1. Introduction
The amount and distribution of epidermal melanin determine the color of skin. Because Asians have more melanin than Caucasians, they have better natural photoprotection. As a result, they have a higher risk of pigmentary diseasescaused by skin darkening due to increased melanin in the skin layers. The most prevalent epidermal abnormalities are lentigines, ephelides and melasma, while nevus of Ota and Hori’s nevus are also typical dermal pigmentary diseases in this group [
1,
2].
Asian people have a higher-end range of skin phototypes, varying from Fitzpatrick types III to V, compared to Caucasians, who usually have skin varying form phototype 1 to 3 [
3]. For this reason, physicians continue to be cautious towards Asian patients due to the increased risk of pigmentary changes and scarring following any surgery or laser therapy that may cause skin irritation, since they respond to aesthetic treatment modalities differently, given the higher presence of melanin in their epidermis [
4,
5].
A laser is an optical and electronic device capable of emitting a coherent beam of light. The theoretical bases that led to the construction of these devices were proposed by Albert Einstein in 1917. Originally, a machine capable of producing microwaves in a coherent way was built in 1953, and then, 7 years later, a device capable of using a ruby to produce 694 nm light amplification was patented. In 1958, the Q-switching mode, a modality capable of producing light peaks with an extremely high peak power (in the order of Gigawatts) was proposed by Gordon Gould, and then discovered independently in 1961 and 1962 by R.W. Hellwarth and F.J. McClung using a ruby laser. In the subsequent years, different gasses and materials were used to generate coherent light beams with different wavelengths, such as the use of helium and neon to produce an infrared beam, or the use of carbon dioxide to produce a 10,600 nm beam (an ablative laser also used nowadays in the management of various benign clinical conditions, such as seborrheic keratosis, and used in the fractional mode for skin rejuvenation) in 1963. In the subsequent decades, dozens of different lasers, with different purposes, in medicine, as well as in the industrial field, have been developed. In the medical field, lasers targeting more or less selectively specific molecules were preferred and further developed, with the ability to hit a specific target using the theory of “selective photothermolysis”. Laser pulse durations must be less than or equal to the thermal relaxation time of the target, in order to selectively act on pigmented lesions, hair removal, vascular lesions, tattoos and skin resurfacing without damaging the surrounding tissues. The latter situation is particularly worrisome for patients with a high content of chromophores in their skin, demanding a higher degree of attention from clinicians because these individuals respond differently to cosmetic treatment techniques, with increased risks of pigmentary alterations and scarring after any surgery or laser therapy [
1,
2,
3,
4,
5,
6].
Because of this delicate situation, lasers that work directly on chromophores have been explored on Asian people, with excellent outcomes. Lasers with different wavelengths and emission modalities have been proposed, with variable results and side effect risks. Q-switched laser systems release a high amount of energy in brief time intervals (in the range of pico or nanoseconds and with a wavelength of 532–1064 nm) [
6]. These lasers involve the selective destruction of melanosomes by photomechanical and minimal thermal effects while sparing surrounding tissues, making them the most efficient and safe therapy for benign hyperpigmentation [
7]. Although a big percentage of the current literature proposes the use of this kind of laser on Caucasian populations, more and more scientific evidence suggests that this laser may be equally effective also on people of Asian descent, especially those with lighter phototypes [
7]. That is why this article aims to study the efficacy of Q-switched lasers also on darker phototypes, so that clinicians can feel more confident and be more aware of the results when patients with darker skin colors come into the clinic.
This article looks at the safety and effectiveness of Q-switched 1064/532 nm picosecond lasers in removing various forms of benign hypermelanosis in Asian people, and also evaluates the possible associated side effects.
2. Materials and Methods
During the period ranging from 1 January 2019 to 1 January 2021, Asian patients with benign hyper-pigmentation were consecutively enrolled in this study at three different Italian dermatological clinics: Magna Graecia University (Catanzaro, Italy), Tor Vergata University (Rome, Italy) and Villa Bella Antiaging Center (Bologna, Italy).
The following patients were not included in the study: those who had undergone previous laser or light treatments for removing hyperpigmentation, those on gold-containing medications, those who had undergone exfoliating procedures within the last 3 months or surgical procedures of any kind within the last year, those with prior skin inflammatory conditions (in order to reduce the risk of Koebner phenomena) as well as keloids, those with hypersensitivity to light (visible and near-infrared), those on medications that make users more sensitive to light, anticoagulant and immunosuppressant treatments, those in gestation or who were breast-feeding, those with a personal or family background of skin malignancy, as well as those who had had sunlight exposure in the three weeks prior to the treatment. The study was approved by a local ethics committee, all patients signed an informed consent form acknowledging the procedure’s risks, and all patients agreed to be photographed and to be shown the photographs.
Lesions were clinically categorized into epidermal and dermal lesions through a spectral analysis of melanin (Antera). is the analysis was based on a 3D camera connected to a computer that allows the precise measurement of skin structures. It was also possible to analyze the skin in two and three dimensions and to conduct a multi-spectrum observation of the pigmentation of the epidermis and dermis, in order to decide a better treatment for the patients.
The patients were treated with a 1064/532 nm Q-switched laser system (SmartPico, Deka M.E.L.A., Calenzano, Italy), which delivers ultrashort pulses to provide the selective photothermolysis of the target (melanin) with minor thermal damage to adjacent biological tissues.
The treatment parameters were as follows, though they were flexible and based on the area of interest, type of hyperpigmentation and skin phototype: picosecond 1064 nm, 0.8–3 J/cm2 for dermic lesions and picosecond 532 nm, 0.3–1 J/cm2 for epidermal ones. The following criteria were used in the treatment of melasma: fluence 0.5–1.5 J/cm2, 1–2 Hz and picosecond 1064 nm.
The laser was used with a single pulse and several passes until the treated lesion was whitened. The interval between laser treatments was at least 30 days, or until the tissue had completely healed from the last procedure. Three months following the last surgery, a final examination and follow-up visit was held; the clinical aim was the total elimination of the lesion.
Clinical photographic documentation was completed before the first session and was repeated three months later. The same camera (Nikon 5600d, Nikon Corporation, Minato City, Tokyo, Japan) and settings were used, as well as the same shooting options, a dual flash and the same illuminance.
Two dermatologists independently reviewed the photos and assigned a score on a 5-point scale to the outcome of the hyperpigmentation reduction procedure:
- -
0–20% removal, score 0;
- -
20–40% removal, score 1;
- -
40–60% removal, score 2;
- -
60–80% removal, score 3;
- -
80–100% removal, score 4.
During the three-month follow-up, the patients were given a visual analogue scale (VAS) from 1 to 10 to evaluate their contentment.
Statistica 14.0 was used to analyze the data (mean, standard deviations and rate calculations) (TIBCO Software, Palo Alto, CA, USA).
3. Results
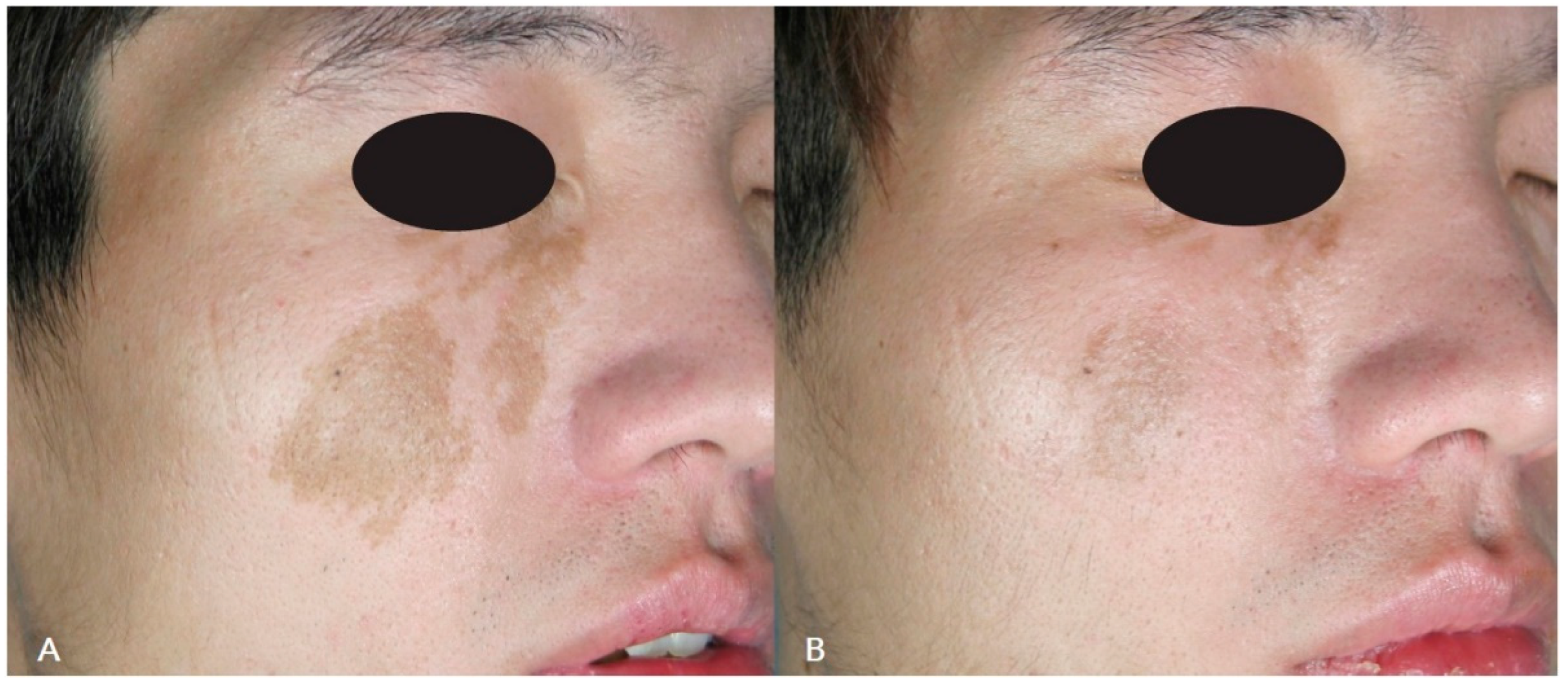
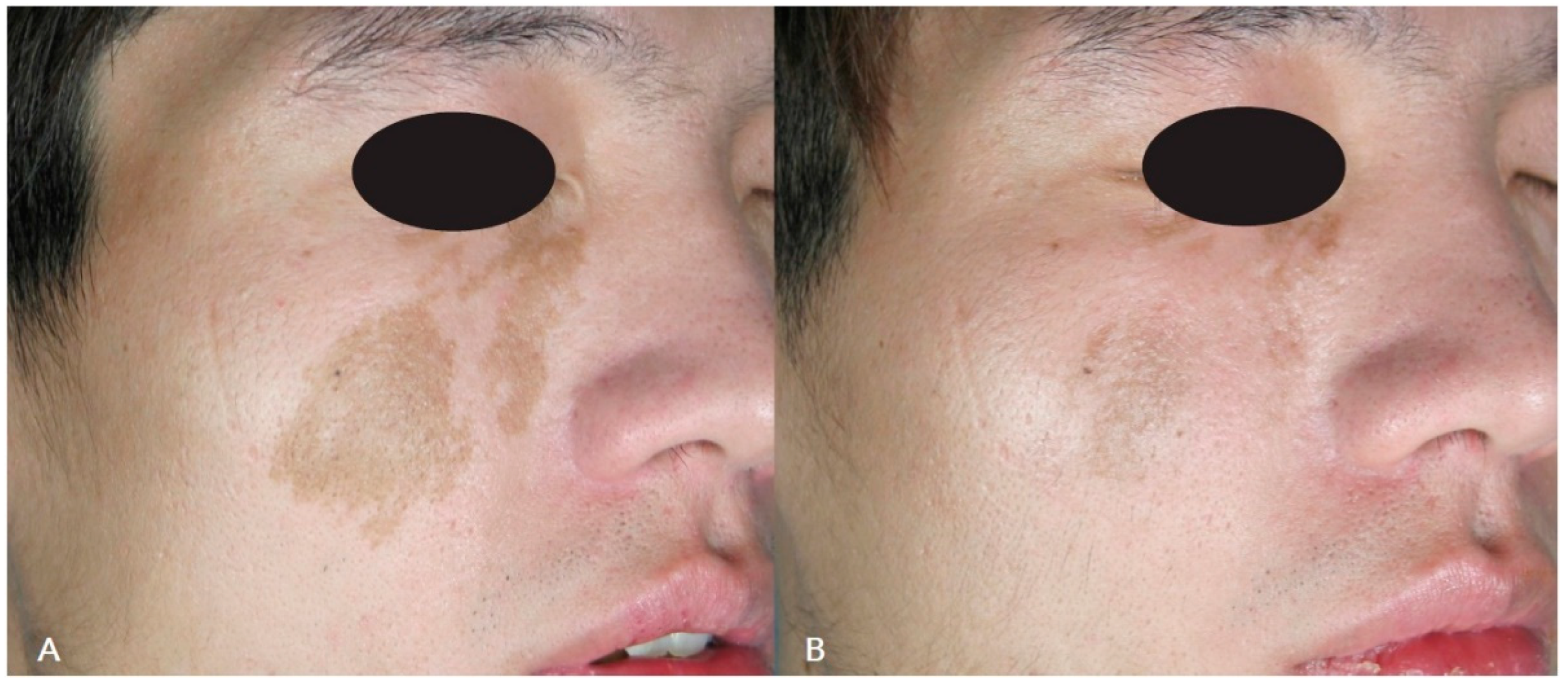
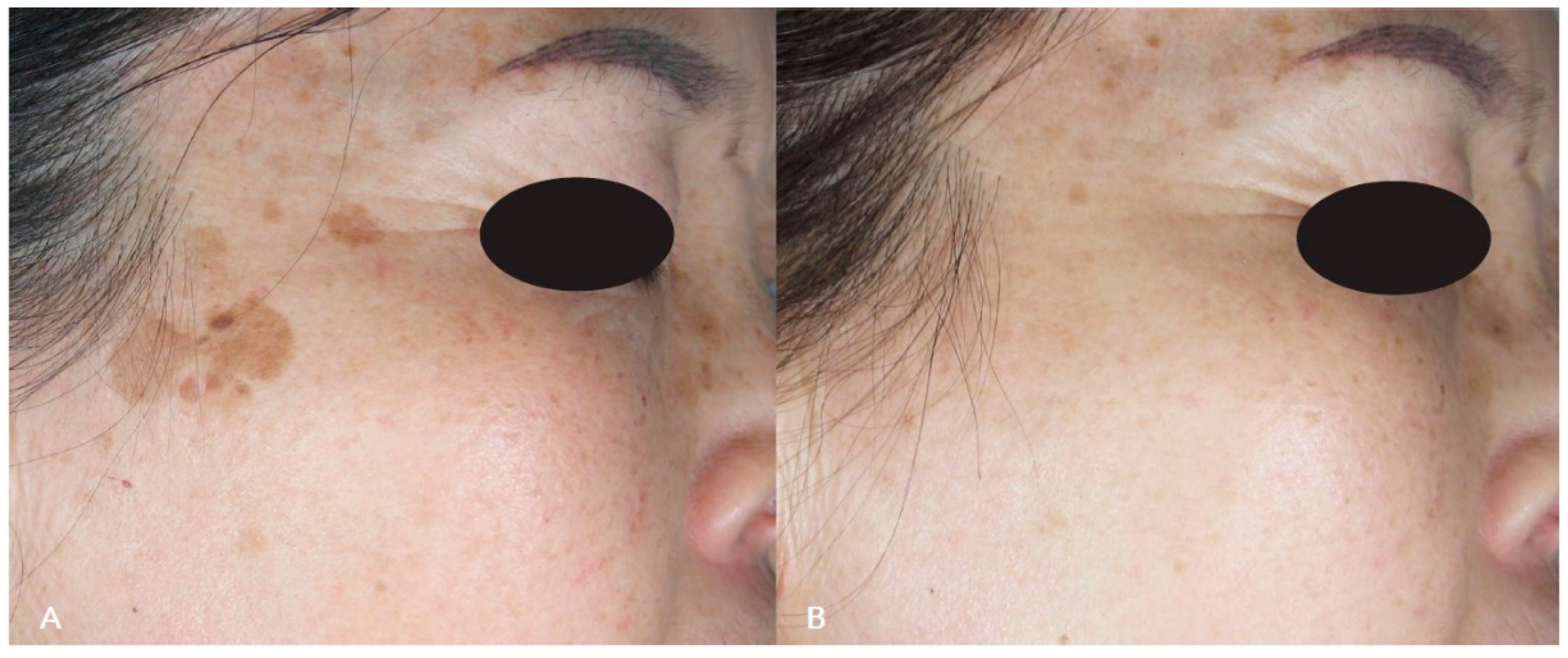
A total of 31 participants were included in the research; 25 (80.4%) of them were women, and 6 were men (19.4%). The average age was 48.96 ± 13.68 years. According to the Fitzpatrick scale, the participants’ skin tones varied from type II (n = 2, or 6.4%), through type III (n = 13, or 41.9%), to type IV (n = 16, or 51.6%). Just 3 (9.7%) cases of hypermelanosis affected the dermis, while 28 cases of hypermelanosis (90.3%) included the epidermis. There were only two melanoses (6.4%) on the extremities and one (3.2%) on the trunk, with the majority of hypermelanoses (n = 28, or 90.3%) occurring on the face.
The elimination of hyperpigmentation required up to four treatments, with 1.6 ± 0.7 sessions being the average amount of treatments. Dermal lesions may instead require more treatments (
Figure 1,
Figure 2,
Figure 3,
Figure 4 and
Figure 5).
A clinical evaluation reported a mean score of 2.70 ± 0.78, with a higher mean score being reported for epidermal hyperpigmentation and a lower score being reported for dermal melanosis, indicating a generally lower level of success in the therapy of the latter type of lesions.
Patients reported a mean VAS score of 7.03 ± 1.35, with the patients treated for more superficial lesions reporting a higher score than those with other types of lesions. The results of the VAS score appeared to be unaffected by the patients’ age.
No significant adverse events happened, and all patients tolerated the therapy well. Most of the participants who had received laser treatment described temporary perilesional erythema and edema, occasionally accompanied by itching that went away on its own in 1 to 3 days. Other common post-treatment changes included the treated area of melanosis getting darker and being covered by a flaky or crusty formation, which was exfoliated and turned into temporary hypopigmentation until completely healed (when there were no more visible effects) within 30 days.
Table 1 reports the characteristics of the patients. We underline how the VAS scale score was strictly linked to the Fitzpatrick phototype: two patients of phototype 2 gave an average VAS of 8.5; thirteen patients of phototype 3 gave an average VAS of 6.61; sixteen patients of phototype 4 had an average VAS of 5.75. This demonstrate how results in darker skin are less satisfying than those in lighter phototypes although they are still considered good outcomes.
4. Discussion
In cosmetic dermatology, the demand for the elimination of benign melanosis is increasing more and more due to aesthetic concerns [
8]. These procedures have been performed on non-Caucasian skin for many years. Some Asian cultures are obsessed with the quality and texture of skin, and whitening products and procedures are widely present on the market. The Korean population, for example, is particularly sensible to skin whitening treatments and to the removal of hypermelanosis. In order to improve and standardize treatments, it is appropriate to have even more information on the experiences of people of these phototypes [
9].
Laser therapy should be applied when it is certain that the lesion is benign [
7]. Ablative lasers were traditionally proposed in the management of lentigos and other superficial melanosis, while in time non ablative laser treatments targeting melanin have also been proposed, arriving nowadays at the use of lasers targeting melanin with very high fluences for a very tiny fraction of a second, in order to prevent surrounding tissue from damage. Before performing any physical therapy on a pigmented lesion, it is crucial to be sure that the lesion is benign; therefore, the use of dermoscopy is often necessary in order to evaluate findings since it is capable of distinguishing potentially worrisome lesions. Dermatoscopes, especially when combining polarized and non-polarized modes, can show all the necessary features to distinguish benign from malignant lesions. Of course, when there is doubt about the nature of the lesion, it is always better to surgically remove it and not to treat it with laser therapy, in order to prevent a recurrence of the lesions and a diagnostic delay in the case of malignant lesions. For example, a pigmented lesion that shows a blue-grey color or globules under dermatoscopy, or non-homogeneous thickenings, a thickening around the follicles or rhomboidal pigmented structures, should not be treated with laser therapy, but instead, an incisional/excisional biopsy should be performed.
Because Asian skin is more pigmented than Caucasian skin, epidermal melanin can interfere with laser treatment on dermal lesions; the absorption spectra of melanin and most cutaneous laser wavelengths overlap significantly [
10]. As a matter of fact, melanin absorbs light and heat considerably well between 532 and 1064 nm, which are values somewhat involved in the majority of commercial lasers currently available. As a result of the increased absorption of laser energy and resultant damage to melanin-laden cells, darker skin poses a considerable challenge, raising the likelihood of undesirable outcomes such as hypopigmentation, hyperpigmentation, and depigmentation [
4]. Furthermore, dark skin keratinocytes degrade melanosomes at a slower rate than white skin keratinocytes do.
The selective elimination of melanosomes has been demonstrated by exposing skin to Q-switched (QS) laser pulses, thanks to their limited thermal effect on surrounding tissues [
7].
Innovative QS lasers effectively remove the smallest pigment particles in hyperpigmentation. They deliver their energy through handpieces with different profiles (round, angular or fractional) to adapt to pigmented lesions and skin discolorations. The different shapes and sizes of the handpiece spots combined with the different emission modes (pico and nanoseconds) make these new laser devices the most flexible laser systems for effective treatment with minimal contraindications. Additionally, these lasers use reflectance mapping of several various light wavelengths to calculate the quantity of melanin in different skin layers, allowing for a standard measurement of aesthetic outcomes. On the other hand, the high cost of the devices, as well as the high cost of maintenance are limitations in terms of the availability of these devices.
All these Q-switched lasers can be used to treat superficial epidermal lesions like lentigines and ephelides, café-au-lait macules, seborrheic keratosis and dermal pigmented lesions such as Ota/Ito nevus, infraorbital hyperpigmentation and drug-induced hyperpigmentation [
11].
In Asians, lentigines are a typical indicator of photoaging. This type of pigmented epidermal lesion responds well to the QS system (532 nm), with the picosecond and nanosecond laser [
12]. The QS alexandrite laser (755 nm) and the QS ruby laser (755 nm) are two other QS lasers employed on Asian lentigines (694 nm). With QS lasers, which benefit from achieving considerable clearance even after one treatment session and are particularly successful for lightly pigmented lentigines, the risk of post-inflammatory hyperpigmentation (PIH) in the Asian population is believed to be around 10–25% [
13,
14].
On the other hand, other studies [
15,
16,
17] use another method to eradicate lentigines: more extended pulsed lasers in the microsecond range that match the epidermis’ thermal relaxation period, limiting the thermal harm to the epidermis. According to these studies, the danger of PIH associated with long-pulsed lasers is decreased because of the absence of the photomechanical impact connected to the use of QS lasers. Nevertheless, our study did not find a significant number of PIH or other severe or mild adverse events.
Moreover, IPL (intense pulsed light) can be used, but it requires many more sessions of treatment, as well as involving a higher risk of side effects and having an overall lower effectiveness [
13], demonstrating that the Q-switched laser is superior to IPL, requiring fewer sessions.
Macules, known as “café au lait spots”, can range in length and diameter from very few millimeters to several centimeters and can be congenital or first manifest themselves during the patient’s younger years [
18].
The use of a fractional Q-switched ruby laser (FQSRL), intense pulsed light (IPL) or pulsed dye laser (PDL) on a café-au-lait macule (CALM) in Asian patients is a safe treatment option, but the risk of recurrence is high [
4,
19]. Q-switched 1064 nm lasers are more commonly used to treat these lesions, with favorable outcomes and no lasting adverse effects, such as scaring, speckled hypopigmentation and post-inflammatory hyperpigmentation (PIH). In addition, there is a much lower risk of recurrence [
20].
Melasma is a symmetrical hypermelanosis that often develops in Asians. It is characterized by hyperpigmented macules present mainly on cheeks, the temporal region and forehead. Solar exposition may enhance hyperpigmentation. It is often associated with pregnancy, birth-control medications and hydantoin-containing drugs. It has a detrimental influence on the patient’s quality of life and does not respond to many treatments. Melasma results from a complicated interplay involving epidermal melanocytes, keratinocytes, dermal fibroblasts, mast cells and vascular endothelial cells, despite being formerly classified as epidermal and dermal [
21,
22]. The etiology is multifactorial, depending on genetic predisposition, but also on skin type and hormones. Melasma may affect the epidermal layer of skin, with an increase of melanin in the basal layer of the epidermis, as well as the dermis, with the presence of macrophages in the dermal papillary layer’s phagocytizing melanin, or affect both layers, thus being more difficult to treat. A wood lamp may also be used to evaluate if an epidermal or dermal component is present in the melasma, as dermal melasma is usually darker when observed under a wood lamp. Melasma severity may be evaluated using the melasma area severity index (MASI). Differential diagnoses include lentigo, friction melanosis, endogenous and exogenous ochronosis, toxic melanoderma, Riehl melanosis, post-inflammatory hyperpigmentation, cutaneous lupus erythematosus, as well as phytophotodermatitis, ototoxicity and actinic lichen planus.
By enhancing the activity of pigment cells, estrogen causes skin pigmentation. Estrogen and progesterone, especially in the event of pregnancy, may act additively or synergistically to cause hyperpigmentation by promoting melanogenesis in melanocytes. [
23]
Asian patients with melasma can be treated with IPL at 570 nm and 590–615 nm filters, improving after 16 weeks. However, re-pigmentation can be observed at the end of treatment, indicating that maintenance therapy may be required [
13,
24]. Otherwise, melasma significantly improves when treated with a 1064 nm wavelength and picosecond laser. It is also safe and well-tolerated by the patients [
25], with minimal risks of PIH, even though the complete resolution is challenging to obtain [
13,
26].
Nevus of Ota is a dendritic melanocytosis of the papillary and upper reticular dermis that affects the eye and surrounding skin and is innervated by the first and second branches of the trigeminal nerve [
27]. QS lasers are beneficial in treating this condition, possibly even with fewer session treatments than usual, to reduce the negative consequences of repeated laser stimulation on the skin [
28,
29].
Unlike nevus of Ota, pigmentation in acquired bilateral nevus of Ota-like macules or Hori’s nevus (ABNOMs) is symmetrical, has a late beginning in adulthood, and does not affect mucosa. Clinically, it is distinguished by the bilateral presence of blue-brown, slate-gray, speckled or confluent macules on the face. The lateral side of the forehead, the temple, the malar region and the root of the nose are the key areas affected by ABNOM [
30]. ABNOMs are usually successfully treated using QS pigment-specific lasers. Treatment responses to these have been less successful than those of the Ota nevus, and numerous successive treatments are necessary to obtain the desired results [
4].
Both in nevus of Ota and Hori’s nevus patients, before introducing ns-QS lasers, treatment procedures like cryotherapy and dermabrasion frequently resulted in scarring or substantial textural or permanent pigmentary alterations. The ns-QS Nd:YAG, ns-QS ruby, and ns-QS alexandrite lasers have proven to provide good clinical results and have become the standard of treatment in the management of these conditions, as well as in treating various forms of benign epidermal and dermal melanosis [
31].
Laser treatment of Asian skin is challenging due to the darker skin color and the higher predisposition to having dyschromia and hyperpigmented lesions. At the same time, adverse reactions can be more evident and long-lasting due to the significant vulnerability of darker skin and the increased absorption of laser energy. Therefore, test locations and long-term follow-up should be addressed when treating darker skin. Sun avoidance or the use of premedication treatments (such as hydroquinone in a percentage variable from 2% to 5%, or creams combining this drug with a small number of steroids or retionids), in order to reduce the quantity of melanin present, may be useful in obtaining better results.
Our findings support what has been published in the medical literature, indicating that Q-switched laser treatments are effective and safe for treating hyperpigmentation in Asian patients. Unlike what some studies have reported, the risk of PIH was minimal and marginal, and there were no serious adverse effects observed. Of course, protection from sun with sunscreen creams and sun avoidance during the peak hours are recommended after any treatment to reduce hyperpigmentation.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}