Abstract
In this work, we present VaccineHero, an extended reality system that aims to reduce children’s discomfort during vaccination. In our proposal, the child wears a headset during vaccination and watches a VR short story. The story includes a hero touching the child’s arm, and the doctor synchronises the insertion of the needle with the VR content so that the child is efficiently distracted. A clinical trial has been carried out involving two doctors and a cohort of 16 children, which showed that the use of VaccineHero reduces children’s discomfort during vaccination by a staggering 40% and completely eliminates extreme discomfort. The implemented solution is extremely affordable, as it can be deployed on simple headsets or even Cardboard devices, a feature that makes it a realistic option for any paediatric practice. It can also be extended to support other medical activities that involve needles, such as blood drawing and blood donation.
1. Introduction
Vaccination is one of medical science’s greatest achievements [1]. Nationwide vaccination programs for children, specifically, constitute one of the most successful public health policies in human history, leading to the eradication or control of several terrible diseases in the past [2]. Yet, not everyone is eager or even willing to have themselves and their children vaccinated. In fact, as recently as 2019, the World Health Organization identified vaccination hesitance as one of the 10 greatest threats to global health [3].
Vaccination hesitance can have many different root causes, with trypanophobia (the fear of needles) and the overall discomfort experienced during the vaccination procedure among the leading ones [4]. With this fear being a lot more common in toddlers [5], it is only natural that children experience high levels of discomfort during procedures that include needles, including vaccinations [6]. Paediatricians from the American Academy of Pediatrics found that 75% of parents sought to delay vaccination due to concerns about their child’s discomfort [7], with approximately 45% of children aged 4–6 years showing serious distress during vaccination [8]. Moreover, 10% of the population completely avoids vaccinations due to a fear of needles [9].
In this work, we aim to limit and, if possible, completely alleviate the discomfort experienced by children during the vaccination procedure. Other researchers have already established that the pain and fear children experience during immunisation can be affected by external factors, such as parents’ behaviour [10,11], breastfeeding (for younger children) [12,13,14], being distracted [15], receiving a massage [16], different body positions [17], sweeteners [18,19], and so on.
Herein, in addressing this problem, we present an extended reality (XR) application called VaccineHero. This application aims to enhance the childhood vaccination process by significantly reducing, if not entirely eliminating, the distress and negative emotions typically associated with it. VaccineHero captivates young users with a 90 s narrative, timed to coincide with the duration of a typical vaccination. Within this immersive virtual world, toddlers take on the role of VaccineHero, an avatar navigating through an adventurous environment that seamlessly merges elements of both virtual and physical reality. The application serves a dual purpose, providing an engaging distraction for the child while also acting as a practical aid for healthcare professionals, ensuring a more streamlined and less distressing vaccination process.
The remainder of this article is organised as follows. We review the relevant state of the art in Section 2, and in Section 3, we present our proposal in detail, including a use-case scenario, the architecture of the system, and some interesting details regarding its implementation. Section 4 details the evaluation of the system, including clinical trials of VaccineHero and an analysis of the gathered data. Finally, in Section 5, we present our concluding remarks and suggest directions for further research.
2. Relevant Literature
The times when medicine was a siloed science are long gone. For more than a century now, medicine has been progressing hand in hand with technology [20] and reaping the benefits of advancements in other fields. Quite often, technological breakthroughs have been followed by related medical breakthroughs or even by the creation of new medical domains.
Advances in electromagnetic radiation led to the development of medical imaging [21]. Advances in mobile technology introduced us to telemedicine [22]. Advances in machine learning gave birth to clinical decision-support systems [23]. And of course, the current advances in artificial intelligence, as seen in tools such as ChatGPT, are expected to again revolutionise healthcare [24].
Similarly, advances in VR technology are impacting various areas of the medical field [25,26,27]. The dominant medical application of VR technology is in education [28,29,30], primarily for the training of surgeons [31,32]. But that is not the only application domain. For example, in rehabilitation, VR can help children with cerebral palsy regain their walking abilities [33], or assist stroke patients in regaining control of their arm movements [34]. For older adults in nursing homes, VR can assist in memory training [35], and burn victims’ acute pain during treatment can be reduced via the use of suitable VR applications [36].
In this work, we focus specifically on the use of VR to assist in children’s vaccinations. This is not a fundamentally new concept. For example, in 2018, in Saudi Arabia, the Ministry of Health launched a VR initiative to help children overcome a fear of immunisation and blood drawing [37]. But, to the best of our knowledge, no data have been published regarding either the specifics of the plan or the effectiveness of the implementation. Similarly, in 2018, the Ogilvy company in Brazil announced the development of a VR solution to support children’s vaccinations [38]. But, there is no indication of the tool ever reaching the market or of its actual effectiveness.
A more recent work that used VR to help with children’s vaccinations and actually reported on the achieved results was published in 2022 [39]. This work is fundamentally different from our approach in the sense that it uses VR as a mood-setting tool before the vaccination and not as an experience that is concurrent with the actual vaccination. More importantly, the authors examined the experience solely from the point of view of medical professionals, considering only the opinions of nurses and not assessing how children actually experienced the vaccination process.
Thus, our study of the relevant literature identifies a clear research gap and unanswered research questions: Can VR be used to enhance the vaccination procedure, as experienced by children? And, if yes, how? We address these questions in the following sections.
3. The VaccineHero System
3.1. Concept and Use Case Scenario
Research has shown that distraction is a very effective way to mitigate both fear and pain associated with vaccination in children [40]. With VaccineHero, we build on this notion and design a system and vaccination procedure that aims to keep the child distracted throughout the vaccination process.
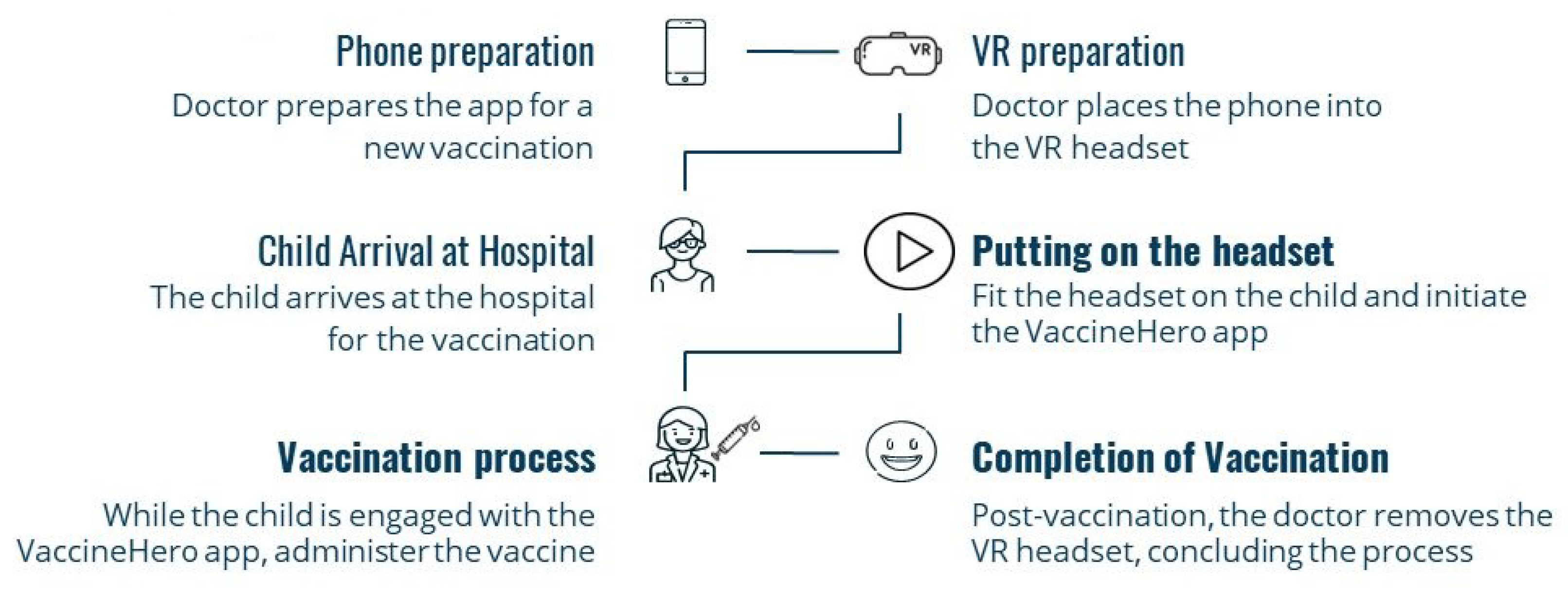
More specifically, in our proposal, vaccination follows the flow shown in Figure 1. During office setup, the VaccineHero app is loaded onto an Android phone, and the phone is placed in a headset. The headset is of a smaller size so it is suitable for children. Offices that receive children of different ages may have multiple headsets of different sizes ready to use.
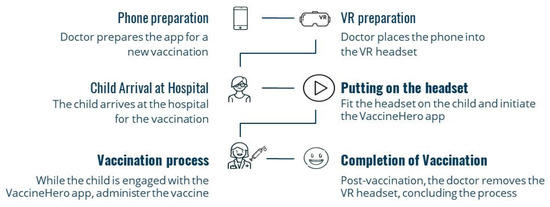
Figure 1.
The vaccination process using VaccineHero. Bold typeface indicates the stages for which the child is present, whereas normal typeface corresponds to preparatory actions before the child’s arrival.
Upon arrival at the clinic or doctor’s office, a child is fitted with a VR headset so that no time is spent contemplating the vaccination procedure and starting to worry. The VR content starts to play, and the child assumes the role of the hero and enjoys an immersive experience in which a 3D world is explored and a magician is encountered.
At this point, we should underline that the doctor is not required to provide an introduction to the VR content but can instead focus on discussing with the parents and examining the child, as they would normally do in any vaccination, even without VaccineHero. This is because an important user requirement in the design of the use case was that the use of the VaccineHero system should introduce the minimum possible overhead for medical personnel. Therefore, the VR content is simple and self-explanatory, meaning that the child can watch it without the need for introductory explanations.
During the immersive experience, the magician twice touches the left arm of the hero. The doctor touches the left arm of the child at the same time, blurring the boundaries between the virtual and physical worlds; hence, the characterisation of our solution is extended rather than virtual reality.
The first time the doctor touches the arm of the child, it is to clean the vaccination area with cotton and alcohol. The second touch is with the needle to deliver the vaccine. Thus, the vaccination is completed seamlessly with the VR content, and the child remains unaware, calm, and free of pain.
Following the completion of the vaccination, the VR story soon concludes, the doctor removes the headset, and the child is free to go, having been both vaccinated and entertained!
3.2. System Architecture
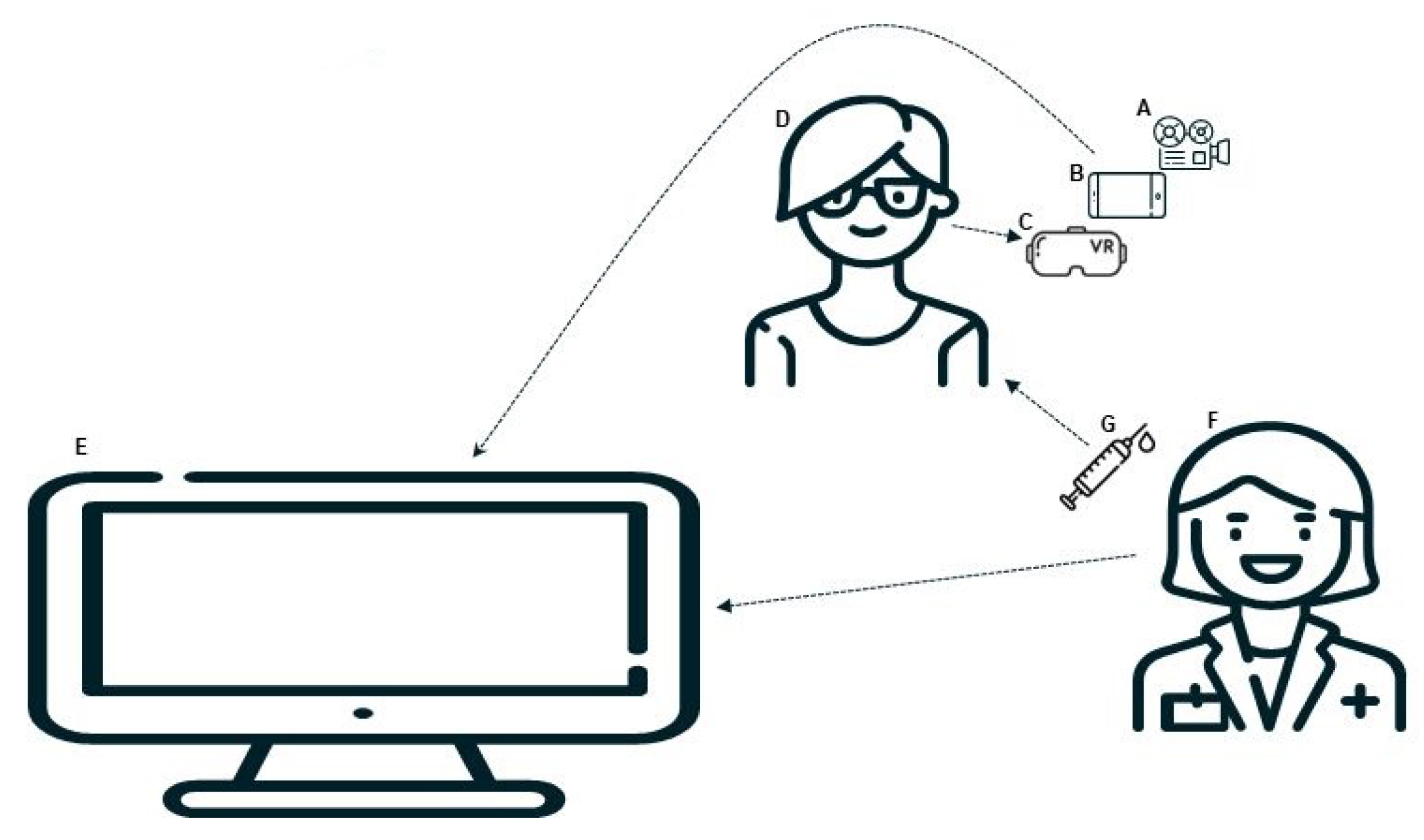
The architecture of the proposed approach is summarised in Figure 2. The core of the VaccineHero solution is a 90-s immersive, three-dimensional experience (A in the figure), including a complete 3D world, as seen from the point of view of an inanimate hero sitting in the centre of the scene, a magician avatar that interacts with the hero, and the accompanying stereophonic sound that completes and enhances the immersion.
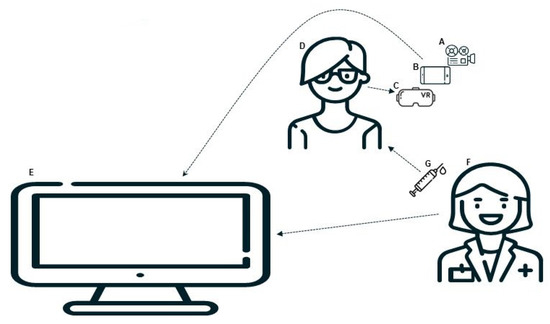
Figure 2.
System architecture.
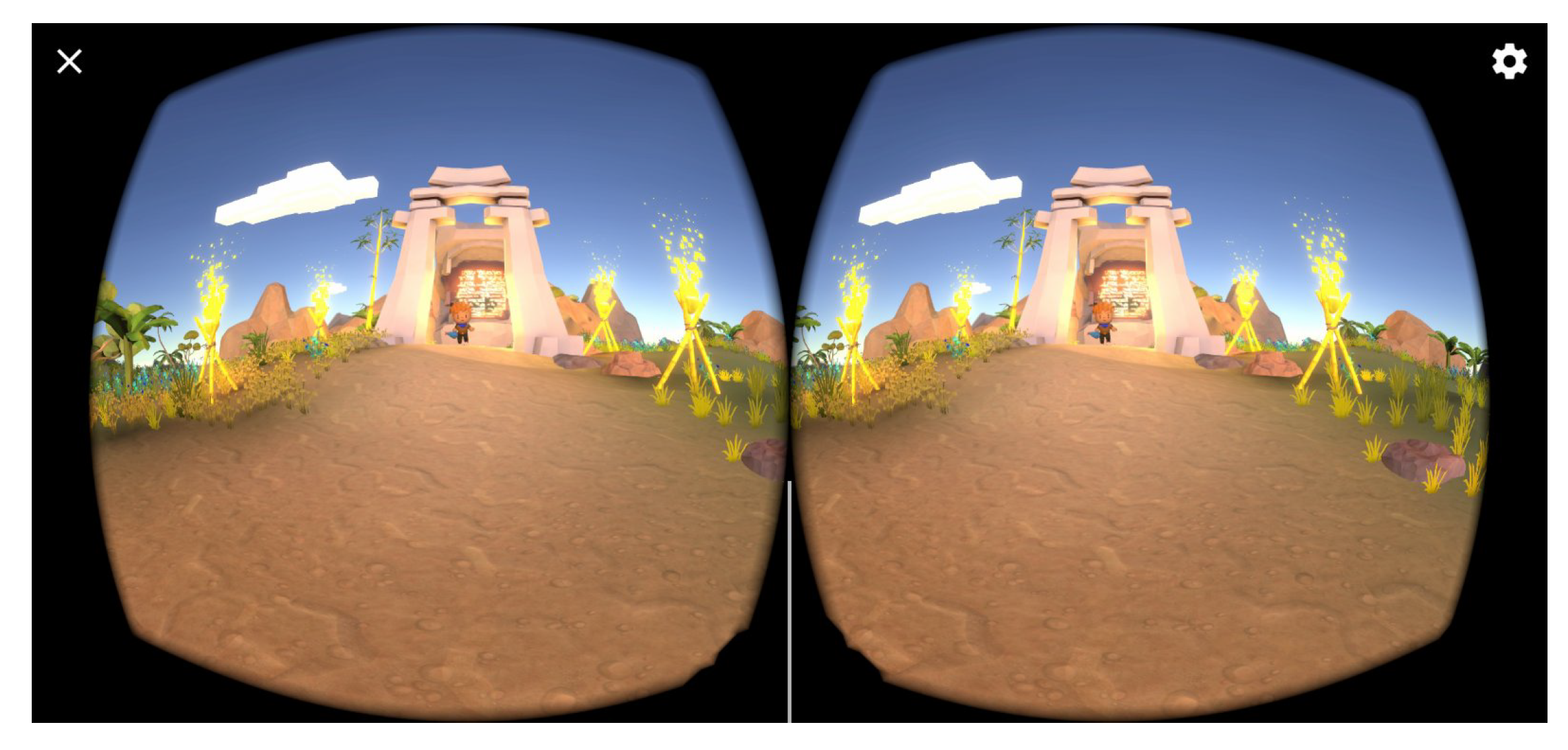
The VR application is loaded onto an Android phone (B) and is set up to project to a headset. In this setup, as shown in Figure 3, the phone’s monitor is divided into two parts, each one displaying the scene as would be seen from the left or right eye, respectively. The minor differences between the two displays, when each one is seen by the left and the right eye, trick the brain into sensing depth where there is none, thus creating a 3D experience.
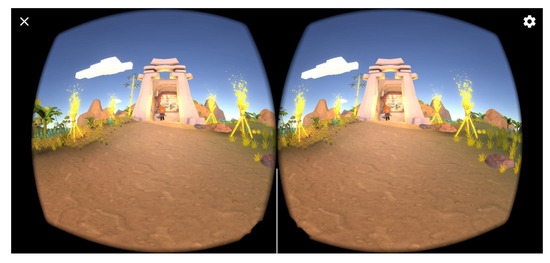
Figure 3.
VR content configured for projection through a headset.
The phone is placed in a headset device (C) that can be fitted on the child patient (D). The headset aligns the two displays with the eyes and forces the viewing of the content in the proper way for the three-dimensional feeling to be stimulated. The child is also fitted with earbuds through which the content’s audio is delivered.
The 3D content that is displayed on the screen on the phone is simultaneously displayed on an external monitor (E) using Miracast [41]. This allows the doctor (F) to observe the progression of the VR story and perfectly time the delivery of the vaccination (G) so that it coincides with the moments in the video when the magician touches the hero’s arm.
3.3. Implementation Considerations
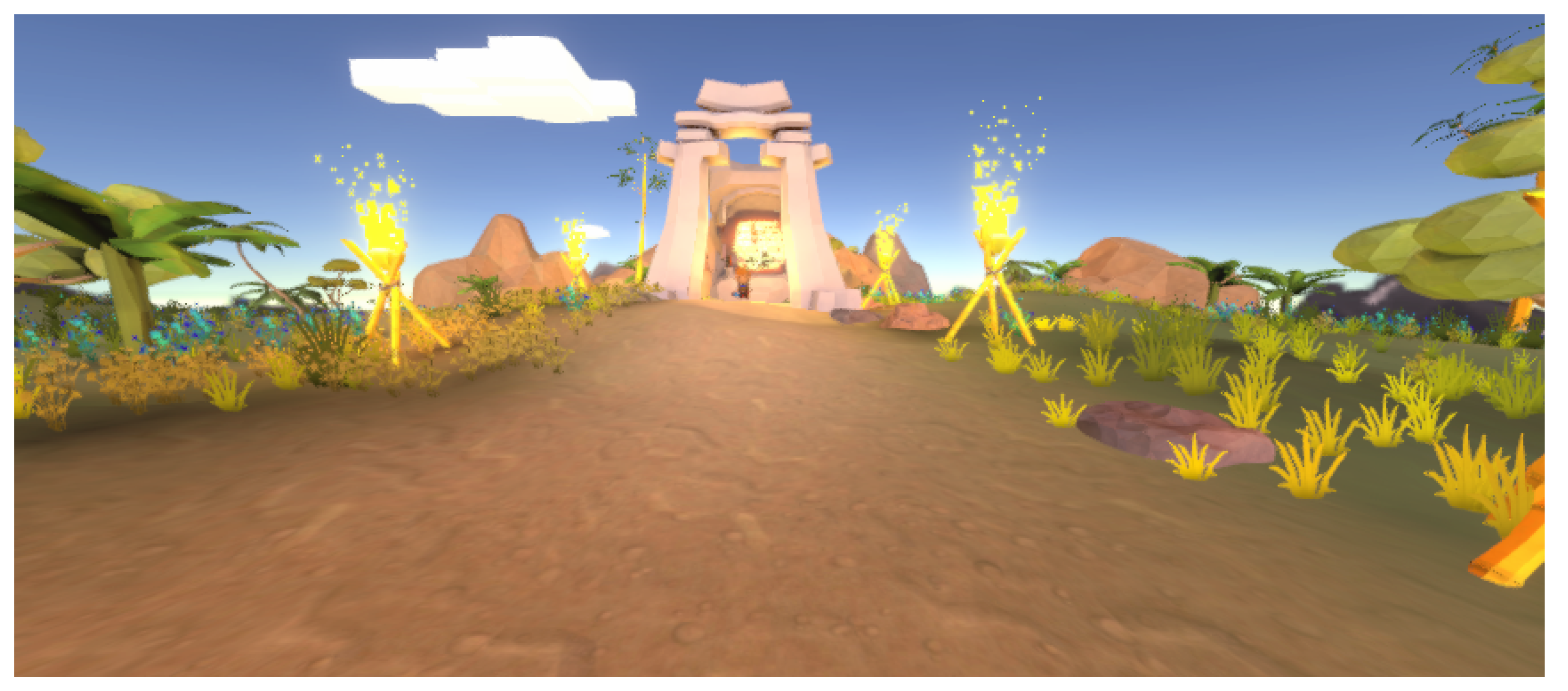
For the implementation of the VaccineHero application, the Unity game engine was utilised in combination with the C# programming language. The main scene of the 3D world (Figure 4) was populated with models from the Unity Asset Store, which were processed as needed through the Unity application to adapt to the needs of the game. The processing included the improvement of the textures and an analysis of the models, as well as the correction of compatibility problems between some of the models and the Unity application.
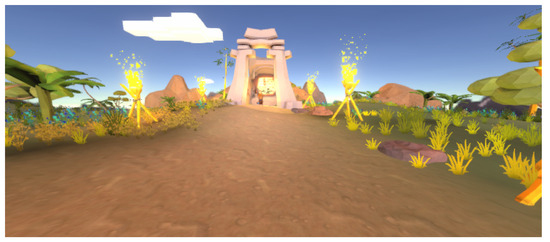
Figure 4.
Main scene.
The models have been enriched with the addition of new functions, such as movements and special effects, which enhance the overall user experience.
When it comes to sound, there is music in the background throughout the story, which helps create a pleasant atmosphere. Additionally, scripts are used to add sounds to different events in the VR world, which combine to create an interesting, pleasant, seamless, and immersive experience for the child. The sounds were added by using an audio source and attaching an audio clip to each relevant component.
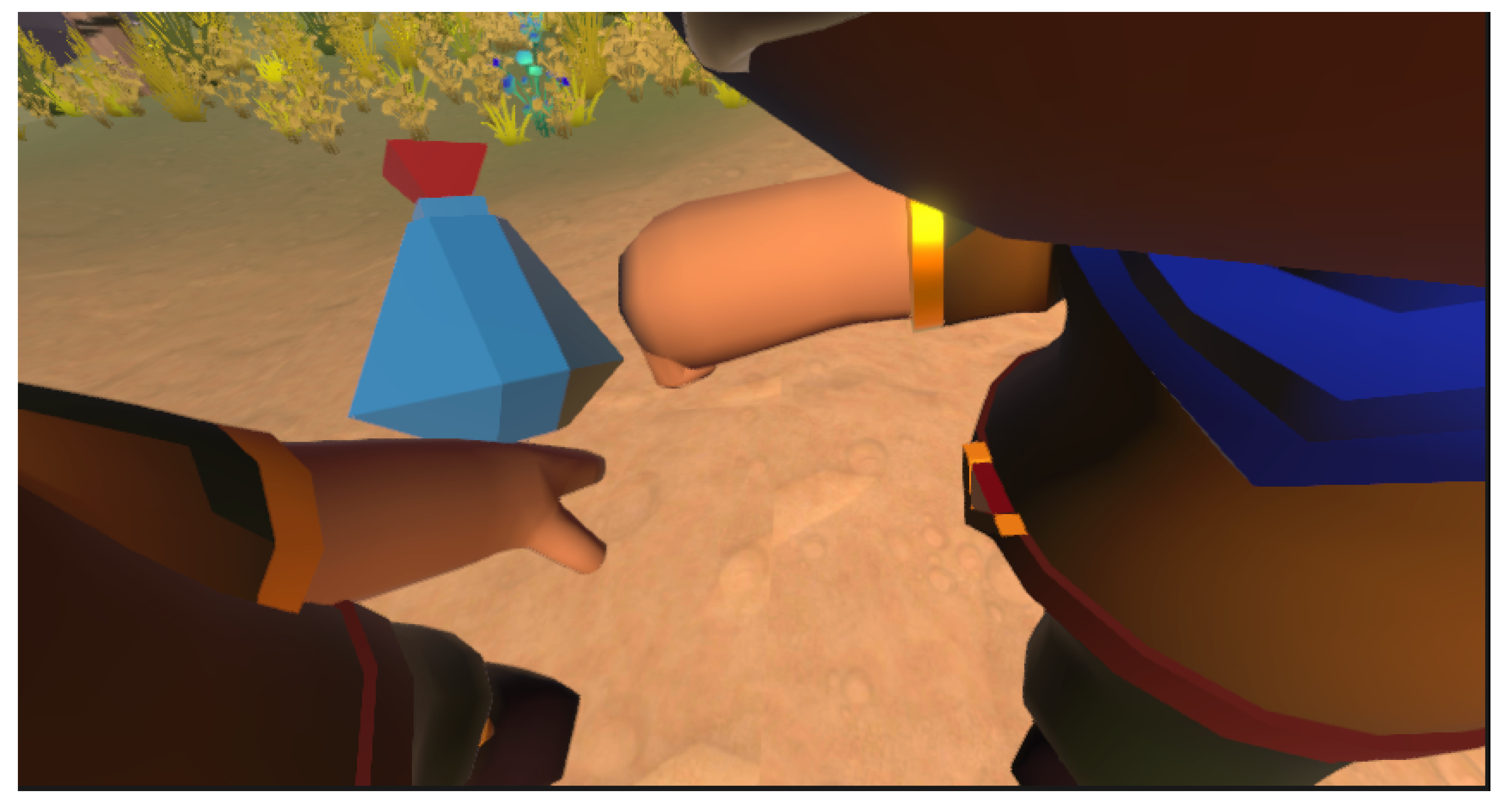
To achieve the connection between the virtual and physical worlds, the story that is presented to the child includes two key moments. In the first one, the magician touches the hero with an elixir (see Figure 5), and in the second one, the magician touches the hero again to bestow magical powers upon them.
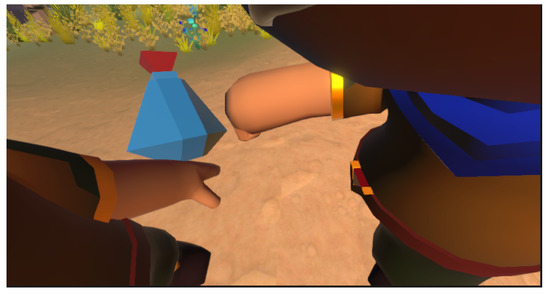
Figure 5.
The magician placing the elixir on the hero’s arm.
Regarding the duration and important key moments of the overall story, one needs to keep in mind that the main goal of the application is to support the vaccination of toddlers. The story is not developed with the intention of optimising its artistic value or even stimulating the children but rather to facilitate the work of medical professionals. Therefore, our team observed and timed a number of real-life conventional vaccinations; the average times were logged and then presented to and confirmed by doctors. This is how the overall duration of 90 s was determined, as well as the exact time and duration of each contact between the magician and the hero, so that it would be sufficient for medical professionals to clean the area of vaccination with alcohol, leave enough time for the area to dry, and then return to perform the vaccination at a normal pace.
The decision was made to target the Android operating system in the development of the application. As Android devices are often at the lower end in terms of cost and processing capabilities, the graphics were adjusted to render correctly on devices with limited processing power. This was done in a manner that ensures any reduction in detail does not affect the scene’s descriptiveness, vividness, or believability.
A peculiarity of the implementation is that the story was designed to be experienced in first person, with the camera placed where the eyes of the hero would be. As the camera is allowed to rotate freely to follow the movement of the head of the child, the head was removed from the hero avatar. This way, we avoid the danger of it interfering with the camera and appearing in the display, making it seem as if the child was looking inside their own head.
Despite the fact that VaccineHero offers a novel approach to easing vaccination discomfort, practical challenges may still exist. Initial costs for VR headsets could be a barrier for some clinics. Additionally, healthcare providers would need training to use the technology effectively. Institutional resistance to the adoption of technology and the absence of on-site technical support could also hinder seamless implementation.
To address these practical limitations, it should be noted that the VaccineHero application was designed with compatibility in mind. Although any headset can be used, the design specifically targets two solutions: inexpensive Google Cardboard and more robust, disinfectable headsets. This flexibility aims to address the issue of equipment costs and availability, making it easier for a range of healthcare providers to implement the application to better support the real-life application of vaccinations. The first solution involves the now-discontinued Google Cardboard, which is still available for purchase in various stores. The advantage of Cardboard is that it is made of cheap materials (see Figure 6 and when purchased in bulk, it can cost just a few cents per item. Thus, it can be treated as a single-use expendable item, which is thrown away after the vaccination, similar to cotton and needles.

Figure 6.
Mobile placement in Google Cardboard.
The other solution is a more robust headset, such as the one presented in Figure 7. After each use, it can be sprayed with disinfectant and then wiped clean. In both cases, given the medical nature of the application, the fundamental requirement is that no tools are reused by different patients if they have not first been properly disinfected.

Figure 7.
A more professional model of a headset.
4. Clinical Trials and Evaluation
4.1. Ground Truth
We were not able to locate any similar study that used VR to facilitate vaccination and published quantified data regarding the discomfort levels of children for us to use in comparison with our approach. Therefore, to assess the efficacy of our approach, we can only compare it against the conventional immunisation approach.
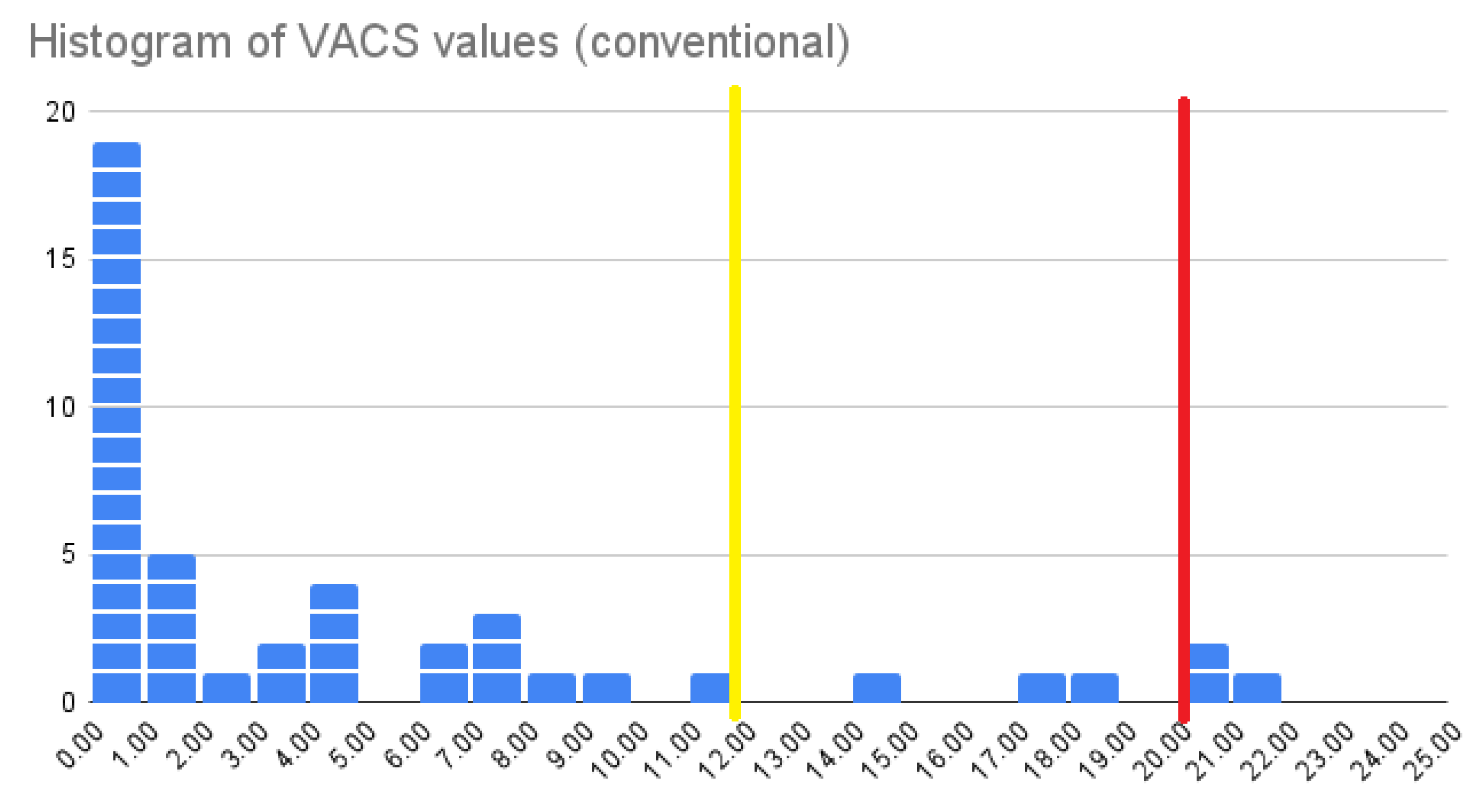
In previous work, we applied the conventional immunisation approach to a cohort of 40 children and recorded the VACS values [6]. VACS, the Vaccination Discomfort Scale, is a methodological tool that quantifies children’s discomfort during vaccination on a scale from 0 to 25, with 0 indicating no discomfort at all and 25 corresponding to maximum distress.
In Figure 8, we present a histogram of the VACS values for the cohort of 40 children aged 2–12 years old who were vaccinated conventionally. In our previous work, we found that doctors considered vaccination procedures to be smooth with acceptable levels of discomfort in children when VACS values did not surpass 19, whereas children considered the experience acceptable when VACS values were below 11. These two thresholds are indicated in the figure with red and yellow colours, respectively.
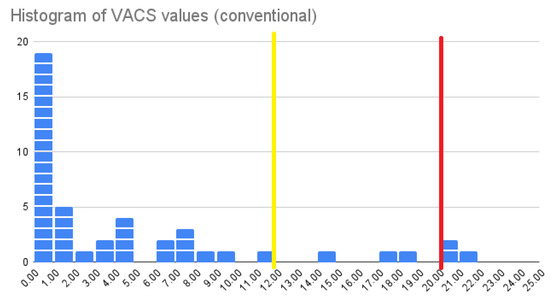
Figure 8.
Histogram of VACS values for the conventional vaccination approach.
In that cohort, we observed that the average VACS value for children’s vaccinations was 4.752; 40% of children did not experience any discomfort at all (with a VACS value of 0), and for the remaining children that did experience some discomfort, the average VACS value was 7.92.
These are the values against which we compare the performance of VaccineHero.
4.2. Trial Settings
To assess the efficacy of the VaccineHero system and validate the proposed approach, a clinical trial was set up involving two doctors with independent clinical practices. The doctors’ offices are located in Athens and Argos, Greece. The doctors were trained by our team in the use of the VaccineHero system. VaccineHero was deployed on their phones, and Miracast was activated to connect to the TV monitors in their offices. The doctors were also trained in the use of the Vaccination Discomfort Scale to assess children’s discomfort in a uniform and objective manner. Participants were recruited using convenience sampling.
Specifically, all children visiting one of the paediatric clinics participating in this research were considered. The two inclusion criteria were:
- The child was between 2 and 12 years old.
- The accompanying parent/guardian was sufficiently fluent in Greek to provide written informed consent.
These are the same inclusion criteria as in the earlier study [6] against which the performance of VaccineHero was evaluated.
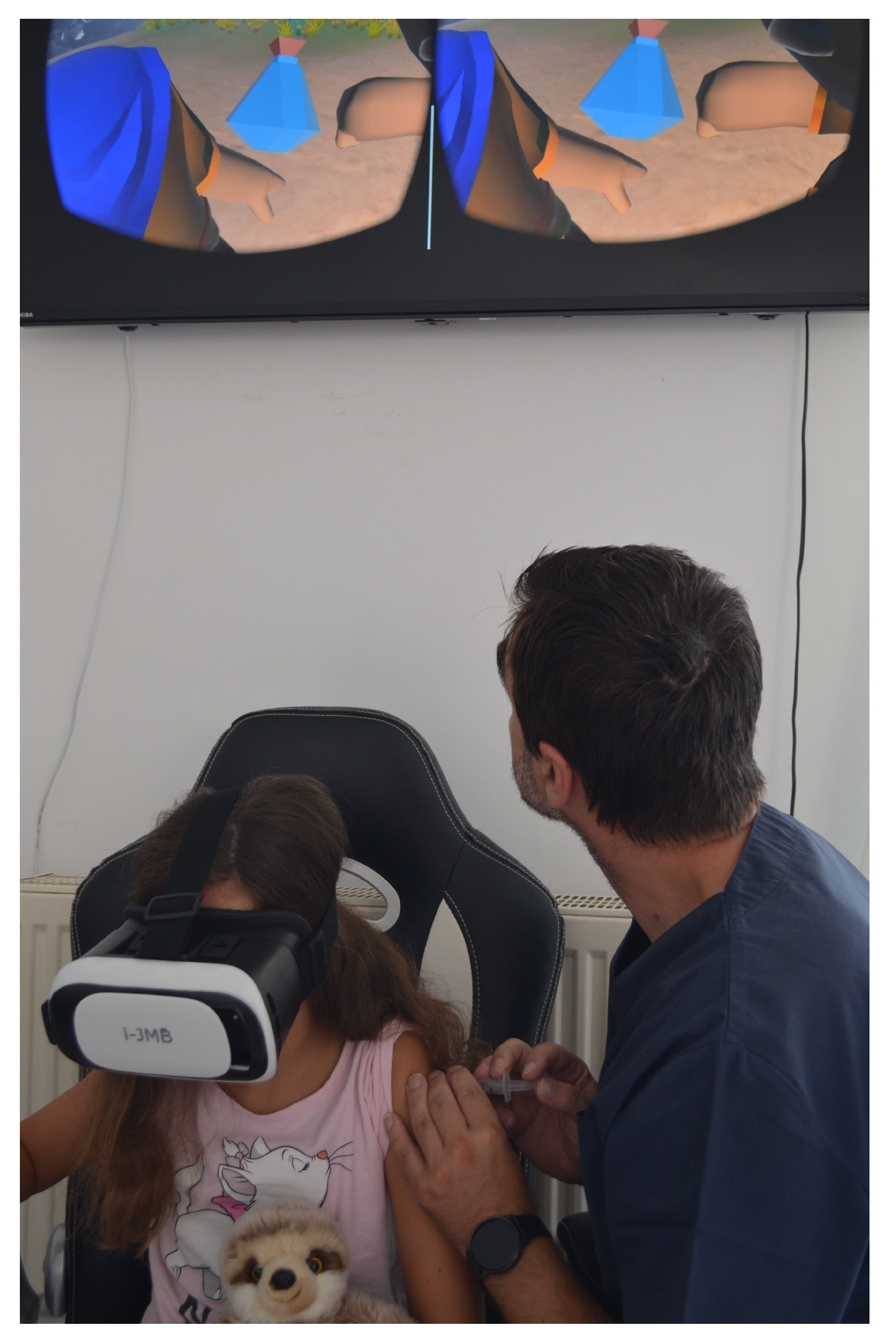
In Figure 9, we can see one of the doctors using the VaccineHero system to complete the immunisation of a young girl. In the figure, we can see the doctor observing the external monitor to perfectly time the delivery of the vaccination. For each such immunisation, the VACS scale data were recorded and forwarded to our team in an anonymised manner to be further processed as needed for our research.
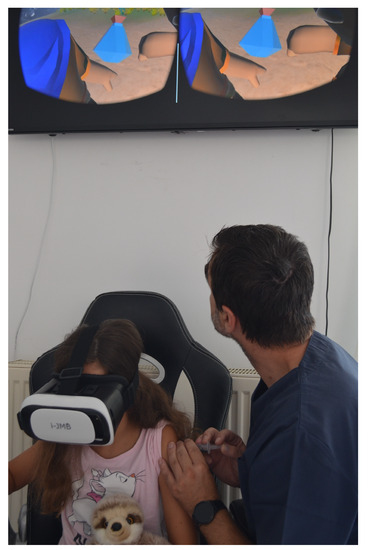
Figure 9.
Vaccination of a young girl using the VaccineHero system in a doctor’s office. The doctor watches the external monitor to synchronise the insertion of the needle with the VR content.
4.3. Clinical Data and Findings
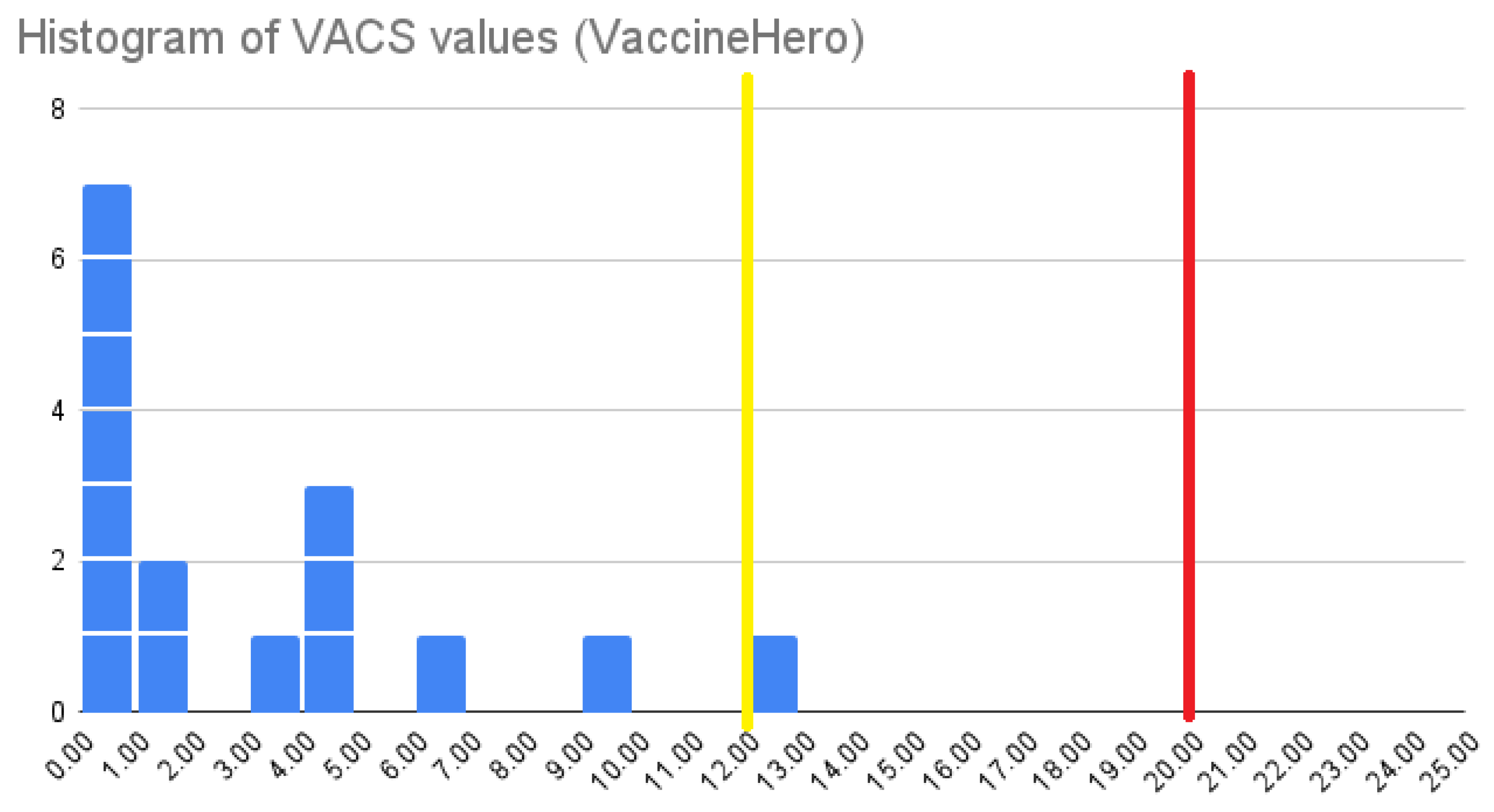
In total, 16 young patients aged 4–12 years old, with a mean age of 8.28 years, ranging from 3 years, 3 months, and 8 days old to 12 years, 9 months, and 22 days old, were vaccinated using the VaccineHero application in the period between 6 June and 4 July 2023. Of these children, 81.25% were boys and 18.75% were girls. All of them had completed the Greek-recommended vaccination schedule without any side effects or negative experiences in the past. The vaccination process took place in Greece. The VACS values were recorded for the children’s experiences, and a histogram of these values is presented in Figure 10. These parameters are similar to those of the cohort reported in [6], making the findings of the two studies directly comparable.
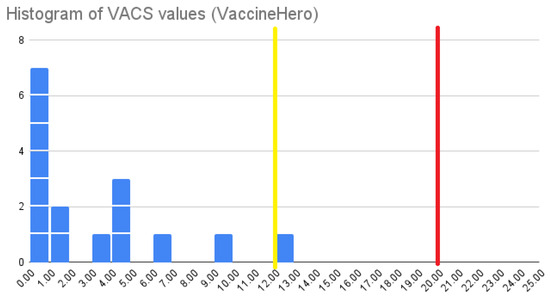
Figure 10.
Histogram of VACS values when using VaccineHero.
When comparing the two histograms (in Figure 8 and Figure 10), we can see that the percentage of children who experienced no discomfort whatsoever when vaccinated conventionally was 40%, which increased to 44% when using the VaccineHero system. Taking into account the relatively small cohort of 16 children in the VaccineHero trial, we consider this 10% increase to be marginal. Therefore, it is inconclusive whether VaccineHero indeed helps more children experience a discomfort-free immunisation, but it is clear that it does not augment the percentage of children who are troubled by the experience. We conclude that when considering only the percentage of children that experience any level of discomfort, VaccineHero is at least as good as the conventional approach. Therefore, it fulfils the principle of “First, do no harm”, which is central to the ethics of healthcare.
Let us now examine the observed VACS values in more detail. When examining the whole cohort of children, we acquired an average VACS value of 2.75. This constitutes a reduction of 42% compared to the 4.752 average VACS value observed when using the conventional vaccination approach. Similarly, when focusing only on the children for whom the VACS value was greater than zero, i.e., the children who did feel some level of discomfort, the average VACS value when using VaccineHero was 4.89. This amounts to a reduction of 38% compared to the 7.92 average VACS value observed when following the conventional immunisation method.
Another point to consider is how bad things can get for children. The maximum observed VACS value when using VaccineHero was 12. This is considerably lower than the value of 19, which doctors considered acceptable discomfort, and very close to the value of 11, which was considered acceptable by children. For comparison, in the conventional vaccination approach, the maximum observed VACS value was 21, which was above the acceptable thresholds for both doctors and children.
Overall, we conclude that VaccineHero does not necessarily alter the percentage of children who feel some discomfort. But for those children who do feel discomfort, it makes a huge difference, reducing their discomfort levels by approximately 40% and making the overall experience acceptable to both children and doctors.
5. Conclusions
In this work, we presented VaccineHero, an extended reality system that aims to reduce toddlers’ discomfort during the immunisation procedure. After discussing the relevant literature, we presented the main concept of our proposal and illustrated the implementation of the VaccineHero system. A clinical trial involving two different clinics and doctors was performed, and the efficacy of the system was compared against the conventional immunisation method.
An impressive—in our subjective opinion—reduction of 40% in children’s measured discomfort was observed, and extreme discomfort was completely eliminated, which validates our approach and establishes the efficacy of our implementation. With young children making up a quarter of the world’s population, any intervention that affects the quality of their experience in a procedure as frequent as children’s vaccinations, and by extension, the quality of the experience of their parents, is an intervention that has the potential to make a huge difference in the quality of life of many people.
The fact that VaccineHero requires only a simple headset that is cheap, easy to acquire, and reusable; a simple Android phone; and a TV monitor that most doctors’ offices already have, makes it a very affordable solution. This, combined with the fact that no special prior knowledge is required by the doctors, who can be trained to use the system within a few minutes, makes VaccineHero easy to be widely adopted, thus having the potential to reach and help thousands of children. In fact, we are currently in the process of deploying VaccineHero and training physicians in a number of locations in Athens and other cities in Greece that are further away from the capital.
We are, of course, pleased with the reduction we observed in children’s discomfort when using VaccineHero, as well as its potential to reach even more children. Still, much more can be done to further extend both the current work and the system in general. Regarding the evaluation of our work, we intend to continue gathering data so that we can perform an assessment using a data set comprising several hundred patients. This will allow us to calculate the average VACS values with greater reliability and smaller error margins. It will also be interesting to examine not just the overall VACS values, which describe the total discomfort experienced by the child throughout the procedure, but also the independent components to assess the stages of the vaccination procedure in which VaccineHero has the biggest impact and in which stages more could be achieved.
Similarly, it will be interesting to examine whether age, gender, or other external parameters have a correlation with the experienced discomfort and the effectiveness of the VaccineHero system. Examining this was not possible in the current study, given the size of the cohort. Therefore, such considerations are part of our immediate future work.
When examining VaccineHero from a different perspective, we can see that it comprises a combination of visual and audio modalities. From a psychologist’s perspective, it would also be interesting to investigate whether it is the overall immersion or specifically the visual or audio stimuli that have the greatest impact on reducing discomfort. This question is outside the scope of our own work and expertise, but we welcome potential exploration by others and would be happy to provide assistance and relevant resources to interested researchers.
Regarding the features of the system, it is currently configured to suit vaccination in the left arm, which works best for right-handed children. With right-handed individuals constituting 90–95% of the population [42,43], this means that there is an additional 5–10% that are not served equally by this version of VaccineHero. In our future work, we intend to make the application configurable so that the immunisation arm can be selected by the doctor.
Finally, regarding the scope of application, vaccination is not the only possibility. Distractions have been shown to have a positive impact on the blood drawing experience [44,45], and fear of needles has been found to be a deterrent for blood donation [46]. New versions of the application can be adapted to support both of these medical procedures, helping not only children but also adults who may experience discomfort with procedures that involve needles.
Author Contributions
Conceptualisation, S.A., V.R., M.W., and V.P.; methodology, M.W. and V.P.; software, V.R.; validation, S.A; resources, S.A., M.W., and V.P.; data curation, M.W.; writing—original draft preparation, S.A., V.R., and M.W.; writing—review and editing, V.P. and G.L.; visualisation, V.R. and M.W; supervision, M.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The research described herein has been approved by the Research Ethics Committee of the University of Peloponnese (approval number 15884/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cassimos, D.C.; Effraimidou, E.; Medic, S.; Konstantinidis, T.; Theodoridou, M.; Maltezou, H.C. Vaccination Programs for Adults in Europe, 2019. Vaccines 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, W.A.; Ahmet, R. Simply put: Vaccination saves lives. Proc. Natl. Acad. Sci. USA 2017, 114, 4031–4033. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-(2019) (accessed on 4 August 2023).
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef]
- Orenius, T.; LicPsych, S.H.; Mikola, K.; Ristolainen, L. Fear of Injections and Needle Phobia among Children and Adolescents: An Overview of Psychological, Behavioral, and Contextual Factors. Sage Open Nurs. 2018, 4, 2377960818759442. [Google Scholar] [CrossRef]
- Wallace, M.; Antonopoulos, S.; Poulopoulos, V. VACS: VAccination disComfort Scale. Clin. Pract. 2022, 12, 1078–1091. [Google Scholar] [CrossRef]
- Hough-Telford, C.; Kimberlin, D.W.; Aban, I.; Hitchcock, W.P.; Almquist, J.; Kratz, R.; O’Connor, K.G. Vaccine delays, refusals, and patient dismissals: A survey of pediatricians. Pediatrics 2016, 138, e20162127. [Google Scholar] [CrossRef]
- Jacobson, R.M.; Swan, A.; Adegbenro, A.; Ludington, S.L.; Wollan, P.C.; Pol, G.A. Making vaccines more acceptable—Methods to prevent and minimize pain and other common adverse events associated with vaccines. Vaccine 2001, 19, 2418–2427. [Google Scholar] [CrossRef]
- Taddio, A.; Appleton, M.; Bortolussi, R.; Chambers, C.; Dubey, V.; Halperin, S.; Hanrahan, A.; Ipp, M.; Lockett, D.; MacDonald, N.; et al. Reducing the pain of childhood vaccination: An evidence-based clinical practice guideline. Coll. Emerg. Med. Team 2010, 182, E843–E855. [Google Scholar] [CrossRef]
- Badovinac, S.; Gennis, H.; Riddell, R.P.; Garfield, H.; Greenberg, S. Understanding the Relative Contributions of Sensitive and Insensitive Parent Behaviors on Infant Vaccination Pain. Children 2018, 5, 80. [Google Scholar] [CrossRef] [PubMed]
- Blount, R.L.; Devine, K.A.; Cheng, P.S.; Simons, L.E.; Hayutin, L. The impact of adult behaviors and vocalizations on infant distress during immunizations. J. Pediatr. Psychol. 2008, 33, 1163–1174. [Google Scholar] [CrossRef]
- Esfahani, M.S.; Sheykhi, S.; Abdeyazdan, Z.; Jodakee, M.; Boroumandfar, K. A comparative study on vaccination pain in the methods of massage therapy and mothers’ breast feeding during injection of infants referring to Navabsafavi Health Care Center in Isfahan. Iran. J. Nurs. Midwifery Res. 2013, 18, 494–498. [Google Scholar] [PubMed]
- Osinaike, B.B.; Oyedeji, A.O.; Adeoye, O.T.; Dairo, M.D.; Aderinto, D.A. Effect of breastfeeding during venepuncture in neonates. Ann. Trop. Paediatr. 2007, 27, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.; Miller, L.W.; Phillipp, B.L.; Blass, E.M. Breastfeeding is analgesic in healthy newborns. Pediatrics 2002, 109, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.L.; MacLaren, J.E.; Fortson, B.L.; Friedman, A.; DeMore, M.; Lim, C.S.; Shelton, E.; Gangaram, B. Randomized clinical trial of distraction for infant immunization pain. Pain 2006, 125, 165–171. [Google Scholar] [CrossRef]
- Golinau, B.; Krane, E.; Seybold, J.; Almgren, C.; An, K.J. Non-pharmacological techniques for pain management in neonates. Semin. Perinatol. 2007, 31, 318–322. [Google Scholar] [CrossRef]
- Lacey, C.M.; Finkelstein, M.; Thygeson, M.V. The impact of positioning on fear during immunizations: Supine versus sitting up. J. Pediatr. Nurs. 2008, 23, 195–200. [Google Scholar] [CrossRef]
- Thyr, M.; Sundholm, A.; Teel, L.; Rahm, V.A. Oral glucose as an analgesic to reduce infant distress following immunization at the age of 3, 5 and 12 months. Acta Paediatr. 2007, 96, 233–236. [Google Scholar] [CrossRef]
- Golestan, M.; Sadrebafghi, M.; Karbasi, S.A.; Eslami, Z.; Hashemi, A.; Mirnaseri, F.; Mosadegh, M.M.; Kholasehzadeh, R. Comparison Pain relieving effects of glucose and water in neonates. Iran. J. Pediatr. 2006, 16, 441–446. [Google Scholar]
- Thomas, L. On the Science and Technology of Medicine. Daedalus 1988, 117, 299–316. Available online: http://www.jstor.org/stable/20025180 (accessed on 4 August 2023).
- Bradley, W.G. History of medical imaging. Proc. Am. Philos. Soc. 2008, 152, 349–361. [Google Scholar]
- Maglogiannis, I.G.; Karpouzis, K.; Wallace, M. Image and signal processing for networked e-health applications. In Synthesis Lectures on Biomedical Engineering; Springer: Cham, Switzerland, 2005; Volume 1, pp. 1–108. [Google Scholar]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. NPJ Digit. Med. 2020, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.S. Role of chat gpt in public health. Ann. Biomed. Eng. 2023, 51, 868–869. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.; Haleem, A. Virtual reality applications toward medical field. Clin. Epidemiol. Glob. Health 2020, 8, 600–605. [Google Scholar] [CrossRef]
- Li, L.; Yu, F.; Shi, D.; Shi, J.; Tian, Z.; Yang, J.; Wang, X.; Jiang, Q. Application of virtual reality technology in clinical medicine. Am. J. Transl. Res. 2017, 9, 3867. [Google Scholar]
- Javaid, M.; Haleem, A. Industry 4.0 applications in medical field: A brief review. Curr. Med. Res. Pract. 2019, 9, 102–109. [Google Scholar] [CrossRef]
- Coyne, L.; Merritt, T.A.; Parmentier, B.L.; Sharpton, R.A.; Takemoto, J.K. The past, present, and future of virtual reality in pharmacy education. Am. J. Pharm. Educ. 2019, 83, 3. [Google Scholar] [CrossRef]
- Lin, M.T.Y.; Wang, J.S.; Kuo, H.M.; Luo, Y. A study on the effect of virtual reality 3D exploratory education on students’ creativity and leadership. Eurasia J. Math. Sci. Technol. Educ. 2017, 13, 3151–3161. [Google Scholar] [CrossRef]
- Mazurek, J.; Kiper, P.; Cieślik, B.; Rutkowski, S.; Mehlich, K.; Turolla, A.; Szczepańska-Gieracha, J. Virtual reality in medicine: A brief overview and future research directions. Hum. Mov. 2019, 20, 16–22. [Google Scholar] [CrossRef]
- Khan, R.; Plahouras, J.; Johnston, B.C.; Scaffidi, M.A.; Grover, S.C.; Walsh, C.M. Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy. Cochrane Database Syst. Rev. 2018, 8, CD008237. [Google Scholar] [CrossRef]
- Bracq, M.-S.; Michinov, E.; Jannin, P. Virtual Reality Simulation in Nontechnical Skills Training for Healthcare Professionals: A Systematic Review. Simul. Healthc. 2019, 14, 188–194. [Google Scholar] [CrossRef]
- Ghai, S.; Ghai, I. Virtual reality enhances gait in cerebral palsy: A training dose-response meta-analysis. Front. Neurol. 2019, 10, 236. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.K.; Lourenço, C.B.; Chilingaryan, G.; Sveistrup, H.; Levin, M.F. Arm motor recovery using a virtual reality intervention in chronic stroke: Randomized control trial. Neurorehabilit. Neural Repair 2013, 27, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Optale, G.; Urgesi, C.; Busato, V.; Marin, S.; Piron, L.; Priftis, K.; Gamberini, L.; Capodieci, S.; Bordin, A. Controlling memory impairment in elderly adults using virtual reality memory training: A randomized controlled pilot study. Neurorehabilit. Neural Repair 2010, 24, 348–357. [Google Scholar] [CrossRef]
- Kipping, B.; Rodger, S.; Miller, K.; Kimble, R.M. Virtual reality for acute pain reduction in adolescents undergoing burn wound care: A prospective randomized controlled trial. Burns 2012, 38, 650–657. [Google Scholar] [CrossRef]
- Ministry of Health. MOH Launches VR to Help Kids Overcome Fear of Immunization. 3 August 2018. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2018-08-03-0017.aspx (accessed on 5 August 2023).
- Ogilvy. VR Vaccine. Available online: https://www.ogilvy.com.br/hermes-1/ (accessed on 5 August 2023).
- Chang, Z.Y.; Kang, G.C.; Koh, E.Y.L.; Fong, R.J.K.; Tang, J.; Goh, C.K.; Tan, N.C. Immersive Virtual Reality in Alleviating Pain and Anxiety in Children During Immunization in Primary Care: A Pilot Randomized Controlled Trial. Front. Pediatr. 2022, 10, 847257. [Google Scholar] [CrossRef]
- Taddio, A.; Ilersich, A.; McMurtry, C.M.; Bucci, L.M.; MacDonald, N.E. Foodborne and Animal Contact Disease Outbreaks: Managing pain and fear: Playing your CARDs to improve the vaccination experience. Can. Commun. Dis. Rep. 2021, 47, 87. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, A.M.; PremChander, R.T.; Nagaraja, G.S. Extended Display Mode Using Android Miracast. In Proceedings of the International Conference Computational Systems for Health & Sustainability, Bangalore, India, 17–18 April 2015; pp. 84–86. [Google Scholar]
- Annett, M. The binomial distribution of right, mixed, and left handedness. Q. J. Exp. Psychol. 1967, 19, 327–333. [Google Scholar] [CrossRef]
- Porac, C.; Coren, S. Relationships among lateral preference behaviors in human beings. Behav. Brain Sci. 1978, 2, 311–312. [Google Scholar] [CrossRef]
- Çelikol, Ş.; Tural, B.E.; Yıldızlar, O. Children’s Pain, Fear, and Anxiety During Invasive Procedures. Nurs. Sci. Q. 2019, 32, 226–232. [Google Scholar] [CrossRef]
- Piazza, J.R.; Merkel, S.; Rothberg, B.; Gargaro, J.; Kullgren, K. Understanding both sides of the blood draw: The experience of the pediatric patient and the phlebotomist. Patient Exp. J. 2022, 9, 35–45. [Google Scholar] [CrossRef]
- Yuan, S.; Hoffman, M.; Lu, Q.; Goldfinger, D.; Ziman, A. Motivating factors and deterrents for blood donation among donors at a university campus–based collection center. Transfusion 2011, 51, 2438–2444. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).