
Combining MUSHRA Test and Fuzzy Logic in the Evaluation of Benefits of Using Hearing Prostheses

Abstract
:1. Introduction
- Evaluate the most common listening situations encountered by the elderly hearing-impaired person;
- Evaluate the benefits of the hearing instruments by taking into account the degree of hearing loss, the experience of the user, and the type of hearing devices used;
- Evaluate non-acoustic indicators and aspects of hearing device use;
- Be easy to implement in a large number of hearing care settings and take advantage of existing staff resources and typical audiological equipment;
- Allow for a quick assessment of benefits, i.e., the procedure should not be time consuming and tiring;
- Be implemented as an easy-to-use software application.
1.1. Background of the Study—Evaluating the Effectiveness of Hearing Aid Use
- Free-field tonal audiogram—an audiometric test is performed twice for a given patient, at a minimum of two-week intervals. The test is performed without a hearing aid and then with a hearing aid in place. The fitting gain is calculated by comparing the hearing threshold waveform curves in the presence of a hearing aid and without a hearing aid for three frequency components: 500, 1000, and 2000 Hz [26].
- Acceptable Noise Level (ANL) test—is a method of determining how much noise a patient can tolerate while listening to the target signal/speaker. The test is conducted by first setting the patient’s speech to the most comfortable level (MCL). Then noise, such as speech babble, is added, and the patient is asked to adjust it to the highest level they can accept or “tolerate” while following the story told in the original speech signal. The level selected is called the Background Noise Level (BNL). ANL is defined as MCL minus BNL. This is the lowest SNR that is acceptable to the patient. People with a low ANL (<7 dB) may become regular users of hearing aids because they are willing to put up with amplified noise levels close to the signal of interest. Conversely, people with high ANL (>13 dB) are likely to use hearing aids less often or not at all because they find amplified noise undesirable in too many situations. Of course, there is a large gray area in the middle (ANL values between 7 and 13 dB) for which the acceptance of hearing aids is uncertain [27].
- Speech intelligibility test in silence—the most commonly used verbal material is lists of single-syllable words. The patient’s task is to repeat the words given by a speaker 1 m away from the listener. The sound level of the administered test is 65 dB. The percentage of correctly repeated words is tested first when the patient does not have a hearing aid, and then the procedure is repeated with a hearing aid in place. The free-field test is repeated after a minimum of two weeks. The speech intelligibility benefit is expressed as the difference in the percentage of correctly repeated words in the presence of a hearing aid and without a hearing aid [28].
- Hearing in Noise Test (HINT) is a test of hearing in noise that measures sentence recognition against background noise. The verbal material consists of 250 sentences, which are divided into 25 lists. This test can be conducted in silence. In this case, a threshold for sentence recognition is obtained. If the test is conducted in noise, it allows estimating the SNR threshold for speech recognition in noise. By employing this test, it is possible to show the advantage of binaural directional hearing and, thus, binaural prosthetics [29,30].
- Quick speech-in-noise test (QuickSIN) allows for a short (test duration is about 1 min) estimation of the SNR level at which the patient will achieve 50% correct responses. The verbal material contains sentences that consist of five keywords each, presented against a background of noise (four-talker babble noise). The SNR level can be adjusted. Possible settings are 25, 20, 15, 10, 5, and 0 dB [30].
- EC (Ease of Communication)—the ability to communicate in silence, the effort to communicate under relatively easy listening conditions;
- RV (Reverberation)—the ability to communicate in the presence of echoes, describes understanding speech in moderately reverberant conditions;
- BN (Background Noise)—the ability to communicate in the presence of background noise describes speech understanding in the presence of multiple speakers or other competing listening conditions (environmental noise);
- To compare the functioning of a given person with a hearing aid(s) with the results of a reference group using hearing aids successfully [36];
- To document the benefits of using hearing aids in different environments to improve (eliminate) ineffective fittings as well as to compare the gain using various hearing aids or different hearing aid programs [36];
- To confirm the effectiveness of new selection and tuning procedures for hearing aids or other assistive listening devices [31].
2. Materials and Methods
Method Modification
3. Results
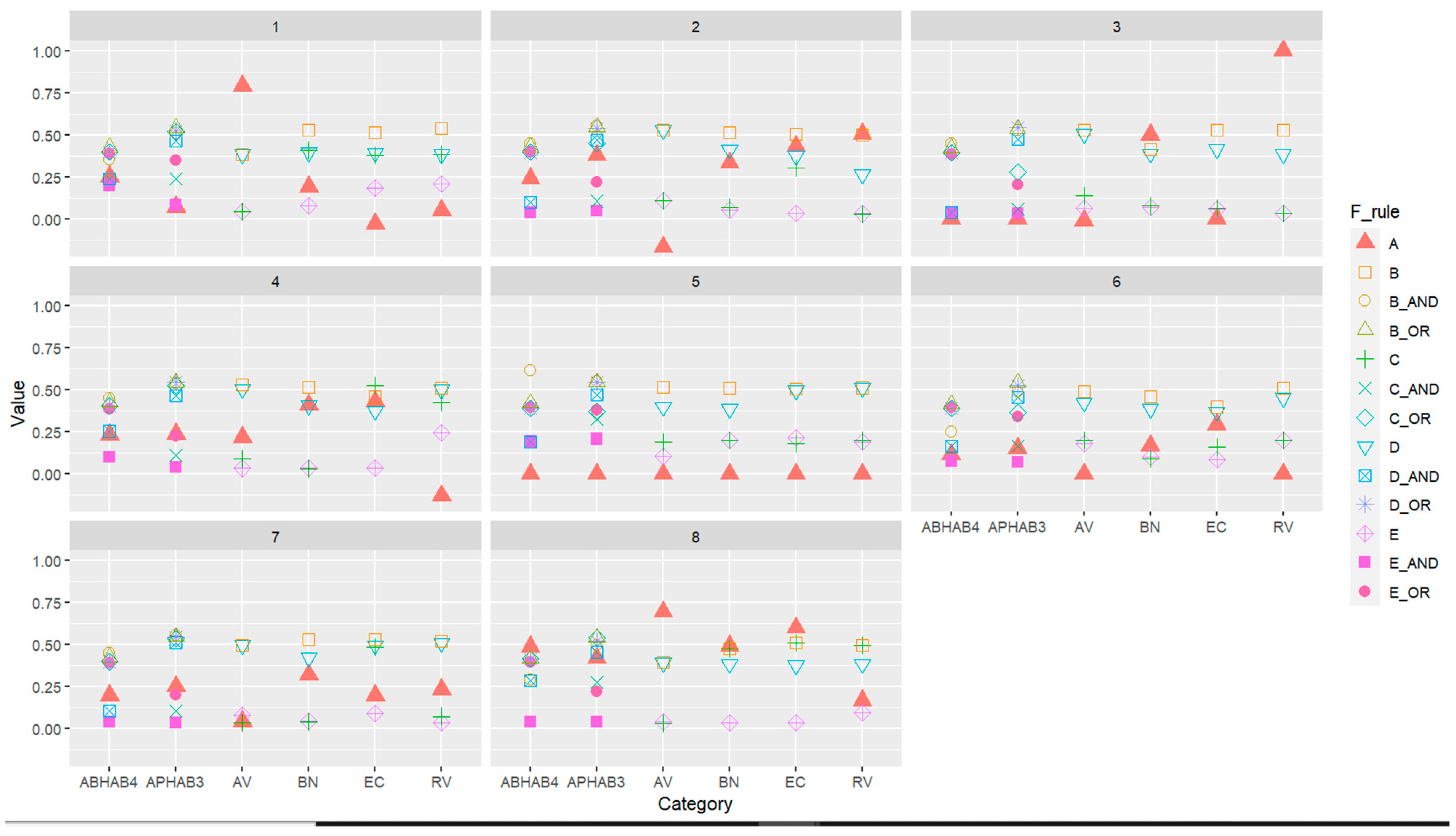
- Classically, the gain is calculated as the difference between average ratings without hearing aids and average ratings in hearing aids (denoted as A—in Figure 10).
- In a modification of the method using fuzzy logic to determine the profit in a given category (EC, BN, RV, AV), the following rule variants were used:
- IF Category without HA Evaluation OR Category with HA Evaluation THEN Rating of benefit—in this case, the number of inputs of the system will correspond to the number of evaluations made in the category, i.e., from 2 to 12 (denoted as B—in Figure 10).
- IF Category without HA Evaluation AND Category with HA Evaluation THEN Rating of benefit—in which case the number of system entries will correspond to the number of assessments made in the category, i.e., from 2 to 12 (denoted as C—in Figure 10).
- IF Mean of category without HA Evaluation OR Mean of category with HA Evaluation THEN Rating of benefit—in this case, the number of inputs of the system will equal 2 (denoted as D—in Figure 10).
- IF Mean of category without HA Evaluation AND Mean of category with HA Evaluation THEN Rating of benefit—in this case, the number of inputs of the system will equal 2 (denoted as E—in Figure 10).
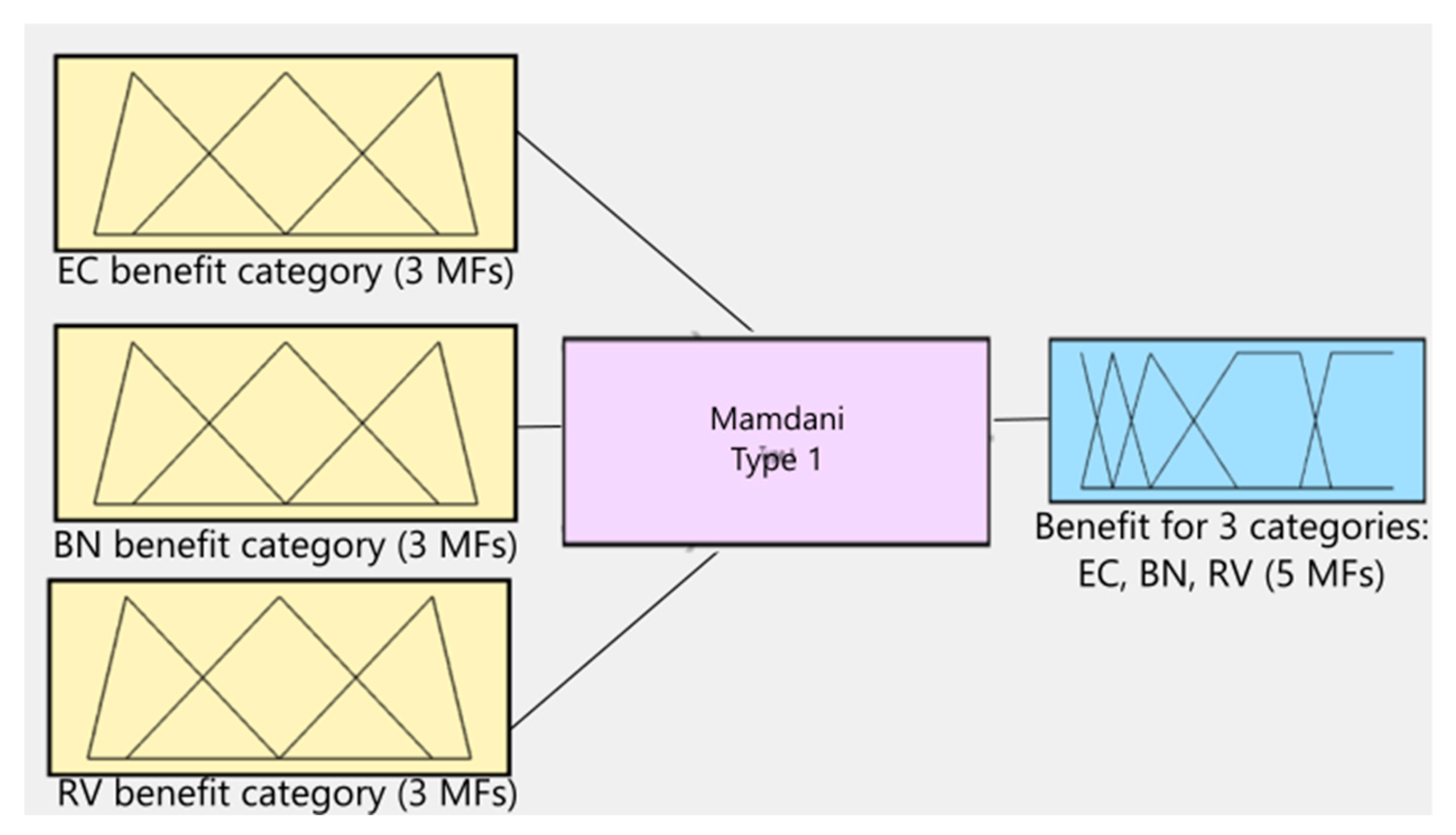
- In a modification of the method using fuzzy logic to determine the expected profit for the three categories (EC, BN, RV), the following rule variants were used:
- IF Benefit of EC category Evaluation OR Benefit of BN category Evaluation OR Benefit of RV category Evaluation THEN Rating of benefit—in this case, the number of inputs of the system corresponds to the number of categories.
- IF Benefit of EC category Evaluation AND Benefit of BN category Evaluation AND Benefit of RV category Evaluation THEN Rating of benefit—in this case, the number of system inputs corresponds to the number of categories.
- In a modification of the method using fuzzy logic to determine the expected profit for the four categories (EC, BN, RV, AV), the following rule variants were used:
- IF Benefit of EC category Evaluation OR Benefit of BN category Evaluation OR Benefit of RV category Evaluation OR Benefit of AV category Evaluation THEN Rating of benefit—in this case, the number of inputs of the system corresponds to the number of categories.
- IF Benefit of EC category Evaluation AND Benefit of BN category Evaluation AND Benefit of RV category Evaluation Benefit of RV category Evaluation AND Benefit of AV category Evaluation THEN Rating of benefit—in which case the number of system inputs corresponds to the number of categories.
4. Discussion
5. Conclusions and Future Research Aspects
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wasmann, J.W.A.; Lanting, C.P.; Huinck, W.J.; Mylanus, E.A.; van der Laak, J.W.; Govaerts, P.J.; Swanepoel, D.W.; Moore, D.R.; Barbour, D.L. Computational audiology: New approaches to advance hearing health care in the digital age. Ear Hear. 2021, 42, 1499. [Google Scholar] [CrossRef] [PubMed]
- Wasmann, J.W.; Pragt, L.; Eikelboom, R.; Swanepoel, D.W. Digital approaches to automated and machine learning assessments of hearing: Scoping review. J. Med. Internet Res. 2021, 24, e32581. [Google Scholar] [CrossRef]
- Almufarrij, I.; Dillon, H.; Dawes, P.; Moore, D.R.; Yeung, W.; Charalambous, A.P.; Munro, K.J. Web- and app-based tools for remote hearing assessment: A scoping review. Int. J. Audiol. 2022, 62, 699–712. [Google Scholar] [CrossRef]
- Schlittenlacher, J.; Turner, R.E.; Moore, B.C.J. Audiogram estimation using Bayesian active learning. J. Acoust. Soc. Am. 2018, 144, 421–430. [Google Scholar] [CrossRef]
- AI’s Latest Frontier Part 3: An AI Chatbot for Audiology. Available online: https://computationalaudiology.com/ais-latest-frontier-part-3-an-ai-chatbot-for-audiology/ (accessed on 2 August 2023).
- Swanepoel, D.W.; Manchaiah, V.; Wasmann, J.W.A. The Rise of AI Chatbots in Hearing Health Care. Hear. J. 2023, 76, 26–30. [Google Scholar] [CrossRef]
- Healy, E.W.; Johnson, E.M.; Pandey, A.; Wang, D. Progress made in the efficacy and viability of deep-learning-based noise reduction. J. Acoust. Soc. Am. 2023, 153, 2751. [Google Scholar] [CrossRef]
- Lesica, N.A.; Mehta, N.; Manjaly, J.G.; Deng, L.; Wilson, B.S.; Zeng, F.G. Harnessing the power of artificial intelligence to transform hearing healthcare and research. Nat. Mach. Intell. 2021, 3, 840–849. [Google Scholar] [CrossRef]
- World Health Organization, “World Report on Hearing.” Geneva. 2021. Available online: https://www.who.int/publications/i/item/9789240020481 (accessed on 26 July 2023).
- Giordano, P.; Argentero, P.; Canale, A.; Lacilla, M.; Albera, R. Evaluation of hearing aid benefit through a new questionnaire: CISQ (Complete Intelligibility Spatiality Quality). Acta Otorhinolaryngol. Ital. 2013, 5, 329–336. [Google Scholar]
- Löhler, J.; Gräbner, F.; Wollenberg, B.; Schalttmann, P.; Schönweiler, R. Sensitivity and specificity of the abbreviated profile of hearing aid benefit (APHAB). Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 3593–3598. [Google Scholar] [CrossRef]
- Turan, S.; Unsal, S.; Kurtaran, H. Satisfaction assessment with Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire on people using hearing aid having Real Ear Measurement (REM) eligibility. Int. Tinnitus J. 2019, 2, 97–102. [Google Scholar] [CrossRef]
- Shi, L.-F.; Doherty, K.A.; Kordas, T.M.; Pellegrino, J.T. Short-Term and Long-Term Hearing Aid Benefit and User Satisfaction: A Comparison between Two Fitting Protocols. J. Am. Acad. Audioil. 2007, 18, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.A.; Lutman, M.E. Relative benefits of linear analogue and advanced digital hearing aids. Int. J. Audiol. 2004, 43, 144–155. [Google Scholar] [PubMed]
- Mendel, L.L. Subjective and Objective Measures of Hearing Aid Outcome. AudiologyOnline [Online]. 2009. Available online: http://www.audiologyonline.com/articles/subjective-and-objective-measures-hearing-891 (accessed on 30 August 2023).
- Cox, R.M. Measuring Hearing Aid Outcomes: Part 1. J. Am. Acad. Audiol. 1999, 10. [Google Scholar] [CrossRef]
- Humes, L.E. Dimensions of hearing aid outcome. J. Am. Acad. Audiol. 1999, 10, 26–39. [Google Scholar]
- Jorgensen, L.E. Verification and validation of hearing aids: Opportunity not an obstacle. J. Otol. 2019, 11, 57–62. [Google Scholar] [CrossRef]
- Brian, T.A. Self-Report Assessment of Hearing Aid Outcome—An Overview. AudiologyOnline. 2007. Available online: http://www.audiologyonline.com/articles/self-report-assessment-hearing-aid-931 (accessed on 27 August 2023).
- Noble, W. Self-Assessment of Hearing; Plural Publishing Inc.: San Diego, CA, USA, 2013. [Google Scholar]
- Noble, W.; Jensen, S.N.; Naylor, G.; Bhullar, N.; Akeroyd, M.A. A short form of the Speech, Spatial and Qualities of Hearing scale suitable for clinical use: The SSQ12. Int. J. Audiol. 2013, 52, 409–412. [Google Scholar] [CrossRef]
- Tognola, G.; Mainardi, A.; Vincenti, V.; Cuda, D. Benefit of hearing aid use in the elderly: The impact of age, cognition and hearing impairment. ACTA Otorhinolaryngol. Ital. 2019, 39, 409. [Google Scholar] [CrossRef]
- Rehm, J.B.; Üstün, T.; Shekhar, S. On the development and psychometric testing of the WHO screening instrument to assess disablement in the general population. Int. J. Methods Psychiatr. Res. 1999, 8, 110–122. [Google Scholar]
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; von Korff, M.; Pull, C. Developing the World Health Organization Disability Assessment Schedule 2.0. 2010. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2971503/ (accessed on 27 August 2023).
- Schinkel-Bielefeld, N.; Kunz, P.; Zutz, A.; Buder, B. Evaluation of Hearing Aids in Everyday Life Using Ecological Momentary Assessment: What Situations Are We Missing? Am. J. Audiol. 2020, 29, 591–609. [Google Scholar] [CrossRef]
- Bray, V.; Nilsson, M. Assessing Hearing Aid Fittings: An Outcome Measures Battery Approach. In Strategies for Selecting and Verifying Hearing Aid Fittings; Thieme Medical Publishers: New York, NY, USA, 2002; pp. 151–175. [Google Scholar]
- Nabelek, A.K.; Tucker, F.M.; Letowski, T.R. Toleration of background noises: Relationship with patterns of hearing aid use by elderly persons. J. Speech Hear. Res. 1991, 34, 679–685. [Google Scholar]
- Mertens, G.; Andreis, E.; Clement, C.; Cochet, E.; Hofkens-Vand den Brandt, A.; Jacquemin, L.; Jonssen, I. Contralateral hearing aid use in adult cochlear implant recipients: Retrospective analysis of auditory outcomes. Int. J. Audiol. 2023. [Google Scholar] [CrossRef]
- Duncan, K.; Aarts, N. A Comparison of the HINT and Quick SIN Tests. J. Speech-Lang. Pathol. Audiol. 2006, 30, 86–94. [Google Scholar]
- Kilion, M.C.; Niquette, P.A.; Gudmundsen, G.I.; Revit, L.J.; Banerjee, S. Development of a quick speech-in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. J. Acoust. Soc. Am. 2004, 4, 2395–2405. [Google Scholar] [CrossRef]
- Sabin, A.T.; Van Tasell, D.J.; Rabinowitz, B.; Dhar, S. Validation of a Self-Fitting Method for Over-the-Counter Hearing Aids. Trends Hear. 2020, 3, 589. [Google Scholar] [CrossRef]
- Li, Q. A novel Likert scale based on fuzzy sets theory. Expert Syst. Appl. 2013, 40, 1609–1618. [Google Scholar]
- Vonglao, P. Application of fuzzy logic to improve the Likert scale to measure latent variables. Kasetsart J. Soc. Sci. 2017, 38, 337–344. [Google Scholar]
- Memmedova, K.; Ertuna, B. Development of a Fuzzy Likert Scales to Measure Variables in Social Sciences. Inf. Sci. 2023, in press. [Google Scholar] [CrossRef]
- Völker, C.T.; Bisitz, R.; Huber, B.; Kollmeier, I.S.M.; Ernst, A. Modifications of the MUlti stimulus test with Hidden Reference and Anchor (MUSHRA) for use in audiology. Int. J. Audiol. 2018, 57 (Suppl. 3), 92–104. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.M.; Alexander, G.C. The abbreviated profile of hearing aid benefit. Ear Hear. 1995, 16, 176–186. [Google Scholar] [CrossRef]
- Hojan, E. Protetyka Słuchu; Wydawnictwo Naukowe UAM: Poznań, Poland, 2014; pp. 715–721. [Google Scholar]
- Maidment, D.W.; Barker, A.B.; Xia, J.; Ferguson, M.A. A systematic review and meta-analysis assessing the effectiveness of alternative listening devices to conventional hearing aids in adults with hearing loss. Int. J. Audiol. 2018, 57, 721–729. [Google Scholar] [CrossRef]
- Simonsen, C.S.; Legarth, S.V. A Procedure for Sound Quality Evaluation of Hearing Aids. Hear. Rev. 2010, 25, 32–37. Available online: https://hearingreview.com/practice-building/practice-management/a-procedure-for-sound-quality-evaluation-of-hearing-aids (accessed on 27 August 2023).
- Moodle Open Source Learning Platform. Available online: https://moodle.org/ (accessed on 27 August 2023).
- Poremski, T.; Szymański, P.; Kostek, B. Assessment of the Effectiveness of a Short-term Hearing Aid Use in Patients with Different Degrees of Hearing Loss. Arch. Acoust. 2019, 44, 719–729. [Google Scholar] [CrossRef]
- Szymański, P.; Poremski, T.; Kostek, B. Pursuing Analytically the Influence of Hearing Aid Use on Auditory Perception in Various Acoustic Situations. Vib. Phys. Syst. 2022, 33, 2022101-1–2022101-8. [Google Scholar] [CrossRef]
- Method for the Subjective Assessment of Intermediate Quality Level of Audio Systems. ITU-R BS.1534-3 (10/2015). Available online: https://www.itu.int/rec/R-REC-BS.1534-3-201510-I/en (accessed on 27 August 2023).
- Beck, D.; Tryanski, D.; Kai Loong Man, B. Sound Quality and Hearing Aids. Hear. Rev. 2021, 28, 30–31. Available online: https://hearingreview.com/hearing-products/hearing-aids/psap/sound-6 (accessed on 27 August 2023).
- Suchomski, P.; Kostek, B.; Czyżewski, A. Hearing aid fitting method based on fuzzy logic processing. Arch. Acoust. 2008, 33, 153–158. Available online: https://acoustics.ippt.gov.pl/index.php/aa/article/view/851/730 (accessed on 27 August 2023).
- World Health Organisation. Report of the Informal Working Group on Prevention of Deafness and Hearing Impairment Programme Planning; World Health Organisation: Geneva, Switzerland, 1991. [Google Scholar]
- Pawlak, Z. Rough sets. Int. J. Comput. Inf. Sci. 1982, 11, 341–356. [Google Scholar] [CrossRef]
- Davidson, A.; Marrone, N.; Wong, B.; Musiek, F. Predicting Hearing Aid Satisfaction in Adults: A Systematic Review of Speech-in-noise Tests and Other Behavioral Measures. Ear Hear. 2021, 42, 1485–1498. [Google Scholar] [CrossRef]
- 2020 and the Future of Hearables. Available online: https://www.forbes.com/sites/forbestechcouncil/2020/05/21/2020-and-the-future-of-hearables/ (accessed on 16 August 2023).
- Aldaz, G.; Puria, S.; Leifer, L. Smartphone-based system for learning and inferring hearing aid settings. J. Am. Acad. Audiol. 2016, 27, 732–749. [Google Scholar] [CrossRef]
- Verma, L.; Sanju, H.K.; Scaria, B.; Awasthi, M.; Ravichandran, A.; Kaki, A.; Prakash, S.G.R. A Comparative Study on Hearing Aid Benefits of Digital Hearing Aid Use (BTE) from Six Months to Two Years. Int. Arch. Otorhinolaryngol. 2017, 21, 224–231. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | Always | 99% |
| B | Almost always | 87% |
| C | Generally | 75% |
| D | Half-the-time | 50% |
| E | Occasionally | 25% |
| F | Seldom | 12% |
| G | Never | 1% |
| Evaluation | Evaluation | Rating of Benefit | |||||
|---|---|---|---|---|---|---|---|
| IF | Category without HA | Never | OR | Category with HA | Never | THEN | No benefit |
| IF | Category without HA | Never | OR | Category with HA | Seldom | THEN | Low benefit |
| IF | Category without HA | Never | OR | Category with HA | Occasionally | THEN | Low benefit |
| IF | Category without HA | Never | OR | Category with HA | Half-of-time | THEN | Significant benefit |
| IF | Category without HA | Never | OR | Category with HA | Generally | THEN | High benefit |
| IF | Category without HA | Never | OR | Category with HA | Almost always | THEN | Great benefit |
| IF | Category without HA | Never | OR | Category with HA | Always | THEN | Great benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Never | THEN | No benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Seldom | THEN | No benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Occasionally | THEN | Low benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Half-of-time | THEN | Significant benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Generally | THEN | High benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Almost always | THEN | Great benefit |
| IF | Category without HA | Seldom | OR | Category with HA | Always | THEN | Great benefit |
| IF | Category without HA | Occasionally | OR | Category with HA | Never | THEN | No benefit |
| APHAB Item Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Occurs | 13 | 12 | 8 | 12 | 14 | 9 | 12 | 10 | 14 | 14 | 13 | 13 | 7 | 13 | 8 | 7 | 11 | 8 | 8 | 12 | 5 | 12 | 6 | 9 |
| Does not occur | 2 | 3 | 7 | 3 | 1 | 6 | 3 | 5 | 1 | 1 | 2 | 2 | 8 | 2 | 7 | 8 | 4 | 7 | 7 | 3 | 10 | 3 | 9 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szymański, P.; Poremski, T.; Kostek, B. Combining MUSHRA Test and Fuzzy Logic in the Evaluation of Benefits of Using Hearing Prostheses. Electronics 2023, 12, 4345. https://doi.org/10.3390/electronics12204345
Szymański P, Poremski T, Kostek B. Combining MUSHRA Test and Fuzzy Logic in the Evaluation of Benefits of Using Hearing Prostheses. Electronics. 2023; 12(20):4345. https://doi.org/10.3390/electronics12204345
Chicago/Turabian StyleSzymański, Piotr, Tomasz Poremski, and Bożena Kostek. 2023. "Combining MUSHRA Test and Fuzzy Logic in the Evaluation of Benefits of Using Hearing Prostheses" Electronics 12, no. 20: 4345. https://doi.org/10.3390/electronics12204345