1. Introduction
Exponential human population growth, rapid industrialization, and urbanization have led to massive waste production [
1]. However, Brundtland’s report “Our Common Future” defined sustainable development as: “the development that meets the needs of the present without compromising the ability of future generations to meet their own needs” [
2]. This indicates how, for decades, the international community’s concern is outlined in economic aspects as well as environmental and social ones.
In the European Union, Italy has been one country committed to mitigating adverse environmental and social impacts. An example of Italian awareness regarding this challenge is the regulation DPR n.254 07/15/2003. It defines sanitary waste as the waste derived from public and private structures that carry out medical and veterinary activities for prevention, diagnosis, treatment, rehabilitation, and research, and all waste produced by sanitary activities regardless of its nature. [
3,
4].
Within the sanitary wastes, there is hazardous waste and infectious waste, which refers to waste that could be harmful to humans and the environment [
5]. It is crucial to pay attention to the entire process, from the appropriate handling to the treatment and final disposition and consider that the total elimination of infectious risk can only be achieved using incineration or sterilization.
The typical treatments and disposal systems for handling infectious waste are incineration, sterilization and subsequent destruction, and in some cases, land disposal [
6]. Despite its high cost and effects on the environment, incineration is the most popular method in many contexts [
7,
8,
9]. However, open burning and waste incineration have contributed to a potential risk to human health, since, during the incineration process, dioxins and furans (PCDD/Fs) are released [
10]. These organic pollutants are considered toxic due to their adverse effects on humans and the environment [
11]. On the other hand, traditional steam sterilization facilities usually require two separate phases for the process, one for sterilization and the second to render the wastes unrecognizable [
12], leading to increased precautionary measures during the waste transport between the two phases.
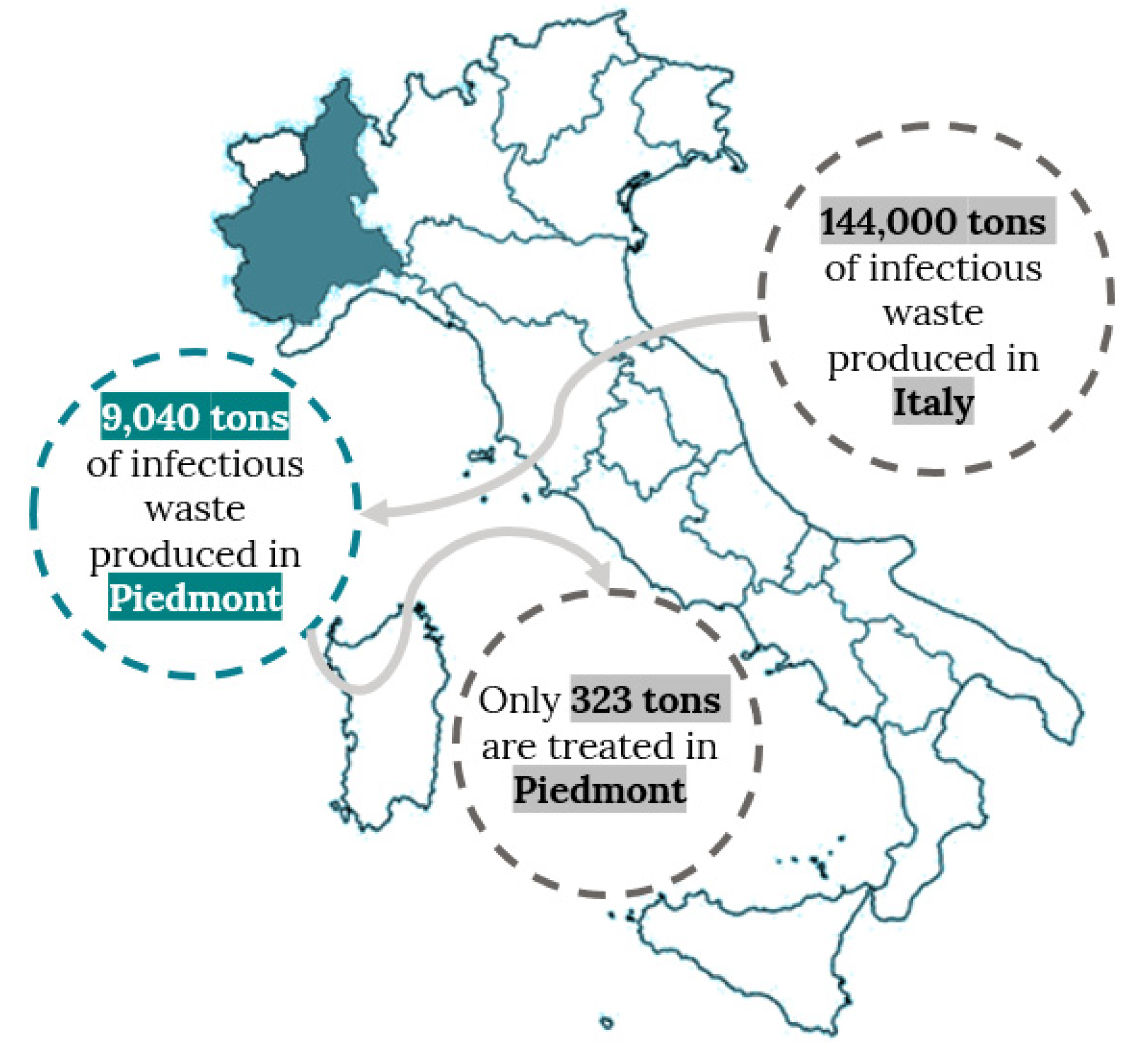
In Italy particularly, the report presented by Istituto Superiore per la Protezione e la Ricerca Ambientale (Higher Institute for Environmental Protection and Research) highlights that infectious waste production in Northern Italy is about 66,600 tons/year, equivalent to 46.4% of the national total, of which, the Piedmont region was responsible for the production of approximately 9040 tons/year [
13].
The primary method of managing infectious waste in Italy is incineration. Nationwide, approximately 66.7% of infectious waste, equivalent to 95,815 tons/year, was handled at incineration plants; the other 33.3% was treated using sterilization [
13,
14]. Additionally, there is the problem concerning the lack of incineration plants for infectious waste or sterilization systems in Piedmont. None of the Italian sterilization plants are located in Piedmont, and there are no incineration facilities in the region authorized by the Italian legislation 152/2006 [
15] to treat the infectious waste directly [
3]. Consequently, all of the waste produced is exported outside Piedmont to other regions, which implies moving infectious waste at least 400 km, increasing health and safety risks.
Given the environmental and social concerns that governments and industries are experiencing, the need to develop methods, systems, and processes that allow for correct and effective waste disposal is unavoidable for any city that aims to become smart and eco-friendly. New technologies focused on sustainability and resource efficiency would counteract the negative social impact of this context. In modern days, while experiencing the effects of COVID-19, the treatment and disposal of infectious waste should be seen as an opportunity to explore ways to generate sustainable solutions, use renewable energy, and improve the population’s quality of life.
This study aims to develop a conceptual design of the main treatment process inside a new infectious waste management system in the Piedmont region. To achieve this, we will use the Design Thinking (DT) framework methodology, a validated, human-centered, and iterative problem solving approach that involves stakeholders from various backgrounds [
16]. DT has been validated as a methodology that can foster sustainability-oriented innovations [
17] by focusing on the users through a flexible development.
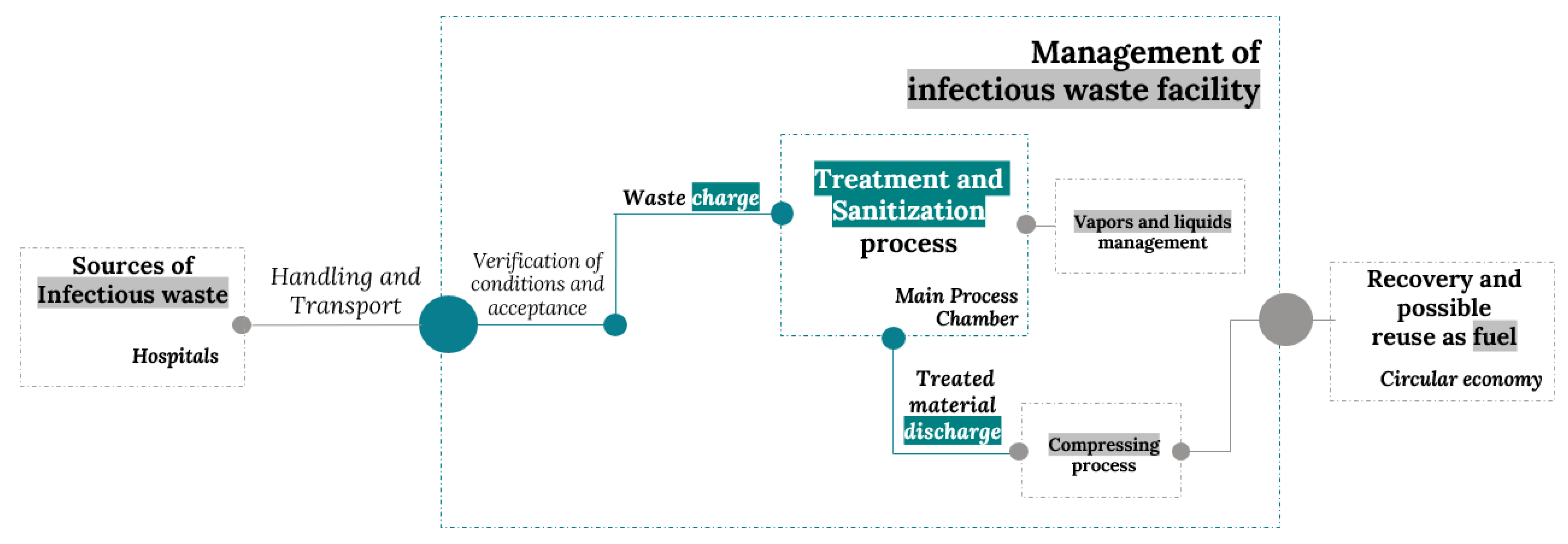
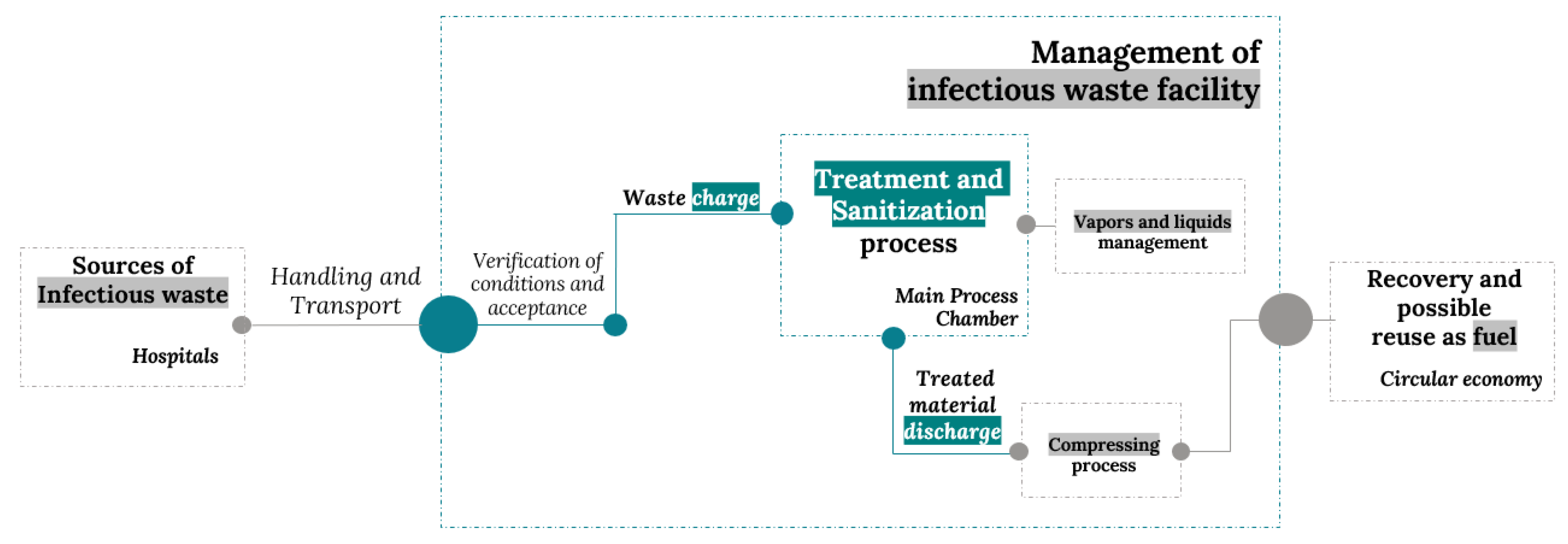
This work is part of a larger research project that attempts to build an automatic process (
Figure 1) for infectious waste management (EWC 180103), characterized by the use of innovative and sustainable technologies, with the challenge to obtain, as a final result, the recovery and possible reuse of infectious waste as a source of renewable energy.
Figure 1 depicts the general scenario of future infectious waste facility management, it should begin with the collection of the infectious waste directly from hospitals and other health facilities, then it must be safely and efficiently transported to a storage center for treatment. After verification of the conditions for acceptance (for example, correct handling and proper packaging) the waste should be taken to the main process chamber for sanitization and the complete elimination of infectious risks. In order to execute this operation, the future management system must include a proper vapor and liquid control system. After the sanitization process, the treated material should be discharged to later be transformed using a compression process into a dry, homogeneous, and compact material. The final process of the future infectious waste management system foresees the recovery and possible reuse of this material as potential refuse-derived fuel.
In the present paper, we focus specifically on the conceptual design of the main process chamber which is responsible for waste treatment and sanitization. Following the waste management system elements proposed by Blackman [
12], which include waste segregation, packaging, transport and handling, treatment, and disposal, this study focuses on the treatment technique. We use the conceptual design definition proposed by Pahl et al. [
18] as the part of the engineering design process where, by identifying the fundamental problems through abstraction and establishing function structures, ideas are concretized into preliminary solutions.
The study is structured as follows: first, we explain the methodology adopted and related works. Second, there is the application of each one of the methodology phases, beginning by describing the problem, context, and stakeholders in the empathize phase. Then we proceed to the define and ideate phases for continuing to the prototyping and testing phases. Finally, we report our results and conclusions.
2. Methodology and Tools
Recently, Design Thinking methodology has been increasingly used by researchers since it shows a new perspective on the challenges posed by interacting with all stakeholders through multidisciplinary groups, formulating a user-centered solution to these problems. Additionally, DT provides a formal process that captures the needs of users [
19]. Its approach is based on creativity, simplicity, and technological innovation, making DT an agent of change [
20]. Together with other methods and tools, it could create resilient, significant, and sustained interventions [
21]. The interest in DT has continued to grow in the last few decades. In recent years, this methodology has been gradually implemented in different companies to create products and services that tend to meet users’ needs better, making them an active part of the creation process [
22]. DT is presented as a methodology to develop human-centered innovation, offering a lens through which challenges can be observed, their needs detected, and be solved. It is a human-centered innovation process that emphasizes observation, collaboration, rapid learning, idea visualization, rapid concept creation prototyping, and simultaneous business analysis, ultimately influencing innovation and strategy [
23].
DT consists of a collection of standard methods in engineering design [
24], but unlike other methodologies from innovation management, it involves the activities of both designers and engineers [
25]. Features such as problem framing, user focus, visualization, experimentation, and iteration allow DT to be an appropriate method for solving complex problems in engineering, such as creating new (or improved) products, services, processes, or technologies), obtaining environmental and social benefits in addition to economic profits [
26]. Through the application of the more than 160 methods and tools associated with DT [
27], these design tools help generate and incubate ideas and, therefore, create innovative solutions [
28].
From the literature review, we found that DT was selected as a methodology framework for similar applications. One example is the design of an organic waste management system solution to evaluate urban recycling in the city of Depok, involving the community and making use of different methods through the various steps of DT such as SCAMPER (Substitute-Combine-Adapt-Modify-Put to another Uses-Eliminate-Reverse), NGT (Nominal Group Technique), and AHP (Analytic Hierarchy Process). DT was validated as an easy-to-use methodology with a fast implementation time and affordable cost [
29]. Another example is the application of DT for organic waste production and management, specifically in Bengaluru city. In this technical report, researchers implemented the empathize, define, and ideate phases by identifying problems and innovative solutions to improve city waste management [
5].
Moreover, DT principles were applied in Ireland to establish a Connected Health Innovation Framework, aligning the healthcare system needs and the software requirements through four stages: identify the healthcare problems/needs, identify the software capabilities, align the users’ requirements, and identify the best solution for healthcare management. This study demonstrates how healthcare innovation supported by DT can complement the engineering process, facilitating the understanding of stakeholders in the context of their day-to-day experiences [
19].
The process of innovation in engineering is a necessity in the search for new ideas that generate value for society, adapting and anticipating changes. According to the literature review, using DT in the process of defining requirements allows for identifying the stages in which this technique is applicable and how it improves the identification of problems, user and stakeholder needs, collection of new perspectives of solutions, generation of solution options and prototypes that allow the representation these ideas. Moreover, the DT approach helps to establish the appropriate scope of innovation for sustainability-oriented solutions. Its strong focus on users and stakeholders encourages the development of sustainability innovation that meets the real needs of users. DT focuses on iterative experimentation and ensures positive sustainability effects while reducing the risk of failure and rejection of innovation. In other words, DT is an approach that uses the designer’s sensitivity and problem-solving method to meet people’s needs in a technologically feasible and commercially viable way.
The previous research provides a foundation that supports the expectations of different investigations about the DT-based approach as an essential but often overlooked asset when addressing sustainability challenges. Lastly, the idea of linking the Sustainability Oriented Innovations (SOI) with DT supports how it can help the organizations with the creation of new technologies, services, and processes intended for environmental and social benefit. SOI challenges like innovation scope, user needs, stakeholder involvement, and assurance of sustainability have specific goals within the DT key principles like problem framing, user focus, diversity, visualization, experimentation, and iteration.
The results of the DT approach can also be seen at the social level for this type of industry; it can help users feel part of the development of a typically rejected technology. DT, in this way, helps to minimize the risk of opposition from the community and phenomena such as Nimby [
30].
Therefore, based on the positive results found in the literature and the DT potential for application, we have selected this user-centered methodology as a framework for the conceptual design of the main automatic treatment chamber for infectious waste management in Piedmont.
DT began to be developed theoretically at Stanford University in California (USA) during the 1970s, and its first for-profit application was carried out by the IDEO design consultancy, who then put together a team to create the first d.school in Stanford, being today its principal forerunner and most significant source of experience [
31]. Considering its experience and the significant availability of validated case studies, this paper has adopted the DT methodology by d.school from Stanford University structured in five phases [
32]: Empathize, Define, Ideate, Prototype, and Test. Since the production costs of a functional prototype are very high and are outside this study’s parameters, we intend to generate a design prototype according to the definition proposed by Polydoras et al. [
33], representing our concept by a CAD model. Consequently, for the test phase, we will evaluate the conceptual design.
As Chasanidou [
34] states, selecting appropriate methods is essential for the correct execution of the DT methodology. The tools can help the team to visualize new perspectives and understand the complexity of the system. Brown [
35], defines three key practices for analyzing a need: insight, observations, and empathy. To get to the insights, we must get as much information as possible about our users and stakeholders during the define phase of the DT methodology. Numerous observation techniques come from anthropology and psychology to empathize in the best possible way and obtain relevant data. Some of them are interviews, context exploration, personas technic, and the Customer Journey Map, used typically during the Define phase. During successive phases, other methods such as brainstorming and focus groups will also be a source of insight, which later will become an input for the definition of the conceptual design requirements.
We considered previously validated studies on DT [
36], and after analyzing the benefits of each tool, we selected for every phase of the methodology a set of tools reported in
Table 1.
This document describes two groups of people: users and stakeholders. Stakeholders refers to a group of people who have a vested interest in the project and are considered key people in the company building a product, often including managers, subject experts, and individuals in charge of verifying compliance with regulations. The user can also be considered a stakeholder; however, not all stakeholders can be considered users. Thus, for this study, the user specifically describes a person who ultimately uses and interacts with the system and who has an actual behavior in the process. Users will be consulted on their views on their needs and desires and will be considered a data resource for technics such as persona and consumer journey map. Opinions from other stakeholders will be also considered during the study.
3. Implementation
The following section will show the implementation of each one of the DT phases described in
Table 1 (empathize, define, ideate, prototype, and test) and the application of the selected tools. To complement the DT definitions, it is important to note that in addition to the five phases reported in
Table 1, the DT process can also be described through three stages called inspiration, ideation, and implementation [
35]. Inspiration is the initial stage. The first part is understanding the problem and the second part is observing how the product is used and how the service is developed. In our scenario, this stage appears during the empathy and define phases. During the ideation stage, it is necessary to generate alternatives and options and to collect ideas to solve the problem by involving users and stakeholders. Notions such as co-creating and brainstorming, typical of the ideate phase, are used in this stage. The implementation stage foresees the prototyping of the possible solution to obtain feedback as soon as possible and, in this way, be able to improve the idea. In our study the implementation stage corresponds to the prototype and test phases.
3.1. Empathize
During the development of new solutions, user interaction can foster the user’s future acceptance of new technologies [
37]. In the empathize phase, we began by analyzing and defining the context of our case. We then characterized the potential users and interacted with them using the established empathize tools.
3.1.1. Piedmont Region Context
In 2018, the Italian production of special waste (produced by industries and companies) amounted to 143.5 million tons. The production of special waste is concentrated in northern Italy, with almost 84.9 million tons/year. Between 2017 and 2018, there was an increase in total production, equal to 3.3%, corresponding to approximately 4.6 million tons/year. In particular, infectious risk wastes produced in Italy amounted to about 144,000 tons/year [
13].
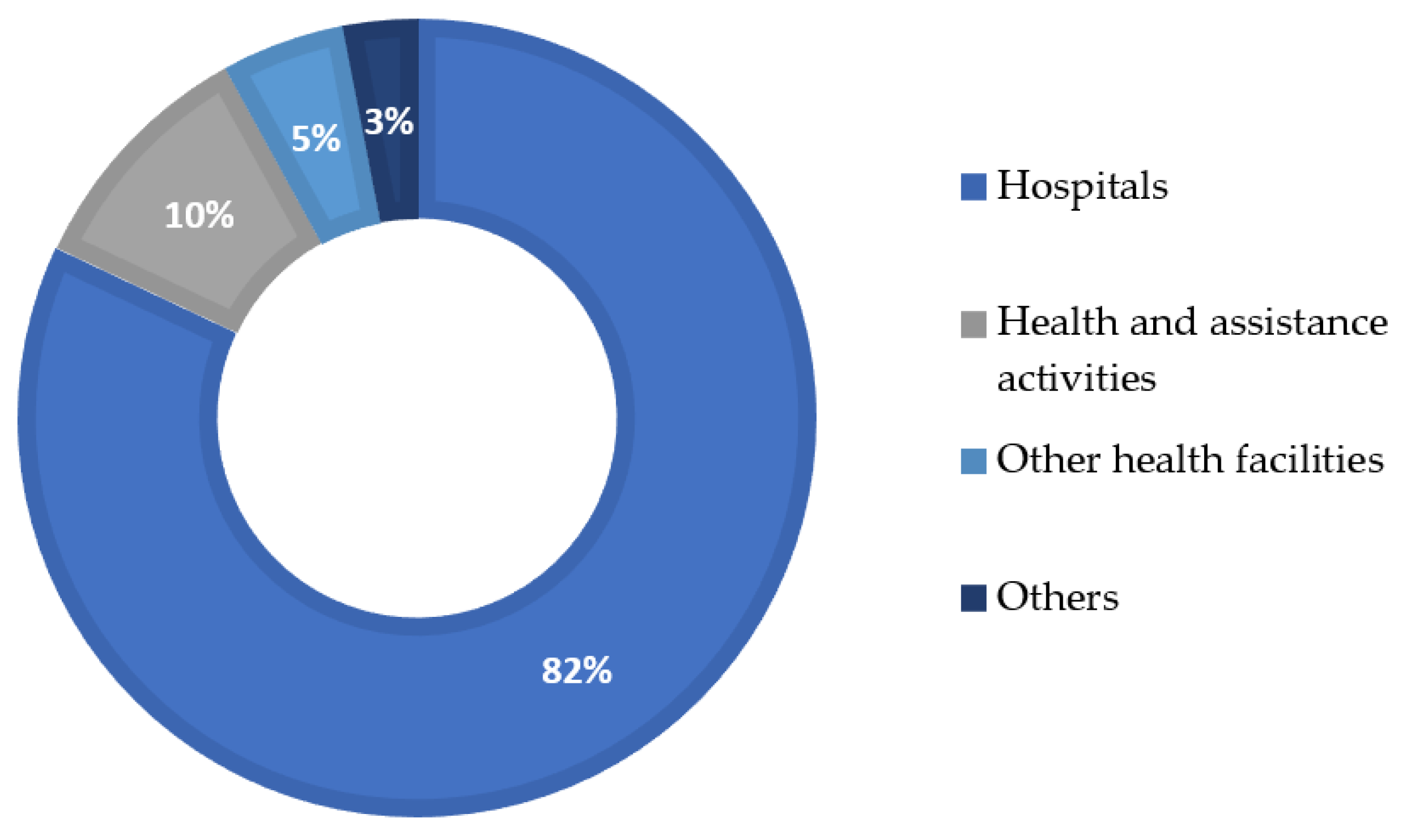
From the last data published by the Piano Regionale di Gestione dei Rifiuti Speciali (Regional Management Plan for special waste), we found that the primary producers of infectious waste (
Figure 2) are hospitals, with 82% of total production. In second place, subjects who carry out health and assistance activities such as, nursing homes, specialist clinics, research institutes, physiotherapy centers, dental centers, and veterinary services (10.4%). In third place, other health facilities, i.e., outpatient clinics or independent laboratories (5%), and in fourth place, subjects who, while carrying out activities other than “health and assistance” or “veterinary services”, have produced infectious waste such as pharmacies and beauty centers (2.6%). [
3]
In 2018, the Piedmont region produced 9040 tons of infectious waste, but only 3.6% was treated inside Piedmont, in the only incineration facility available and authorized to treat this kind of waste (
Figure 3). This incinerator, however, was closed a few years ago. In 2021, all the infectious waste was exported to other regions to be incinerated or sterilized and later destroyed [
3,
13].
Consequently, all the infectious waste produced in Piedmont is sent directly or indirectly (after being in a preliminary warehouse) to other regions, mainly Lombardy, Emilia Romagna, and Liguria. According to the Piedmont regional council [
38], each waste trip to other regions has a capacity of 5 tons, so it is necessary to make more than 1800 trips in a year to transport all of the infectious waste produced in the region. Additionally, the average round trip distance is 1240 km, creating a high environmental impact, producing yearly 7,886,400 kg of CO
2, 3,360,000 kg of PM10, 7,100,050 kg of NOx, and 4,318,176 kg of CO, indirectly affecting the health of the population and creating environmental damage. Therefore, it’s crucial to develop treatment facilities closer to the infectious waste sources within the Piedmont region to mitigate the environmental and health impacts.
3.1.2. Infectious Risk Waste
In Europe, infectious waste is defined and cataloged by the European Waste Catalogue (EWC) as wastes whose collection and disposal are subject to special requirements to prevent infection, and it is classified under the EWC code 180,103 [
39].
Infectious waste in Italy is governed by the regulations on the medical waste management, decree 254/2003; listed in art. 2, it defined “infectious waste” as not only the waste produced by healthcare facilities but also waste produced outside of them with similar infectious risk characteristics [
4]. In other words, all materials that have come into contact with infected or presumed infected biological fluids are considered infectious waste. Furthermore, the kind of waste that must be collected and disposed of by applying special precautions to avoid infections is identified as HP9 “infectious danger” according to EU regulation 1357/2014. Waste with HP9 characteristics contains viable microorganisms or toxins which are known to be or are considered causes of diseases in humans or other living organisms, without concentration limits [
13,
40].
In particular, we aim for a system that can treat primarily hospitals and other health facilities’ waste, including, according to the characterization of the World Health Organization, primarily: infectious waste, suspected to contain pathogens (bacteria, viruses, parasites, or fungi) in sufficient concentration or quantity to cause disease in susceptible hosts, e.g., laboratory cultures, waste from isolation wards, tissues, swabs, materials, or equipment that have been in contact with infected patients; pathological waste, human tissues or fluids, e.g., body parts, blood, and other body fluids; and sharp waste, e.g., needles, scalpels, knives, and blades [
41,
42].
3.1.3. Stakeholders and Personas Technic
The identification of stakeholders allows us to recognize users and groups that may be interested or are involved in the study; identifying and grouping them is part of the empathy phase of DT, since users’ needs are the basis of our analysis. In our study, we define primary stakeholders as any user who has direct contact with waste, for example, hospital managers, doctors/nurses, patients, waste handlers, carriers, and waste management company workers. There are also external stakeholders, such as the government authorities, nearby community, and research centers.
Using the personas technique, we proceed to characterize our active stakeholders. This tool helps to cultivate an innovative mindset and encourages the team to produce ideas through the representation of the stakeholders [
43]. For the creation of
personas, we used explorative qualitative interviews. According to Dickinger [
44], qualitative interviews have a flexible and continuous design, unlike surveys that have a rigid structure. The interviewer uses open questions to direct the conversation flow to obtain the most significant amount of information. According to Revella [
45], to be aware of the user’s patterns, a good rule is to complete at least eight to ten interviews for the
personas. In this order, for our study, we conducted a series of interviews, including three waste management systems managers, two hospitals managers, three workers who are handling the waste, five persons from the nearby community, and ten university students interested in sustainable development, all of them living in Piedmont region. We inquire about their knowledge about infectious waste, waste management systems in Italy, the current Piedmont situation, and techniques. Then we explain our project and ask for opinions.
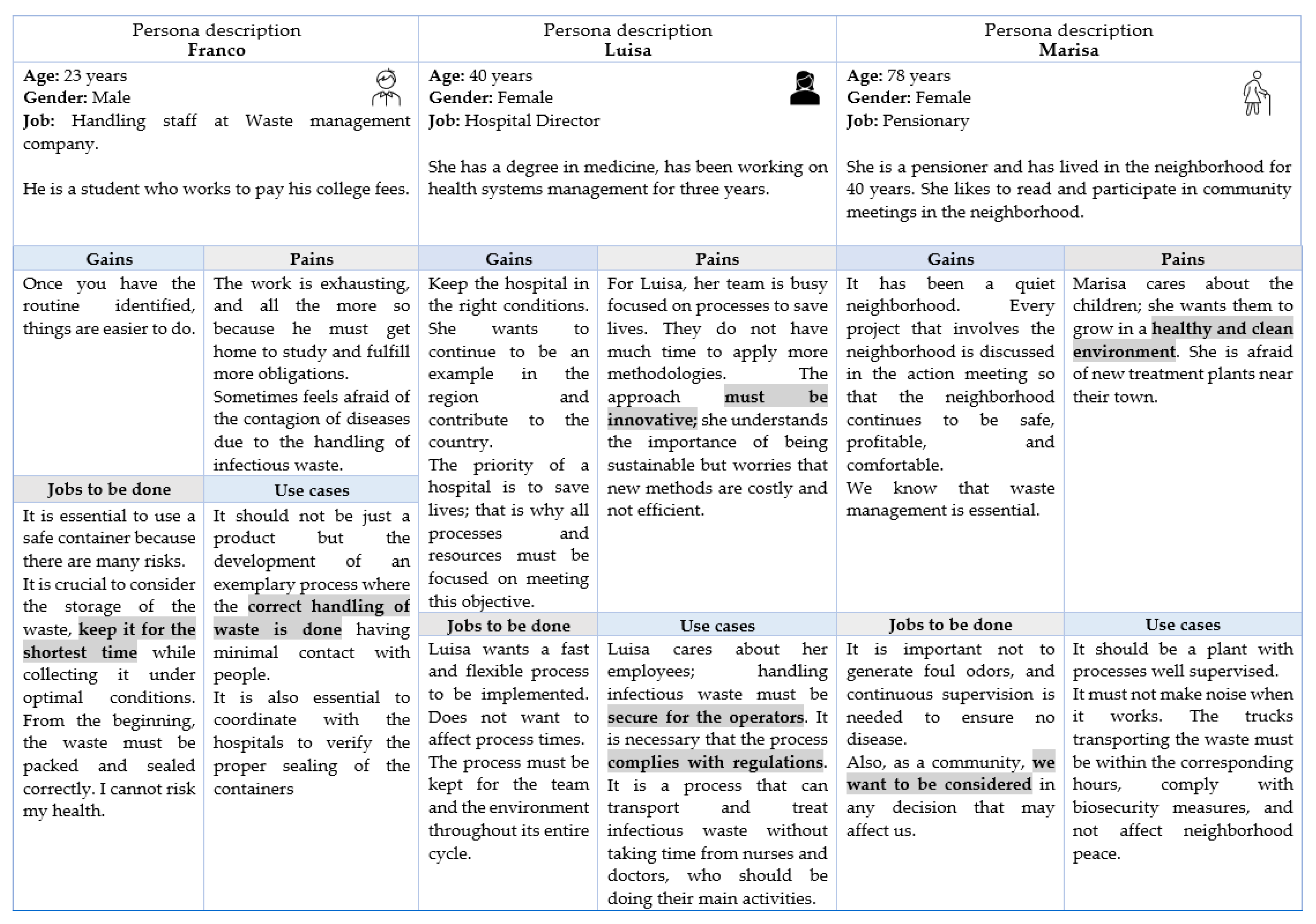
For this paper, we have depicted in
Figure 4 three of the most representative stakeholders, a worker from the company in charge of waste treatment, a hospital director, and a community member. For each one of them, we have reported the gains, pains, jobs to be done, and use cases, according to the user profile suggested by Lewrick [
36].
From the information gathered through the personas, we identified some of our users’ main worries and expectations, mostly related to a safer environment, the safety of operations, regulation compliance, and process innovation. Aligned with DT goals, the community manifests the desire to be included in the development of a new technology and its related process.
3.1.4. Local Regulation
Regarding regulations and their influence as external stakeholders for our study, article 8 of Italian Decree 254/2003 [
4] defines the characteristics of infectious waste treatment. The elimination of infectious risk can only be achieved through incineration or sterilization. Articles 10 and 11 provide specific indications in this regard:
“Infectious waste disposal must be done in incineration plants. Sterilized waste can be used to produce refuse-derived fuel (RDF) or directly to generate energy. Sterilized waste can be disposed of in incineration plants for solid waste or (if these alternatives are not available) they can be disposed of in landfills for non-hazardous waste, for a limited period”.
From this information, we identify the use of sterilization as a potential design strategy and the opportunity to analyze the RDF production for a future scenario.
3.2. Define
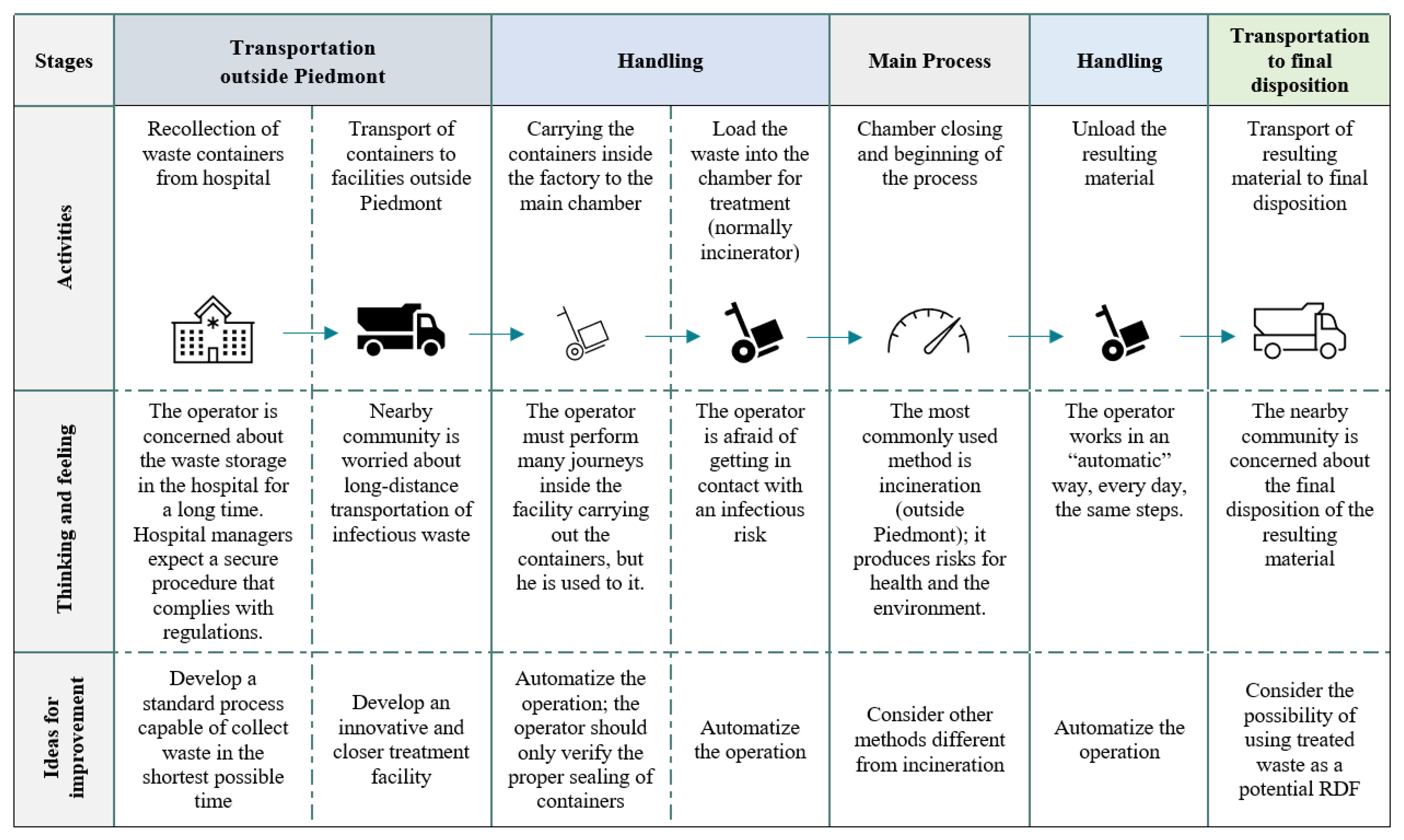
Based on the insights gained from the empathize phase, we use the consumer journey map (
Figure 5) to bring together the context of our research, the activity stages, and the expectations and worries of our stakeholders. It is divided into macro phases, beginning when the wastes are collected from the healthcare unit and ending with the final process in the treatment facility. The visual approach of this tool allows for understanding the overall picture of processes and users’ needs. As Lemon and Verhoef [
46] indicated, it helps to provide a deep understanding of the user experience and can act as the basis for innovation, improving that experience.
Summarizing the problem in Piedmont, there are challenges relating to the absence of incineration plants for infectious waste. The lack of sterilization systems aggravates this issue. Furthermore, the authorized incineration plants are not adjacent to Piedmont, which leads to the need to make long journeys for quite significant distances, even to the order of 400 km.
From the users’ point of view, there is concern about the potential risk of new incinerator plants, the safety of operations, compliance with regulation, and the distances traveled to carry the waste. Furthermore, they expressed their satisfaction at being included in the ongoing investigation. They communicated their interest in being informed about what would happen to the final material after the treatment.
Once we identified the main concerns (or insights) of the users, we expressed the users’ needs as a requirement, considering the users’ thinking and feeling information and the ideas from improvement obtained from the Consumer Journey Map. In
Table 2, we establish the requirements for the conceptual design of the main treatment process.
3.3. Ideate
The requirements determine the function representing the intended relationship between inputs and outputs of a system or machine. The goal of the conceptual design ideate phase is to explore the concepts that may address customer needs. It includes a combination of external search employing benchmarking analysis, internal problem solving through brainstorming, and the exploration of solutions. As Pahl et al. [
18] indicate, we need a system with a clear and straightforward reproduced relationship between inputs and outputs to solve a technical issue.
To identify the initial relationships from the preliminary requirements established in the define phase, we began by analyzing the requirements related to consider other methods different from incineration and procedures compliant to region regulations.
Italian regulations allow two types of treatment management for infectious waste: incineration or sterilization. Since we want to explore other methods different from incineration, we refer to the active regulation of infectious waste management.
Concerning sterilization, the Italian Environment, Government, and Land Protection Department defines it as a physical (heat, ionizing radiation, microwaves) or chemical treatment that allows for a reduction of the microbial load to guarantee an S.A.L. (Sterility Assurance Level) not less than
, which is a 1 in 1,000,000 chance of a non-sterile unit. Sterilization must be carried out according to the UNI 10384/94 Standards employing a procedure that includes shredding and drying for non-recognition and greater effectiveness of the treatment and waste volume and weight reduction [
4].
3.3.1. Standard UNI 10384/94
Within the standards regarding waste management, there is the ISO 14,001 that describes a formal approach to handling waste, the CEN/TS 17,159 that guides the management and safety of high-risk materials and waste, and in Italy, particularly the UNI 10,384.
The UNI 10,384 standard: “Systems and processes for the sterilization of hospital waste,” which dates back to 1994, and is managed by the Ente Nazionale Italiano di Unificazione UNI (Italian national unification organization), provides the criteria for the design, operation, and verification of sterilization systems for infectious waste from public and private healthcare facilities. Furthermore, for treatment systems that involve thermal destruction and systems that use ionizing radiation.
Regarding the concept design requirements, the UNI 10,384, 1994 specifies that:
All the necessary precautions must be taken so that the loading operations in the sterilization system take place in conditions of safety for the operators and the environment.
The sterilization cycle must be carried out automatically according to a succession of phases.
The sterilization conditions, within established limits, must be uniformly achieved in the sterilization chamber, kept at the critical point for the pre-established time, and reproducible.
The sterilization chamber must be equipped with suitable closure or confinement systems. The sterilization cycle must not start until the closing system is closed, blocked, and, where necessary, sealed.
If a loading device is used, the waste must be cased without interference between the containment systems and the loading door.
The chamber must be equipped, in addition to the standard operating equipment, with those necessary for carrying out sample tests to detect the appropriate level of sterilization.
The materials used to build the chamber must resist chemical and physical aggressions deriving from the process and treatable waste.
The number and position of sensors inside the chamber must be specified.
3.3.2. Functional Decomposition
The next step for establishing the relationships in our conceptual design is decomposing the problem functionally, representing it as a single black box operating on material, energy, and signals, as suggested by Ulrich et al. [
47]. The next stage will divide the single black box into sub-functions to obtain a more detailed description of every element and their task oriented to achieve the entire system goal.
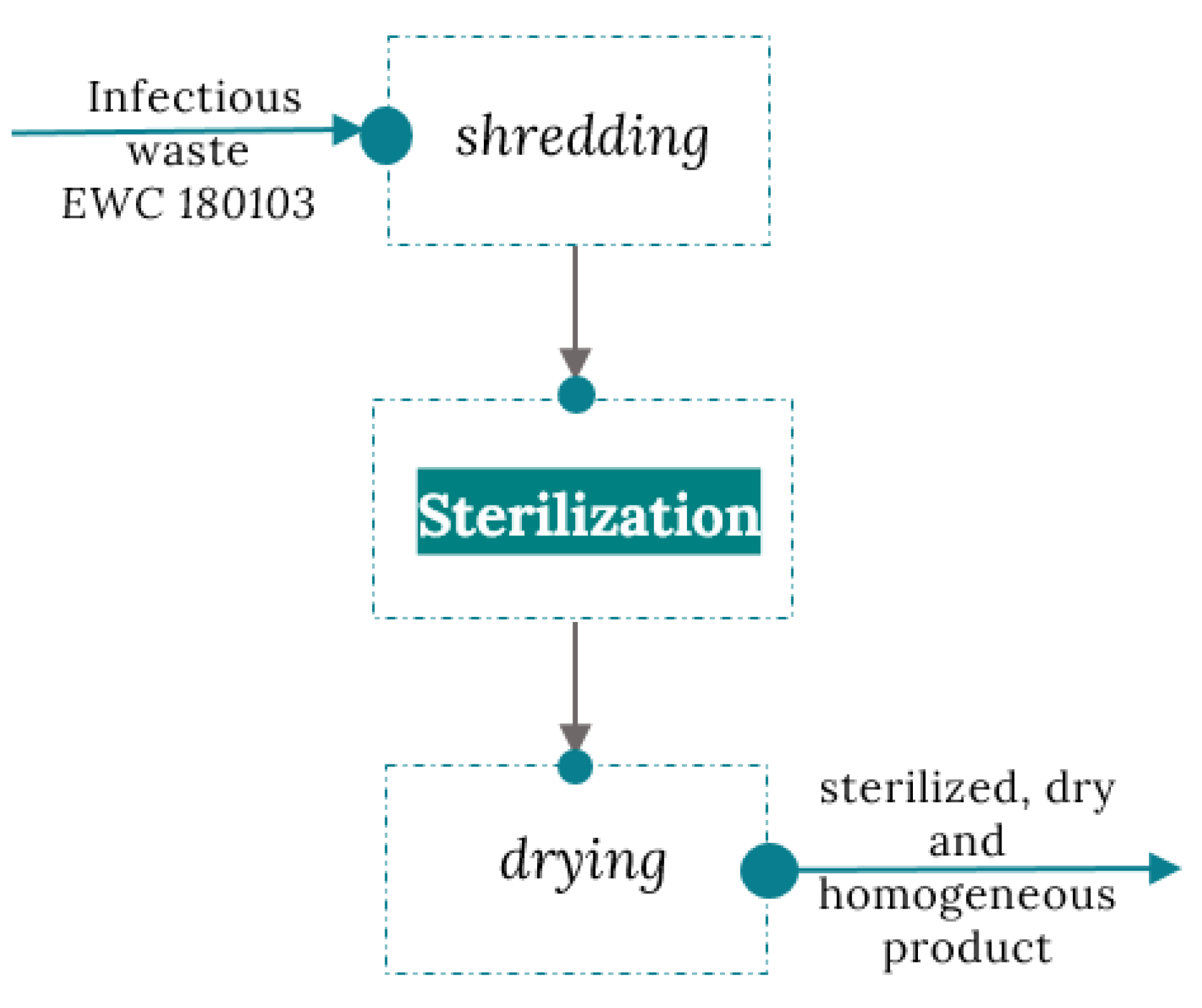
After selecting sterilization as a treatment method, considering the requirements and restrictions of regulations, we represented the first black box of our sterilization chamber in
Figure 6.
3.3.3. Treatment Methods Benchmark
In concept generation and as part of the DT ideate phase, it is beneficial to investigate current treatment methods used to solve the problem. Ulrich et al. [
47] define benchmarking as the exploration of existing processes with similar functionality like that of the system under study. In our case, benchmarking can reveal current concepts that have been implemented and information on the strengths and weaknesses of treatment methods. In this regard, we analyzed currently used sterilization methods and then investigated relevant concepts in Italy for the infectious waste treatment, different from incineration.
Sterilization Methods
Xiao and Hancock, and Lambert [
48,
49] define some of the most used methods for the disposal of infectious waste
Microwave sterilization: The method refers to the inactivation of infectious bacteria by the heat generated from the microwave vibration of the water molecules, achieving the disinfection of the objects. It is suitable for processing infectious and pathological waste (except human organs and infectious animal carcasses); it is not ideal for the treatment of pharmaceutical waste or chemical waste. In economic terms, it is not feasible due to high construction and operating costs.
Chemical disinfection: This method allows for the disinfection of waste with chemicals that eliminate bacteria and viruses. It uses dry and wet compounds that require the same treatment, and waste must be crushed and disinfected. The disadvantages of using wet chemicals are residual liquid, which can be an environmental pollutant, not suitable for all healthcare waste.
Pyrolysis: Pyrolysis is a thermochemical reaction technology. Suitable for all types of medical waste, but due to operation and maintenance requirements, this method is the most expensive. Furthermore, it is not easy to achieve stable combustion, producing exhaust gases and waste that can generate a secondary source of pollution.
Steam sterilization: This method applies high temperatures to generate steam that kills microorganisms and disinfects waste. The advantages of this technology are low installation and maintenance costs; it does not affect the environment and can be applied to all infectious waste.
Since we aim for a system that can also treat pathological waste (including human anatomical residues), microwave sterilization is not feasible. At the same time, chemical disinfection and pyrolysis can generate residual material (liquid and exhaust gases, respectively), which can be a pollutant by themselves. On the other hand, steam sterilization seems a feasible and secure treatment method suitable for our research.
According to Health Care Without Harm (HCWH) [
50], in the European Union some of best practices for infectious waste that use non-incineration technologies range from small units for use at or near the point of generation to high-capacity systems for large medical centers. The majority of non-incineration technologies used in the EU employ low-heat thermal processes and chemical processes. Low-heat thermal processes use thermal energy to decontaminate the waste at temperatures insufficient to cause a chemical breakdown or to support pyrolysis or combustion. In comparison, chemical processes employ disinfectants such as dissolved chlorine dioxide, sodium hypochlorite, peracetic acid, or dry inorganic chemicals. Some of these technologies include autoclaves in the Netherlands, steaming and drying in France, chemical treatment in Spain, steaming and compaction in Germany, as well as vacuum-steam and steam-fragmentation. Microwave treatment in Austria and in other countries such as Italy, France, Germany, Slovenia, Serbia, Slovakia, and Romania. Chemical processes are also used in Italy. Finally, electron beam technologies in Belgium and other countries.
Additionally, in the study “Assessment of Medical Waste Disposal Technologies Based on the AHP” [
51], a hierarchical structure model is used to analyze and evaluate five types of disposal technologies quantitatively for infectious waste in China. The classification weights of the optimal and suboptimal alternatives were studied using sensitivity analysis. The results show that the comprehensive benefits of high-temperature steam sterilization in infectious waste treatments are the best compared to the other methods in terms of social, environmental, technological, and economic factors. These overall results allowed us to define steam sterilization as the selected treatment for the main chamber.
3.3.4. Italian Concepts Initiatives
Next, we considered some relevant infectious waste sterilization initiatives in Italy. We looked for systems (including Italian patents) that have a well-established process. In Italy, we found three companies that include within their services the use of sterilization methods. However, we did not find evidence of the use or field implementation of these systems. The processes used are explained in
Table 3, according to the public information reported by the companies.
From the different available techniques of sterilization, and considering the initiatives reported in
Table 3, we can conclude that most of the systems differ from each other by the sterilization method, the shredding technology, the way of heating up the chamber, and the transportation from the shredding machine to the sterilization chamber.
3.3.5. Brainstorm for Ideation
Convergence is crucial in collaborative problem-solving and decision-making, as the team must focus its resources on the most promising ideas [
55].
Brainstorming allows the team to think on ideas to solve the problem and share the thoughts that arise. After analyzing different possibilities for the main chamber, we use the brainstorming technique to converge into preliminary ideas.
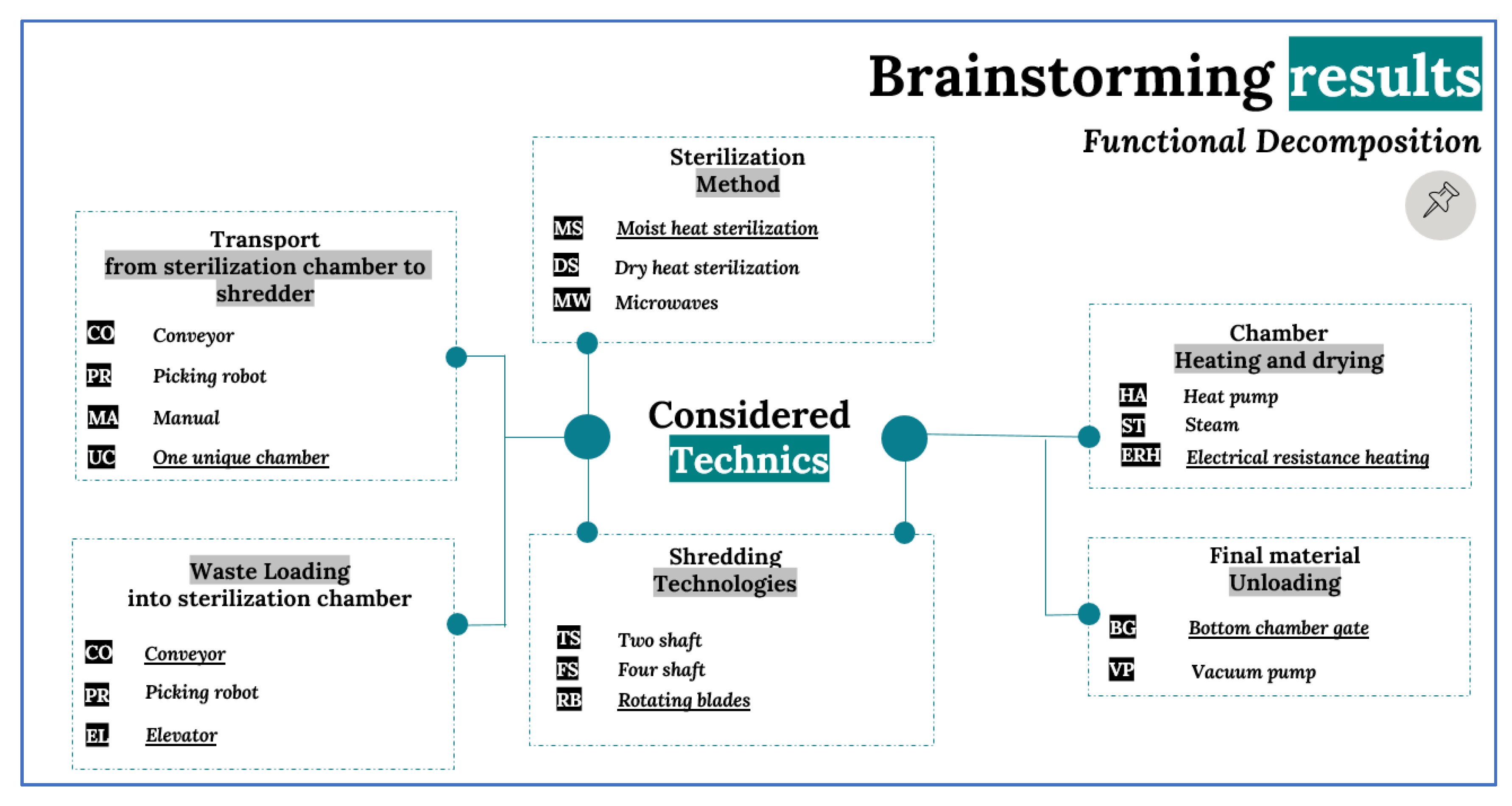
Figure 7 shows the most discussed methods in the technical brainstorming sessions. For each function, the solution selected is underlined. The selection was made considering the feasibility for construction and operation in Italy, success stories, cost, and originality for the Piedmont region.
We decided to use moist heat sterilization for the sterilization method because of its nontoxic characteristics, cycle time, cost, and safe operation [
56]. We have also noted that the systems analyzed in
Table 3 always transport infectious waste from the sterilization chamber to the shredder or vice versa, incurring more space, logistics, and risks. For that reason, we concluded that a suitable alternative could be the design of a single camera for sterilization and shredding, which will be explained in the next DT phase. Regarding the mechanism for heating and drying, we selected electrical resistance heating because of its efficiency and simplicity by converting nearly 100% of the energy in the electricity to heat. The shredding process will be carried out through rotating blades and counter blades at the bottom of the sterilization chamber. Finally, we decided to explore two options for waste loading, one using a conveyor and a second using an elevator. For the material unloading, we will use a gate at the bottom of the chamber to take advantage of the blades and the force of gravity. All the concepts will be further elaborated on and explained in the next section.
3.4. Prototype: A Conceptual Design
The prototype phase in DT aims to concretize the idea by creating an approximation of the product, reflecting on its features and eventual improvements.
Ulrich et al. [
47] define the prototype as an approximation of the product along one or more dimensions of interest. Any entity presenting at least one aspect of the product of interest can be viewed as a prototype. Virtual prototypes can be represented using drawings, mathematical models, simulations, and CAD models.
In our study, we intend to create a design prototype according to the definition given by Polydoras et al. [
33]. Prototypes can be classified according to their ability to serve the distinct stages of the design process; a design prototype mostly represents the form and functional relations of the product. A design prototype allows designers to evaluate various aspects of their ideas before committing to the expense and risks of producing a commercial quantity [
33,
57].
With this aim, according to the previous phases’ results, we focused on the conceptual design. To achieve this goal, we defined the process and its functional interactions and the sterilization cycle, and then propose two CAD concepts.
3.4.1. Process and Functional Interactions
The treatment system aims to transform infectious waste into a dry and homogeneous product with no recognizable parts, which is stable over time. The final product could be stored for long periods before its disposal and recovery. The designed process aims to obtain a fine shredding of the waste, the pulverization of glass parts, and the total elimination of liquids, contributing to the reduction of weight and volume.
This system is based on the moist heat sterilization method. It works under the same conditions as steam autoclaves. The combination of time, temperature, and humidity is achieved in a closed environment under vacuum conditions. However, this process peculiarity consists in treating the waste to a temperature up to 151 °C with the presence of humidity and liquid water, operating under vacuum conditions, without diffused pressure as in autoclaves.
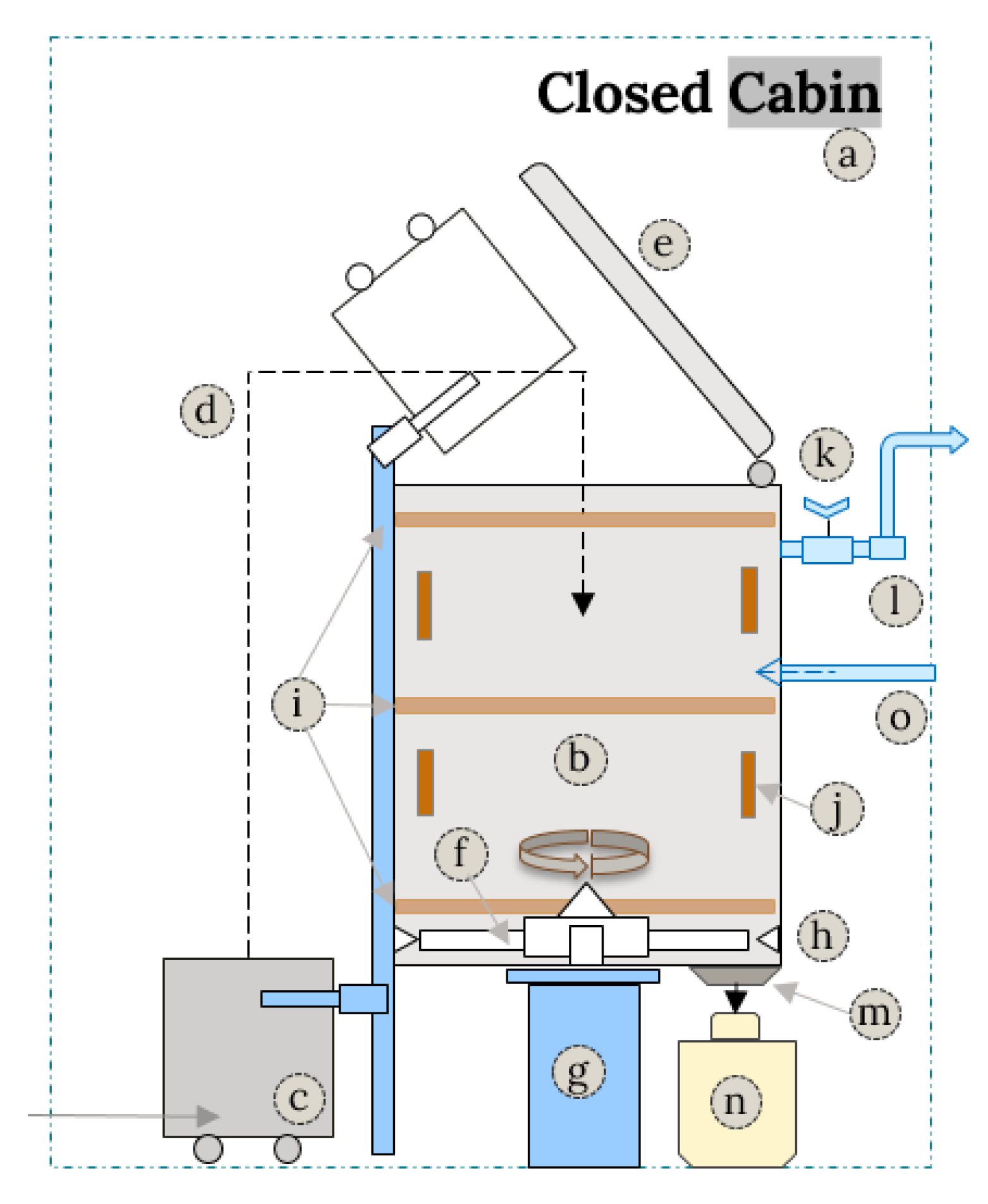
The system (
Figure 8) consists of a closed cabin (a) with all the devices inside it, the sterilization chamber (b) performs automatically thermal cycles that include shredding and evaporation of liquids, overheating up to 151 °C, sterilization at 151 °C, through continuous dosing of water transformed into steam because of the operative conditions, and for an adequate time to ensure microbial elimination. The process ends with a cooling phase and the discharge/unloading of the dehydrated final material.
The waste is introduced to the system using apposite containers (c). An automatic loader (d) deposits the waste inside the sterilization chamber (b) after the lid (e) has been automatically opened.
The sterilization chamber (b) structure is a vertical cylinder in AISI 306 stainless steel, equipped with a sealed lid (e) made in high-temperature resistant silicone rubber gasket and hydraulic locking systems. All the phases of the sterilization treatment, including loading and unloading, occur automatically inside the cabin (a) without moving the waste outside the chamber until the process end.
In the lower part of the chamber, there is a two-blade Hardox 500 stainless steel rotor (f) driven by an electric motor (g). The blades act like hammers; stationary blades (h) are mounted in correspondence inside the chamber to ensure the necessary contact and, therefore, the material crushing. This friction produces an additional source of heat, valuable for our operation.
In the high, middle, and lower sections and around the perimeter, there are electrical resistances (i) that heat further the chamber (b) in a controlled way. Across the entire chamber height (b), there are ten thermocouples (j) installed for measuring the material temperature, six at the bottom chamber along the perimeter, and four more at the middle and upper section.
The chamber is connected to a throttle valve (k) for vacuum control and then to a vacuum pump (l). At the end of the treatment, the unloading gate (m) automatically opens, and the product is discharged by centrifugal force into apposite bags (n).
The system is kept in slight depression during the entire treatment cycle using a throttle valve (k) and the vacuum pump (l). Considering the variable composition of the incoming waste in terms of typology, and therefore in terms of intrinsic moisture, the system includes a valve (o) for pouring the necessary water into the chamber to reach and guarantee the sterilization conditions.
After the waste is loaded, the chamber lid closes automatically, and the rotor at the bottom starts spinning at a low speed. The waste is shredded while the rotor speed progressively increases up to about 1000 rpm. The mass heats up, thanks to the thermal energy generated by the rotation and friction of the blades. This operation leads to the release of intrinsic moisture from the waste. In this way, the temperature gradually increases until it reaches the value of 151 °C. Extra water can be added in this phase if the intrinsic moisture of the waste would not be sufficient to reach the required sterilization conditions. Compared to the traditional moist heat sterilization process used in autoclaves, this process does not operate with saturated steam but with unsaturated steam on a finely shredded material, operating at higher temperatures but with significantly lower pressures.
3.4.2. Sterilization Cycle
According to the previous description, the sterilization cycle follows a sequence of seven steps:
Phase 1: Waste loading: The waste is loaded into the sterilization chamber using an automatic loader, then the lid is automatically closed at the end of loading.
Phase 2: Shredding and Heating: After closing the lid, the rotor begins to rotate until the material is pulverized and the temperature reaches 100 °C. The blade’s profile should be designed to create turbulence on the bottom of the chamber, facilitating the mixing and avoiding depositions on the walls.
Phase 3: Evaporation and overheating: The heat generated by the friction of the material should cause the vaporization of the humidity contained in the waste, and the temperature should remain stable at 100 °C. Humidity and temperature are constantly measured using a probe designed for test chambers at high temperatures.
Phase 4: Overheating: Once all moisture has been removed, the generated heat raises the temperature of the material to 151 °C. Extra water can be added if the waste’s intrinsic moisture is not enough to reach the sterilization conditions.
Phase 5: Sterilization: The material temperature is maintained at 151 °C through water dosage and controlled by the thermocouples. When coming into contact with the material, the water evaporates and becomes steam. The water dosage is controlled so that the heat absorbed by the water evaporation balances the heat produced by the material friction. Additionally, there is extra heat coming from the chamber walls using the electrical resistances. This allows keeping the material moist at a high temperature. The whole chamber must be kept at 151 °C for at least 3 min during each operating cycle to ensure the correct functioning of the sterilization system.
Phase 6: Cooling and drying: The rotor speed decreases and consequently so does the heat generation. If needed, water is sprayed, lowering the temperature to 100 °C. Then, through a vacuum pump, the temperature drops adiabatically until room temperature is reached. During this phase, the heat absorbed by water evaporation exceeds the heat generated by the rotor; therefore, the temperature drops.
Step 7: Unloading: The treated material is discharged by centrifugal force through the discharge gate located at the bottom chamber. Once the material has been completely discharged, the rotor stops.
3.4.3. Computer-Aided Design (CAD)
During the DT prototype phase, CAD provides a visual manifestation of concepts and supports the generated ideas’ transformation into feasible and testable models [
58]. CAD concepts can be quickly created and experienced. It can support team communication by facilitating conversations and feedback regarding solutions for a particular product [
34].
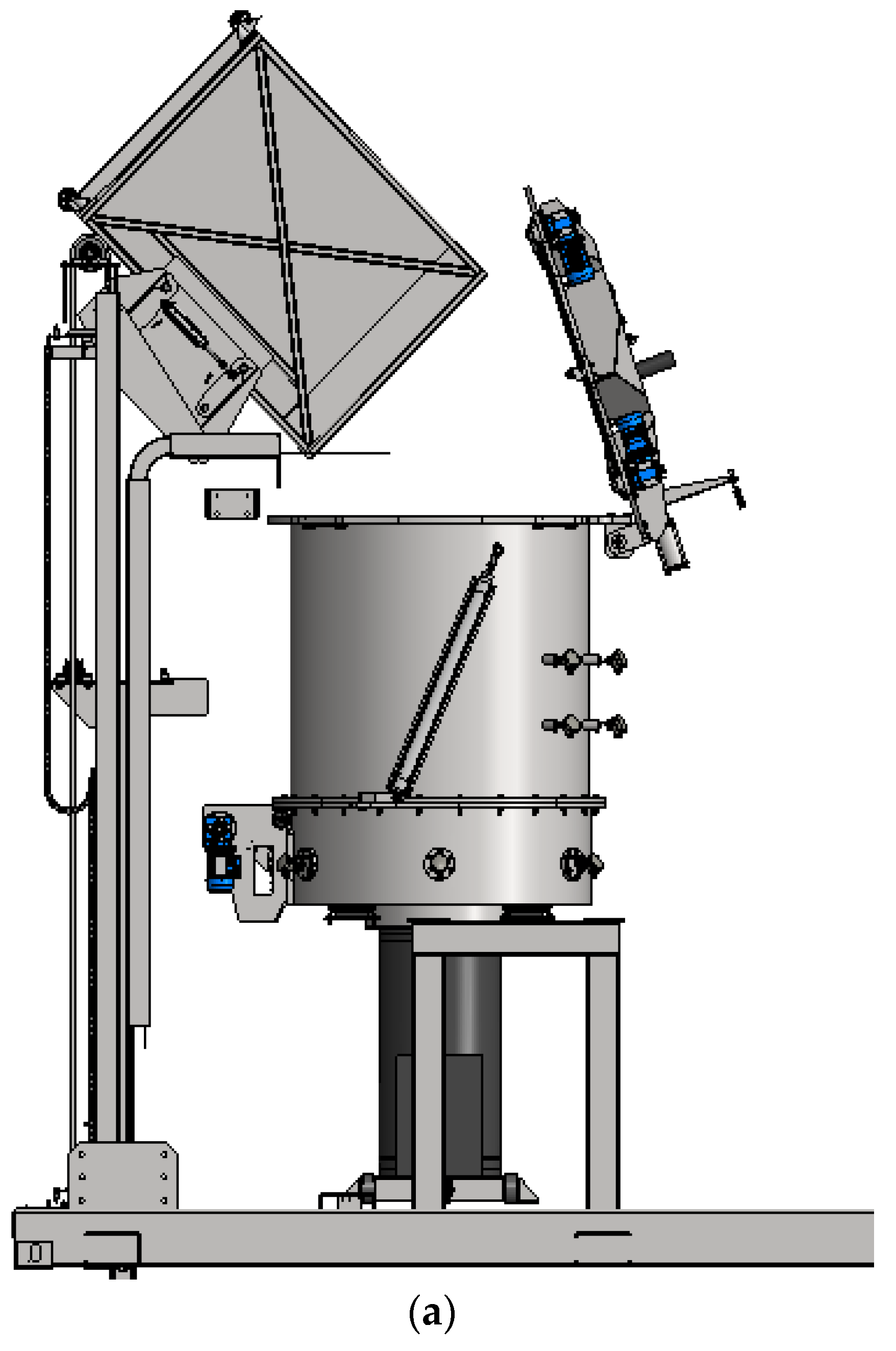
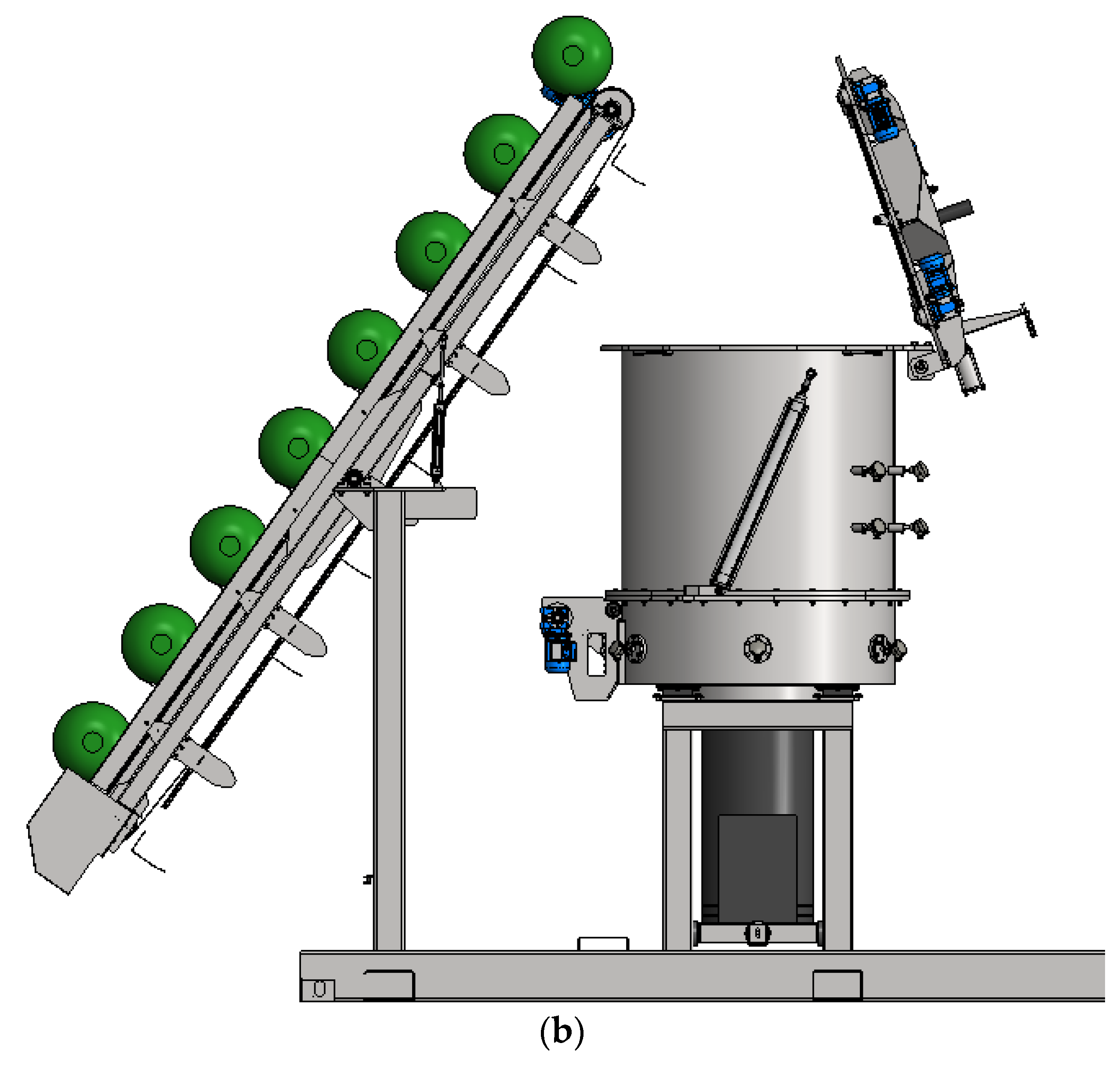
According to the process and functional interactions, we propose a virtual prototype, represented by two concepts using CAD. Due to the importance of the internal process of the chamber, it remains invariable for both concepts. The main differences between them are related to the uploading transportation system.
The first proposed concept (
Figure 9a) consists of a stainless steel trolley to carry all the waste and an automatic uploading system that raises and overturns the loading trolley, allowing the material deposition directly inside the chamber.
The second concept (
Figure 9b) consists of a conveyor belt system for loading waste containers. The conveyor system transports the containers automatically up to the open lid. Then, from a closer distance to the lid, the containers automatically open one by one, depositing the waste inside the chamber.
For both concepts, the operations inside the sterilization chamber are the same as reported in the process and functional interaction section.
3.5. Test: Concept Evaluation
The fifth and final phase of DT corresponds to the test. According to Bresciani [
59], visual representations can guide the designer’s work within a design framework. They allow for bringing together academic knowledge and the practice of design, providing a visual reference for users and stakeholders, in this way, they can support the design process.
This section evaluates the virtual prototype (represented by concept models a and b) according to the user’s requirements, then collects feedback for further improvements. The test phase results were obtained during focus group meetings that included the development team, experts, users, and other stakeholders. For the test phase we have used the concepts designed in the previous section, represented by their CAD models (
Figure 9).
We use the concept scoring technic (
Table 4) proposed by Ulrich et al. [
38] to evaluate the concepts. It uses a weighted selection model to evaluate the concepts variants against the requirements and other criteria deemed relevant by the team. The selection criteria were determined according to the user’s expectations and the Italian regulations described in the previous phases. For every criterion, the team analyzed and agreed on the weight assigned, considering that in this phase we are performing a feasibility analysis for a conceptual design. The same consideration was used for rating the concepts. They were evaluated on a scale of 1 to 5, five being the best and one the worst.
Both concepts used a method different from incineration and were designed to include the users’ perspectives. At the beginning of our exploration, stakeholders specified these requirements; both systems are consistent with them, so these parameters are not included in the evaluation.
It is possible to determine the concept ranking using a weighted sum of ratings. After analyzing both concepts, the results show that concept 1 is more promising than concept 2, with a score of 4.0 against 3.3.
Concept 2 has some downsides due to the loading system that could generate unwanted losses in the environment when opening each of the compartments to deposit the waste inside the chamber. Additionally, concept 2 requires more handling by the operators as they have to locate different compartments on the conveyor. The same happens during cleaning, which should be done one container at a time. On the other hand, concept 1 has a single active trolley, controlled, and transported by the elevator, that later deposits all the waste material inside the chamber, all in a single step, allowing for faster loading times with fewer risks. In this context, we decided to go ahead with concept 1.
After the concept scoring analysis, however, new suggestions for improvement were proposed. The first is the need to add an extractor hood that absorbs any unwanted material escaping from above the chamber. The second is related to vapor and liquid management during the shredding and sterilization process; all the water due to humidity is evaporated. The vapor leaves the chamber through a duct and then is extracted by the vacuum pump. After that, we will include a scrubber for the condensation of water vapor, the absorption of entrained vapors, and dust removal. Finally, regulations request that we have a system for carrying out quick tests.
4. Results
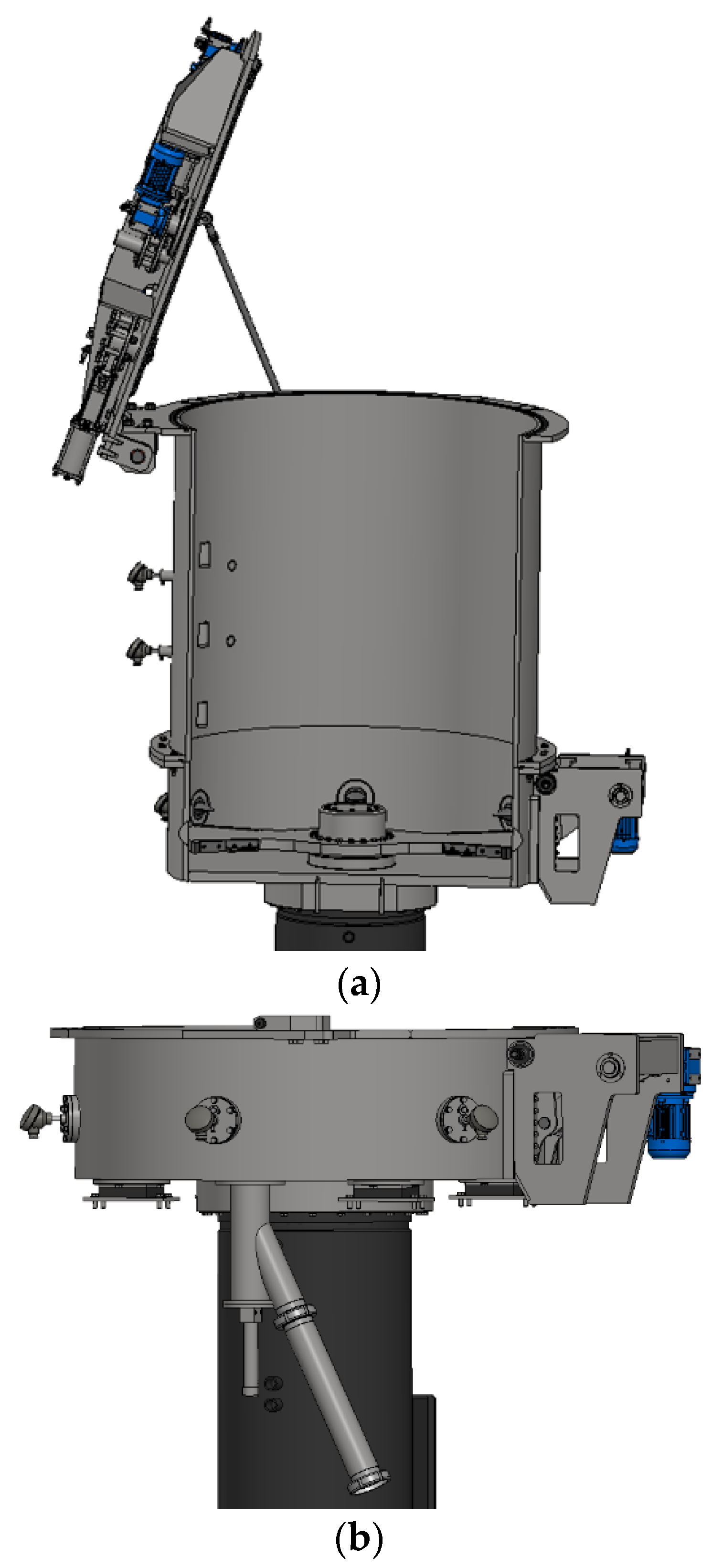
After performing the five phases of DT, we got a final and preliminary concept of the main treatment chamber for an infectious waste management system in Piedmont, Italy. This conceptual design responds to the expectations of the users and is compliant with regulations. When the test phase concluded, some relevant suggestions emerged, leading to the final conceptual design of this study (
Figure 10 and
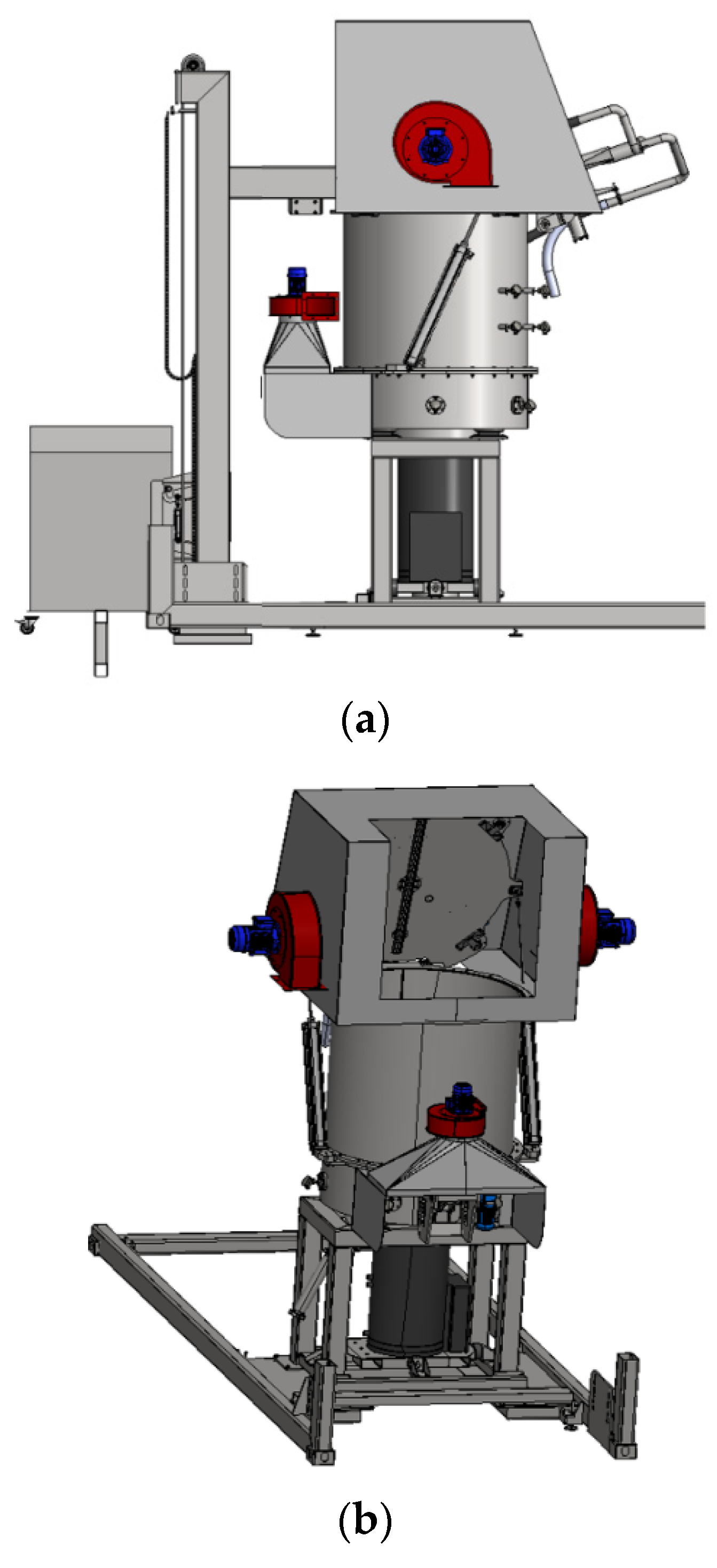
Figure 11). It includes an extractor hood to eliminate any possibility of unwanted material dispersion inside the closed chamber and a sampling device for carrying out the test and sampling extraction under contained conditions. For future steps in the general project design, it is planned to add a scrubber for pollutant control and removal. Our concept design is, therefore, delimitated until the phase before the management of liquids and vapors.
Figure 10a shows the entire automatic chamber system with the extractor hood.
Figure 10b shows the rearview and allows us to visualize the space where the trolley will enter to discharge the waste material into the chamber.
A section view of the chamber is represented in
Figure 11a; the rotor blades are in the lower part, along with the counter blades. It is possible to visualize two of the ten thermocouples and the automatic lid.
Figure 11b, shows the safety extraction valve for the sampling withdrawal test, located in the bottom of the sterilization chamber. This valve will allow for the extraction of a sample of final material after the treatment to evaluate its efficacy.
DT seeks to define solutions where three aspects converge: desirability for the end-user, feasibility, and financial viability. DT brings together what is desirable from the point of view of the users and stakeholders with what is technologically feasible and economically viable [
35]. To validate the desirability, we spoke with stakeholders and potential users during the empathize phase to understand their concerns and desires; we have summarized these thoughts, commonly referred to as “pains and gains”, in
Figure 4. In turn, the feasibility involved designing (during the prototype stage) two virtual prototypes of the solution, evaluated later by experts, stakeholders, and users during the test phase. Creating a virtual design prototype enhances the financial viability since the production costs of a functional prototype are very high. In this way, creating a conceptual design minimizes the economic risk by being able to improve the design without incurring the costs that would entail modifying a physical prototype.
This section concludes the conceptual design of the main sterilization chamber. For futures studies, the idea of including handling robots to perform the trolley loading operations could be further analyzed; this would eliminate the workers’ handling completely, and this way, they would be in charge only of activation of the automatic cycle and operations control.
Finally, another potential future study regards the use of treated waste, since according to Italian regulation [
4], the sterilized infectious waste can be used as a means of producing energy adopting the EWC 191210.
5. Discussion and Conclusions
Innovation and new technologies development are essential for most cities that aim to foster an ecofriendly environment. Potential smart cities request more recent systems in shorter time intervals, often customized to their own needs. Companies and research centers have to collaborate closely within their organization and with partners located in various parts of the world to meet these needs. At the same time, companies have to manage increasing technology and manufacturing complexities due to a quickly growing number of environmental and regulatory rules and requirements. Using collaborative tools and strategies, such as DT, for managing product data and integrating and automating business processes generally results in efficiency improvements. In particular, the knowledge in this domain can be applied to the context of eco-sustainable equipment and strategies, working together with users and stakeholders.
This project explored the application of the DT methodology in engineering and sustainability. Its application in technical areas allowed us to explore the methodology and apply it concretely.
The DT approach as methodology allowed the team to work under an established framework, following a series of phases and tools. Design thinking guided the conceptual design, beginning from a general idea to finally be able to produce a CAD prototype. The first phases (empathize and define) allowed us to understand the stakeholder’s perspective and context and include their suggestions in the development of the study. The personas technique and Customer Journey Map were tools that engaged not only with the users but also with the team members, gathering the stakeholder’s points of view effectively.
The ideate phase was essential to transform these ideas into visual models. The functional decomposition acted as a conductor to understand and solve, step-by-step, each subproblem of the entire system, understanding their interactions and relations. The brainstorming particularly helped the team to converge on solutions considering all the opinions.
The prototype phase, including brainstorming and CAD tools, concretized the idea into a conceptual design represented by two virtual concepts. By following the DT directions, these concepts were designed based on the users’ needs and the current Piedmont region regulations. Users expected a safe and standard process capable of treating waste quickly, a procedure compliant to regulations different from incineration, minimum handling, and shorter distances journeys while transporting waste.
In this way, the study problem is framed and oriented according to the requirements. Many other concepts could be generated using this DT framework. Still, we decided to focalize our efforts on creating a feasible concept, especially in the design of the sterilization chamber. Due to the cruciality of this operation inside the system, we prefer to be cautious in selecting the technique resulting from the brainstorming session.
In the last DT phase, we analyzed and compared the two concepts using the concept scoring method. We established selection criteria according to the stakeholders’ requirements, users and regulations on this matter. We then assigned the weights for each criterion and concept according to the team expertise; it does not mean that the weights are ideal or unique, but that they are certainly a reasonable approximation inside a feasible exploration of concepts. Concluding the test phase, we asked experts for feedback to improve the final concept.
The feedback gave us suggestions on how to improve the concept and insights for the future steps of the project. Our concept “delimits” with the vapor and liquids management system; therefore, for subsequent studies, we propose a scrubber to perform the operations of pollutant control. Also, there is evidence of the potential use of the treated material as RDF. In this regard, for future steps, it could be interesting to consider a pelletizer after sterilization for compressing and molding the final material for later storage. In this way the current paradigm that uses incineration as the primary treatment process within a linear economy approach, will change to a new scenario, using sterilization and a compression process to generate RDF that could be re-integrated into the production cycle within a circular economy approach.
In comparison with other existing facilities, the main improvements of this design are at a local level, the increase in the production and development of our own technologies for the management of infectious waste, looking for new treatment and energy recovery processes. Specifically, in Italy, one of the main improvements in comparison with existing facilities is the use and management of technologies different from the current waste incineration paradigm. Then, an industrial process that guarantees perfect sterilization of the treated waste to obtain a product intended for energy enhancement, through a new completely automatic and locked process for the treatment of infectious waste through shredding and sterilization. The whole process takes place automatically and is isolated inside the main chamber, minimizing the risks for the workers. In addition, it is expected to treat the sterilized waste further to generate derived fuel and enhance the final product. Moreover, this process operates with unsaturated steam on a finely shredded material, operating at higher temperatures but with significantly lower pressures.
Finally, this investigation is a positive example of how to apply the DT methodology as a framework for new technological designs. With the application of the DT during the development of this study, it was possible to analyze the process holistically, considering the perspectives of the technological and social environment and the opinions of experts from the industrial sector, users, and stakeholders, in order to develop a technologically-based conceptual design, obtaining satisfactory results for the parties interested in this project.
At a social level, the approach of the DT method helped users feel part of the development of a technology which usually is rejected. This study provides a successful case of the application of DT in a sector where few studies have been carried out, leading to an increase in interest and opening possibilities for future research. Additionally, it provides a framework and a demonstration of applied tools for future research that intend to apply DT for similar processes.
Through this research, we found improvement opportunities for infectious waste management in the Piedmont region in Italy. To solve the problem, DT includes the users’ needs and involves the community, which is an essential aspect of sustainable developments for eco-friendly cities. The concept result of this study is framed within a feasibility analysis; therefore, it is not definitive. As part of the project, a functional preproduction version of the chamber must be manufactured to verify its performance. This study supports the continuation of the subsequent development phases of the entire system represented in
Figure 1.
We expect that this article could be used as a reference for future investigations related to the application of Design Thinking in engineering designs oriented to sustainability, resource efficiency, and waste management.


 ,
, 
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}