of Participants
2.2.1. Scientific Committee
2.2.2. Expert Panel
- Understand safety requirements: Before the cosmetic product is introduced onto the market, it must undergo evaluation
- Encourage and assist patients, customers, and healthcare professionals in reporting adverse reactions
- Contribute to transparency and communication initiatives by disseminating information that was reliable and consistent from a scientific perspective to encourage the safe and efficient use of cosmetics
- Encourage and facilitate reporting of adverse reactions and coordinating initiatives to improve and expand current reporting options
- Where the participants were dermatologists, they were required to possess knowledge about all available dermatological techniques, the ability to diagnose conditions, assess skin health, teach patients preventative skin care, and keep track of how well skin treatments were working.
2.3. Sampling and Sample Size
2.4. Development of the Data Collection Instrument (Delphi Questionnaire)
2.5. Delphi Questionnaire Round
- An overview of the study’s goals.
- Methodology.
- Candidate categories and selection criteria.
- How many questions must be answered, and how long the exercise should take.
- Timing of the process.
- Potential applications for the data gathered.
- Advantages of participating.
2.6. Data Collection
2.7. Statistical Analysis
2.8. Ethics Approval and Consent to Participate
3. Results
3.1. Development of the Data Collection Instrument (Delphi Questionnaire)
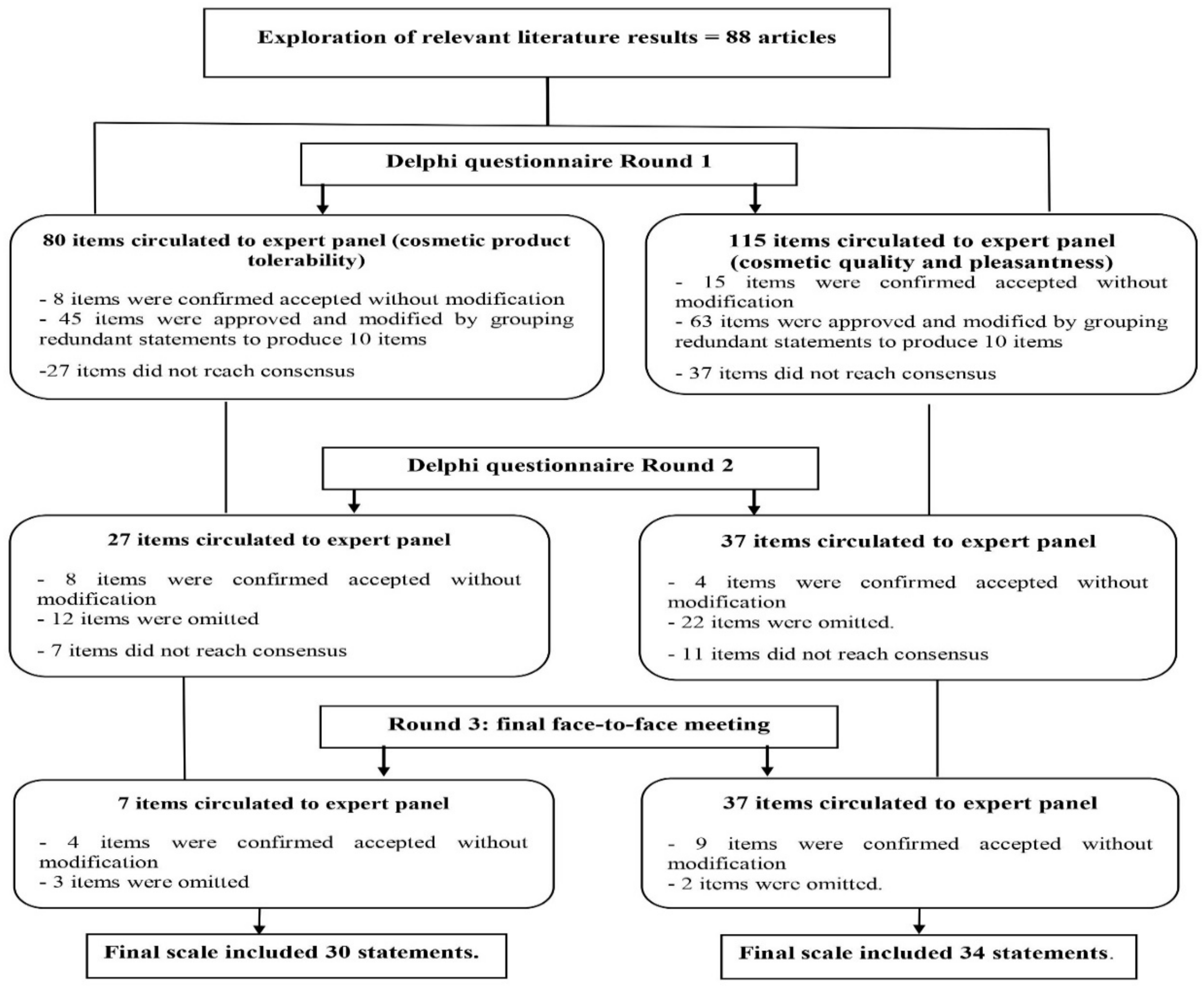
3.2. Delphi Questionnaire Round
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elias, P.M. Stratum corneum defensive functions: An integrated view. J. Investig. Dermatol. 2005, 125, 183–200. [Google Scholar] [CrossRef]
- Haftek, M.; Roy, D.C.; Liao, I.-C. Evolution of skin barrier science for healthy and compromised skin. J. Drugs. Dermatol. 2021, 20, s3–s9. [Google Scholar] [CrossRef] [PubMed]
- Roure, R.; Lanctin, M.; Nollent, V.; Bertin, C. Methods to assess the protective efficacy of emollients against climatic and chemical aggressors. Dermatol. Res. Pract. 2012, 2012, 864734. [Google Scholar] [CrossRef]
- Kim, Y.; Lim, K.M. Skin barrier dysfunction and filaggrin. Arch. Pharm. Res. 2021, 44, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Chandan, N.; Rajkumar, J.R.; Shi, V.Y.; Lio, P.A. A new era of moisturizers. J. Cosmet. Dermatol. 2021, 20, 2425–2430. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, B.E.; Leung, D.Y.M. Pathophysiology of atopic dermatitis: Clinical implications. Allergy Asthma Proc. 2019, 40, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Harrison, I.P.; Spada, F. Breaking the itch-scratch cycle: Topical options for the management of chronic cutaneous itch in atopic dermatitis. Medicines 2019, 6, 76. [Google Scholar] [CrossRef]
- Kahremany, S.; Hofmann, L.; Harari, M.; Gruzman, A.; Cohen, G. Pruritus in psoriasis and atopic dermatitis: Current treatments and new perspectives. Pharmacol. Rep. 2021, 73, 443–453. [Google Scholar] [CrossRef]
- Morris-Jones, R.; Robertson, S.J.; Ross, J.S. Dermatitis caused by physical irritants. Br. J. Dermatol. 2002, 147, 270–275. [Google Scholar] [CrossRef]
- Cork, M.J. The role of Staphylococcus aureus in atopic eczema: Treatment strategies. J. Eur. Acad. Dermatol. Venereol. 1996, 7, 31–37. [Google Scholar] [CrossRef]
- Greive, K. Cleansers and moisturisers: The basics. Wound. Pract. Res. 2015, 23, 76–81. [Google Scholar]
- Wang, Z.; Man, M.-Q.; Li, T.; Elias, P.M.; Mauro, T.M. Aging-associated alterations in epidermal function and their clinical significance. Aging 2020, 12, 5551–5565. [Google Scholar] [CrossRef] [PubMed]
- Willis, C.M.; Shaw, S.; De Lacharriere, O.; Baverel, M.; Reiche, L.; Jourdain, R.; Bastien, P.; Wilkinson, J.D. Sensitive skin: An epidemiological study. Br. J. Dermatol. 2001, 145, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Lumelsky, V.J.; Shur, M.S.; Wagner, S. Sensitive skin. IEEE Sensors J. 2001, 1, 41–51. [Google Scholar] [CrossRef]
- Kwa, M.; Welty, L.J.; Xu, S. Adverse Events Reported to the US Food and Drug Administration for Cosmetics and Personal Care Products. JAMA Int. Med. 2017, 177, 1202–1204. [Google Scholar] [CrossRef]
- Alani, J.I.; Davis, M.D.P.; Yiannias, J.A. Allergy to cosmetics: A literature review. Dermatitis 2013, 24, 283–290. [Google Scholar] [CrossRef]
- Draelos, Z.D. Cosmetics: The Medicine of Beauty. J. Cosmet. Derm. 2015, 14, 91. [Google Scholar] [CrossRef]
- Husain, K. A survey on usage of personal care products especially cosmetics among university students in Saudi Arabia. J Cosmet Dermatol. 2019, 18, 271–277. [Google Scholar] [CrossRef]
- Orton, D.I.; Wilkinson, J.D. Cosmetic Allergy. Am. J. Clin. Dermatol. 2004, 5, 327–337. [Google Scholar] [CrossRef]
- Regulation (EC) No 1223/2009 of the European Parliament and of the Council of 30 November 2009 on Cosmetic Products. Available online: https://eur-lex.europa.eu/legalcontent/EN/TXT/?uri=celex%3A32009R1223 (accessed on 28 May 2021).
- Health and Safety Department, Dubai Municipality. Apply for Consumer Products Registration (MONTAJI). Available online: https://hub.dm.gov.ae/link/servicedetails?servicecode=3560 (accessed on 21 May 2021).
- UAE. Scheme for Cosmetic and Personal Care, & Emirates Authority for Standardization and Metrology. UAE Scheme for Cosmetic and Personal Care. Available online: http://dubai-ecs.com/en/wp-content/uploads/2017/03/CPC-Regulations-UAE.pdf (accessed on 15 June 2021).
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; Zyoud, S.e.H.; Ashames, A. Hidden formaldehyde content in cosmeceuticals containing preservatives that release formaldehyde and their compliance behaviors: Bridging the gap between compliance and local regulation. Cosmetics 2020, 7, 93. [Google Scholar] [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; Zyoud, S.H. An investigation into incidences of microbial contamination in cosmeceuticals in the UAE: Imbalances between preservation and microbial contamination. Cosmetics 2020, 7, 92. [Google Scholar] [CrossRef]
- Dubai Municipality Withdraws 6 Sterilizers for Hands that Do Not Meet Specifications from the Local Market. Localities—Health—Emirates Today. Available online: https://www.emaratalyoum.com/local-section/health/2020-04-01-1.1328166a.(1) (accessed on 12 April 2020).
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; El-Dahiyat, F.; Jamshed, S. Scale validation for the identification of falsified hand sanitizer: Public and regulatory authorities perspectives from United Arab Emirates. BMC Public Health 2020, 20, 1595. [Google Scholar] [CrossRef] [PubMed]
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M. The pandemic of COVID-19 and its implications for the purity and authenticity of alcohol-based hand sanitizers: The health risks associated with falsified sanitizers and recommendations for regulatory and public health bodies. Res. Soc. Adm. Pharm. 2021, 17, 2050–2051. [Google Scholar] [CrossRef] [PubMed]
- Ajman Economy Seized and Confiscated Adulterated Sterilizers. Available online: http://www.alkhaleej.ae/alkhaleej/page/8ab6eebb-42ac-4a05-a8dd-378a41896b57 (accessed on 5 May 2020).
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; Zyoud, S.H. Analysis and Quantification of Alkyl (C12-22) Trimethyl Ammonium Chloride Content in Cosmetics: Regulatory Compliance Gap Analysis. Cosmetics 2021, 8, 103. [Google Scholar] [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; Jairoun, O.; Zyoud, S.H. Analysis of Fluoride Concentration in Toothpastes in the United Arab Emirates: Closing the Gap between Local Regulation and Practice. Cosmetics 2021, 8, 113. [Google Scholar] [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; Ibrahim, B.; Hassali, M.A.; Zyoud, S.H. Risk Assessment of Over-the-Counter Cannabinoid-Based Cosmetics: Legal and Regulatory Issues Governing the Safety of Cannabinoid-Based Cosmetics in the UAE. Cosmetics 2021, 8, 57. [Google Scholar] [CrossRef]
- Berardesca, E.; Farage, M.; Maibach, H. Sensitive skin: An overview. Int. J. Cosmet. Sci. 2013, 35, 2–8. [Google Scholar] [CrossRef]
- Coverly, J.; Peters, L.; Whittle, E.; Basketter, D.A. Susceptibility to skin stinging, non-immunologic contact urticaria and acute skin irritation; is there a relationship? Contact Dermat. 1998, 38, 90–95. [Google Scholar] [CrossRef]
- Pons-Guiraud, A. Sensitive skin: A complex and multifactorial syndrome. J. Cosmet. Dermatol. 2004, 3, 145–148. [Google Scholar] [CrossRef]
- Farage, M.A.; Katsarou, A.; Maibach, H.I. Sensory, clinical and physiological factors in sensitive skin. Contact Dermat. 2006, 55, 1–14. [Google Scholar] [CrossRef]
- de Groot, A.C.; White, I.R.; Flyvholm, M.A.; Lensen, G.; Coenraads, P.J. Formaldehyde-releasers in cosmetics: Relationship to formaldehyde contact allergy. Part 1. Characterization, frequency and relevance of sensitization, and frequency of use in cosmetics. Contact Dermat. 2010, 62, 2–17. [Google Scholar] [CrossRef]
- Lundov, M.D.; Johansen, J.D.; Carlsen, B.C.; Engkilde, K.; Menné, T.; Thyssen, J.P. Formaldehyde exposure and patterns of concomitant contact allergy to formaldehyde and formaldehyde-releasers. Contact Dermat. 2010, 63, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Misery, L.; Boussetta, S.; Nocera, T.; Perez-Cullell, N.; Taieb, C. Sensitive skin in Europe. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Meshkat, B.; Cowman, S.; Gethin, G.; Ryan, K.; Wiley, M.; Brick, A.; Clarke, E.; Mulligan, E. Using an e-Delphi technique in achieving consensus across disciplines for developing best practice in day surgery in Ireland. J. Hosp. Adm. 2014, 3, 1–8. [Google Scholar] [CrossRef]
- Dalkey, N.; Helmer, O. An experimental application of the Delphi method to the use of experts. Manag Sci. 1963, 9, 458–467. [Google Scholar] [CrossRef]
- Dalkey, N.C. The Delphi Method: An Experimental Study of Group Opinion; Rand Corp.: Santa Monica, CA, USA, 1969; Available online: https://www.rand.org/pubs/research_memoranda/RM5888.html (accessed on 14 June 2021).
- Butterwick, D.J.; Paskevich, D.M.; Lagumen, N.G.; Vallevand, A.L.C.; Lafave, M.R. Development of a content-valid technical skill assessment instrument for athletic taping skills. JAH 2007, 35, 147–155. [Google Scholar]
- Lafave, M.; Katz, L.; Butterwick, D. Development of a content-valid standardized orthopedic assessment tool (SOAT). Adv. Health Sci. Educ. Theory Pract. 2008, 13, 397–406. [Google Scholar] [CrossRef]
- Lafave, M.R.; Butterwick, D.J.; Murray, R.P.; Freeman, T.; Lau, B.H. Content validity of the Rodeo-SCAT. Int. J. Sports Med. 2013, 34, 170–175. [Google Scholar] [CrossRef]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef]
- Gustafson, D.H.; Shukla, R.K.; Delbecq, A.; Walster, G.W. A comparative study of differences in subjective likelihood estimates made by individuals, interacting groups, delphi groups, and nominal groups. Organ Behav. Hum. Perf. 1973, 9, 280–291. [Google Scholar] [CrossRef]
- Graefe, A.; Armstrong, J.S. Comparing face-to-face meetings, nominal groups, delphi and prediction markets on an estimation task. Int. J. Forecasting 2016, 27, 183–195. [Google Scholar] [CrossRef]
- El Metodo Delphi: Landeta, Jon: Libros. Available online: https://www.amazon.es/El-metodo-delphi-Jon-Landeta/dp/8434428369 (accessed on 12 February 2022).
- Jones, J.; Hunter, D. Consensus methods for medical and healthservices research. Br. Med. J. 1995, 311, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.M.; Cantrill, J.A. Consensus methods in prescribing research. J. Clin. Pharm. Ther. 2001, 26, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Rowe, G.; Wright, G. The Delphi technique as a forecasting tool: Issues and analysis. Int. J. 1999, 15, 353–375. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Getachew, M.; Tewelde, T. Cosmetic Use and Its Adverse Events among Female Employees of Jimma University, Southwest Ethiopia. Ethiop. J. Health Sci. 2018, 28, 717–724. [Google Scholar] [CrossRef]
- Huf, G.; Rito, P.d.N.; Presgrave, R.d.F.; Boas, M.H.S.V. Adverse reactions to cosmetic products and the Notification System in Health Surveillance: A survey. Braz. J. Epidemiol. 2013, 16, 1017–1020. [Google Scholar] [CrossRef]
- Bilal, A.I.; Tilahun, Z.; Osman, E.D.; Mulugeta, A.; Shekabdulahi, M.; Berhe, D.F. Cosmetics use-related adverse events and determinants among Jigjiga town residents, Eastern Ethiopia. Dermatol. Ther. 2017, 7, 143–153. [Google Scholar] [CrossRef]
- Di Giovanni, C.; Arcoraci, V.; Gambardella, L.; Sautebin, L. Cosmetovigilance survey: Are cosmetics considered safe by consumers? Pharmacol. Res. 2006, 53, 16–21. [Google Scholar] [CrossRef]
- Korichi, R.; Pelle-De-Queral, D.; Gazano, G.; Aubert, A. Why women use makeup: Implication of psychological traits in makeup functions. J. Cosmet. Sci. 2008, 59, 127–137. [Google Scholar] [PubMed]
- FDA. “Hypoallergenic” Cosmetics. 2020. Available online: https://www.fda.gov/cosmetics/cosmetics-labeling-claims/hypoallergeniccosmetics#Hypoallergenic_Cosmetics (accessed on 5 June 2022).
- Hamann, C.R.; Bernard, S.; Hamann, D.; Hansen, R.; Thyssen, J.P. Is there a risk using hypoallergenic cosmetic pediatric products in the United States? J. Allergy Clin. Immunol. 2015, 135, 1070–1071. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, R.; Hafner, M.d.F.S.; Rangel, M.G. Evaluation of the presence of allergens in children’s products available for sale in a big city. An. Bras Dermatol. 2018, 93, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Ashique, K.T.; Chandrasekhar, D. Role of clinical pharmacist in cosmetovigilance of misuse and abuse of topical corticosteroids. Indian J. Dermatol. 2017, 62, 213–214. [Google Scholar] [CrossRef] [PubMed]
- Allison, D.G.; Higginson, P.; Martin, S. Antibiotic resistance awareness: A public engagement approach for all pharmacists. Int. J. Pharm. Pr. 2017, 25, 93–96. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Panelists’ Characteristics | Groups | Frequency | Percentage |
|---|---|---|---|
| Educational level | Bachelor’s degree or equivalent | 25 | 50% |
| Master’s degree or equivalent | 18 | 36% | |
| Ph.D. | 7 | 14% | |
| Type of Organization | Private | 20 | 40% |
| Public (government) | 20 | 40% | |
| Both | 10 | 20% | |
| Work experience | <1 year | 6 | 12% |
| 1 to 5 years | 21 | 42% | |
| 6 to10 years | 8 | 16% | |
| 11 to 15 years | 7 | 14% | |
| ≥16 years | 8 | 16% | |
| Position | Pharmacovigilance officer | 15 | 30% |
| Dermatologist | 20 | 40% | |
| Cosmetic Safety Assessor | 15 | 30% | |
| Region/country | EU | 17 | 34% |
| USA | 12 | 24% | |
| GCC | 11 | 22% | |
| Canada | 10 | 20% |
| Main End Points Evaluation of Good Skin Compatibility of the Cosmetic Product (Cutaneous Tolerance) | ||
|---|---|---|
| Erythema: Evaluation | Score | Agreement Rate n (%) |
| No Erythema | 0 | 41 (82%) |
| Very slightly Erythema (hardly visible) in at least ¾ of the application area | 1 | 44 (88%) |
| Clearly visible Erythema, uniformly allocated on at least ¾ of the application area | 2 | 43 (86%) |
| Important Erythema (dark red) | 3 | 50 (100%) |
| Purpuric Erythema | 4 | 48 (96%) |
| Edema: Evaluation | ||
| No Edema | 0 | 47 (94%) |
| Very slightly Edema and palpable on at least ¾ of the application area, or smaller edema on a smaller surface | 1 | 44 (88%) |
| Slight Edema (Edges well defined) on at least ¾ of the application area. | 2 | 45 (90%) |
| Severe Edema (1 mm thick at less) on the surface greater than the application area | 3 | 48 (96%) |
| Severe Edema (1 mm thick at least) on the surface greater than the application area | 4 | 49 (98) |
| Papule/vesicles/bullae/pustules: Evaluation | ||
| No Papule, vesicles, bullae, or pustules | 0 | 50 (100%) |
| Papules or very small vesicles (less than about 1 mm in diameter) | 1 | 50 (100%) |
| Vesicles of 1 to 2 mm in diameter | 2 | 50 (100%) |
| Pustules | 3 | 47 (94%) |
| Bullae with clear liquid | 4 | 42 (84%) |
| Dryness/Desquamation: Evaluation | ||
| No Dryness and Desquamation | 0 | 44 (88%) |
| Slight Dryness = mat, unpolished aspect, on at least ¾ of the application area or pulverulent (whitish) aspect on a surface smaller than ¾ of the application area | 1 | 46 (88%) |
| Clear dryness = pulverulent aspect on at least ¾ of the application area or desquamatory aspect on a surface smaller than ¾ of the application area | 2 | 46 (92%) |
| Moderate desquamation = desquamatory aspect on at least ¾ of the application area, or presence of thick squamae on a surface smaller than ¾ of the application area | 3 | 48 (96%) |
| Severe desquamation = presence of thick squamae or at least ¾ of the application area, with possibility of tegument fissuration | 4 | 49 (98%) |
| Detergent effect: Evaluation | ||
| No rugosity | 0 | 49 (98%) |
| Slight rugosity = slightly worn aspect on at least ¾ of the application area or clearly worn aspect on a surface smaller than ¾ of the application area | 1 | 50 (100%) |
| Clear rugosity = clearly worn aspect on at least ¾ of the application area or very worn aspect (presence of wrinkles with well-pronounced crests) | 2 | 50 (100%) |
| Moderate rugosity = very worn aspect on at least ¾ of the application area or presence of deep wrinkles on a surface smaller than ¾ of the application area | 3 | 46 (92%) |
| Severe rugosity = presence of deep wrinkles on at least ¾ of the application area | 4 | 42 (84%) |
| Reflectivity: Evaluation | ||
| No Reflectivity | 0 | 46 (92%) |
| Slight Reflectivity = slightly shiny aspect on at least ¾ of the application area or clearly shiny aspect on a surface smaller than ¾ of the application area | 1 | 47 (94%) |
| Clear Reflectivity = shiny aspect on at least ¾ of the application area or varnished aspect on a surface smaller than ¾ of the application area | 2 | 49 (98%) |
| Moderate Reflectivity = glossy aspect on at least ¾ of the application area or glazed aspect on a surface smaller than ¾ of the application area | 3 | 48 (96%) |
| Severe Reflectivity = glazed aspect, deeply shimmering, on at least ¾ of the application area | 4 | 45 (90%) |
| Cosmetic Product’ Efficacy | Agreement Rate n (%) |
|---|---|
| 44 (88%) |
| 45 (96%) |
| 48 (96%) |
| 49 (98%) |
| 49 (98%) |
| 50 (100%) |
| 50 (100%) |
| 50 (100%) |
| 49 (98%) |
| 40 (40%) |
| 44 (88%) |
| 43 (86%) |
| 43 (68%) |
| 42 (84%) |
| 45 (90%) |
| 46 (92%) |
| 50 (100%) |
| 46 (92%) |
| 44 (88%) |
| 41 (82%) |
| 43 (86%) |
| 47 (94%) |
| 48 (96%) |
| 49 (98%) |
| 45 (90%) |
| 44 (88%) |
| 41 (82%) |
| Cosmetic product’ quality | |
| 41 (82%) |
| 43 (86%) |
| 45 (90%) |
| 49 (98%) |
| 43 (86%) |
| 45 (90%) |
| 45 (90%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jairoun, A.A.; Al-Hemyari, S.S.; Shahwan, M.; El-Dahiyat, F.; Zyoud, S.H.; Jairoun, O.; Shayeb, M.A. Development and Validation of an Instrument to Appraise the Tolerability, Safety of Use, and Pleasantness of a Cosmetic Product. Cosmetics 2023, 10, 15. https://doi.org/10.3390/cosmetics10010015
Jairoun AA, Al-Hemyari SS, Shahwan M, El-Dahiyat F, Zyoud SH, Jairoun O, Shayeb MA. Development and Validation of an Instrument to Appraise the Tolerability, Safety of Use, and Pleasantness of a Cosmetic Product. Cosmetics. 2023; 10(1):15. https://doi.org/10.3390/cosmetics10010015
Chicago/Turabian StyleJairoun, Ammar Abdulrahman, Sabaa Saleh Al-Hemyari, Moyad Shahwan, Faris El-Dahiyat, Sa’ed H. Zyoud, Obaida Jairoun, and Maher Al Shayeb. 2023. "Development and Validation of an Instrument to Appraise the Tolerability, Safety of Use, and Pleasantness of a Cosmetic Product" Cosmetics 10, no. 1: 15. https://doi.org/10.3390/cosmetics10010015
APA StyleJairoun, A. A., Al-Hemyari, S. S., Shahwan, M., El-Dahiyat, F., Zyoud, S. H., Jairoun, O., & Shayeb, M. A. (2023). Development and Validation of an Instrument to Appraise the Tolerability, Safety of Use, and Pleasantness of a Cosmetic Product. Cosmetics, 10(1), 15. https://doi.org/10.3390/cosmetics10010015