1. Introduction
Stretch marks, also called striae, are a form of tissue damage on the skin due to an excessive stretching of the dermis [
1,
2]. Stretch marks are commonly associated with pregnancy and affect between 60% and 90% of women during their pregnancy [
3]. In reality, they occur as the result of tearing of the dermis during periods of rapid growth of the body or some body parts. Therefore, around 27% of adolescents are concerned by stretch marks [
3]. As they are caused by the sudden expansion of the skin, especially in areas where fat is most likely to be stored in our body, obesity may lead to the apparition of stretch marks. Stretch marks are thus usually found on the breasts, thighs, and belly, especially near the navel, upper arms, underarms, and lower back, both in women and men [
4].
Stretch marks affect the dermis by preventing the fibroblasts from organising collagen fibres to keep up with the skin’s stretching. The collagen bundles are altered, lose their orientation, and are organised into a fibrotic structure, while the elastic network is also disrupted [
5]. As a result, the skin appears less firm, less deformable, and less plastic. This normally leads to epidermal tearing, which can produce a lesion in the form of a visible stretch mark. Stretch marks could be classified into six different types depending on their appearance and epidemiology;
striae atrophicans (thinned skin),
striae gravidarum (following pregnancy),
striae distensae (stretched skin),
striae rubrae (red),
striae albae (white),
striae nigra (black), and
striae caerulea (dark blue) [
4]. Over time, stretch marks tend to atrophy and lose pigmentation, depending on how recent they are on the skin. Thus, hyper-pigmented stretch marks related to an acute stage are characterised by the initial erythematous, and a chronic stage is characterised by a hypo-pigmented and atrophic lesion [
6].
Current treatment involves invasive methods such as laser therapy, light therapy, collagen injection, laser lipolysis, radiofrequency techniques, and microdermabrasion [
1,
6,
7]. A topical solution may be used, and among these, a formulation with CAST has been described to improve stretch marks, but its mechanism of action is poorly described [
8,
9,
10,
11]. CAST is one of the most known traditional medicinal plants. It has long been used to promote skin repair and wound healing, and it is a medicinal remedy present in the Ayurvedic system and traditional Chinese medicine [
12]. It grows in cultivated fields in Madagascar and other Asian and African countries. It expresses, in its tiny and round leaves, as secondary metabolites, some biologically active triterpenic molecules (asiaticoside, asiatic acid and madecassic acid) [
13]. CAST is a promising candidate to solve stretch mark concerns as it enhances cell production and matrix components and improves tensile strength [
12]. Clinical studies have shown that the application of a formulation with CAST significantly improved stretch mark appearance [
9,
14]. We have also previously conducted a clinical study on 54 women divided into two groups (the control group applying a placebo formula without CAST and a group using a formulation with CAST [
15]). The volunteers used the product three times per day for one month. After four weeks of using the CAST formulation, skin thickness at the edge and in the centre of the stretch marks was significantly increased in comparison to the placebo, such as skin vascularisation and elasticity for a visual reduction in stretch marks appearance [
15]. Following this preliminary work, we wanted to explore the mechanism of action of CAST further, and the aim of this study was to unveil potential unknown pathways that can be impacted by CAST at the in vitro and ex vivo levels. Transcriptomic analysis was performed in order to identify potential new actors in stretch mark-related fibrosis, such as CGTF. Modulation of its expression by CAST could be the result of improvement of the dermal matrix, improving the quality of the dermis and thus reducing stretch mark damages.
2. Materials and Methods
The aim of this study was to evaluate the active ingredient obtained from Centella asiatica (supplied by Givaudan Active Beauty, Argenteuil, France) as a new way to solve stretch mark concerns.
Centella CAST (INCI: asiaticoside, asiatic acid, madecassic acid) was obtained by Indena Spa, Viale Ortles 12, Milan, Italy. The product is obtained through the extraction, fractionation, and recombination of terpenes typical of Centella asiatica, which are the major bioactive constituents. These include asiaticoside, in which a trisaccharide moiety is linked to the aglycone asiatic acid, madecassoside, and madecassic acid. Centella asiatica is sourced in Madagascar, and leaves are hand collected from spontaneous growth during their growing season, harvested, and naturally dried. After a preliminary extraction of Centella soft extract, the product is concentrated and purified to the first fraction of asiaticoside. Discarded solutions are concentrated, the pH is adjusted, and the fraction is purified to obtain the madecassic and asiatic acid fractions. The asiaticoside fraction and the acids fraction are then mixed to match the specifications. This natural extract has a very fixed composition and is composed of asiaticoside (about 10–16%), asiatic acid (about 6–9%) and madecassossic acid (about 10–14%).
2.1. Wound Healing on Fibroblast
Fibroblasts (NIH-3T3, ATCC CRL-1658) were maintained in supplemented DMEM medium (Gibco®, Life Technologies, Carlsbad, CA, USA) containing 10% fetal bovine serum (FBS), (Hyclone, Logan, UT, USA) and 1% antibiotics (Sigma-Aldrich, St. Louis, MO, USA) (DMEM complete medium) at 37 °C 5% CO2. NIH-3T3 (105 cells/well) were seeded in 96-well Essen ImageLock plates (Essen BioScience, Ann Arbor, MI, USA) and grown to 80% confluence in a CO2-humidified incubator. After 24 h, the scratch was made using the 96-pin WoundMaker (Essen BioScience, Ann Arbor, MI, USA). Fibroblasts were treated with CAST at 1, 5, 10, 25, or 50 µg/mL. FBS 10% was used as a positive control. Wound images were taken every hour for 36 h, and the data were analysed using the integrated metric “relative wound density” from the live-content cell imaging system IncuCyte HD (Essen BioScience, Ann Arbor, MI, USA). The experiments were performed in triplicate wells.
2.2. Transcriptomic Analysis on Fibroblast
Normal human dermal fibroblasts (NHDFs) freshly isolated from non-stretch-marked or from stretch-marked areas from the same donor were seeded at 300,000 cells per well in 6-well plates and cultivated in DMEM medium (Gibco®, Life Technologies, Carlsbad, CA, USA) supplemented by FBS with 10% and 1% antibiotics (Sigma-Aldrich, St. Louis, MO, USA). After 48 h of culture, NHDFs were rinsed two times with PBS (Gibco®, Life Technologies, Carlsbad, CA, USA) and allowed to rest in FCS-free medium overnight before stimulation. Cells were stimulated with CAST extract at 10 µg/mL versus untreated condition. After 24 h of stimulation, total RNA was extracted using the extract-all method (Fisher Scientific, Hampton, NH, USA). RNA quality was controlled, and reverse transcription was performed to obtain cDNA using the Verso cDNA kit (Thermo Fisher Scientific, Waltham, MA, USA). RT-qPCR was performed on specific pre-coated plates (Applied Biosystems, Foster City, CA, USA) designed to study the transcriptomic expression of different genes involved in fibrosis and matrix remodelling with 10 ng of cDNA per well using CFX96 Touch (Biorad, Hercules, CA, USA) and Universal Taqman mix (Quantabio, Beverly, MA, USA). CTGF: Unique Assay ID qHsaCED0002044, FAK: Unique Assay ID qHsaCED0001879, MMP1: Unique Assay ID qHsaCID0017039, MMP7: Unique Assay ID qHsaCID0011537. The relative quantification (RQ) of gene expression was calculated according to POP4 (Ribonuclease/MRP subunit) (POP4: qHsaCID0015127) and B2M (Beta-2-Microglobulin) (B2M: qHsaCID0015347) housekeeping genes. The data are expressed in fold change relative to normal fibroblasts or to untreated stretch-marked fibroblasts.
2.3. Collagen Network Analysis on Skin Explant
Skin explants were obtained according to ethical and regulatory rules and under the agreement of the participants. Skin explants with stretch marks from a 60-year-old female volunteer donor (Biopredic International, Saint Grégoire, France) were treated topically with CAST at 0.5% for 5 days. Each day, treatment and medium (Genoskin, Toulouse, France) were renewed, and explants were incubated at 37 °C 5% CO2.
INCI placebo: AQUA/WATER, CETYL ALCOHOL, GLYCERYL STEARATE, PEG-75 STEARATE, CETETH-20, STEARETH-20, ISODECYL NEOPENTANOATE, PHENOXYETHANOL.
After 5 days, skin biopsies were fixed in formalin (Sigma-Aldrich, St. Louis, MO, USA) for 48 h and then dehydrated overnight by automated dehydration using Histocore Pearl (Leica, Wetzlar, Germany). After dehydration, skin explants were included in paraffin (Leica, Wetzlar, Germany), and skin sections of 4 µm were obtained with a microtome (Leica, Wetzlar, Germany). Paraffin was removed thanks to xylene baths (Sigma-Aldrich, St. Louis, MO, USA) followed by ethanol (VWR International, Radnor, PA, USA) dehydration. Skin slices were stained with a ready-to-use Sirius red colouration (Labo Modern, Gennevilliers, France) before mounting on a thin glass slide. Dermis structure was observed using a bright field, and collagen fibre orientation was analysed in polarised light. Under polarised light, collagen I fibres were detected using the red channel of a slide scanner (Olympus, Tokyo, Japan). The quantity of collagen I was quantified using ImageJ 1.53k software on the whole dermis. Furthermore, the images were oriented with the epidermal part up at 90° of the x-axis. The images were then processed to remove a 200 μm thickness from the outer-most stratum corneum to eliminate the papillary dermis for the orientation analysis of collagen fibres. The conditioned images were processed by a segmentation algorithm, allowing the analysis to focus only on the collagen fibres. Based on a plane parallel to the epidermis, collagen I fibres were quantified at 10° intervals in order to evaluate collagen I occupation in the dermis.
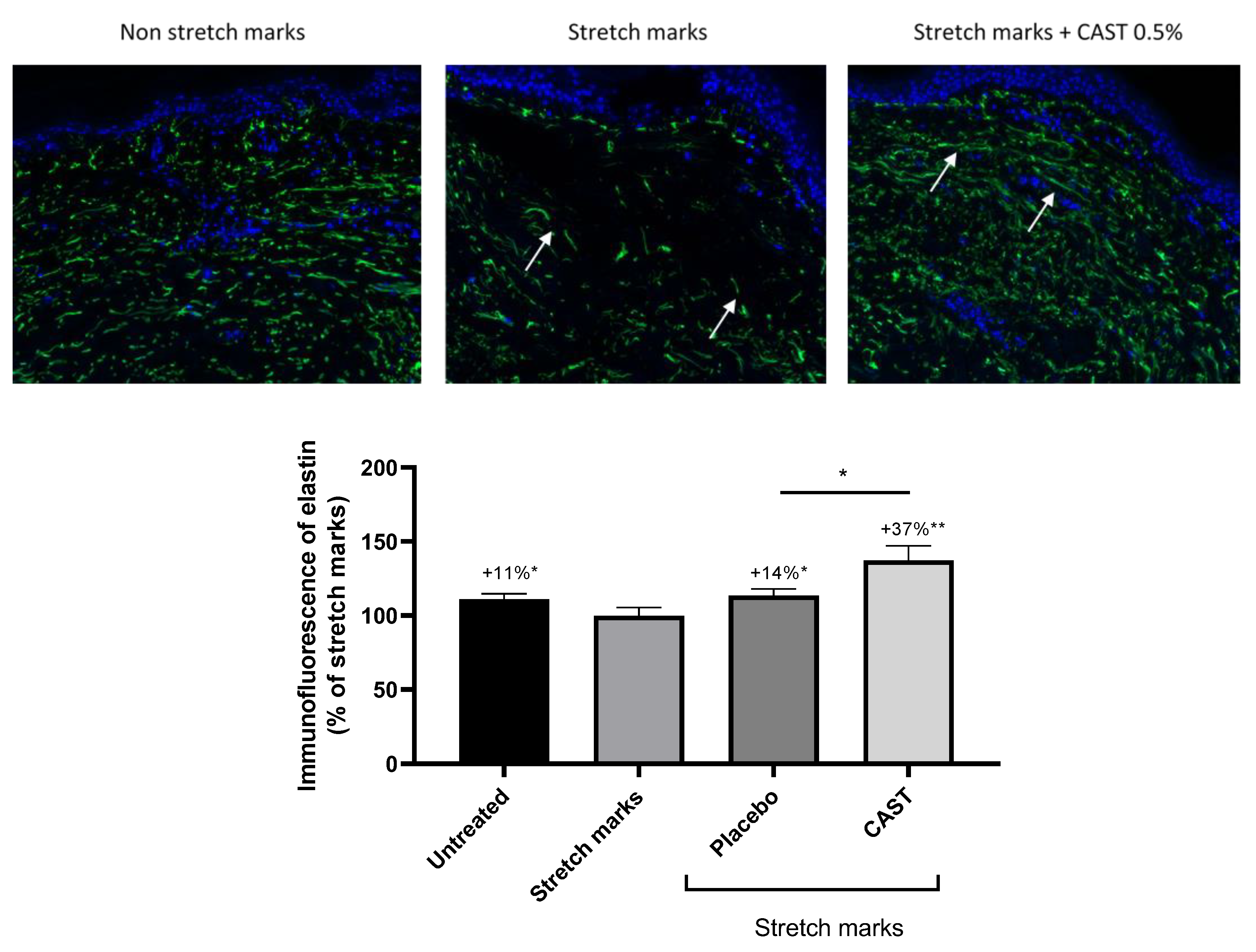
2.4. Elastin Immunofluorescence on Skin Explant
The skin explants were cultivated and treated as previously described. Paraffin was removed thanks to xylene baths followed by ethanol dehydration. Antigenic sites were revealed with a citrate buffer (Sigma-Aldrich, St. Louis, MO, USA). Then, skin sections were BSA-saturated (Sigma-Aldrich, St. Louis, MO, USA) for 30 min, followed by immunostaining to specifically detect elastin (1/75e, Santa-Cruz, Dallas, TX, USA). After overnight incubation of the primary antibody at 4 °C, skin sections were washed and incubated for 1 h with secondary antibody (Anti-mouse, 1/500e, Abcam, Cambridge, UK). The staining was observed using fluorescent microscopy (Zeiss, Axio observer, Iena, Germany). Relative fluorescence was quantified for all images using ImageJ 1.53k software.
2.5. Statistical Analysis
For all studies, a Shapiro-Wilk test was used to verify whether the raw data followed the Gaussian Law. In the case of normally distributed data, the mean values were compared with untreated conditions or normal skin conditions (no stretch marks) using an unpaired t-student test. In the case of non-normally distributed data, a Mann–Whitney U test was used. For all statistical tests, we considered significant results as follows: # p < 0.1, * p < 0.05, ** p < 0.01 and *** p < 0.001.
4. Discussion
Stretch mark concerns are mainly characterized by fibrotic skin. We showed that fibroblasts isolated from stretch-marked tissue expressed fibrosis markers (CTGF and PTK2), leading to an intense Sirius red staining on stretch-marked skin sections. CAST has been described to promote in vitro fibroblast migration, matrix components, and collagen synthesis [
13,
16]. In 2023, Leite Diniz et al. described tissue regeneration, cell migration, and wound repair processes that were mediated by CAST extract, where, among the active compounds, asiatic acid is especially involved in this activity [
17]. Interestingly, during our study, we confirmed that CAST enhanced fibroblast migration, but on stretch-marked skin explants, the quantity of collagen I was not impacted by the treatment. We hypothesized that the effect of CAST at the in vitro level may be different than the effect on ex vivo skin explants depending on the physio-pathological environment and expression of complex markers. For example, a previous study using animal models showed that CAST fastens skin healing by the formation of a thick epidermal layer but with a moderate formation of granulation tissues and collagen, which corroborates our observation in humans [
11,
18]. In the context of pulmonary fibrosis, CAST was able to decrease fibrosis by decreasing collagen I content as well [
19]. However, in addition to the quantity of collagen, the orientation and maturation of the collagen beams are essential. Using three-dimensional video, a study has demonstrated that collagen bundles are disrupted in stretch marks with marked separation of bundles and disorganisation of collagen fibrils, leading to this fibrotic organisation [
20]. By using specific software that quantifies collagen fibres in all directions, we showed that the occupation of the dermis by collagen bundles was significantly improved following treatment with CAST. Finally, regarding collagen, CAST was able to promote maturation and restore the orientation of the bundles without enhancing the quantity of collagen. The elastic fibre network is also disrupted in stretch marks associated with micro fragmentation, and newly formed immature elastic fibres are found in those gaps [
20,
21,
22,
23]. By increasing elastin synthesis, CAST is able to promote elastic fibre networks, and staining analysis has shown the restoration of long, thick, and mature elastic fibres. Indeed, CAST was able to reduce fibrotic gene expression and also matrix degradation via MMPs to prevent this anarchic dermis organisation. Among them, connective-tissue growth factor (CTGF) is upregulated in various types of physio-pathological fibrosis [
24]. Interestingly, an upregulation of CTGF in a stretch mark context has never been described. During our work, we compared a gene expression profile from normal skin and stretch-mark skin, which demonstrated that stretch-mark-related fibrosis involved a strong overexpression of gene coding for CTGF. This CTGF upregulation, which is reversed by topical application of CAST, showed evidence of an improvement in fibrosis through the control of the CTGF pathway. Overexpression of metalloproteinase within a fibrosis context has already been described in the literature by Giannandrea et al. in 2014. They are key proteases for matrix remodelling, but upregulation is the result of fibrosis [
25]. Likewise, our study has revealed that by promoting dermis organisation among the components, CAST works on the physio-pathological pathways of stretch marks.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}